
Aortic Stenosis: Time for a Sex-Based Approach?

 , , , , ,
, , , , , {kind=link}
Abstract
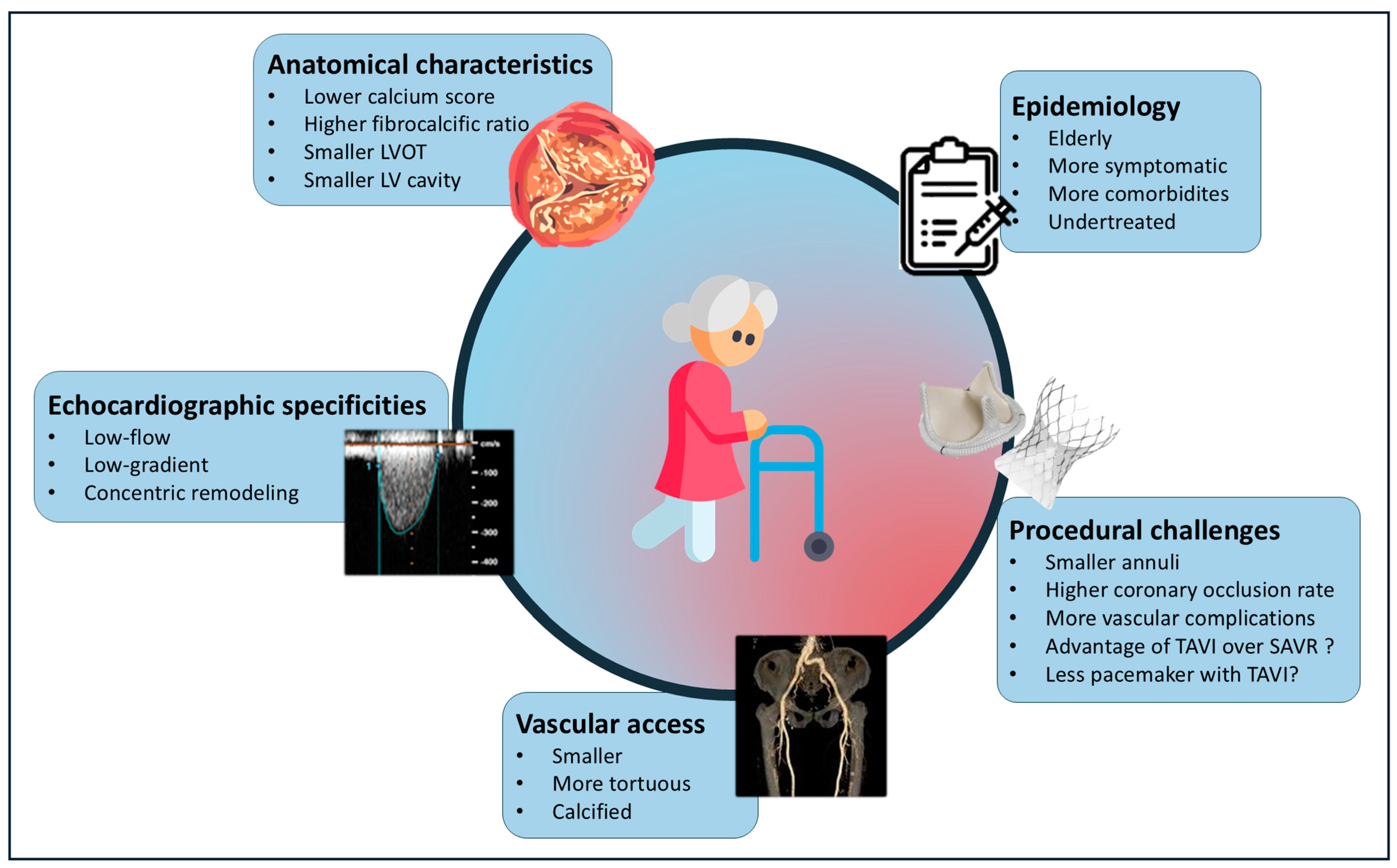
1. Epidemiology of Aortic Stenosis in Women
2. Aortic Stenosis Pathophysiology and Diagnosis
2.1. Anatomical Differences
2.2. Specificities of Echocardiographic Assessment in Women
2.3. Left Ventricular Response and Myocardial Fibrosis
2.4. Valve Calcification and Fibrosis
2.5. Disease Progression
2.6. Potential Mechanisms Underlying Sex Differences
3. Treatment
3.1. Do Women Have Equal Access to Treatment?
3.2. Management of AS in Women: More Advantages for TAVI?
3.3. TAVI and the Challenge of Female-Specific Anatomical Characteristics
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DesJardin, J.T.; Chikwe, J.; Hahn, R.; Hung, J.; Delling, F. Sex differences and similarities in valvular heat disease. Circ. Res. 2022, 130, 455–473. [Google Scholar] [CrossRef]
- Mascherbauer, J.; Kammerlander, A.; Nitsche, C.; Bax, J.; Delgado, V.; Evangelista, A.; Laroche, C.; Maggioni, A.P.; Magne, J.; Vahanian, A.; et al. Sex-related differences in severe native valvular heart disease: The ESC-EORP Valvular Heart Disease II survey. Eur. Heart J. 2024, 45, 3818–3833. [Google Scholar] [CrossRef] [PubMed]
- Généreux, P.; Sharma, R.P.; Cubeddu, R.J.; Aaron, L.; Abdelfattah, O.M.; Koulogiannis, K.P.; Marcoff, L.; Naguib, M.; Kapadia, S.R.; Makkar, R.R.; et al. The Mortality Burden of Untreated Aortic Stenosis. J. Am. Coll. Cardiol. 2023, 82, 2101–2109. [Google Scholar] [CrossRef] [PubMed]
- Tribouilloy, C.; Bohbot, Y.; Rusinaru, D.; Belkhir, K.; Diouf, M.; Altes, A.; Delpierre, Q.; Serbout, S.; Kubala, M.; Levy, F.; et al. Excess Mortality and Undertreatment of Women with Severe Aortic Stenosis. J. Am. Heart Assoc. 2021, 10, e018816. [Google Scholar] [CrossRef]
- Williams, M.; Kodali, S.K.; Hahn, R.T.; Humphries, K.H.; Nkomo, V.T.; Cohen, D.J.; Douglas, P.S.; Mack, M.; McAndrew, T.C.; Svensson, L.; et al. Sex-Related Differences in Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Patients with Severe Aortic Stenosis: Insights from the PARTNER Trial. J. Am. Coll. Cardiol. 2014, 63, 1522–1528. [Google Scholar] [CrossRef] [PubMed]
- González-Mansilla, A.; Martinez-Legazpi, P.; Prieto, A.; Gomá, E.; Haurigot, P.; del Villar, C.P.; Cuadrado, V.; Delgado-Montero, A.; Prieto, R.; Mombiela, T.; et al. Valve area and the risk of overestimating aortic stenosis. Heart 2019, 105, 911–919. [Google Scholar] [CrossRef]
- Leye, M.; Brochet, E.; Lepage, L.; Cueff, C.; Boutron, I.; Detaint, D.; Hyafil, F.; Iung, B.; Vahanian, A.; Messika-Zeitoun, D. Size-adjusted left ventricular outflow tract diameter reference values: A safeguard for the evaluation of the severity of aortic stenosis. J. Am. Soc. Echocardiogr. 2009, 22, 445–451. [Google Scholar] [CrossRef]
- Bahlmann, E.; Cramariuc, D.; Minners, J.; Lønnebakken, M.T.; Ray, S.; Gohlke-Baerwolf, C.; Nienaber, C.A.; Jander, N.; Seifert, R.; Chambers, J.B.; et al. Small aortic root in aortic valve stenosis: Clinical characteristics and prognostic implications. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 404–412. [Google Scholar] [CrossRef]
- Wagener, M.; Reuthebuch, O.; Heg, D.; Tüller, D.; Ferrari, E. Low-Gradient, and paradoxical Low-Flow, Low-Gradient Aortic Stenosis After Transcatheter Aortic Valve Implantation: A report from The SwissTAVI Registry. J. Am. Heart Assoc. 2023, 12, e029489. [Google Scholar] [CrossRef]
- Sen, J.; Huynh, Q.; Stub, D.; Neil, C.; Marwick, T.H. Prognosis of severe low-flow, low-gradient aortic stenosis by stroke volume index and transvalvular flow rate. Cardiovasc. Imaging 2021, 14, 915–927. [Google Scholar] [CrossRef]
- Wheatley, C.M.; Snyder, E.M.; Johnson, B.D.; Olson, T.P. Sex differences in cardiovascular function during submaximal exercise in humans. Springerplus 2014, 3, 445. [Google Scholar] [CrossRef]
- Guzzetti, E.; Poulin, A.; Annabi, M.S.; Zhang, B.; Kalavrouziotis, D.; Couture, C.; Dagenais, F.; Pibarot, P.; Clavel, M.A. Transvalvular flow, sex, and survival after valve replacement surgery in patients with severe aortic stenosis. J. Am. Coll. Cardiol. 2020, 75, 1897–1909. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Garcia, D.; Dumesnil, J.G. Energy loss index in aortic stenosis;from fluid mechanics concept to clinical application. Circulation 2013, 127, 1101–1104. [Google Scholar] [CrossRef]
- Garcia, D.; Pibarot, P.; Dumesnil, J.; Sakr, F.; Durand, L.-G. Assessment of Aortic Valve Stenosis Severity: A new Index Based on the Energy Loss Concept. Circulation 2000, 101, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Bahlmann, E.; Cramariuc, D.; Gerdts, E.; Gohlke-Baerwolf, C.; Nienaber, C.A.; Eriksen, E.; Wachtell, K.; Chambers, J.; Kuck, K.H.; Ray, S. Impact of pressure recovery on echocardiographic assessment of asymptomatic aortic stenosis: A SEAS substudy. JACC Cardiovasc. Imaging 2010, 3, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Bahlmann, E.; Gerdts, E.; Cramariuc, D.; Gohlke-Baerwolf, C.; Nienaber, C.A.; Wachtell, K.; Seifert, R.; Chambers, J.B.; Kuck, K.H.; Ray, S. Prognostic value of energy loss index in asymptomatic aortic stenosis. Circulation 2013, 127, 1149–1156. [Google Scholar] [CrossRef]
- Ullah, W.; Sana, M.K.; Mukhtar, M.; Syed, S.H.; Zahid, S.; Alkhouli, M.; Vishnevsky, A. Transcatheter Aortic Valve Replacement Across Hemodynamic Subtypes of Severe Aortic Valve Stenosis: A Network Meta-analysis. J. Soc. Cardiovasc. Angiogr. Interv. 2024, 3, 101255. [Google Scholar] [CrossRef]
- Webb, J.; Offen, S. Low-flow, low-gradient aortic stenosis: An understanding is still a long way off. EuroIntervention 2024, 20, 1364–1365. [Google Scholar] [CrossRef]
- Barletta, G.; Del Bene, M.; Venditti, F.; Pilato, G.; Stefano, P. Surgical aortic valve replacement and left ventricular remodeling: Survival and sex-related differences. Echocardiography 2021, 38, 1095–1103. [Google Scholar] [CrossRef]
- Kuneman, J.H.; Singh, G.K.; Pio, S.M.; Hirasawa, K.; Hautemann, D.; van der Kley, F.; Marsan, N.A.; Knuuti, J.; Delgado, V.; Bax, J.J. Sex differences in left ventricular remodelling in patients with severe aortic valve stenosis. Eur. Heart J. Cardiovasc. Imaging 2022, 23, 781–789. [Google Scholar] [CrossRef]
- Tastet, L.; Kwiecinski, J.; Pibarot, P.; Capoulade, R.; Everett, R.J.; Newby, D.E.; Shen, M.; Guzzetti, E.; Arsenault, M.; Bédard, É.; et al. Sex-Related Differences in the Extent of Myocardial Fibrosis in Patients with Aortic Valve Stenosis. JACC Cardiovasc. Imaging 2020, 13, 699–711. [Google Scholar] [CrossRef] [PubMed]
- Kwak, S.; Singh, A.; Everett, R.J.; Treibel, T.A.; Lim, J.; Won, S.; Williams, M.C.; Loganathan, K.; Bing, R.; Craig, N.; et al. Sex-Specific Association of Myocardial Fibrosis with Mortality in Patients with Aortic Stenosis. JAMA 2024, e245593. [Google Scholar] [CrossRef]
- Rosenhek, R.; Binder, T.; Porenta, G.; Lang, I.; Christ, G.; Schemper, M.; Maurer, G.; Baumgartner, H. Predictors of outcome in severe, asymptomatic aortic stenosis. N. Engl. J. Med. 2000, 343, 611–617. [Google Scholar] [CrossRef] [PubMed]
- Pawade, T.; Clavel, M.-A.; Tribouilloy, C.; Dreyfus, J.; Mathieu, T.; Tastet, L.; Renard, C.; Gun, M.; Jenkins, W.S.A.; Macron, L.; et al. Computed tomography aortic valve calcium scoring in patients with aortic stenosis. Circ. Cardiovasc. Imaging 2018, 11, e007146. [Google Scholar] [CrossRef]
- Powers, A.; Ali, M.; Lavoie, N.; Haujir, A.; Mogensen, N. Aortic Valve Calcification Density Measured by MDCT in the Assessment of Aortic Stenosis Severity. Circ. Cardiovasc. Imaging 2024, 5, e016267. [Google Scholar] [CrossRef]
- Simard, L.; Cote, N.; Dagenais, F.; Mathieu, P.; Couture, C.; Trahan, S.; Bosse, Y.; Mohammadi, S.; Page, S.; Joubert, P.; et al. Sex-related discordance between aortic valve calcification and hemodynamic severity of aortic stenosis: Is valvular fibrosis the explanation? Circ. Res. 2017, 120, 681–691. [Google Scholar] [CrossRef]
- Cartlidge, T.R.; Bing, R.; Kwiecinski, J.; Guzzetti, E.; Pawade, T.A.; Doris, M.K.; Adamson, P.D.; Massera, D.; Lembo, M.; Peeters, F.E.C.M.; et al. Contrast-Enhanced Computed Tomography Assessment of Aortic Stenosis. Heart 2021, 107, 1905–1911. [Google Scholar] [CrossRef] [PubMed]
- Lembo, M.; Joshi, S.S.; Geers, J.; Bing, R.; Carnevale, L.; Pawade, T.A.; Doris, M.K.; Tzolos, E.; Grodecki, K.; Cadet, S.; et al. Quantitative Computed Tomography Angiography for the Evaluation of Valvular Fibrocalcific Volume in Aortic Stenosis. JACC Cardiovasc. Imaging 2024, 11, 1351–1362. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.; Mathieu, T.; Melissopoulou, M.; Cimadevilla, C.; Codogno, I.; Huart, V.; Duval, X.; Vahanian, A.; Messika-Zeitoun, D. Sex Differences in the Progression of Aortic Stenosis and Prognostic Implication: The COFRASA-GENERAC Study. JACC Cardiovasc. Imaging 2016, 4, 499–501. [Google Scholar] [CrossRef]
- Cramariuc, D.; Rogge, B.P.; Lønnebakken, M.T.; Boman, K.; Bahlmann, E.; Gohlke-Bärwolf, C.; Chambers, J.B.; Pedersen, T.R.; Gerdts, E. Sex differences in cardiovascular outcome during progression of aortic valve stenosis. Heart 2015, 101, 209–214. [Google Scholar] [CrossRef]
- Woodward, H.; Zhu, D.; Hadoke, P.; MacRae, V. Regulatory Role of Sex Hormones in Cardiovascular Calcification. Int. J. Mol. Sci. 2021, 22, 4620. [Google Scholar] [CrossRef] [PubMed]
- Eildermann, K.; Goldmann, S.; Krause, U.; Backhoff, D.; Schöndube, F. Differences in Androngen Receptor Expression in Human Heart Tissue in Various Types of Cardiomyopathy and in Aortic Valve Stenosis. J. Cardiovasc. Dev. Dis. 2023, 10, 466. [Google Scholar] [PubMed]
- Le Nezet, E.; Marqueze-Pouey, C.; Guisle, I.; Clavel, M.-A. Molecular Feature of Calcific Aortic Stenosis in Female and Male Patients. CJC Open 2024, 6, 1125–1137. [Google Scholar] [CrossRef] [PubMed]
- Abdoun, K.; Tastet, L.; Bedard, E.; Arsenault, M.; Pibarot, P.; Clavel, M.-A. Effect of Early Menopause and Hormone Replacement Therapy on Aortic Stenosis Progression. Can. J. Cardiol. 2025, S0828-282X. [Google Scholar] [CrossRef]
- Sharma, A.; Ogunmoroti, O.; Fashanu, O.E.; Zhao, D.; Ouyang, P.; Budoff, M.J.; Thomas, I.C.; Michos, E.D. Associations of endogenous sex hormone levels with the prevalence and progression of valvular and thoracic aortic calcification in the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2022, 341, 71–79. [Google Scholar] [CrossRef]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease: Developed by the Task Force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2022, 43, 561–632. [Google Scholar] [CrossRef]
- Bienjonetti-Boudreau, D.; Fleury, M.-A.; Voisine, M.; Paquin, A.; Chouinard, I.; Tailleur, M.; Duval, R.; Magnan, P.-O.; Beaudoin, J.; Salaun, E.; et al. Impact of sex on the management and outcome of aortic stenosis patients. Eur. Heart J. 2021, 27, 2683–2691. [Google Scholar] [CrossRef]
- Nakase, M.; Tomii, D.; Maznyczka, A.; Samim, D.; Lanz, J.; Praz, F.; Stortecky, S.; Reineke, D.; Windecker, S.; Pilgrim, T. Sex-Specific Difference in Upstream Cardiac Damage in Patients with Aortic Stenosis Undergoing TAVR. JACC Cardiovasc. Interv. 2024, 10, 1252–1265. [Google Scholar] [CrossRef]
- Hartzell, M.; Malhotra, R.; Yared, K.; Rosenfield, H.R.; Walker, J.D.; Wood, M.J. Effect of Gender on Treatment and Outcomes in Severe Aortic Stenosis. Am. J. Cardiol. 2011, 107, 1681–1686. [Google Scholar] [CrossRef]
- Freed, B.H.; Sugeng, L.; Furlong, K.; Mor-Avi, V.; Raman, J.; Jeevanandam, V.; Lang, R.M. Reasons for Nonadherence to Guidelines for Aortic Valve Replacement in Patients with Severe Aortic Stenosis and Potential Solutions. Am. J. Cardiol. 2010, 105, 1339–1342. [Google Scholar] [CrossRef]
- Chaker, Z.; Badhwar, V.; Alqahtani, F.; Aljohani, S.; Zack, C.J.; Holmes, D.R.; Rihal, C.S.; Alkhouli, M. Sex Differences in the Utilization and Outcomes of Surgical Aortic Valve Replacement for Severe Aortic Stenosis. J. Am. Heart Assoc. 2017, 6, e006370. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.M.; O’Brien, S.M.; Wu, C.; Sikora, J.A.H.; Griffith, B.P.; Gammie, J.S. Isolated aortic valve replacement in North America comprising 108,687 patients in 10 years: Changes in risks, valve types, and outcomes in the Society of Thoracic Surgeons National Database. J. Thorac. Cardiovasc. Surg. 2009, 137, 82–90. [Google Scholar] [CrossRef]
- Eleid, M.F.; Sorajja, P.; Michelena, H.I.; Malouf, J.F.; Scott, C.G.; Pellikka, P.A. Flow-Gradient Patterns in Severe Aortic Stenosis with Preserved Ejection Fraction: Clinical Characteristics and Predictors of Survival. Circulation 2013, 128, 1781–1789. [Google Scholar] [CrossRef]
- Skelding, K.A.; Yakubov, S.J.; Kleiman, N.S.; Reardon, M.J.; Adams, D.H.; Huang, J.; Forrest, J.K.; Popma, J.J. Transcatheter Aortic Valve Replacement Versus Surgery in Women at High Risk for Surgical Aortic Valve Replacement (from the CoreValve US High Risk Pivotal Trial). Am. J. Cardiol. 2016, 118, 560–566. [Google Scholar] [CrossRef]
- Chandrasekhar, J.; Dangas, G.; Yu, J.; Vemulapalli, S.; Suchindran, S.; Vora, A.N.; Baber, U.; Mehran, R. Sex-Based Differences in Outcomes with Transcatheter Aortic Valve Therapy. J. Am. Coll. Cardiol. 2016, 68, 2733–2744. [Google Scholar] [CrossRef]
- Saad, M.; Nairooz, R.; Pothineni, N.V.K.; Almomani, A.; Kovelamudi, S.; Sardar, P.; Katz, M.; Abdel-Wahab, M.; Bangalore, S.; Kleiman, N.S.; et al. Long-Term Outcomes with Transcatheter Aortic Valve Replacement in Women Compared with Men. JACC Cardiovasc. Interv. 2018, 11, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Tchetche, D.; Pibarot, P.; Bax, J.J.; Bonaros, N.; Windecker, S.; Dumonteil, N.; Nietlispach, F.; Messika-Zeitoun, D.; Pocock, S.J.; Berthoumieu, P.; et al. Transcatheter vs. surgical aortic valve replacement in women: The RHEIA trial. Eur. Heart J. 2025, 2, ehaf133. [Google Scholar] [CrossRef] [PubMed]
- Tchetche, D. Transcatheter vs. surgical aortic valve replacement in women: A pooled analysis of the Rheia and PARTNER 3 trials. In Proceedings of the TCT 2024, Washington, DC, USA, 29 October 2024. [Google Scholar]
- Shan, Y.; Pellikka, P.A. Aortic stenosis in women. Heart 2020, 106, 970–976. [Google Scholar] [CrossRef]
- Akinseye, O.A.; Jha, S.K.; Ibebuogu, U.N. Clinical outcomes of coronary occlusion following transcatheter aortic valve replacement: A systematic review. Cardiovasc. Revasc. Med. 2018, 19, 229–236. [Google Scholar] [CrossRef]
- Freitas-Ferraz, A.B.; Tirado-Conte, G.; Dagenais, F.; Ruel, M.; Al-Atassi, T.; Dumont, E.; Mohammadi, S.; Bernier, M.; Pibarot, P.; Rodés-Cabau, J. Aortic Stenosis and Small Aortic Annulus. Circulation 2019, 139, 2685–2702. [Google Scholar] [CrossRef]
- O’connor, S.A.; Morice, M.-C.; Gilard, M.; Leon, M.B.; Webb, J.G.; Dvir, D.; Rodés-Cabau, J.; Tamburino, C.; Capodanno, D.; D’ascenzo, F.; et al. Revisiting Sex Equality with Transcatheter Aortic Valve Replacement Outcomes. J. Am. Coll. Cardiol. 2015, 66, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Rodés-Cabau, J.; Ribeiro, H.B.; Mohammadi, S.; Serra, V.; Al-Atassi, T.; Iñiguez, A.; Vilalta, V.; Nombela-Franco, L.; de Ibarra Sánchez, J.I.S.; Auffret, V.; et al. Transcatheter or surgical aortic valve replacement in patients with severe aortic stenosis and small aortic annulus. Circulation 2024, 149, 644–655. [Google Scholar] [CrossRef]
- Sà, M.; Jacquemyn, X.; Van den Eynde, J.; Chu, D.; Serna-Gallegos, D.; Ebels, T.; Clavel, M.-A.; Pibarot, P.; Sultan, I. Impact of Prosthesis-Patient Mismatch After Surgical Aortic Valve Replacement: Systematic Review and Meta-Analysis of Reconstructed Time-to-Event Data of 122 989 Patients with 592 952 Patient-Years. Am. Heart Assoc. 2024, 13, e033176. [Google Scholar] [CrossRef]
- Dahou, A.; Mahoub, H.; Pibarot, P. Prothesis-Patient Mismatch after Aortic Valve Replacement. J. Am. Coll. Cardiol. Imaging 2016, 9, 924–933. [Google Scholar]
- Herrmann, H.C.; Mehran, R.; Blackman, D.J.; Bailey, S.; Möllmann, H.; Abdel-Wahab, M.; Ben Ali, W.; Mahoney, P.D.; Ruge, H.; Wood, D.A.; et al. Self-expanding or balloon-expandable TAVR in patients with a small aortic annulus. N. Engl. J. Med. 2024, 390, 1959–1971. [Google Scholar] [CrossRef] [PubMed]
- Tchétché, D.; Mehran, R.; Blackman, D.J.; Khalil, R.F.; Möllmann, H.; Abdel-Wahab, M.; Ali, W.B.; Mahoney, P.D.; Ruge, H.; Bleiziffer, S.; et al. Transcatheter Aortic Valve Implantation by Valve Type in Women with Small Annuli: Results From the SMART Randomized Clinical Trial. JAMA Cardiol. 2024, 9, 1106. [Google Scholar] [CrossRef]
- Ferrante, G.; Pagnotta, P.; Petronio, A.S.; Bedogni, F.; Brambilla, N.; Fiorina, C.; Giannini, C.; Mennuni, M.; De Marco, F.; Klugmann, S.; et al. Sex differences in postprocedural aortic regurgitation and mid-term mortality after transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2014, 84, 264–271. [Google Scholar] [CrossRef] [PubMed]
- Vlastra, W.; Chandrasekhar, J.; García Del Blanco, B.; Tchétché, D.; De Brito, F.S.; Barbanti, M.; Kornowski, R.; Latib, A.; D’Onofrio, A.; Ribichini, F.; et al. Sex Differences in Transfemoral Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2019, 74, 2758–2767. [Google Scholar] [CrossRef]
- Sherwook, M.; Xiang, K.; Matsouaka, R.; Li, Z.; Vemulapalli, S. Incidence, temporal trends, and associated outcomes of vascular and bleeding complications in patients undergoing transfemoral transcatheter aortic valve replacement: Insights from the society of thoracic surgeons/American college of cardiology transcatheter valve therapies Registry. Circ. Cardiovasc. Interv. 2020, 13, e008227. [Google Scholar]
- Naoum, C.; Blanke, P.; Dvir, D.; Pibarot, P.; Humphries, K.; Webb, J.; Leipsic, J. Clinical Outcomes and Imaging Findings in Women Undergoing TAVR. JACC Cardiovasc. Imaging 2016, 9, 483–493. [Google Scholar] [CrossRef]
- Ravaux, J.M.; Di Mauro, M.; Vernooy, K.; Hof, A.W.V.; Veenstra, L.; Kats, S.; Maessen, J.G.; Lorusso, R. Do Women Require Less Permanent Pacemaker After Transcatheter Aortic Valve Implantation? A Meta-Analysis and Meta-Regression. J. Am. Heart Assoc. 2021, 10, e019429. [Google Scholar] [CrossRef] [PubMed]
- Pibarot, P.; Ternacle, J.; Jaber, W.; Salaun, E.; Dahou, A. Structural deterioration of transcatheter versus surgical aortic valve bioprotheses in the PARTNER 2 trial. J. Am. Coll. Cardiol. 2020, 76, 1830–1843. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zimmerli, A.; Liabot, Q.; Tzimas, G.; Akodad, M.; Salihu, A.; Weerts, V.; Antiochos, P.; Sellers, S.L.; Monney, P.; Muller, O.; et al. Aortic Stenosis: Time for a Sex-Based Approach? J. Clin. Med. 2025, 14, 2691. https://doi.org/10.3390/jcm14082691
Zimmerli A, Liabot Q, Tzimas G, Akodad M, Salihu A, Weerts V, Antiochos P, Sellers SL, Monney P, Muller O, et al. Aortic Stenosis: Time for a Sex-Based Approach? Journal of Clinical Medicine. 2025; 14(8):2691. https://doi.org/10.3390/jcm14082691
Chicago/Turabian StyleZimmerli, Aurelia, Quentin Liabot, Georgios Tzimas, Mariama Akodad, Adil Salihu, Victor Weerts, Panagiotis Antiochos, Stephanie L. Sellers, Pierre Monney, Olivier Muller, and et al. 2025. "Aortic Stenosis: Time for a Sex-Based Approach?" Journal of Clinical Medicine 14, no. 8: 2691. https://doi.org/10.3390/jcm14082691
APA StyleZimmerli, A., Liabot, Q., Tzimas, G., Akodad, M., Salihu, A., Weerts, V., Antiochos, P., Sellers, S. L., Monney, P., Muller, O., Fournier, S., & Meier, D. (2025). Aortic Stenosis: Time for a Sex-Based Approach? Journal of Clinical Medicine, 14(8), 2691. https://doi.org/10.3390/jcm14082691