

Association between Bone Turnover Markers and Fracture Healing in Long Bone Non-Union: A Systematic Review



Abstract
1. Introduction
2. Materials and Methods
Grouping of Studies and Synthesis of Data
3. Results
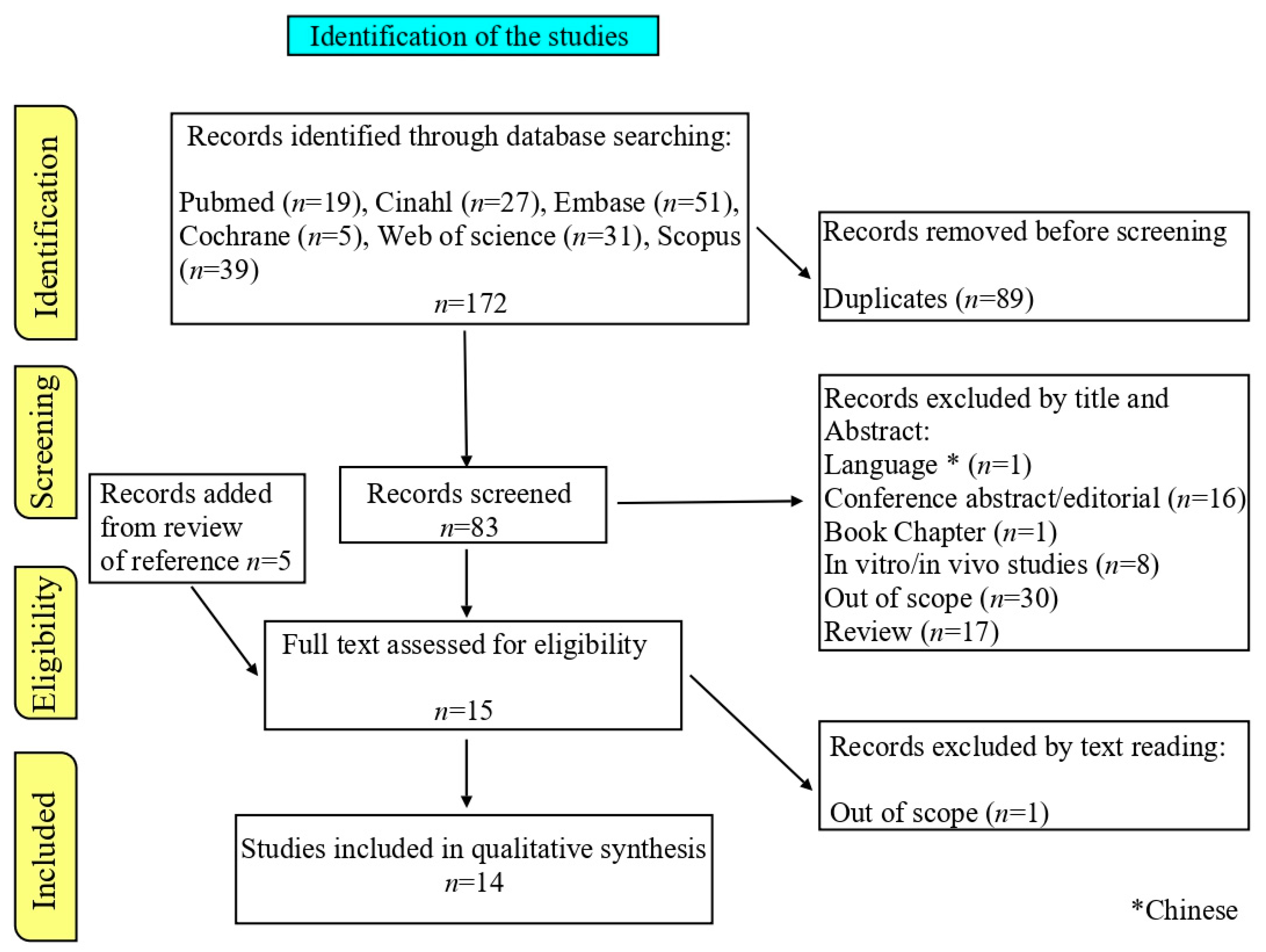
3.1. Study Selection
3.2. Study Characteristics
3.3. Study Reporting
- Healed fracture vs. healthy subjects (different patients and subjects).
- Healed fracture vs. non-union (different patients).
- Progression of the fracture healing over time in the same patient (healed or not healed).

{kind=link}
{kind=link}
| Reference | Sample Size | Site of Fracture | Gender (%Female) | Age | BTMs | Sampling Schedule | Number of Non-Unions | Findings |
|---|---|---|---|---|---|---|---|---|
| [22] | 33 NU pz and 35 hc (CTR) | Ulna, radius, humerus, fibula, femur, tibia, clavicle, metatarsus, scaphoid | NU: 31% CTR: 62% | NU: 18–78 (mean: 44) CTR: 23–78 (mean: 32) | Proteomic studies SELDI-TOF-MS and 2D-DIGE | - | 33 vs. 35 hc | Up/downregulation in NU vs. CTR: inter-α trypsin inhibitor, hepcidin, S100A8, S100A9, glycated hemoglobin β subunit, PACAP related peptide, complement C3 α-chain, apolipoprotein E, complement C3 and C6 subunits |
| [23] | 102 pz | Femur and tibia; 47% patients have additional fractures in other sites. | 31% | 18–50 (mean: 23) | CTx, P1NP (serum) | 6 and 12 weeks after fracture | 20/102 | CTx and P1NP (6 weeks) associated with healing at 12 weeks. |
| [24] | 26 DU or NU pz (3 months diagnosis) | Femur, tibia, fibula, humerus, unknown | 42% | 19–65 (mean: 40) | BAP, CTx, CICP, int-OC, N-Mid OC, OPG, RANKL (serum) | T0 and after 6, 12, and 24 weeks | 1/24 | BAP level is higher at 6 weeks in patients showing early healing. CICP, int-OC, N-Mid OC levels were lower at 6 weeks in patients that heal after 24 weeks |
| [25] | 36 pz | Tibial plateau fractures | 39% | 22–73 (mean: 46) | Collagen X (serum) | T0 and after 3, 6, and 12 weeks from treatment | - | Delayed peaks of collagen X expression in patients treated with external fixation or staged open reduction internal fixation |
| [26] | 16 NU pz; 18 and 14 age-matched pz healed within 6 months and 1 month | Long bones | NU: 0% Age-matched pz: 0% | 20–39 | OPG, RANKL, BAP, OC (serum) and deossipirolidine (DPD) (urine) | - | 16 vs. 18–14 matched healed subjects | OPG levels were higher in NU patients compared to CTR No difference in DPD levels in NU vs. healed patients |
| [27] | 49 pz | Radius, humerus. | 82% | 46–76 | Vitamin D3, PTH, BAP, CTx, TRAP5b (serum) | T0, before surgery, and after 1, 4, 8, and 52 weeks | 0 | No difference in BTM levels over time. |
| [28] | 168 pz | Tibia/fibula | 14% | 20–79 (mean: 32) | NTX, BSAP (BAP), P1NP and N-Mid OC (serum) | T0 before surgery, and after 8, 12, 24, and 36 e 72 weeks | 29/168 DU (6 months) 9/168 NU (12 months) | BAP, P1NP and N-Mid OC levels were lower in DU (at 8–12 and 24 weeks) |
| [29] | 15 NU and 15 healed with similar fractures | Femur, tibia, forearm, humerus | NU: 20% Healed: 20% | 20–70 (mean: 46.7 NU) 22–75 (mean: 46.4 healed) | TRACP, P1NP, CTx, BAP (serum) | T0 before surgery, and after 1, 2, 4, 8, 12, 52 weeks | 15 NU vs. 15 healed pz | CTx (1 week) is lower in DU, TRACP is lower after 2–4 weeks BAP and P1NP levels: no significant difference in U and NU |
| [30] | 26 DU or NU pz (3 months diagnosis) 13 ONFH pz | Femur, tibia, fibula, humerus, unknown | DU/NU: 42% ONFH: 8% | DU/NU: 19–65 (mean: 40) ONFH: 21–53 (mean: 42) | BAP, CTx, CICP, N-Mid OC, OPG, RANKL (serum) | T0, before surgery, and 12 and 24 weeks, after surgery. | 1/24 | CICP increase, CTx decrease (good outcome pz) |
| [31] | 20 pz | Tibial shaft fractures treated non-operatively | 5% | 16–61 (mean: 33.7) | CICP, P1NP, BAP (serum) | 1, 4, 8, 14 days and 5, 10, 14, 20 weeks post-fracture | 3/20 DU (20 weeks) | CICP lower in DU vs. U at 20 weeks P1NP higher in DU vs. U at 10 weeks BAP DU vs. U no significant difference |
| [32] | 14 pz | tibial shaft fractures | 36% | 21–70 (mean: 43.7) | CTx, BAP, N-Mid OC (serum) | 1, 7, 17, 28, 42, 60, 90, 180, and 365 days post-fracture | 4/14 DU | BAP higher in DU vs. U at 1, 26, 52 weeks OC increase is delayed (1 month) in DU vs. U (60th vs. 90th day) |
| [33] | 121 pz and 108 hc | Tibia–fibula fractures | Pz: 12% CTR: 14% | 18–45 | OC, osteopontin (mRNA and protein in serum) | 4, 7, 10, 15, 20, 28 days post fracture | 19/121 (DU 24 weeks) | OC higher (protein) higher in U vs. DU at day 20 and 28 Osteopontin no statistical difference among groups |
| [34] | 50 pz | Closed tibial fractures treated non-operatively | 22% | 16–82 (mean: 30.7) | BAP, OC (in 14 patients) (serum) | 0, 2, 4, 6, 8, 10, 12, 14, 16, 18, 20 weeks post fracture | 9/50 DU (20 weeks) | OC lower in DU vs. U (8 and 16 weeks) BAP no significant differences |
| [35] | 95 pz | Tibia–fibula fractures treated non-operatively | - | 18–45 | ALP (serum) | 14, 21, 28, 45, 60, and 90 days post fracture | 18/95 DU (6 months) 8/95 NU (9 months) | BAP is higher for U > DU > NU (no significant difference) |
| BTMs | Findings | Endpoint of Sampling Showing Significant Difference | Reference |
|---|---|---|---|
| BAP | >in early U | 6 weeks | [24] |
| ↑ in U | 12 weeks | [30] | |
| <in DU | 8–12–24 weeks | [28] | |
| >in DU | 1, 26, 52 weeks | [32] | |
| U vs. DU:NS | 5–10–14–20 weeks | [31] | |
| U > DU > NU but NS | 3 weeks | [35] | |
| U vs. DU:NS | 8–16 weeks | [34] | |
| U vs. NU:NS | - | [26] | |
| U vs. NU:NS | 1–2–4–8–12–52 weeks | [29] | |
| OC | <in DU | 8–12–24 weeks | [28] |
| <in DU | 6 weeks | [24] | |
| ↑ in DU delayed vs. U | 60th vs. 90th day | [32] | |
| >in U | 20–28 days (protein by Western blot assay) | [33] | |
| <in DU | 8–16 weeks | [34] | |
| U vs. NU:NS | - | [26] | |
| CICP | ↓ in NU | 24 weeks | [30] |
| <in DU | 6 weeks | [24] | |
| <in DU | 20 weeks | [31] | |
| P1NP | <in DU | 6 weeks | [23] |
| <in DU | 8–12–24 weeks | [28] | |
| >in DU | 10 weeks | [31] | |
| U vs. NU:NS | 1–2–4–8–12–52 weeks | [29] | |
| <in DU | 1 week | [29] | |
| <in DU | 6 weeks | [23] | |
| CTx | ↓ in U | 12, 24 weeks | [30] |
| U vs. NU:NS | 6, 12, 24 weeks | [24] | |
| U vs. NU:NS | 1, 4, 8, 52 weeks | [27] | |
| U vs. NU:NS | 1, 2, 4, 7, 12, 25, 52 weeks | [32] | |
| NTX | U vs. NU:NS | - | [28] |
| TRACP5b | ↓ in DU | 2–4 weeks | [29] |
| U vs. NU:NS | 1, 4, 8, 52 weeks | [27] | |
| OPG | >in NU | - | [26] |
| U vs. NU:NS Delayed peaks in NU ↑ | 12–24 weeks 12 (U) vs. 24 (NU) weeks | [24] [30] | |
| RANKL | NS | [30] | |
| U vs. NU:NS | - | [26] | |
| Collagen X | Delayed peaks with staged open reduction internal fixation | 6–12–24 weeks | [25] |
| Proteomics | < or > for different protein (see text) | - | [22] |
3.4. Analyzed Studies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mock, C.; Cherian, M.N. The Global Burden of Musculoskeletal Injuries: Challenges and Solutions. Clin. Ortho. Rela. Res. 2008, 466, 2306–2316. [Google Scholar] [CrossRef]
- Mills, L.A.; Aitken, S.A.; Simpson, A.H.R.W. The risk of non-union per fracture: Current myths and revised figures from a population of over 4 million adults. Acta Orthop. 2017, 88, 434–439. [Google Scholar] [CrossRef]
- Andrzejowski, P.; Giannoudis, P.V. The ‘diamond concept’ for long bone non-union management. J. Orthop. Traumatol. 2019, 20, 21–34. [Google Scholar] [CrossRef]
- Drug FADAUFA. Guidance Document for Industry and Cdrh Staff for the Preparation of Investigational Device Exemptions and Premarket Approval Applications for Bone Growth Stimulator Devices. 1998. Available online: https://www.federalregister.gov/documents/1998/04/28/98-11158/guidance-document-for-industry-and-cdrh-staff-for-the-preparation-of-investigational-device (accessed on 15 December 2023).
- Wiss, D.A.; Garlich, J.; Hashmi, S.; Neustein, A. Risk Factors for Development of a Recalcitrant Femoral. Nonunion: A Single Surgeon Experience in 122 Patients. J. Orthop. Trauma. 2021, 35, 619–625. [Google Scholar] [CrossRef]
- Negus, O.J.; Watts, D.; Loveday, D.T. Diabetes: A major risk factor in trauma and orthopaedic surgery. Br. J. Hosp. Med. 2021, 82, 1–5. [Google Scholar] [CrossRef]
- Hellwinkel, J.E.; Miclau, T., 3rd; Provencher, M.T.; Bahney, C.S.; Working, Z.M. The Life of a Fracture: Biologic Progression, Healing Gone Awry, and Evaluation of Union. JBJS Rev. 2020, 8, e1900221. [Google Scholar] [CrossRef]
- Odvina, C.V.; Zerwekh, J.E.; Rao, D.S.; Maalouf, N.; Gottschalk, F.A.; Pak, C.Y. Severely suppressed bone turnover: A potential complication of alendronate therapy. J. Clin. Endocrinol. Metab. 2005, 90, 1294–1301. [Google Scholar] [CrossRef]
- Tucker, W.A.; Birt, M.C.; Heddings, A.A.; Horton, G.A. The Effect of Postoperative Nonsteroidal Anti-inflammatory Drugs on Nonunion Rates in Long Bone Fractures. Orthopedics 2020, 43, 221–227. [Google Scholar] [CrossRef]
- Tobiume, H.; Kanzaki, S.; Hida, S.; Ono, T.; Moriwake, T.; Yamauchi, S.; Tanaka, H.; Seino, Y. Serum bone alkaline phosphatase isoenzyme levels in normal children and children with growth hormone (GH) deficiency: A potential marker for bone formation and response to GH therapy. J. Clin. Endocrinol. Metab. 1997, 82, 2056–2061. [Google Scholar] [CrossRef][Green Version]
- Moser, S.C.; van der Eerden, B.C.J. Osteocalcin-A Versatile Bone-Derived Hormone. Front. Endocrinol. 2019, 9, 794. [Google Scholar] [CrossRef]
- Coulibaly, M.O.; Sietsema, D.L.; Burgers, T.A.; Mason, J.; Williams, B.O.; Jones, C.B. Recent advances in the use of serological bone formation markers to monitor callus development and fracture healing. Crit. Rev. Eukaryot. Gene Expr. 2010, 20, 105–127. [Google Scholar] [CrossRef] [PubMed]
- Deveza, L.A.; Kraus, V.B.; Collins, J.E.; Guermazi, A.; Roemer, F.W.; Bowes, M.; Nevitt, M.C.; Ladel, C.; Hunter, D.J. Association Between Biochemical Markers of Bone Turnover and Bone Changes on Imaging: Data from the Osteoarthritis Initiative. Arthritis Care Res. 2017, 69, 1179–1191. [Google Scholar] [CrossRef] [PubMed]
- D’Oronzo, S.; Brown, J.; Coleman, R. The role of biomarkers in the management of bone-homing malignancies. J. Bone Oncol. 2017, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Coghlan, R.F.; Oberdorf, J.A.; Sienko, S.; Aiona, M.D.; Boston, B.A.; Connelly, K.J.; Bahney, C.; LaRouche, J.; Almubarak, S.M.; Coleman, D.T.; et al. A degradation fragment of type X collagen is a real-time marker for bone growth velocity. Sci. Transl. Med. 2017, 9, eaan4669. [Google Scholar] [CrossRef] [PubMed]
- Mödder, U.I.; Hoey, K.A.; Amin, S.; McCready, L.K.; Achenbach, S.J.; Riggs, B.L.; Melton, L.J., 3rd; Khosla, S. Relation of age, gender, and bone mass to circulating sclerostin levels in women and men. J. Bone Miner. Res. 2011, 26, 373–379. [Google Scholar] [CrossRef] [PubMed]
- Starlinger, J.; Santol, J.; Kaiser, G.; Sarahrudi, K. Close negative correlation of local and circulating Dickkopf-1 and Sclerostin levels during human fracture healing. Sci. Rep. 2024, 19, 6524. [Google Scholar] [CrossRef] [PubMed]
- Chubb, S.A. Measurement of C-terminal telopeptide of type I collagen (CTX) in serum. Clin. Biochem. 2012, 45, 928–935. [Google Scholar] [CrossRef]
- Breulmann, F.L.; Hatt, L.P.; Schmitz, B.; Wehrle, E.; Richards, R.G.; Della Bella, E.; Stoddart, M.J. Prognostic and therapeutic potential of microRNAs for fracture healing processes and non-union fractures: A systematic review. Clin. Transl. Med. 2023, 13, e1161. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar] [CrossRef]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields. Edmont. Alta. Herit. Found. Med. Res. 2004, 13, 1–31. [Google Scholar]
- de Seny, D.; Cobraiville, G.; Leprince, P.; Fillet, M.; Collin, C.; Mathieu, M.; Hauzeur, J.P.; Gangji, V.; Malaise, M.G. Biomarkers of inflammation and innate immunity in atrophic nonunion fracture. J. Transl. Med. 2016, 14, 258. [Google Scholar] [CrossRef]
- Stewart, S.K. Fracture Non-Union: A Review of Clinical Challenges and Future Research Needs. Malays. Orthop. J. 2019, 13, 1–10. [Google Scholar] [CrossRef]
- Granchi, D.; Gómez-Barrena, E.; Rojewski, M.; Rosset, P.; Layrolle, P.; Spazzoli, B.; Donati, D.M.; Ciapetti, G. Changes of Bone Turnover Markers in Long Bone Nonunions Treated with a Regenerative Approach. Stem Cells Int. 2017, 2017, 3674045. [Google Scholar] [CrossRef]
- Working, Z.M.; Peterson, D.; Lawson, M.; O’Hara, K.; Coghlan, R.; Provencher, M.T.; Friess, D.M.; Johnstone, B.; Miclau, T., 3rd; Bahney, C.S. Collagen X Longitudinal Fracture Biomarker Suggests Staged Fixation in Tibial Plateau Fractures Delays Rate of Endochondral Repair. J. Orthop. Trauma. 2022, 36, S32–S39. [Google Scholar] [CrossRef]
- Marchelli, D.; Piodi, L.P.; Corradini, C.; Parravicini, L.; Verdoia, C.; Ulivieri, F.M. Increased serum OPG in atrophic nonunion shaft fractures. J. Orthop. Traumatol. 2009, 10, 55–58. [Google Scholar] [CrossRef]
- Wölfl, C.; Schuster, L.; Höner, B.; Englert, S.; Klein, R.; Hirche, C.; Münzberg, M.; Grützner, P.A.; Kneser, U.; Harhaus, L. Influence of extracorporeal shock wave therapy (ESWT) on bone turnover markers in organisms with normal and low bone mineral density during fracture healing: A randomized clinical trial. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2017, 6, Doc17. [Google Scholar] [CrossRef]
- Kumar, M.; Shelke, D.; Shah, S. Prognostic potential of markers of bone turnover in delayed-healing tibial diaphyseal fractures. Eur. J. Trauma. Emerg. Surg. 2019, 45, 31–38. [Google Scholar] [CrossRef]
- Moghaddam, A.; Müller, U.; Roth, H.J.; Wentzensen, A.; Grützner, P.A.; Zimmermann, G. TRACP 5b and CTX as osteological markers of delayed fracture healing. Injury 2011, 42, 758–764. [Google Scholar] [CrossRef]
- Granchi, D.; Ciapetti, G.; Gómez-Barrena, E.; Rojewski, M.; Rosset, P.; Layrolle, P.; Spazzoli, B.; Donati, D.M.; Baldini, N. Biomarkers of bone healing induced by a regenerative approach based on expanded bone marrow-derived mesenchymal stromal cells. Cytotherapy 2019, 21, 870–885. [Google Scholar] [CrossRef]
- Kurdy, N.M. Serology of abnormal fracture healing: The role of PIIINP, PICP, and BsALP. J. Orthop. Trauma. 2000, 14, 48–53. [Google Scholar] [CrossRef]
- Herrmann, M.; Klitscher, D.; Georg, T.; Frank, J.; Marzi, I.; Herrmann, W. Different kinetics of bone markers in normal and delayed fracture healing of long bones. Clin. Chem. 2002, 48, 2263–2266. [Google Scholar]
- Ali, S.; Singh, A.; Yadav, M.; Siddiqui, S.; Pandey, V.; Mahdi, A.A.; Srivastava, R.N. Can impaired diaphyseal fracture healing be predicted early?: A cohort study of biomarkers. J. Clin. Orthop. Trauma. 2019, 10, S37–S46. [Google Scholar] [CrossRef]
- Oni, O.O.; Mahabir, J.P.; Iqbal, S.J.; Gregg, P.J. Serum osteocalcin and total alkaline phosphatase levels as prognostic indicators in tibial shaft fractures. Injury 1989, 20, 37–38. [Google Scholar] [CrossRef]
- Singh, A.; Ali, S.; Mahdi, A.A.; Srivastava, R.N. Evaluation of serum alkaline phosphatase as a biomarker of healing process progression of simple diaphyseal fractures in adult patients. Int. Res. J. Biol. Sci. 2013, 2, 40–43. [Google Scholar]
- Golub, E.E.; Boesze-Battaglia, K. The role of alkaline phosphatase in mineralization. Curr. Opin. Orthop. 2007, 18, 444–448. [Google Scholar] [CrossRef]
- Brown, J.P.; Albert, C.; Nassar, B.A.; Adachi, J.D.; Cole, D.; Davison, K.S.; Dooley, K.C.; Don-Wauchope, A.; Douville, P.; Hanley, D.A. Bone turnover markers in the management of postmenopausal osteoporosis. Clin. Biochem. 2009, 42, 929–942. [Google Scholar] [CrossRef]
- Takahashi, M.; Kushida, K.; Nagano, A.; Inoue, T. Comparison of the analytical and clinical performance characteristics of an N-MID versus an intact osteocalcin immunoradiometric assay. Clin. Chim. Acta 2000, 294, 67–76. [Google Scholar] [CrossRef]
- Halleen, J.M.; Tiitinen, S.L.; Ylipahkala, H.; Fagerlund, K.M.; Väänänen, H.K. Tartrate-resistant acid phosphatase 5b (TRACP 5b) as a marker of bone resorption. Clin. Lab. 2006, 52, 499–509. [Google Scholar]
- Takegahara, N.; Kim, H.; Choi, Y. RANKL biology. Bone 2022, 159, 116353. [Google Scholar] [CrossRef]
- Kanis, J.A.; Norton, N.; Harvey, N.C.; Jacobson, T.; Johansson, H.; Lorentzon, M. SCOPE 2021: A new scorecard for osteoporosis in Europe. Arch. Osteoporos. 2021, 16, 82. [Google Scholar] [CrossRef]
- Eastell, R.; Szulc, P. Use of bone turnover markers in postmenopausal osteoporosis. Lancet Diabetes Endocrinol. 2017, 5, 908–923. [Google Scholar] [CrossRef]
- Ashcherkin, N.; Patel, A.A.; Algeciras-Schimnich, A.; Doshi, K.B. Bone turnover markers to monitor oral bisphosphonate therapy. Cleve Clin. J. Med. 2023, 90, 26–31. [Google Scholar] [CrossRef]
- Mattia, L.; Gossiel, F.; Walsh, J.S.; Eastell, R. Effect of age and gender on serum growth differentiation factor 15 and its relationship to bone density and bone turnover. Bone Rep. 2023, 18, 101676. [Google Scholar] [CrossRef]
- Oh, E.S.; Rhee, E.; Oh, K.W.; Lee, W.Y.; Baek, K.H.; Yoon, K.H.; Kang, M.I.; Yun, E.J.; Park, C.Y.; Choi, M.G.; et al. Circulating osteoprotegerin levels are associated with age, waist-to-hip ratio, serum total cholesterol, and low-density lipoprotein cholesterol levels in healthy Korean women. Metabolism 2005, 54, 49–54. [Google Scholar] [CrossRef]
- Schini, M.; Vilaca, T.; Gossiel, F.; Salam, S.; Eastell, R. Bone Turnover Markers: Basic Biology to Clinical Applications. Endocr. Rev. 2023, 44, 417–473. [Google Scholar] [CrossRef]
- Siderius, M.; Arends, S.; Kobold, A.M.; Wagenmakers, L.; Koerts, K.; Spoorenberg, A.; van der Veer, E. Serum levels of bone turnover markers including calculation of Z-scores: Data from a Dutch healthy reference cohort. Bone Rep. 2023, 19, 101724. [Google Scholar] [CrossRef]
- Diemar, S.S.; Dahl, S.S.; West, A.S.; Simonsen, S.A.; Iversen, H.K.; Jørgensen, N.R. A Systematic Review of the Circadian Rhythm of Bone Markers in Blood. Calcif. Tissue Int. 2023, 112, 126–147. [Google Scholar] [CrossRef]
- Chitwood, J.R.; Chakraborty, N.; Hammamieh, R.; Moe, S.M.; Chen, N.X.; Kacena, M.A.; Natoli, R.M. Predicting fracture healing with blood biomarkers: The potential to assess patient risk of fracture nonunion. Biomarkers 2021, 26, 703–717. [Google Scholar] [CrossRef]
- Szulc, P.; Naylor, K.; Hoyle, N.R.; Eastell, R.; Leary, E.T. Use of CTX-I and PINP as bone turnover markers: National Bone Health Alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Osteoporos. Int. 2017, 28, 2541–2556. [Google Scholar] [CrossRef]
- Christensen, G.L.; Halgreen, J.R.; Milenkovski, M.; Köse, A.; Quardon, N.; Jørgensen, N.R. Bone turnover markers are differentially affected by pre-analytical handling. Osteoporos. Int. 2019, 30, 1137–1141. [Google Scholar] [CrossRef]


| Reference | Country of Publication | Aim of the Study | Design of the Study | Qualitative Score * |
|---|---|---|---|---|
| [22] | Belgium | Comparison between BTM levels’ (non-union vs. healthy subjects) | Observational | 84% |
| [23] | USA | Evaluation of BTM levels’ changes over time | RCT (patients treated with or without vitamin D) | 89% |
| [24] | Multi-center (Italy, Germany, France, Spain) | Evaluation of BTM levels’ changes over time | Prospective, controlled | 89% |
| [25] | USA | Evaluation of Collagen X levels’ changes over time | Prospective longitudinal study | 74% |
| [26] | Italy | Comparison between BTM levels’ (fractured vs. healed subjects) | Observational study | 80% |
| [27] | Germany | Evaluation of BTM levels’ changes over time | RCT and prospective longitudinal study for BTMs evaluation | 69% |
| [28] | India | Evaluation of BTM levels’ changes over time | Prospective observational study—Level of evidence 2 | 83% |
| [29] | Germany | Evaluation of BTM levels’ changes over time | Prospective open control study | 93% |
| [30] | Multi-center (Italy, Germany, France, Spain) | Evaluation of BTM levels’ changes over time | Prospective, controlled, phase 2 trial (treatment with culture-expanded MSC) | 92.5% |
| [31] | United Kingdom | Evaluation of BTM levels’ changes over time | Prospective observational study | 92.5% |
| [32] | Germany | Evaluation of BTM levels’ changes over time | Prospective observational study | 92.5% |
| [33] | India | Evaluation of BTM levels’ changes over time | Prospective observational study | 93% |
| [34] | United Kingdom | Evaluation of BTM levels’ changes over time | Prospective observational study | 62% |
| [35] | India | Evaluation of BTM levels’ changes over time | Prospective observational study | 60% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perut, F.; Roncuzzi, L.; Gómez-Barrena, E.; Baldini, N. Association between Bone Turnover Markers and Fracture Healing in Long Bone Non-Union: A Systematic Review. J. Clin. Med. 2024, 13, 2333. https://doi.org/10.3390/jcm13082333
Perut F, Roncuzzi L, Gómez-Barrena E, Baldini N. Association between Bone Turnover Markers and Fracture Healing in Long Bone Non-Union: A Systematic Review. Journal of Clinical Medicine. 2024; 13(8):2333. https://doi.org/10.3390/jcm13082333
Chicago/Turabian StylePerut, Francesca, Laura Roncuzzi, Enrique Gómez-Barrena, and Nicola Baldini. 2024. "Association between Bone Turnover Markers and Fracture Healing in Long Bone Non-Union: A Systematic Review" Journal of Clinical Medicine 13, no. 8: 2333. https://doi.org/10.3390/jcm13082333
APA StylePerut, F., Roncuzzi, L., Gómez-Barrena, E., & Baldini, N. (2024). Association between Bone Turnover Markers and Fracture Healing in Long Bone Non-Union: A Systematic Review. Journal of Clinical Medicine, 13(8), 2333. https://doi.org/10.3390/jcm13082333