Abstract
Osteoporosis leads to increased risk of falls, and thus an increase in fractures, highlighting here hip fractures, that result in high mortality, functional disability, and high medical expenditure. The aim is to summarise the available evidence on effective non-pharmacological interventions to prevent the triad osteoporosis/falls risk/hip fracture. A scoping review was conducted consulting the Scientific Electronic Library Online (Scielo), National Institute for Health and Care Excellence (NICE), Cumulative Index to Nursing & Allied Health Literature (CINAHL) y PubMed.databases. Inclusion criteria were articles published between 2013 and 2019, in Spanish or English. In addition, publications on a population over 65 years of age covering non-pharmacological interventions aimed at hip fracture prevention for both institutionalised patients in long-stay health centres or hospitals, and patients cared for at home, both dependent and non-dependent, were included. Sixty-six articles were selected and 13 non-pharmacological interventions were identified according to the Nursing Interventions Classification taxonomy, aimed at preventing osteoporosis, falls, and hip fracture. The figures regarding the affected population according to the studies are alarming, reflecting the importance of preventing the triad osteoporosis, falls risk, and hip fracture among the population over 65 years of age. The most effective interventions were focused on increasing Bone Mineral Density through diet, exercise, and falls prevention. As a conclusion, primary prevention should be applied to the entire adult population, with special emphasis on people with osteoporosis.
1. Introduction
Osteoporosis is an asymptomatic skeletal disease characterised by low bone mass density and structural deterioration of the bone tissue, resulting in increased bone fragility and susceptibility to fractures, especially hip fractures. Currently, hip fractures are considered one of the most common causes of hospital admission to orthopaedic surgery and traumatology services, affecting more than 200 million people worldwide [1]. In addition, admittances amount to more stays than those caused by diabetes, ischemic heart disease, or breast cancer [2,3], being one of the diseases with greatest socioeconomic impact given its high morbidity and its impact on mortality [3,4,5].
The bone capital is constituted between 15–30 years of age, and in the 10 years following menopause, in the case of women, or around 50 for men, it is a preventive factor for hip fracture. As we grow, bone mass begins to decrease and bone porosity increases, making bones more fragile. This, in turn, increases the chances of suffering a hip fracture [6,7].
The World Health Organization (WHO), in joint action with the International Osteoporosis Foundation (FIO), states that “the number of hip fractures due to osteoporosis is expected to triple over the next 50 years from 1.7 million in 1990 to 6.3 million by 2050”. This means a 6% increase in its incidence among males and 21% in women over 65 years of age. It is important to note that three out of four cases will be women [7,8,9]. Hip fracture rates show great variability between countries, with around 90% of cases in people over 65 years of age. Considering demographic trends, an increase in the number of hip fractures is expected in the coming years [10].
The evolution of the incidence rate of hip fracture has not developed uniformly. However, in most countries, it has increased. Thus, in countries such as the United States, between 1928 and 1942 and from 1973 to 1982, the incidence of hip fracture has been five times higher, from 135.8 to 675.8 per 105 inhabitants. A similar case occurs between 1992 and 2005, where the annual mean of hip fractures was 957.3 per 105 inhabitants in women, and 414.4 per 105 inhabitants in males [11]. These figures are close to those from other countries such as Australia, where there was an increase of approximately 11% in both sexes between 1997 and 2007, from 14,909 to 16,534 cases, estimating that the number of hip fractures will have increased between four and five times by the year 2051 [12].
In Spain, the prevalence of falls among the population over 65 years who reside in the community is around 32%, and between 45–49% among institutionalised people. Falls increase proportionally with age in both sexes and in all ethnic groups. A total of 119,857 hip fractures are recorded among males, and 415.421 in females. The incidence rates per sex were 259.24/105 inhabitants/year in males, and 664.79/105 inhabitants/year in women in 1997; 325.30/105 inhabitants/year and 766.37/105 inhabitants/year in 2010 for males and females, respectively [1,10,13].
Given the relevance of the problem, it is important to get acquainted with the modifiable risk factors, and those that are not, related to osteoporosis, falls risks, and hip fracture. Unmodifiable risk factors include [14]:
- Age: In general, for every decade, the risk of fracture is multiplied by 1.4–1.8.
- Sex: Women have three times more fractures than men.
- Ethnicity: Caucasians have a higher risk of fracture.
- Family history of fracture.
- Early menopause.
Modifiable risk factors include [15,16,17,18,19,20,21,22,23,24,25,26]:
- Body Mass Index (BMI).
- Toxic habits: tobacco and alcohol.
- Diet.
- Sedentary lifestyle and/or low mobility.
- Diseases and medicines.
- Environment (obstacles at home, in the person’s environment...).
- Fear of falling.
Of all of the above, a personal history of fracture in adulthood, low weight, smoking habit, and corticosteroid use generates greater risk. In particular, malnutrition is associated with increased predisposition towards hip fractures. However, higher fat and lean mass are associated with reduced rates of hip fracture. Also, vision problems, early menopause (before age 45), dementia, weak health, low calcium and vitamin D intake, low physical activity, and alcohol consumption (>2 units per day) generate less risk [1,14,17,18,19,20,21,22,23,24,25,26].
This is why it is important to assess the risk of hip fracture. Taking into account the most important risk factors, different evaluation scales have been developed. The tool developed by WHO from studies of population groups in Europe, North America, Asia and Australia is called FRAX ® (Bone fragility fracture risk calculator) [University of Sheffield, Sheffield, UK] [27]. The systematic use of this tool plays a relevant role in Primary Care (AP) and it is based on individual models that use clinical risk factors with the bone mineral density (BMD) of the hip, allowing the calculation of the 10-year probability of fracture, both of the hip and other osteoporotic fractures such as clinical vertebral, forearm or shoulder fractures. [27,28].
From the point of view of primary and secondary prevention, it is important to consider that osteoporosis, falls, and hip fracture are not isolated phenomena, but are part of the same chain of risk. Thus, osteoporosis coupled with modifiable factors create a risk of falls. This one, in turn, causes the hip fracture risk to increase.
Therefore, this work aims to answer the question “What are the most effective non-pharmacological interventions to prevent the triad: osteoporosis, falls risk, and hip fracture in the population over 65 years?”, so as to identify the available evidence on effective non-pharmacological interventions to prevent this triad.
2. Experimental Section
The literature was reviewed following the Arksey and O’Malley’s [29] scoping review method. The Preferred. Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [30] international standard for revisions was applied afterwards in order to collect articles data by following a logical structure and to increase quality, integrity, and consistency, as well as having greater transparency of the revisions and improving their interpretation. The following question was proposed: What are the most effective non-pharmacological interventions to prevent the triad: osteoporosis, falls risk, and hip fracture in the population over 65 years of age? According to the PICO (Patient or problem, Intervention, Comparison, Outcome) strategy [31], the items Population (population over 65 years of age); Intervention (preventive measures); Comparison (not preventive measures), and Outcome (osteoporosis, falls risk, and hip fracture) were stablished.
The following electronic databases were consulted: Scielo, National Institute for Health and Care Excellence (NICE), Cumulative Index to Nursing & Allied Health Literature (CINAHL), and PubMed. The key words selected were: aged; frail elderly; hip fractures; prevention and control; primary prevention; primary care; nurses; smoking; body fat mass; food; nutrition; diet; exercise; exercise therapy; motor activity; treatment; risk factors; accidental falls; osteoporosis; bone mineral density; incidence; epidemiology. They were combined using the booleans AND and OR resulting in the search strategies summarised in Table 1. The search was conducted between November and December 2019.

Table 1.
Search strategies, databases, and references.
As eligibility criteria, the search was limited to: published between 2013 and 2019 in Spanish and English, and with access to the full text. Including articles with a population over the age of 65 and covering non-pharmacological interventions aimed at the prevention of hip fracture, both for institutionalised patients in long-stay health centres or hospitals, and patients cared for at home, both dependent and non-dependent. Also, risk factors that increase the likelihood of osteoporosis, falls, and hip fracture such as diet, toxic habits (tobacco, caffeine, alcohol), underlying diseases, medication, activity and exercise, and multifactorial programmes were assessed. No specific ethnicity was selected. This was complemented by a manual search in relevant websites such as WHO, International Osteoporosis Foundation (FIO), Spanish Society of Rheumatology, and Spanish Society of Internal Medicine.
The references were first reviewed by title and summary for pre-screening. Those studies that met the eligibility criteria were selected. The full critical reading assessment was performed by two researchers, and the disagreements were resolved by a third evaluator.
Critical appraisal was performed following the Critical Appraisal Skills Programme (CASP) [32], the Berra S. et al. tool for descriptive studies [33], and Appraisal of Guidelines Research and Evaluation (AGREE) for clinical practice guidelines [34]. Those who met the CASP screening requirements and scored more than five on the total of the used grid were selected. The structure of the Scottish Intercollegiate Guidelines Network (SING) [35] was used for the evidence synthesis.
The relevant data were extracted from each article, and a table of synthesis of results was prepared, including authorship, method, and summary of results. The extraction was carried out by pairs and, whenever there was some mismatch, it was subjected to the assessment of a third evaluator. Data were gathered by type of intervention:
- Lifestyle modifications: diet, and activity and physical exercise.
- Falls prevention: medication, balance-enhancing therapies, use of incontinence absorbers, and multifactorial programmes.
- Other measures: use of hip protectors.
Interventions aimed at preventing osteoporosis, falls, and hip fracture were identified and classified according to the Nursing Interventions Classification (NIC) taxonomy: 1100 nutrition management; 6490 falls prevention; 2380 medication management; 1850 improving sleep; 486 environmental management: safety; 5510 health education; 1806 help with self-care: transfer; 0221 exercise therapy: ambulation; 0200 exercise promotion; 4978 improve communication: visual deficit; 4720 cognitive stimulation; 6460 dementia management; and 0610 urinary incontinence care. The results were structured by meeting the identified interventions.
As for the information bias of the individual studies, it is specified in the synthesis. To avoid the risks of bias between overrepresented studies, the selected individual studies also included in the selected reviews were identified and eliminated. This prevented biases that affect cumulative evidence.
3. Results
A total of 643 references were identified, from which 66 were selected according to eligibility criteria as presented in Figure 1.
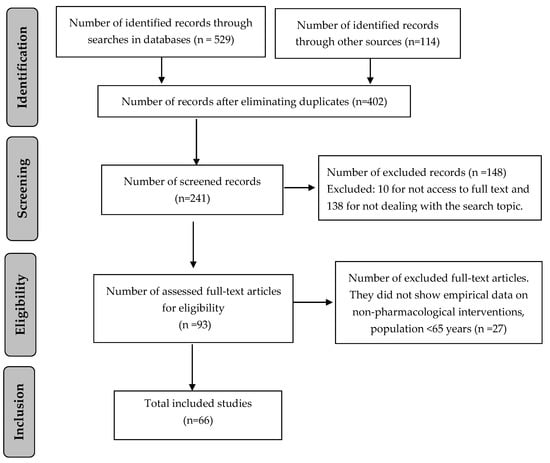
Figure 1.
Flow chart of screening process.
The results section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
3.1. Lifestyle Modifications to Prevent Osteoporosis and Hip Fracture
3.1.1. Diet
Calcium intake decreases bone loss, though it does not have a direct effect on the reduction of fractures in postmenopausal patients with osteoporosis. The recommended amount for patients with osteoporosis or under glucocorticoid treatment is 1500mg/day. That is, between four and four servings are needed to meet calcium needs, considering that a serving of dairy is equivalent to about 300 mg of this mineral (250 mL of milk = 2 yoghurts = 30 g, or 2 slices of cured cheese = 100 g of blue fish eaten with thorns such as 4 sardines in oil = 188 g of dried figs = 200 g of raw chickpeas = 286 g of tofu= 330 g of spinach or chard) [36,37,38].
About 50% of the population with osteoporosis has low serum levels of vitamin D, which is essential for bone development and maintenance as it helps the calcium absorption from food in the bowel, and also ensures the correct renewal and mineralisation of bone tissue [1,39,40,41].
This deficiency could be caused by several reasons such as insufficient intake, limited exposure to sunlight, or because the kidneys cannot convert vitamin D into its active form in the body. In adults, vitamin D deficiency causes osteomalacia, which causes bone pain and muscle weakness [1,7,39,40,41,42,43]. Foods containing this vitamin are quite limited: fatty fish (salmon, tuna, sardines, and mackerel); eggs; liver; and, in some countries, fortified foods such as margarine, dairy, and cereals such as in the United States, where the milk supply is fortified with 400 IU of vitamin D per litre, as well as many plant-based alternatives, such as soy milk, almond milk, and oat milk [7,44,45,46].
Vitamin D is acquired mainly through sun exposure, but this should be moderate. For example, in summer, short exposures (15–20 min) are advised outside of peak solar radiation hours; in autumn and winter, exposures should be increased [39,42]. In people with skin pathologies, brief exposures are recommended. This exhibition should be repeated two to three times per week [43]. Still, in published studies, sun exposure alone does not yield positive results on hip fractures, but vitamin D (800 IU/day) and calcium supplementation is recommended in institutionalised elderly patients [44,45,46].
As for the intake of isoflavones, nutritional supplements (magnesium, copper, zinc, iron, silica, boron, strontium, and manganese), and the consumption of proteins, their effectiveness in terms of decreased hip fracture is not so clear; there is little scientific evidence in this regard [37,47,48,49,50,51].
3.1.2. Tobacco, Alcohol, and Caffeine
Alcohol, caffeine, and tobacco consumption should be avoided, as they increase the risk of frailty fracture by demineralising the bone [18]. The maximum recommended consumption is 15 packs of tobacco/year, 3 units of alcohol/day (1 unit: 8–10 g of alcohol), and 4 cups of coffee/day [52,53,54,55].
3.1.3. Activity and Physical Exercise
Exercise should be performed on a regular basis and with the appropriate intensity for each person, assessed by considering their age, physical condition, and presence of diseases. For example: aquatic exercise is a viable and interesting strategy for older women with osteoporosis who have balance problems and difficulties in exercising on the ground [56]. High-intensity exercise has a significant effect on femoral neck Bone Mineral Density (BMD), but can also lead to problems in the lumbar spine in postmenopausal women, so caution should be exercised [57].
Carrying out muscle-strengthening activities and improving balance is recommended at least 3 days a week for people over 65 years, especially for those with mobility difficulties. Exercise against resistance (contractions of muscle groups with weights or bands) and maintenance exercise (walking, climbing stairs, cycling, swimming, doing Pilates…) help increase muscle strength, tolerance to exercise, and self-confidence [58]. Impact and gravity-based exercises are also effective as the bone adapts and responds to the main direction of mechanical loads (trabecular reorientation) such as shearing, compression, traction, bending, and torsion [58].
The use of oscillating or vibrating platforms for strength and balance exercises increases functional mobility more than exercises not performed on a platform [57,58].
No evidence has been found on the usefulness of Tai-Chi or unipodal exercises for fracture prevention, although they help maintain balance [58].
3.2. Falls Prevention
3.2.1. Medication
It is advisable to remove or minimise all medicines in general. Special attention should be paid to drugs: psychoactives, those that decrease BMD, and which imply a risk of postural hypotension [43].
Drugs responsible for falls increase in older people:
o Psychoactives: hypnotics, anxiolytics, antidepressants, antiepileptics, benzodiazepines, opioids, etc. [59,60]
o Drugs at risk of postural hypotension: diuretics, antihypertensives [61,62,63,64]. Medication that can cause postural hypotension, foot problems and the use of appropriate footwear should also be evaluated [43,65,66].
Drugs that decrease BMD: glucocorticoids, l-thyroxine, heparin, antiepileptics, neuroleptics, chemotherapy, GnRH, aromatase inhibitors, methotrexate, cyclosporine A, vitamin A and synthetic retinoids, lithium, and antidepressants [54,67].
The recommended treatment is bisphosphonate. People with this treatment show a substantially lower risk of frailty fracture and mortality [68].
3.2.2. Exercise Therapies to Improve Balance
Using the cane requires less attention while walking than when using walking aids, and its use may therefore prevent falls. However, the forward body inclination while walking with a cane may also favour them [45]. The use of canes improves confidence and functional capacity of the person, although these can as well limit the ability to obtain information from the environment and/or perform simultaneous tasks [7].
The cane improves balance in stroke patients and significantly reduces body sway in patients with peripheral vestibular balance disorders [68].
3.2.3. Use of Incontinence Absorbers
Urgency, frequency, nocturia, and urinary incontinence are associated with a higher likelihood of falls among the elderly [7,69], as they often lead to people having to get up several times at night to urinate or forces them to use incontinence absorbers, thus limiting hip joint movement and walking skills, and increasing the risk of falling and, therefore, of fractures [25,66].
3.2.4. Multifactorial Intervention Programmes
Multifactorial programmes focused on the systematic assessment of different risk factors and individualised intervention are highly useful in reducing the occurrence of falls among older people. Multifactorial intervention programmes (both in the community and in institutionalised populations) that have shown to be effective in preventing falls include the following elements: regular physical exercise to gain muscle strength and balance, advice instructions and interventions on risks at home, assessment and management of vision, and review of pharmacological treatments (modification or decrease) [20].
When promoting the participation of the elderly in multifactorial intervention programmes to prevent falls, it is important that health professionals assess the possible barriers for their implementation (fear of falling, physical barriers...) [21]. In addition, a careful approach should be followed as falls prevention programmes may as well be ineffective or have adverse effects [70,71].
In addition, it is also necessary to consider the user’s environment so as to adapt it and help the person with the necessary nursing interventions towards the promotion of their autonomy. It is also necessary to train both them and their relatives and/or caregivers in the correct handling of the environment, that is, training and learning on transfers (bed-armchair-WC), and modifications of the environment (having chairs with armrests, installing handles in the toilet and room, raising the toilet seat, evaluating the height of the bed, railings...) [71]. However, programmes based solely on changes in the environment and the education of patients and family members do not appear to be able to reduce, on their own, the risk of falls [27].
In the case of geriatric institutions, in order to reduce the incidence of falls, it is recommended to carry out individual education on risk factors and prevention strategies, as well as establishing targets. These strategies, conducted by a trained occupational therapist, reduce the frequency of falls in high-risk seniors living in the community [25,28,72].
3.3. Other Measures
Use of Hip Protectors
These protectors are placed in the hip area and their function is to absorb the impact of falls and reduce the risk of proximal femur fractures. Its use does not imply a decrease in the number of falls in at-risk patients and, although its effect on the reduction of fractures is not clear, its use is indeed recommended, mainly two-sided protectors in elderly people at high risk of fracture, especially institutionalised ones, as long as they agree to use them and these are properly applied [73].
As for their adverse effects, these are mild and rare and, therefore, do not limit their recommendation. However, many people refuse to use protectors due to the discomfort, difficulty in using them with absorbers, and the need to receive help to place them [73,74].
Table 2.
Results from review articles.
Table 3.
Results from clinical studies.
Table 4.
Results from descriptive studies.
Table 5.
Results from clinical practice guideline.
As a summary of the results, Table 6 identifies the interventions described in the consulted literature and their correspondence with the NIC nurse interventions and the level of evidence and degree of recommendation classified with SING.
Table 6.
Recommended interventions related to the Nursing Interventions Classification.
4. Discussion
In response to the research question, 13 scientifically evidenced non-pharmacological interventions aimed at the prevention of the triad osteoporosis, falls risks, hip fracture in a population over 65 years have been found.
The main recommendations extracted were:
- Evidence level 1+/Degree of recommendation C: Ca and vitamin D supplements in patients treated with glucocorticoids, that consume isoflavones, and with an intake of the following supplements: magnesium, copper, zinc, iron, silica, boron, strontium, manganese, and over-protein consumption [7,14,44,53,75].
- Evidence level 2++/Degree of recommendation B: Ensure a contribution of 1500 mg of calcium/day (each serving of dairy: 300 mg) and vitamin D, exposure to sunlight 15–20 min 2–3 days per week, exercise regularly and progressively (abandon sedentary lifestyle), abandon toxic habits or, if not possible, decrease them as much as possible (alcohol and tobacco), decrease caffeine consumption (increases urinary calcium excretion and hinders its absorption), exercises on vibrating platform [1,7,44,45,46,52,53,54,55,58].
- Evidence level 2+/Degree of recommendation B: Avoid falls risk factors, control medication and diseases, perform educational programmes, adapt the environment and home, address interventions in multifactorial and multidisciplinary programmes, use aid devices such as the cane, and be careful with the use of incontinence absorbers [70].
- Evidence level 2-/Degree of recommendation D: Use of hip protectors, consumption of tea, onion, or vitamin K79 supplements [73,74].
Thus, our study showed the importance of carrying out interventions to prevent the triad osteoporosis, falls risks, hip fracture such as: a calcium-rich diet of 1500mg/day to increase bone mass, in addition to a vitamin D-rich contribution that is acquired mainly through sun exposure, but moderately as recommended by the clinical practice guidelines for patients at risk of frailty fractures [36,37]. Toxic habits such as caffeine, alcohol, and tobacco should be avoided, or at least decrease their consumption [52,53,54,55]. Regarding the intake of isoflavones, nutritional supplements (magnesium, copper, zinc, iron, silica, boron, strontium, and manganese), and protein consumption, there is little scientific evidence to demonstrate their direct effectiveness in reducing hip fractures [6,37,47,48,49,50,51].
In addition, exercising promotes the mass, architecture, and bone structure adaptation, and reduces falls risk. This is especially so with those activities aimed at improving balance and muscle strengthening, thus preventing the triad: osteoporosis, falls risk, and hip fracture [52,53,54,55,56]. Among the activities that may be carried out, water exercises stand out, especially for those persons with balance problems and difficulties in exercising on the ground; also, exercises against resistance (muscle group contractions with weights or bands) and maintenance exercise (walking, climbing stairs, cycling, swimming, Pilates...) that help increase muscle strength, exercise tolerance and self-confidence [54,58].
Special emphasis should be placed on medication adjustment and control of underlying diseases as they increase the presence of osteoporosis and falls, causing an increased risk of hip fracture [61,62,63,64]. These are as psychoactive drugs (hypnotics, anxiolytics, antidepressants, antiepileptics, benzodiazepines, opioids, etc.), those that decrease bone mass density (glucocorticoids, l-thyroxine, heparin, antiepileptics, neuroleptics, chemotherapy, the Gonadotropin-releasing hormone (GnR), aromatase inhibitors, methotrexate, cyclosporine A, vitamin A, and synthetic retinoids, lithium, and antidepressants), and those that pose a risk of postural hypotension (diuretics, antihypertensives) [43,54,59,60,61,62,63,64,67].
Bisphosphonates are recommended as they have shown a substantially lower risk of frailty fracture and mortality among people who take them [68]. It is also important to adapt the environment to the needs of each person, to be careful and monitor episodes of incontinence, as well as the use of absorbents especially at night, and with regard to the use of hip protectors, this is limited, recommended only for those at high risk who accept their use and properly apply them [25,66,73,74].
The limitations of the study refer to the language restriction, the established time period, and the heterogeneity of studies on the incidence of hip fracture. The language of the articles included has been English and Spanish. However, this limitation is counteracted by the universality of both languages and the fact that most of the scientific information found is in either English or Spanish.
Another limitation is that only articles published between 2013–2019 were selected, and previous reference articles may exist. This is offset by the abundance of works existing in this period, by the inclusion of the quality criterion after the critical reading, and the reference search. Eventually, a total of 66 articles including randomised controlled trials, systematic reviews with or without meta-analysis, and clinical practice guidelines published between 2013–2019 were selected.
Another limitation is that data regarding the situation of the evolution of the hip fracture incidence is heterogeneous. The population represented is not entirely homogeneous, varying from one study to another, as well as the time period studied, the design of the works, the methods of analysis used, the results, and the conclusions drawn from each of them. Heterogeneity also makes quantitative synthesis difficult. Despite this, the figures in the studies remain alarming, reflecting the importance of preventing the triad osteoporosis, falls risk, and hip fracture among the population over 65 years. Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
5. Conclusions
Therefore, it is considered essential to establish a strategy for non-pharmacological interventions to prevent hip fracture due to fragility before and during pharmacological treatment in patients with osteoporosis or at risk of such fractures. These are interventions where the nurse has a primary job, but the responsibility is not only his/hers: It is essential to have professionals from other fields, be it healthcare or not (social workers, physiotherapists, occupational therapists...), in order to provide comprehensive care.
These therapies or actions should have a life cycle approach. Therefore, it is necessary to start from childhood in childcare consultations, emphasising the relevant measures to achieve a greater peak in bone mass such as adequate calcium intake, exercise, and non-acquisition of toxic habits. Subsequently, in adult consultations, educational interventions will aim to reinforce all these measures, in addition to those related to environment safety and the reduction of falls such as avoiding or decreasing the use of absorbers, as they limit mobility, thus increasing the risk of falling.
These interventions should include age-appropriate nutritional and health status assessments, as they contribute to better functional recovery and reduced mortality. For this purpose, a balanced diet is advised with an adequate intake of proteins and avoiding excess salt. The Mediterranean diet is fostered here for including foods that contain bioactive components with antioxidant, anti-inflammatory, and alkalising properties that contribute to the improvement of bone health. However, there are few specific studies that have assessed the effect of the Mediterranean diet on bone health.
On the other hand, given the evidence found and the high incidence of hip fractures, osteoporosis and falls among the population over 65 years, further research in non-pharmacological interventions is considered of particular relevance to prevent this triad and increase the level of evidence.
Author Contributions
Conceptualization, M.B.S.-G. and M.N.-M.; methodology, J.G.-S. and M.R.-M.; software, A.P.-D. and G.D.-C.; validation, M.R.-M., M.B.S.-G. and M.N.-M.; formal analysis, G.D.-C., M.B.S.-G. and J.G.-S.; investigation, A.P.-D. and M.R.-M.; resources, M.B.S.-G. and M.N.-M.; data curation, J.G.-S. and A.P.-D.; writing—original draft preparation, A.P.-D. and G.D.-C.; writing—review and editing, M.R.-M. and M.B.S.-G.; visualization, G.D.-C., J.G.-S.; supervision, M.B.S.-G. and M.N.-M.; project administration, A.P.-D. and M.N.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Acknowledgments
In this section you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Osteoporosis: Assessing the Risk of Fragility Fracture. Clinical Guideline. NICE. Available online: https://www.nice.org.uk/guidance/cg146 (accessed on 20 September 2019).
- Shepstone, L.; Lenaghan, E.; Cooper, C.; Clarke, S.; Fong-Soe-Khioe, R.; Fordham, R.; Gittoes, N.; Harvey, I.; Harvey, N.; Heawood, A.; et al. Screening in the community to reduce fractures in older women (SCOOP): A randomised controlled trial. Lancet 2018, 391, 741–747. [Google Scholar] [CrossRef]
- Turner, D.; Khioe, R.F.S.; Shepstone, L.; Lenaghan, E.; Cooper, C.; Gittoes, N.; Harvey, N.; Holland, R.; Howe, A.; McCloskey, E.; et al. The Cost-Effectiveness of Screening in the Community to Reduce Osteoporotic Fractures in Older Women in the UK: Economic Evaluation of the SCOOP Study. J. Bone Miner. Res. 2018, 33, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Tajeu, G.S.; Delzell, E.; Smith, W.; Arora, T.; Curtis, J.R.; Saag, K.G.; Morrisey, M.A.; Yun, H.; Kilgore, M.L. Death, Debility, and Destitution Following Hip Fracture. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2013, 69, 346–353. [Google Scholar] [CrossRef] [PubMed]
- Irwin, A.N.; Billups, S.J.; Heilmann, R.M.F. Labor Costs and Economic Impact of a Primary Care Clinical Pharmacy Service on Postfracture Care in Postmenopausal Women. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2015, 35, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Osteoporosis and Musculoskeletal Disorders. Osteoporosis. Calcium IOF. Available online: https://www.iofbonehealth.org/osteoporosis-musculoskeletal-disorders/osteoporosis/prevention/calcium (accessed on 20 September 2019).
- Ballesteros-Álvaro, A.M.; Crespo-de las Heras, M.I.; Pérez-Alonso, J.; Delgado-González, E.; González-Esteban, M.P. Intervenciones No Farmacológicas Que son Efectivas para Prevenir la Fractura de Cadera por Fragilidad en Atención Primaria. Evidentia 2013, 10. Available online: http://www.index-f.com/evidentia/n44/ev9218.php (accessed on 30 August 2019).
- Joint WHO/FAO Expert Consultation. Dieta, Nutrición y Prevención de Enfermedades Crónicas; OMS: Geneve, Switzerland, 2003; pp. 132–135. [Google Scholar]
- Osteoporosis and Musculoskeletal Disorders. Osteoporosis. Fracture Risk Assessment. IOF. Available online: https://www.iofbonehealth.org/osteoporosis-musculoskeletal-disorders/osteoporosis/diagnosis/fracture-risk-assessment (accessed on 20 September 2019).
- Rapp, K.; Büchele, G.; Dreinhöfer, K.; Bücking, B.; Becker, C.; Benzinger, P. Epidemiology of Hip Fractures. Zeitschrift für Gerontologie und Geriatrie. Available online: https://www.ncbi.nlm.nih.gov/pubmed/29594444 (accessed on 25 January 2019). [CrossRef]
- Fernández-García, M.; Martínez, J.; Olmos, J.; González-Macías, J.; Hernández, J. Tendencia secular de la incidencia de la fractura de cadera en el mundo. Rev. Osteoporos. Metab. Miner. 2015, 7, 121–132. [Google Scholar] [CrossRef][Green Version]
- Crisp, A.; Dixon, T.; Jones, G.; Cumming, R.G.; Laslett, L.L.; Bhatia, K.; Webster, A.; Ebeling, P.R. Declining incidence of osteoporotic hip fracture in Australia. Arch. Osteoporos. 2012, 7, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Fernández-García, M.; Martínez, J.; Olmos, J.; González-Macías, J.; Hernández, J. Revisión de la incidencia de la fractura de cadera en España. Rev. Osteoporos. Metab. Miner. 2015, 7, 115–120. [Google Scholar] [CrossRef][Green Version]
- Carbonell Abella, C.; Martinez Laguna, D.; Muñoz Torres, M.; Nogués Solán, X.; Perez Martin, A. Fragilidad Ósea; Organización Médica Colegial, Fundación para la Formación: Madrid, Spain, 2013; pp. 9–29. Available online: https://www.ffomc.org/sites/default/files/PAS%20FRAGILIDAD%20OSEA.pdf (accessed on 26 September 2019).
- Søgaard, A.J.; Holvik, K.; Omsland, T.K.; Tell, G.S.; Dahl, C.; Schei, B.; Falch, J.A.; Eisman, J.A.; Meyer, H.E. Abdominal obesity increases the risk of hip fracture. A population-based study of 43,000 women and men aged 60–79 years followed for 8 years. Cohort of Norway. J. Intern. Med. 2014, 277, 306–317. [Google Scholar] [CrossRef]
- Giner, M.; Montoya-García, M.-J.; Miranda, C.; Vázquez, M.Á.; Miranda, M.; Pérez-Cano, R. Influencia de la obesidad sobre la microarquitectura y las propiedades biomecánicas en pacientes con fractura de cadera. Rev. Osteoporos. Metab. Miner. 2017, 9, 20–27. [Google Scholar] [CrossRef]
- Lopez, M.G.; Omsland, T.K.; Søgaard, A.J.; Meyer, H.E. Self-perceived memory loss is associated with an increased risk of hip fracture in the elderly: A population-based NOREPOS cohort study. BMC Geriatr. 2015, 15, 134. [Google Scholar] [CrossRef]
- Osteoporosis. Clinical Guideline. NICE. Available online: https://www.nice.org.uk/guidance/qs149. (accessed on 20 September 2019).
- Bakken, M.S.; Schjøtt, J.; Engeland, A.; Engesaeter, L.B.; Ruths, S.; Engesæter, L.B. Antipsychotic Drugs and Risk of Hip Fracture in People Aged 60 and Older in Norway. J. Am. Geriatr. Soc. 2016, 64, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Soliman, Y.; Meyer, R.; Baum, N. Falls in the Elderly Secondary to Urinary Symptoms. Rev. Urol. 2016, 18, 28–32. [Google Scholar] [PubMed]
- Visschedijk, J.; Caljouw, M.; Balen, R.; Hertogh, C.; Achterberg, W. Fear of falling after hip fracture in vulnerable older persons rehabilitating in a skilled nursing facility. J. Rehabil. Med. 2014, 46, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.G.; Fraga, G.P.; Barros, M.B.D.A. Falls among the elderly: Risk factors in a population-based study. Rev. Bras. Epidemiol. 2014, 17, 705–718. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Benetou, V.; Orfanos, P.; Feskanich, D.; Michaëlsson, K.; Pettersson-Kymmer, U.; Eriksson, S.; Grodstein, F.; Wolk, A.; Bellavia, A.; Ahmed, L.A.; et al. Fruit and Vegetable Intake and Hip Fracture Incidence in Older Men and Women: The CHANCES Project. J. Bone Miner. Res. 2016, 31, 1743–1752. [Google Scholar] [CrossRef]
- Bliemel, C.; Oberkircher, L.; Eschbach, D.; Lechler, P.; Balzer-Geldsetzer, M.; Ruchholtz, S.; Bücking, B. Impact of Parkinson’s disease on the acute care treatment and medium-term functional outcome in geriatric hip fracture patients. Arch. Orthop. Trauma Surg. 2015, 135, 1519–1526. [Google Scholar] [CrossRef]
- Leland, N.E.; Gozalo, P.; Bynum, J.; Mor, V.; Christian, T.J.; Teno, J.M. What happens to patients when they fracture their hip during a skilled nursing facility stay? J. Am. Med. Dir. Assoc. 2015, 16, 767–774. [Google Scholar] [CrossRef]
- Chen, K.; Chang, S.; Lin, P. Frailty as a Predictor of Future Fracture in Older Adults: A Systematic Review and Meta-Analysis. Worldviews Evid.-Based Nurs. 2017, 14, 282–293. [Google Scholar] [CrossRef]
- McCloskey, E.; Johansson, H.; Harvey, N.; Shepstone, L.; Lenaghan, E.; Fordham, R.; Harvey, I.; Howe, A.; Cooper, C.; Clarke, S.; et al. Management of Patients with High Baseline Hip Fracture Risk by FRAX Reduces Hip Fractures-A Post Hoc Analysis of the SCOOP Study. J. Bone Miner. Res. 2018, 33, 1020–1026. [Google Scholar] [CrossRef]
- Navarro, R.G.; García, P.G.; Hernández, C.M.; Sauras, Á.C.; Enguídanos, S.V. [Primary and Secondary Prevention of Hip Fragility Fracture in Teruel Health Sector, Aragon, Spain]. Rev. Esp. Salud Publica 2017, 91, e201701002. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, U.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Alonso Coello, P.; Ezquerro Rodríguez, O.; Fargues Garcia, I.; Garcia Alamino, J.M.; Marzo Castillejo, M.; Navarra Llorens, M.; Pardo Pardo, J.; Subirana Casacuberta, M.; Urrutia Cuchí, G. Enfermería Basada en la Evidencia. Hacia la Excelencia en los Cuidados; DAE: Madrid, Spain, 2004; Available online: https://ebevidencia.com/wp-content/uploads/2013/08/EBE.-Hacia-la-excelencia-en-cuidados.pdf (accessed on 29 November 2019).
- CASPe. Programa de Habilidades en Lectura Crítica Español. Alicante (España). 2018. Available online: http://www.redcaspe.org/herramientas/instrumentos (accessed on 30 September 2019).
- Berra, S.; Elorza-Ricart, J.M.; Estrada, M.-D.; Sánchez, E. Instrumento para la lectura crítica y la evaluación de estudios epidemiológicos transversales. Gac. Sanit. 2008, 22, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Flórez Gómez, I.D.; Montoya, D.C. Las guías de práctica clínica y el instrumento AGREE II. Metodología de investigación y lectura crítica de estudios. Rev. Colomb. de Psiquiatr. 2011, 40, 563–576. [Google Scholar] [CrossRef]
- Marzo–Castillejo, M.; Viana-Zulaica, C. Calidad de la evidencia y grado de recomendación. Guías Clín. 2007, 7, 65–82. [Google Scholar]
- Holvik, K.; Ahmed, L.A.; Forsmo, S.; Gjesdal, C.G.; Grimnes, G.; Samuelsen, S.O.; Schei, B.; Blomhoff, R.; Tell, G.S.; Meyer, H.E. No increase in risk of hip fracture at high serum retinol concentrations in community-dwelling older Norwegians: The Norwegian Epidemiologic Osteoporosis Studies. Am. J. Clin. Nutr. 2015, 102, 1289–1296. [Google Scholar] [CrossRef]
- Dahl, C.; Søgaard, A.J.; Tell, G.S.; Forsén, L.; Flaten, T.P.; Hongve, D.; Omsland, T.K.; Holvik, K.; Meyer, H.E.; Aamodt, G. Population data on calcium in drinking water and hip fracture: An association may depend on other minerals in water. A NOREPOS 1 1Norwegian Epidemiologic Osteoporosis Studies. study. Bone 2015, 81, 292–299. [Google Scholar] [CrossRef]
- Bian, S.; Hu, J.; Zhang, K.; Wang, Y.; Yu, M.; Ma, J. Dairy product consumption and risk of hip fracture: A systematic review and meta-analysis. BMC Public Health 2018, 18, 165. [Google Scholar] [CrossRef]
- Avenell, A.; Mak, J.C.S.; O’Connell, D. Vitamin D and vitamin D analogues for preventing fractures in post-menopausal women and older men. Cochrane Database Syst. Rev. 2014, 2014, CD000227. [Google Scholar] [CrossRef] [PubMed]
- Finnes, T.; Lofthus, C.M.; Meyer, H.E.; Søgaard, A.J.; Tell, G.S.; Apalset, E.M.; Gjesdal, C.; Grimnes, G.; Schei, B.; Blomhoff, R.; et al. A combination of low serum concentrations of vitamins K1 and D is associated with increased risk of hip fractures in elderly Norwegians: A NOREPOS study. Osteoporos. Int. 2015, 27, 1645–1652. [Google Scholar] [CrossRef] [PubMed]
- Hiligsmann, M.; Burlet, N.; Fardellone, P.; Al-Daghri, N.; Reginster, J.Y. Public health impact and economic evaluation of vitamin D-fortified dairy products for fracture prevention in France. Osteporos. Int. 2016, 28, 833–840. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5306172/ (accessed on 28 November 2019). [CrossRef] [PubMed]
- Vitamin D—International Osteoporosis Foundation. 2017. Available online: https://www.iofbonehealth.org/osteoporosis-musculoskeletal-disorders/osteoporosis/prevention/vitamin-d (accessed on 29 August 2019).
- Recomendaciones Sobre Osteoporosis. Sociedad Española de Reumatología. 2017. Available online: https://www.ser.es/wp-content/uploads/2018/03/Recomendaciones_OP_DEF.pdf (accessed on 10 December 2019).
- Weaver, C.M.; Alexander, D.D.; Boushey, C.J.; Dawson-Hughes, B.; Lappe, J.M.; LeBoff, M.S.; Liu, S.; Looker, A.C.; Wallace, T.C.; Wang, D.D. Calcium plus vitamin D supplementation and risk of fractures: An updated meta-analysis from the National Osteoporosis Foundation. Osteoporos. Int. 2015, 27, 367–376. [Google Scholar] [CrossRef]
- Montoya, M.J.; Vázquez, M.A.; Miranda, C.; Miranda, M.J.; Pérez-Cano, R.; Giner, M. Influencia de la vitamina D sobre la microestructura y propiedades biomecánicas de pacientes con fractura de cadera. Rev. Osteoporos. Metab. Miner. 2017, 9, 121–129. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S1889-836X2017000400121&lng=es (accessed on 25 November 2019). [CrossRef]
- Poole, C.D.; Smith, J.C.; Davies, J.S. The short-term impact of vitamin D-based hip fracture prevention in older adults in the United Kingdom. J. Endocrinol. Investig. 2014, 37, 811–817. [Google Scholar] [CrossRef]
- Amador-Licona, N.; Moreno-Vargas, E.V.; Martínez-Cordero, C. Ingesta de Proteína, Lípidos Séricos y Fuerza Muscular en Ancianos. Nutr. Hosp. 2018, 35, 65–70. [Google Scholar] [CrossRef]
- Fung, T.T.; Meyer, H.E.; Willett, W.C.; Feskanich, D. Protein intake and risk of hip fractures in postmenopausal women and men age 50 and older. Osteoporos. Int. 2017, 28, 1401–1411. [Google Scholar] [CrossRef]
- Langsetmo, L.; Shikany, J.M.; Cawthon, P.M.; Cauley, J.A.; Taylor, B.C.; Vo, T.N.; Bauer, U.C.; Orwoll, E.S.; Schousboe, J.T.; Ensrud, K.E.; et al. The Association Between Protein Intake by Source and Osteoporotic Fracture in Older Men: A Prospective Cohort Study. J. Bone Miner. Res. 2017, 32, 592–600. [Google Scholar] [CrossRef]
- Díaz Curiel, M. Action of vitamin K on bone health. Rev. Osteoporos. Metab. Miner. 2015, 7, 33–38. Available online: http://scielo.isciii.es/pdf/romm/v7n1/en_revision2.pdf (accessed on 17 November 2019). [CrossRef]
- Rosendahl-Riise, H.; Sulo, G.; Karlsson, T.; Drevon, C.A.; Dierkes, J.; Tell, G.S. Limited Benefit of Fish Consumption on Risk of Hip Fracture among Men in the Community-Based Hordaland Health Study. Nutrition 2018, 10, 873. [Google Scholar] [CrossRef] [PubMed]
- Øyen, J.; Gjesdal, C.G.; Nygård, O.K.; Lie, S.A.; Meyer, H.E.; Apalset, E.M.; Ueland, P.M.; Pedersen, E.R.; Midttun, Ø.; Vollset, S.E.; et al. Smoking and Body Fat Mass in Relation to Bone Mineral Density and Hip Fracture: The Hordaland Health Study. PLoS ONE 2014, 9, e92882. [Google Scholar] [CrossRef] [PubMed]
- Herland, T.; Apalset, E.M.; Tell, G.S.; Lehmann, S.; Eide, G.E. Airflow limitation as a risk factor for low bone mineral density and hip fracture. Eur. Clin. Respir. J. 2016, 3, 32214. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Pereira, R.; De Carvalho, J.F.; Paula, A.P.; Zerbini, C.; Domiciano, D.S.; Gonçalves, H.; Danowski, J.S.; Neto, J.F.M.; Mendonça, L.M.C.; Bezerra, M.C.; et al. Guidelines for the prevention and treatment of glucocorticoid-induced osteoporosis. Rev. Bras. Reum. 2012, 52, 580–593. [Google Scholar] [CrossRef]
- Bisphosphonates for Treating Osteoporosis. NICE. Available online: https://www.nice.org.uk/guidance/ta464 (accessed on 20 September 2019).
- Narváez, L.M.C.; Almario, A.E.E. Actividad física para mejorar fuerza y equilibrio en el adulto mayor. Univ. Salud 2017, 19, 94. [Google Scholar] [CrossRef]
- Feskanich, D.; Flint, A.J.; Willett, W.C. Physical activity and inactivity and risk of hip fractures in men. Am. J. Public Health 2014, 104, e75–e81. [Google Scholar] [CrossRef] [PubMed]
- Skelton, D.A.; Bailey, C.; Howel, D.; Cattan, M.; Deary, V.; Coe, D.; De Jong, L.D.; Gawler, S.; Gray, J.; Lampitt, R.; et al. Visually Impaired OLder people’s Exercise programme for falls prevenTion (VIOLET): A feasibility study protocol. BMJ Open 2016, 6, e011996. [Google Scholar] [CrossRef]
- Machado-Duque, M.E.; Castaño-Montoya, J.P.; Medina-Morales, D.A.; Castro-Rodríguez, A.; González-Montoya, A.; Machado-Alba, J.E. Association between the use of benzodiazepines and opioids with the risk of falls and hip fractures in older adults. Int. Psychogeriatr. 2017, 30, 941–946. [Google Scholar] [CrossRef]
- Brännström, J.; Lövheim, H.; Gustafson, Y.; Nordström, P. Association Between Antidepressant Drug Use and Hip Fracture in Older People Before and After Treatment Initiation. JAMA Psychiatry 2019, 76, 172. [Google Scholar] [CrossRef]
- Lai, C.-L.; Kuo, R.N.; Chen, H.-M.; Chen, M.-F.; Chan, K.A.; Lai, M.-S. Risk of hip/femur fractures during the initiation period of α-adrenoceptor blocker therapy among elderly males: A self-controlled case series study. Br. J. Clin. Pharmacol. 2015, 80, 1208–1218. [Google Scholar] [CrossRef]
- Dore, D.; Zullo, A.R.; Mor, V.; Lee, Y.; Berry, S.D. Age, Sex, and Dose Effects of Nonbenzodiazepine Hypnotics on Hip Fracture in Nursing Home Residents. J. Am. Med. Dir. Assoc. 2018, 19, 328–332.e2. [Google Scholar] [CrossRef]
- Sosa-Henríquez, M.; Curiel, M.D.; Pérez, A.D.; Alonso, C.G.; Macías, J.G.; Minguella, J.F.; Rubio, J.F.; Saidler, L.M.; Solán, X.N.; Hernandez, D.H. Guía de prevención y tratamiento de la osteoporosis inducida por glucocorticoides de la Sociedad Española de Medicina Interna. Rev. Clín. Esp. 2008, 208, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Johansen, J.S.; Havnes, K.; Halvorsen, K.H.; Haustreis, S.; Skaue, L.W.; Kamycheva, E.; Mathiesen, L.; Viktil, K.K.; Granas, A.G.; Garcia, B.H. Interdisciplinary collaboration across secondary and primary care to improve medication safety in the elderly (IMMENSE study): Study protocol for a randomised controlled trial. BMJ Open 2018, 8, e020106. [Google Scholar] [CrossRef] [PubMed]
- Vázquez, F.L.; Bonis, J.; Cerezo, V.B.; Hernández, S.H.; Sánchez, L.J.; Holgado Diaz, A. Prevención de fractura osteoporótica en España: Uso de fármacos antes y después de una fractura de cadera. Rev. de Osteoporos. Metab. Miner. 2015, 7, 54–62. [Google Scholar] [CrossRef]
- Lee, V.W.Y.; Leung, T.P.Y.; Lee, V.W.H. Outpatient Medication Use in Chinese Geriatric Patients Admitted for Falls. Am. J. Ther. 2016, 23, e1729–e1735. [Google Scholar] [CrossRef] [PubMed]
- Van Geel, T.A.C.M.; Bliuc, D.; Geusens, P.P.M.; Center, J.R.; Dinant, G.-J.; Tran, T.; van den Bergh, J.; McLellan, A.R.; Eisman, J.A. Reduced mortality and subsequent fracture risk associated with oral bisphosphonate recommendation in a fracture liaison service setting: A prospective cohort study. PLoS ONE 2018, 13, e0198006. [Google Scholar] [CrossRef]
- Olmo, J.; Roman, P.; Leon, M.; Mena, P.; Ignatowitz, U.; Fuentes, M.; Almagro, M.; Martínez, E.; Torres, J.; Canteras, M. Riesgo de fractura osteoporótica mayor y de cadera en pacientes con accidente cerebrovascular en fase aguda: Estudio prospectivo multicéntrico. Rev. Osteoporos. Metab. Miner. 2014, 6, 40–45. [Google Scholar] [CrossRef]
- Sánchez-Hernández, N.; Sáez-López, P.; Paniagua-Tejo, S.; Valverde-García, J. Resultados tras la aplicación de una vía clínica en el proceso de atención al paciente geriátrico con fractura de cadera osteoporótica en un hospital de segundo nivel. Rev. Esp. Cir. Ortop. Traumatol. 2016, 60, 1–11. [Google Scholar] [CrossRef]
- Tiedemann, A.; Sherrington, C.; Lord, S.R. The role of exercise for fall prevention in older age. Motriz Rev. Educ. Fís. 2013, 19, 541–547. [Google Scholar] [CrossRef]
- Fernandez, M.A.; Griffin, X.L.; Costa, M.L. Management of hip fracture: Figure 1. Br. Med. Bull. 2015, 115, 165–172. [Google Scholar] [CrossRef]
- Maximos, M.; Chang, F.; Patel, T. Risk of falls associated with antiepileptic drug use in ambulatory elderly populations. Can. Pharm. J. Rev. Pharm. Can. 2017, 150, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Cianferotti, L.; Fossi, C.; Brandi, M.L. Hip Protectors: Are They Worth it? Calcif. Tissue Int. 2015, 97, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Santesso, N.; Carrasco-Labra, A.; Brignardello-Petersen, R. Hip protectors for preventing hip fractures in older people. Cochrane Database Syst. Rev. 2014, CD001255. [Google Scholar] [CrossRef]
- Romero Pérez, A.; Rivas Velasco, A. Adherence to Mediterranean diet and bone health. Nutr. Hosp. 2014, 29, 989–996. Available online: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0212-16112014000500005 (accessed on 17 November 2019). [PubMed]

© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).