
Understanding Cybersickness and Presence in Seated VR: A Foundation for Exploring Therapeutic Applications of Immersive Virtual Environments

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sherman, W.R. Understanding Virtual Reality: Interface, Application, and Design; Morgan Kaufmann Publishers: Amsterdam, The Netherlands; Boston, MA, USA, 2003; ISBN 978-1-55860-353-0. [Google Scholar]
- Carvalho, B.; Soares, M.; Neves, A.; Soares, G.; Lima, A. Virtual Reality Devices Applied to Digital Games: A Literature Review. In Ergonomics in Design: Methods and Techniques (Human Factors and Ergonomics); CRC Press: Boca Raton, FL, USA, 2016; pp. 125–140. ISBN 978-1-4987-6071-3. [Google Scholar]
- National Research Council. Virtual Reality: Scientific and Technological Challenges; National Academy Press: Washington, DC, USA, 1995; ISBN 9780585023021. [Google Scholar] [CrossRef]
- Stone, R. Virtual Reality for Interactive Training: An Industrial Practitioner’s Viewpoint. Int. J. Hum. Comput. Stud. 2001, 55, 699–711. [Google Scholar] [CrossRef]
- Sevilla, G. Meta Captures 90% of VR Headset Market Share. Available online: https://www.emarketer.com/content/meta-captures-90-of-vr-headset-market-share (accessed on 15 March 2025).
- Ryan, M.-L. Immersion vs. Interactivity: Virtual Reality and Literary Theory. SubStance 1999, 28, 110–137. [Google Scholar] [CrossRef]
- Slater, M. Place Illusion and Plausibility Can Lead to Realistic Behaviour in Immersive Virtual Environments. Philos. Trans. R. Soc. B Biol. Sci. 2009, 364, 3549–3557. [Google Scholar] [CrossRef] [PubMed]
- Bowman, D.A.; McMahan, R.P. Virtual Reality: How Much Immersion Is Enough? Computer 2007, 40, 36–43. [Google Scholar] [CrossRef]
- Jastrzębski, D.; Żebrowska, A.; Rutkowski, S.; Rutkowska, A.; Warzecha, J.; Ziaja, B.; Pałka, A.; Czyżewska, B.; Czyżewski, D.; Ziora, D. Pulmonary Rehabilitation with a Stabilometric Platform after Thoracic Surgery: A Preliminary Report. J. Hum. Kinet. 2018, 65, 79–87. [Google Scholar] [CrossRef]
- Cieślik, B.; Mazurek, J.; Wrzeciono, A.; Maistrello, L.; Szczepańska-Gieracha, J.; Conte, P.; Kiper, P. Examining Technology-Assisted Rehabilitation for Older Adults’ Functional Mobility: A Network Meta-Analysis on Efficacy and Acceptability. NPJ Digit. Med. 2023, 6, 159. [Google Scholar] [CrossRef]
- Hibbard, P.B. Virtual Reality for Vision Science. Curr. Top. Behav. Neurosci. 2023, 65, 131–159. [Google Scholar] [CrossRef]
- Loetscher, T.; Barrett, A.M.; Billinghurst, M.; Lange, B. Immersive Medical Virtual Reality: Still a Novelty or Already a Necessity? J. Neurol. Neurosurg. Psychiatry 2023, 94, 499–501. [Google Scholar] [CrossRef]
- Rutkowski, S.; Bogacz, K.; Czech, O.; Rutkowska, A.; Szczegielniak, J. Effectiveness of an Inpatient Virtual Reality-Based Pulmonary Rehabilitation Program among COVID-19 Patients on Symptoms of Anxiety, Depression and Quality of Life: Preliminary Results from a Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 16980. [Google Scholar] [CrossRef]
- Lange, B.; Koenig, S.; Chang, C.-Y.; McConnell, E.; Suma, E.; Bolas, M.; Rizzo, A. Designing Informed Game-Based Rehabilitation Tasks Leveraging Advances in Virtual Reality. Disabil. Rehabil. 2012, 34, 1863–1870. [Google Scholar] [CrossRef]
- Cieślik, B.; Juszko, K.; Kiper, P.; Szczepańska-Gieracha, J. Immersive Virtual Reality as Support for the Mental Health of Elderly Women: A Randomized Controlled Trial. Virtual Real. 2023, 27, 2227–2235. [Google Scholar] [CrossRef] [PubMed]
- De Luca, R.; Torrisi, M.; Piccolo, A.; Bonfiglio, G.; Tomasello, P.; Naro, A.; Calabrò, R.S. Improving Post-Stroke Cognitive and Behavioral Abnormalities by Using Virtual Reality: A Case Report on a Novel Use of Nirvana. Appl. Neuropsychol. Adult 2018, 25, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Moral-Bofill, L.; Lópezdelallave, A.; Pérez-Llantada, M.C.; Holgado-Tello, F.P. Adaptation to Spanish and Psychometric Study of the Flow State Scale-2 in the Field of Musical Performers. PLoS ONE 2020, 15, e0231054. [Google Scholar] [CrossRef] [PubMed]
- Laakasuo, M.; Palomäki, J.; Abuhamdeh, S.; Lappi, O.; Cowley, B.U. Psychometric Analysis of the Flow Short Scale Translated to Finnish. Sci. Rep. 2022, 12, 20067. [Google Scholar] [CrossRef]
- Csikszentmihalyi, M. Flow: The Psychology of Optimal Experience. 1990. Available online: https://www.researchgate.net/publication/224927532_Flow_The_Psychology_of_Optimal_Experience (accessed on 3 March 2025).
- Norsworthy, C.; Jackson, B.; Dimmock, J.A. Advancing Our Understanding of Psychological Flow: A Scoping Review of Conceptualizations, Measurements, and Applications. Psychol. Bull. 2021, 147, 806–827. [Google Scholar] [CrossRef]
- Schüler, J. Arousal of Flow Experience in a Learning Setting and Its Effects on Exam Performance and Affect. Z. Pädagog. Psychol. 2007, 21, 217–227. [Google Scholar] [CrossRef]
- Jackson, S.A.; Thomas, P.R.; Marsh, H.W.; Smethurst, C.J. Relationships between Flow, Self-Concept, Psychological Skills, and Performance. J. Appl. Sport Psychol. 2001, 13, 129–153. [Google Scholar] [CrossRef]
- Tussyadiah, I.; Wang, D.; Jia, C. Virtual Reality and Attitudes Toward Tourism Destinations. In Information and Communication Technologies in Tourism 2017; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Verma, S.; Warrier, L.; Bolia, B.; Mehta, S. Past, present, and future of virtual tourism-a literature review. Int. J. Inf. Manag. Data Insights 2022, 2, 100085. [Google Scholar] [CrossRef]
- Horsak, B.; Simonlehner, M.; Schöffer, L.; Dumphart, B.; Jalaeefar, A.; Husinsky, M. Overground Walking in a Fully Immersive Virtual Reality: A Comprehensive Study on the Effects on Full-Body Walking Biomechanics. Front. Bioeng. Biotechnol. 2021, 9, 780314. [Google Scholar] [CrossRef]
- Sikorska, J. Między realnością a wirtualnością. Wykorzystanie fotogrametrii w grze wideo Zaginięcie Ethana Cartera. Images Int. J. Eur. Film Perform. Arts Audiov. Commun. 2017, 21, 165–175. Available online: https://www.ceeol.com/search/article-detail?id=732233 (accessed on 15 March 2025). [CrossRef]
- Dreesmann, N.J.; Su, H.; Thompson, H.J. A Systematic Review of Virtual Reality Therapeutics for Acute Pain Management. Pain Manag. Nurs. Off. J. Am. Soc. Pain Manag. Nurses 2022, 23, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Weech, S.; Kenny, S.; Barnett-Cowan, M. Presence and Cybersickness in Virtual Reality Are Negatively Related: A Review. Front. Psychol. 2019, 10, 158. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator Sickness Questionnaire: An Enhanced Method for Quantifying Simulator Sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar] [CrossRef]
- Bos, J.E.; Bles, W.; Groen, E.L. A Theory on Visually Induced Motion Sickness. Displays 2008, 29, 47–57. [Google Scholar] [CrossRef]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in Fully Immersive Virtual Environments: An Evaluation of Potential Adverse Effects in Older Adults and Individuals with Parkinson’s Disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef]
- Bles, W.; Bos, J.E.; de Graaf, B.; Groen, E.; Wertheim, A.H. Motion Sickness: Only One Provocative Conflict? Brain Res. Bull. 1998, 47, 481–487. [Google Scholar] [CrossRef]
- Sevinc, V.; Berkman, M.I. Psychometric Evaluation of Simulator Sickness Questionnaire and Its Variants as a Measure of Cybersickness in Consumer Virtual Environments. Appl. Ergon. 2020, 82, 102958. [Google Scholar] [CrossRef]
- Díaz-García, A.; González-Robles, A.; Mor, S.; Mira, A.; Quero, S.; García-Palacios, A.; Baños, R.M.; Botella, C. Positive and Negative Affect Schedule (PANAS): Psychometric Properties of the Online Spanish Version in a Clinical Sample with Emotional Disorders. BMC Psychiatry 2020, 20, 56. [Google Scholar] [CrossRef]
- Rzeźniczek, P.; Lipiak, A.; Bilski, B.; Laudańska-Krzemińska, I.; Cybulski, M.; Chawłowska, E. Exploring the Participant-Related Determinants of Simulator Sickness in a Physical Motion Car Rollover Simulation as Measured by the Simulator Sickness Questionnaire. Int. J. Environ. Res. Public Health 2020, 17, 7044. [Google Scholar] [CrossRef]
- Zainal, N.H.; Chan, W.W.; Saxena, A.P.; Taylor, C.B.; Newman, M.G. Pilot Randomized Trial of Self-Guided Virtual Reality Exposure Therapy for Social Anxiety Disorder. Behav. Res. Ther. 2021, 147, 103984. [Google Scholar] [CrossRef]
- Lee, D.; Hong, S.; Jung, S.; Lee, K.; Lee, G. The Effects of Viewing Smart Devices on Static Balance, Oculomotor Function, and Dizziness in Healthy Adults. Med. Sci. Monit. 2019, 25, 8055–8060. [Google Scholar] [CrossRef] [PubMed]
- Elsenbast, C. The Use of the Simulator Sickness Questionnaire in High Immersive Virtual Reality—Avalidation Study in Educational Practice. 2022. Available online: https://www.researchgate.net/publication/358089321_The_use_of_the_Simulator_Sickness_Questionnaire_in_high_immersive_Virtual_Reality_-A_validation_study_in_educational_practice (accessed on 13 March 2025).
- Litleskare, S.; Calogiuri, G. Camera Stabilization in 360° Videos and Its Impact on Cyber Sickness, Environmental Perceptions, and Psychophysiological Responses to a Simulated Nature Walk: A Single-Blinded Randomized Trial. Front. Psychol. 2019, 10, 2436. [Google Scholar] [CrossRef] [PubMed]
- Palmisano, S.; Constable, R. Reductions in Sickness with Repeated Exposure to HMD-Based Virtual Reality Appear to Be Game-Specific. Virtual Real. 2022, 26, 1373–1389. [Google Scholar] [CrossRef]
- Kim, Y.S.; Won, J.; Jang, S.-W.; Ko, J. Effects of Cybersickness Caused by Head-Mounted Display-Based Virtual Reality on Physiological Responses: Cross-Sectional Study. JMIR Serious Games 2022, 10, e37938. [Google Scholar] [CrossRef]
- Lee, J.; Kim, M.; Kim, J. A Study on Immersion and VR Sickness in Walking Interaction for Immersive Virtual Reality Applications. Symmetry 2017, 9, 78. [Google Scholar] [CrossRef]
- Elmezeny, A.; Edenhofer, N.; Wimmer, J. Immersive Storytelling in 360-Degree Videos: An Analysis of Interplay Between Narrative and Technical Immersion. J. Virtual Worlds Res. 2018, 11. [Google Scholar] [CrossRef]
- Skorupska, E.; Dybek, T.; Rychlik, M.; Jokiel, M.; Dobrakowski, P.; Szczerba, A.; Wotzka, D.; Jankowska, A. A Potential Objective Sign of Central Sensitization: Referred Pain Elicited by Manual Gluteus Minimus Muscle Exploration Is Coincident with Pathological Autonomic Response Provoked by Noxious Stimulation. Pain Res. Manag. 2023, 2023, 4030622. [Google Scholar] [CrossRef]
- Skorupska, E.; Dybek, T.; Wotzka, D.; Rychlik, M.; Jokiel, M.; Pakosz, P.; Konieczny, M.; Domaszewski, P.; Dobrakowski, P. MATLAB Analysis of SP Test Results—An Unusual Parasympathetic Nervous System Activity in Low Back Leg Pain: A Case Report. Appl. Sci. 2022, 12, 1970. [Google Scholar] [CrossRef]
- Le, N.Q. Inducing the Overview Effect Using Virtual Reality. Master’s Thesis, San Jose State University, San Jose, CA, USA, 2020. [Google Scholar] [CrossRef]
- Gerber, S.M.; Jeitziner, M.-M.; Wyss, P.; Chesham, A.; Urwyler, P.; Müri, R.M.; Jakob, S.M.; Nef, T. Visuo-Acoustic Stimulation That Helps You to Relax: A Virtual Reality Setup for Patients in the Intensive Care Unit. Sci. Rep. 2017, 7, 13228. [Google Scholar] [CrossRef]
- Van Gemert, T.; Hornbæk, K.; Knibbe, J.; Bergström, J. Towards a Bedder Future: A Study of Using Virtual Reality While Lying Down. In Proceedings of the 2023 CHI Conference on Human Factors in Computing Systems, Hamburg, Germany, 23–28 April 2023; ACM: New York, NY, USA, 2023; p. 877. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Indicator | Pre Mean (SD) | Post Mean (SD) | Delta (Post-Pre) | Wilcoxon p-Value |
|---|---|---|---|---|
| General Discomfort | 1.17 (0.38) | 1.77 (0.63) | 0.6 | 0.0001 |
| Fatigue | 1.53 (0.63) | 1.7 (0.7) | 0.17 | 0.1967 |
| Eye Strain | 1.37 (0.56) | 2.03 (0.81) | 0.66 | 0.0002 |
| Difficulty Concentrating | 1.23 (0.43) | 1.57 (0.68) | 0.34 | 0.0124 |
| Headache | 1.07 (0.25) | 1.5 (0.78) | 0.43 | 0.0059 |
| Mental Fog | 1.17 (0.38) | 1.47 (0.68) | 0.3 | 0.0293 |
| Blurred Vision | 1.03 (0.18) | 1.43 (0.63) | 0.4 | 0.003 |
| Feeling of Swaying with Eyes Closed | 1.03 (0.18) | 1.3 (0.53) | 0.27 | 0.0114 |
| Dizziness | 1.0 (0.0) | 1.27 (0.52) | 0.27 | 0.0114 |
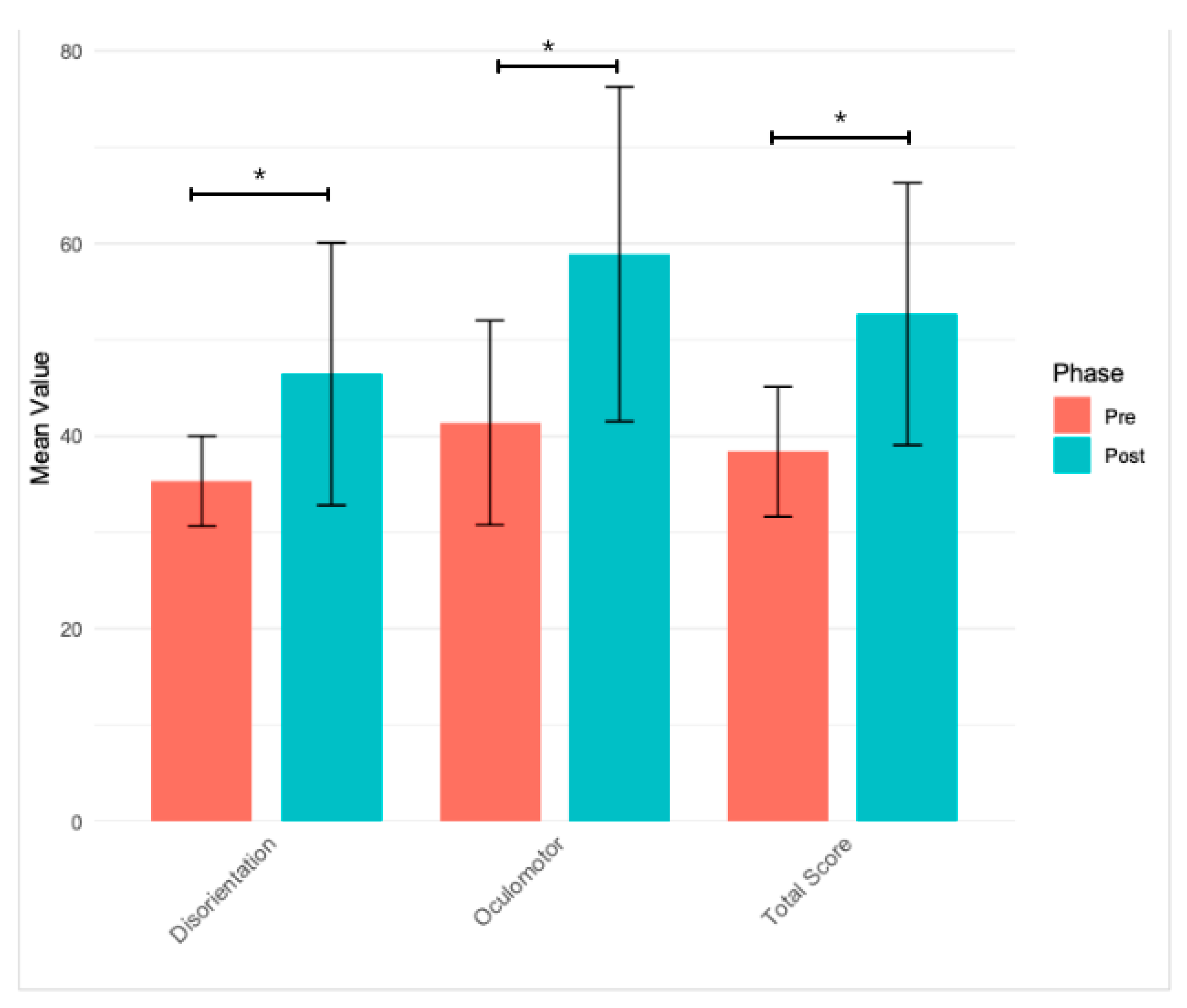
| Oculomotor Symptoms | 41.39 (10.61) | 58.89 (17.36) | 17.5 | 0.0001 |
| Disorientation Symptoms | 35.33 (4.68) | 46.44 (13.62) | 11.11 | 0.0001 |
| Total Score | 38.36 (6.74) | 52.67 (13.6) | 14.31 | <0.0001 |
| Positive | Negative | |
|---|---|---|
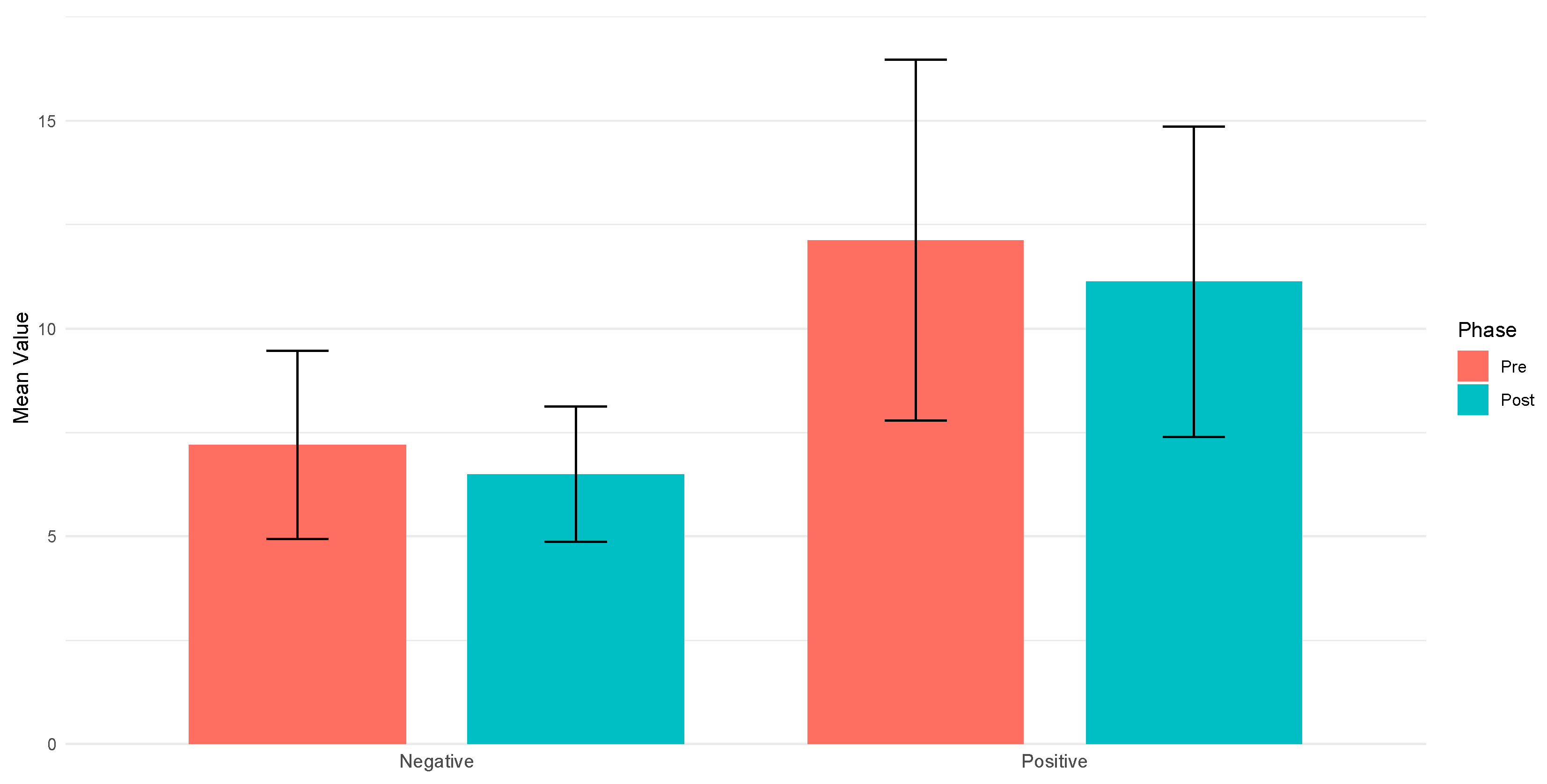
| Mean (SD) Pre | 12.13 (4.34) | 7.2 (2.27) |
| Mean (SD) Post | 11.13 (3.73) | 6.5 (1.63) |
| Delta (Post-Pre) | −1.0 | −0.7 |
| Wilcoxon p-value | 0.097 | 0.151 |
| Survey Item | Mean Score | Standard Deviation |
|---|---|---|
| I felt like I was actually there in the environment of the presentation. | 3.74 | 2.06 |
| It seemed as though I actually took part in the action of the presentation. | 3.28 | 1.83 |
| I had the impression that I was in the same place as the characters and/or objects in the presentation. | 3.25 | 1.75 |
| I felt as though I was physically present in the environment of the presentation. | 3.33 | 1.79 |
| I felt as though I could interact with the characters and/or objects in the presentation. | 2.61 | 2.44 |
| I had the impression that I could act in the environment of the presentation. | 2.83 | 2.13 |
| I had the impression that I could move around among the characters and/or objects in the presentation. | 3.09 | 1.88 |
| It seemed to me as though I could do whatever I wanted in the environment of the presentation. | 2.68 | 2.33 |
| Survey Item | Mean Score | Standard Deviation |
|---|---|---|
| I felt competent enough to meet the demands of the situation. | 3.7 | 1.12 |
| I acted spontaneously and automatically, without having to think. | 3.63 | 1.27 |
| I had a strong sense of what I wanted to do. | 3.47 | 1.17 |
| I had a good idea of how well I was doing when engaged in the task/activity. | 3.47 | 1.01 |
| I was completely focused on the task at hand. | 3.53 | 1.11 |
| I felt a complete sense of control over what I was doing. | 3.3 | 1.24 |
| I was not worried about what others might think of me. | 3.83 | 1.34 |
| The way time passed seemed different than usual. | 4.07 | 1.01 |
| The experience was extremely satisfying for me. | 3.73 | 1.14 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pawełczyk, W.; Olejarz, D.; Gaweł, Z.; Merta, M.; Nowakowska, A.; Nowak, M.; Rutkowska, A.; Batalik, L.; Rutkowski, S. Understanding Cybersickness and Presence in Seated VR: A Foundation for Exploring Therapeutic Applications of Immersive Virtual Environments. J. Clin. Med. 2025, 14, 2718. https://doi.org/10.3390/jcm14082718
Pawełczyk W, Olejarz D, Gaweł Z, Merta M, Nowakowska A, Nowak M, Rutkowska A, Batalik L, Rutkowski S. Understanding Cybersickness and Presence in Seated VR: A Foundation for Exploring Therapeutic Applications of Immersive Virtual Environments. Journal of Clinical Medicine. 2025; 14(8):2718. https://doi.org/10.3390/jcm14082718
Chicago/Turabian StylePawełczyk, Witold, Dorota Olejarz, Zofia Gaweł, Magdalena Merta, Aleksandra Nowakowska, Magdalena Nowak, Anna Rutkowska, Ladislav Batalik, and Sebastian Rutkowski. 2025. "Understanding Cybersickness and Presence in Seated VR: A Foundation for Exploring Therapeutic Applications of Immersive Virtual Environments" Journal of Clinical Medicine 14, no. 8: 2718. https://doi.org/10.3390/jcm14082718
APA StylePawełczyk, W., Olejarz, D., Gaweł, Z., Merta, M., Nowakowska, A., Nowak, M., Rutkowska, A., Batalik, L., & Rutkowski, S. (2025). Understanding Cybersickness and Presence in Seated VR: A Foundation for Exploring Therapeutic Applications of Immersive Virtual Environments. Journal of Clinical Medicine, 14(8), 2718. https://doi.org/10.3390/jcm14082718