Abstract
Little is known about monthly home visits, a traditional Japanese Buddhist custom, wherein Buddhist priests visit their parishioners’ homes every month. This study aimed to explore this custom in terms of community health care. Qualitative data were collected from 14 Buddhist priests from various areas, followed by quantitative data collection on all the temples in the Osaka parish, where 486 questionnaires were distributed and 299 were retrieved. From the interviews, the functions of the monthly home visits were categorized into the following six categories: “finding incidents”, “preventing suicides”, “caring for older people”, “grief care”, “a peaceful passing”, and “connecting people”. Ninety-one percent of Buddhist priests made monthly home visits in the Osaka parish, with a median of 30.0 times per month. The median duration of their visits was 25.0 min. Those who carried out a high number of monthly home visits had more experience in: noticing dementia or physical deterioration; being asked for advice about a serious issue; dealing with the grief of bereavement; finding someone whom they were concerned about, but being unsure to what extent to get involved; finding someone in cardiopulmonary arrest or unconsciousness; and finding someone whom they were concerned about but not knowing where to ask for help.
1. Introduction
Historically, Buddhism has supported a wide range of people’s lives in Japan (Schrimpf 2018). Since the Heian Era, which began in the 8th century when Kyoto became the imperial capital, health care in Japan has long been provided by Buddhist “priest-doctors”, where commoners found medical help in Buddhist temples. From the late 19th century, Buddhist priest doctors were challenged by both Chinese herbal medicine (kanpō) and European medical thought. After the Meiji Restoration, which aimed to establish a modern and strong nation-state, the new government developed the medical licensing system, leading to the current system created following the German model. Recently, since Buddhist temples are known to be managed mainly through the income from funeral rites and mourning services, temples are often criticized as “funeral Buddhism”; this means that Buddhist priests focus on holding rites for the deceased, and not on helping living people. In response to this criticism, according to Takahashi (2022), interfaith chaplaincy influenced by Western psychotherapy, overseas Buddhism, and traditional Japanese folk customs were established to meet the needs of the medical community as this community does not focus on religion but has high, and sometimes excessive, expectations of spiritual care. This is a framework that does not provide religious care, only spiritual care. However, only 212 interfaith chaplains exist in the country, which is far from the universal system (Society for Interfaith Chaplaincy in Japan n.d.). Taniyama and Becker (2014) suggest another possible answer to this criticism such as monthly services consisting of sutra chanting followed by chatting over tea. Chanting and chatting cannot be separated; if they create good relations between the monks and bereaved families, they can serve as a monthly time of healing for the bereaved. Although this is not explicitly stated, Japanese people with knowledge of Buddhism will know that they are referring to the “monthly home visit”.
Monthly home visits—Tsuki-Mairi (月参り) in Japanese—is a traditional Japanese Buddhist custom in which Buddhist priests visit the homes of their parishioners to perform ancestral rites and offerings for the dead, on the nearest deathday of every month (Jodo Shu, 2018). As these visits have been taken for granted in Japanese culture, they have not been the subject of much research in Japan, and there is little epidemiological literature in English on them; these have not been mentioned in pioneering works on ancestor worship in contemporary Japan (Smith 1974). Photos of a monthly home visit can be seen in Figure 1. Additionally, a video of a monthly home visit can be viewed in the Supplementary Materials (S1).

Figure 1.
Photos of a monthly home visit in Kyushu (left) and Osaka (right).
The first epidemiological studies in English on monthly home visits comprised what we had previously revealed using geographic information analysis (viz., large regional differences exist in the practice of monthly home visits, whose distribution was similar in different denominations) (Ogawa et al. 2022a), but we do not have data on when the practice began. This study is an attempt to explore this custom, which has not been the subject of academic research with scientifically valid methods, with a view to finding undiscovered solutions to contemporary social issues.
Today, the aging of modern Japanese society casts a heavy shadow. By the middle of the 21st century, it is estimated that the aging rate—calculated as the percentage of people aged over 60 years in the total population—will be 40%, and the number of people with dementia will be approximately 10% of the total population (Cabinet Office 2017). Nowadays, families are not reliable enough as social resources, given that 30% of households that include older persons are single-person households, and 30% are older married-couple households (Cabinet Office 2017). Considering that as people get older, a decrease in cognitive or physical abilities tends to occur at any time, older people are clearly at a risk of discontinuing community life against their will, as shown by empirical research. A longitudinal study conducted in Tokyo found that half of an older population with cognitive decline were unable to continue living in the community over a five-year period (Okamura et al. 2022). Therefore, there is a need for a novel outreach system to look after older people who are not being cared for or looked after. However, social resources to support older people are depleted due to the population shrinking and aging (Sano et al. 2023). Collaboration with Buddhist temples and priests, or the reallocation of existing resources that have not even been regarded as social resources by health care professionals, are a possible solution. Therefore, this study proposes the use of Buddhis priests and temples in this area (Okamura et al. 2018; Ogawa et al. 2022b).
According to a survey conducted by the Ministry of Education, Culture, Sports, Science and Technology (2016), there were more than 353,000 Buddhist priests in Japan compared with 76,000 Shinto and 32,000 Christian priests. The number of Buddhist priests in Japan is larger than that of its police officers (260,000) (National Police Agency 2021). Temples and priests are large social resources that have been overlooked in the healthcare area.
In this study, our research questions were to analyze the characteristics of monthly home visits from the perspective of health care, and not religious studies, based on the perception and behavior of priests. Furthermore, by exploring unknown data on these monthly home visits from the perspective of care, we expect to provide evidence for repositioning the existing resources for older people’s secular support system.
2. Results
2.1. Qualitative Approach
Ten Buddhist priests, who regularly carried out monthly home visits and had been selected by snowball sampling, were interviewed during 2018 without any concerns. Table 1 lists the basic data of the interviewees.

Table 1.
Interviewees.
Concerning what the interviewees considered to be the function of the monthly home visits in the present era, the following six categories emerged: “finding incidents”, “preventing suicides”, “caring for older people”, “grief care”, “a peaceful passing”, and “connecting people”. The discourses representing each category or subcategory are listed in Table 2. As has been stated previously, these were incorporated into the quantitative questionnaire.
Table 2.
Categories, subcategories, and citations concerning what the interviewees considered to be the function of monthly home visits in the present era.
In addition, during free conversations, they expressed confidence in, and enjoyment of, their monthly home visits. In response to this, we included a scale in the questionnaire that asked about mental well-being.
At that time, there was a problem with a group of juvenile motorcycle gangs. They were gathering at a house I visited. When I was arguing with them about stopping the dangerous group of motorcycle runaways, the parents there told me that they had given up on them. So, I said to them, “You gave birth to them; so, you are responsible for them, and as parents, you should stand together against them.” Then, I told the gang “I will not even give you a funeral, if you die,” and they were surprised. After a while, the bad boys stopped doing bad things. After a long time, I went to an old lady’s funeral, and two young men in business suits came and thanked me for what I had done (i.e., stopped them, that had made them return to the right way). I was happy.(Z)
I, myself, listen to an old lady for a long time because her stories are interesting, but some priests try to leave (the house) at 5 pm.(K)
Many priests are unaware about the monthly visits having a function of grief care. However, I think it is amazing that they are doing it naturally, without recognizing that it is grief care. It means there is a treasure in that custom that no one knows about.(N)
2.2. Quantitative Approach
Of the 486 questionnaires distributed, 299 (62% response rate) were retrieved (Table 3). There were 280 males, 16 females, 1 other, and 2 non-respondents; 156 (52%) were 60 years of age or older. Of these, 271 (91%) indicated that they carried out monthly home visits.
Table 3.
Comparative characteristics of Buddhist priests who carried out and did not carry out monthly home visits.
We compared 271 Buddhist priests who carried out monthly home visits with 27 who did not. While the two groups did not differ in terms of age, gender, or other qualifications they possessed, the priests who did not make monthly home visits were more likely to interact with the public sector, as shown in Table 3.
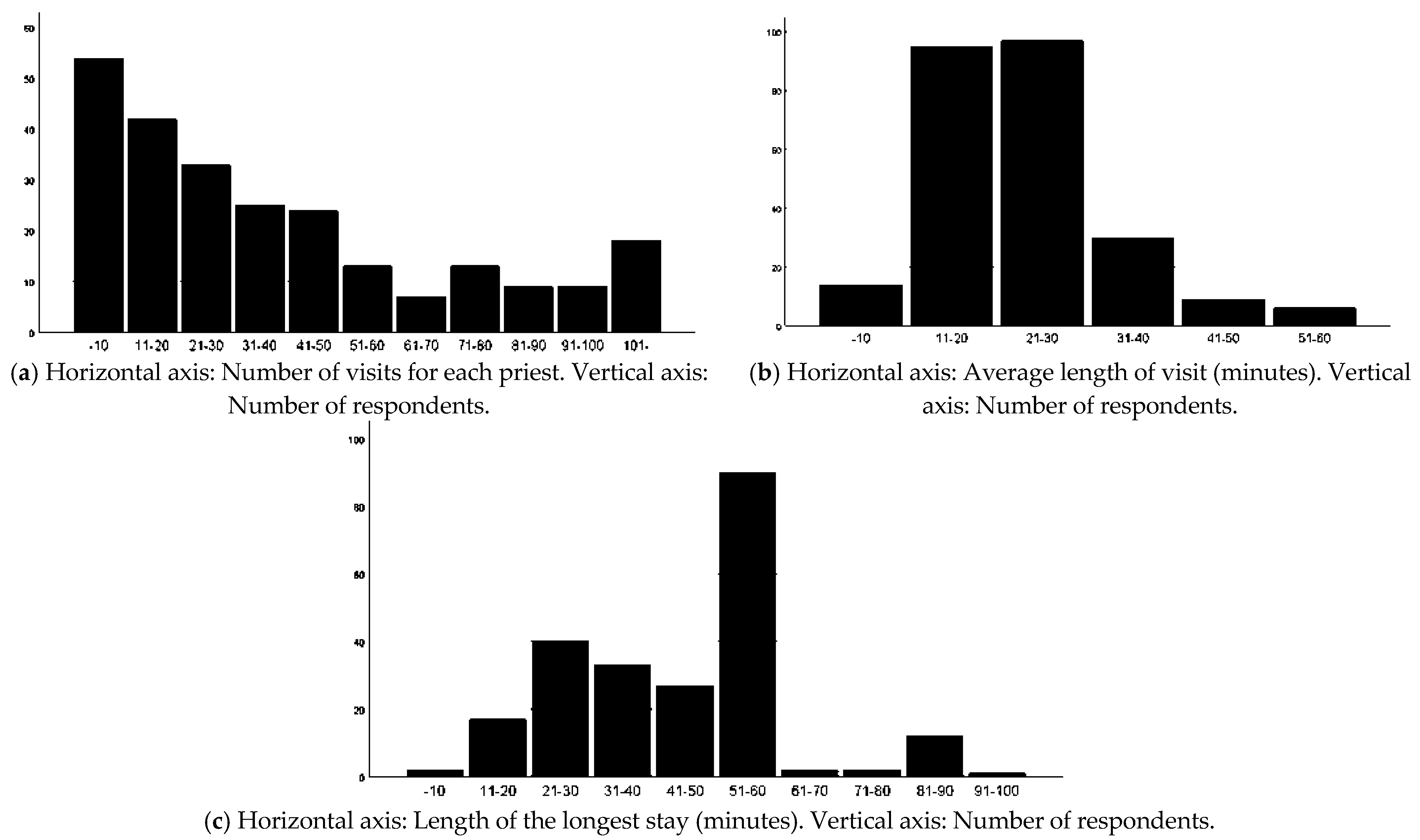
Among the respondents who answered regarding conducting monthly home visits, 246 filled in the number of their monthly home visits. The average number of monthly visits for each priest was 42.3 (±39.4), and the median was 30.0 (Figure 2a). The average duration of visits was 26.1 (±10.5) minutes, with a median of 25.0 min (Figure 2b), and the longest stay was 53.6 (±26.4) minutes, with a median of 60 min (Figure 2c). As for the longest stay, the number of respondents decreased significantly over 60 min (92% of the respondents stayed less than 60 min), suggesting that the respondents may have a tendency to try to finish once they reached the 60-min time limit.
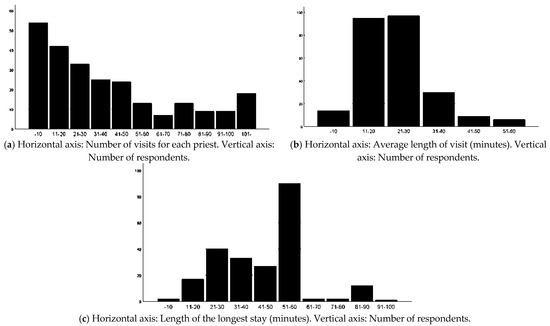
Figure 2.
Basic information of the monthly home visits. (a) Distribution of the number of monthly home visits per month; (b) distribution of the average duration of visits; (c) distribution of the longest duration of visit.
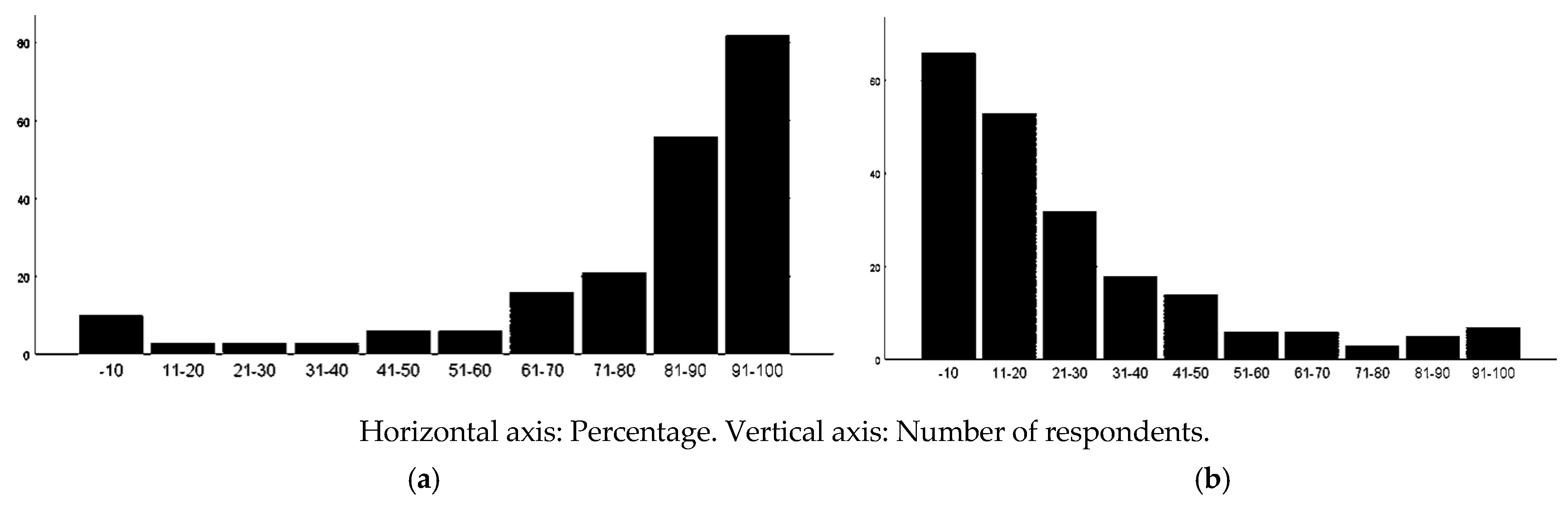
The proportion of visits to older persons was 78.8 (±29.1)%, with a median of 88% (Figure 3a). The proportion of homes visited where the older person lived alone was 25.8 (±24.1)%, with a median of 20.0% (Figure 3b).
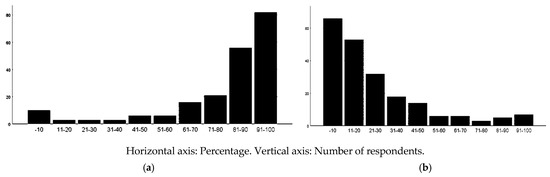
Figure 3.
Older persons who were met in the monthly home visits. (a) Distribution of percentage of visits to older persons; (b) distribution of percentages of homes visited where the older person lived alone.
While 90% of the respondents reported that the number of monthly home visits had decreased compared with 10 years ago, 89% expected it to decrease in the future. Half of the respondents answered that they did not know when their monthly home visits began, whereas among those who did know, more than half answered that it was between the establishment of the modern nation of Japan (1868) and the end of World War II (1945) (Table 4).
Table 4.
The beginning of monthly home visits.
The Buddhist priests’ recognition and practices relating to monthly home visits are presented in Table 5. Concerning their recognition, in order from the most common, comprised opportunities to deepen trust with parishioners (86%), for older persons living alone to talk with a Buddhist priest (77%), and for Buddhist priests to watch over older persons and notice any unusual changes in them (53%). Concerning practice, in order from most common, the priests reported that they had experienced listening to people’s recent situations (79%), consultations regarding Buddhist matters (74%), and noticing dementia or physical deterioration (67%). When priests with a high number of monthly home visits were compared with the usual priests, there was no difference in recognition, but they had more experience in noticing dementia or physical deterioration; being asked for advice about a serious issue and support in daily life; dealing with the grief of bereavement; finding someone whom they were concerned about but being unsure as to what extent to get involved; finding someone in cardiopulmonary arrest or unconsciousness; and finding someone whom they were concerned about, but not knowing where to ask for help. Furthermore, they tended to have more experience in listening to family relationship and financial problems. They also had a tendency to have more attachment to the community.
Table 5.
Buddhist priests’ recognition and practice concerning monthly home visits.
3. Discussion
The fact that despite monthly home visits being practiced in so many temples but has neither been a subject of academic research, nor is it available in the English literature, is in itself, an interesting phenomenon. This may be because it is perceived as too common, to the extent that no researcher has been willing to investigate it, or perhaps do not see the value in it because it is an old practice. Regarding collaborating with religious workers in the care of older people in the community, there have been reports from a spiritual care perspective. According to Ilmi et al. (2024), these are spiritual interventions that use mindfulness, singing, etc., and not those used in this study; hence, the idea that traditions that have been practiced unchanged for a long time, in their original form, are conducive to community care. In this regard, to the best of our knowledge, this study adopted a direction that has not been previously studied.
In terms of recognition, there was no difference between priests who did 60 and more visits, and those who did less than 60. However, concerning the practice, there were differences. More monthly home visits were related to having more experience of facing the crises and sufferings of older people living in the community. Simultaneously, the priests were increasing their opportunities to be relied upon by older people and their attachment to the community. These experiences increase their competence as community resources. While this study also revealed that the tradition of monthly home visits is gradually weakening, unexpectedly high recognition from the medical and care arenas will lead to a reassessment of its value in the Buddhist community, which in turn, could lead to an increase in its potential for community care.
Historically, all citizens were registered at temples through their family during the Edo period. This system clearly has its foundation in old familism and the Danka system, whose influence is still significant, and population coverage large. Considering that the seven traditional Buddhist denominations in Japan were harmonious with the modern nation state, apparently violent and radical ideologies come from a very new religion, and not from traditional Buddhism. Hence, it is possible for these denominations to work with the secular state and move toward age-friendly communities. Monthly home visits could become a way of looking after older people who are suffering from loneliness in modern communities.1
This study described monthly home visits from an epidemiological and medical perspective. However, in terms of behavior, this does not mean that religious practice is legitimatized by medical evidence. Schrimpf (2018), citing Rothstein (2004), accurately and critically discussed the current situation in Japan as “no religion of the modern world will successfully be able to claim authority without some kind of scientific legitimization”. Buddhist priests who perform monthly home visits do not see themselves as practicing medicine or trying to compete with it; neither do the residents see it as such. We report that monthly home visits have a multifaceted value; it is practical even when assessed through the methodology of medicine. We hope that this study will provide an opportunity for contemporary Japanese medicine, which is facing a variety of challenges, such as an increased number of people with dementia, frailty, multi-comorbidity, and difficulty with medical decision-making, to recognize externalities and encourage communication with the religious community.
This study also raises an issue with the Japanese Buddhist community. As discussed in the Introduction section, the Japanese Buddhist community has been subjected to the so-called “funeral Buddhism” criticism. In response, “original” Buddhism was complementary, and alternative medicine in the modern sense of the term obscures the reality of religious practice. Benedict (2018) conducted deeply engaged participation research, reporting that the essence of Buddhist hospice (Vihāra) lies not only in religious rituals, but also in treating the patient as a person. This echoes the monthly home visit, which is also an act of caring for people, with priests conducting outreach for those who cannot afford to go to the temples.
As previously mentioned, after the German medical system was introduced in the Meiji Era, only biological medicine was considered medical care. This led to criticism of “Western medicine” and the emergence of a notion that “Eastern medicine” is holistic and preferable medicine, which is in fact an “invented tradition”. Unlike such claims, this paper argues that the monthly home visit is purely a religious act that is linked to people’s well-being and safety, and that respect should be paid to those involved in it. In other words, monthly home visits tell us what biological medicine, which Japanese people regard as Western medicine, is missing.
Contemporary Japan has several schemes, wherein, someone makes regular visits to an older person’s home to detect changes early and reduce risks. One scheme is a business practice by Japan Post, in which, once a month, a postal worker visits and writes a report to relatives. The other is a long-term care insurance scheme, in which, on certification, a helper regularly provides physical care relating to meals, toileting and bathing, and assistance with daily living, such as cleaning, laundry, shopping, and cooking, at their own home. To compare these secular services and monthly home visits, we had no scientific data; accordingly, we are not arguing that monthly home visits are superior to existing services but suggest that it can be one option for community residents. Grief care and peaceful passing, which were identified in this study, are unique functions of the monthly home visits by Buddhist priests, who have a wealth of experience in bereavement and death, and might be difficult to replace with other visiting services. Although we could not find data concerning community residents, some data suggest that 71% of care workers in geriatric institutions wanted support from outside by Buddhist priests to manage the anxiety and distress of the residents (Okamura et al. 2018). This is collateral evidence that monthly home visits are easily accepted in contemporary society. However, to gain data concerning the benefit and challenges of the monthly home visit is the mission of future research.
The policy recommendations from this study are as follows. First, we propose officially recognizing through official government texts, etc., the clinical collaborations between community comprehensive support centers—key players created by the government in the community comprehensive care system (Japan International Cooperation Agency (JICA) 2022)—and Buddhist temples, and doing this without financial collaboration. This proposal can be immediately implemented and quickly accomplished, given that, one of the tasks of a community comprehensive care center is community networking. Second, in recent years, some Buddhist priests living in temples, but working in the secular system as caregivers, have emerged as public health nurses, and sometimes medical doctors. It is only natural for the secular state to pay them for their work through the insurance system. They could provide momentum to strengthen community care in Japan, but as nothing is known about this either, it is a subject for future research.
A limitation of this study is that its quantitative data was limited to the Osaka parish, and as the rate of implementation of the monthly home visit custom varies widely by region (Ogawa et al. 2022a), all of the categories that emerged in the qualitative approach in the questionnaires could not be included for realistic reasons. For example, questions such as, “Have you ever experienced finding a person who was committing suicide or had committed a suicide?” could not be included because it might be too provocative. Finally, this study was based on the authentic history of Japanese Buddhism and may be from the male perspective. Regarding gender differences, the OECD report (Ferrant et al. 2014) indicates that unpaid care work is still predominantly performed by females. On the other hand, the WHO report (Boniol et al. 2019) indicates that the percentage of females in the healthcare profession is increasing. Given that our focus is on the care activities of Buddhist priests, it can be argued that more females should enter this field. Further research focusing on gender differences, especially on the interaction between the female priest and male/female laity, is needed.
4. Materials and Methods
4.1. Methodology
This study used a mixed methods approach and adopted an exploratory sequential design to explore diverse perspectives and uncover relationships that existed between the intricate layers of our multifaceted research questions, as were stated above (i.e., questions including what and how) (Creswell and Clark 2007; Shorten and Smith 2017; Tashakkori and Creswell 2007). To obtain an overall picture of the issue, first, qualitative data collection and analysis were conducted, and using this as a basis, thereafter, quantitative data collection and analysis were conducted. An overview of this study’s methodology is described in Table 6 to enable readers to understand it in the specific context.
Table 6.
An overview of this study.
The study was not intended to benefit any particular religion or denomination but rather to explore how existing resources are autonomously being transformed in response to an aging secular society, and whether collaborations with existing resources, such as Buddhist temples and priests, can be incorporated into a national dementia strategy.
4.2. Qualitative Approach
4.2.1. Participants
Experience has shown that the activities of Buddhist priests have remained unchanged over the ages, but due to their activities not being computerized, it was expected, that information would not be found in a desk search or in the gray literature. As there was no reason to keep the Buddhist priests’ activities secret, and given that, they had always responded openly to our questions, we decided that the best way to grasp the actual situation would be by asking the priests who actually conduct the activities. Fourteen Buddhist priests—five from Osaka, six from Akita (northeast area), two from Kanagawa (south of Tokyo), and one from Nagoya—who regularly conducted monthly home visits, were selected by snowball sampling.
4.2.2. Methods
This simple interview guide included the number of visits per day; descriptions of the houses visited and behavior during the visits; subjects of talk; whether or not they had met people with challenges such as dementia, withdrawal symptoms, etc.; and any impressive episodes they wished to talk about. The contents of the interviews were immediately shared with the team.
4.2.3. Data
The interviews were audio recorded and verbally transcribed. The verbatim transcripts were sent to the participants for approval of the contents.
4.2.4. Analysis
A qualitative descriptive approach (Neergaard et al. 2009) was adopted, as it is useful in exploratory studies in which little is known about the topic in question. What interviewees considered to be the function of the monthly home visits in the present era was analyzed. Text fragments were coded using MAXQDQ 2022®. Constant comparisons were conducted.
4.3. Quantitative Approach
4.3.1. Participants
Priests attached to all the 486 temples in Osaka parish, belonging to one of the seven main denominations of Japanese Buddhism.
4.3.2. Methods
The questionnaires were mailed to the participants and retrieved. This study was conducted from 1 to 30 October 2022.
4.3.3. Data
In addition to basic characteristics (sex and age), the questionnaire inquired whether the priests were involved in any activities (i.e., other than being Buddhist priests), and whether they collaborated with the public sector. The reason for including this question was because of the interest in the Buddhist priests’ social engagement.
The priests were asked if they conducted monthly home visits, and if they answered that they did not, the survey was ended then and there. Those who answered that they did visit were asked about the number of monthly home visits by their temple, and the number of its priests who were engaged in them. Additionally, they were asked about the number of monthly visits to houses with older people, the number of older people who lived alone, average duration of visits, and maximum duration of a visit. The questionnaire also included questions on how long they had been following this custom, whether it was currently decreasing, and whether they thought it would decrease in the future.
Based on the qualitative data, the priests were asked about their perceptions and practices related to monthly home visits. The research team discussed the qualitative data and formulated questions on the themes that emerged from the qualitative analysis. The questions are shown in Table 7.
Table 7.
Questions about the priests’ perceptions and practices concerning monthly home visits in the questionnaire.
Additionally, they were asked about trust in general, general trust in the community, and attachment to the community as well as about mental well-being using the Japanese version of the World Health Organization-Five Well-Being Index (Awata et al. 2007), in which a score of 12 or less indicates poor mental well-being.
4.3.4. Analysis
Buddhist priests who carried out monthly home visits and those who did not were compared with respect to age, gender, whether or not they had collaborations with the government, and whether or not they had other qualifications, using the χ-square test, as this study was interested in the differences between priests who performed many monthly home visits, and those who did not. The number of monthly home visits for each priest (n) was calculated using the formula below.
n = (total number of visits)/(number of priests involved)
As the 75 percentile was 60, priests who made 60 and over monthly visits and those who made less visits, were similarly compared using the χ-square test. A p-value below 0.05 was regarded as statistically significant. Furthermore, considering that this was an exploratory research study, a p-value below 0.01 was regarded as a tendency.
5. Conclusions
This study described monthly home visits from an epidemiological and medical perspective. The monthly home visit is purely a religious act that is linked to people’s well-being and safety, and where respect should be paid to those involved in it. Considering that the social resources to support older people are being depleted because of population shrinking and aging, collaboration with Buddhist resources is a possible solution for healthcare professionals. However, at this time, there is very little available data on traditional Buddhist resources to which health services researchers can refer, so the findings from this study will provide a basis for future dialogue.
Supplementary Materials
A video of a monthly home visit with English translation can be viewed in the Supplementary Materials available at https://www.youtube.com/watch?v=pJv2cG8xovA (accessed on 27 April 2025). The original data presented in the study are openly available at 10.6084/m9.figshare.28869626.
Author Contributions
Study concept and design: Y.O., A.T., C.U., M.N. and T.O.; Acquisition of data: Y.O., A.T., C.U., M.N. and T.O.; Analysis and interpretation of data: Y.O., A.T., C.U., M.N. and T.O.; Drafting of the manuscript: Y.O. and T.O.; Critical revision of the manuscript for important intellectual content: Y.O., A.T., C.U., M.N. and T.O. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Grant-in-Aid for Scientific Research (JSPS KAKENHI Grant Number JP20K20336) by Japan Society for the Promotion of Science. Y.O. received this grant.
Institutional Review Board Statement
The study protocol was approved by the Ethics Committee of Taisho University (18-021) on 6 August 2018.
Informed Consent Statement
Written informed consent was obtained from all research participants. The research was completed in accordance with the Declaration of Helsinki as revised in 2013. Written informed consent for publication was obtained from individuals who can be identified in the figures.
Data Availability Statement
All quantitative data in this study are included in this published article and its Supplementary Materials. The qualitative data that support the findings of this study are available from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Note
| 1 | According to Ogawa et al. (2022a), in Japan, the monthly home visit is universally implemented in a wide range of denominations including older and more conservative Buddhism. Considering that, as far as we searched, there is no previous research on a similar practice, the community outreach practice of Buddhist priests might be a phenomenon worth mentioning that represents one of the possibilities of Buddhist practice. On the other hand, in areas with more ancient Buddhist traditions and more followers than in Japan, people tend to visit temples more often, so the need for community outreach might be small. This was beyond the scope of our current research, and is the topic of further research. |
References
- Awata, Shuichi, Per Bech, Sumiko Yoshida, Masashi Hirai, Susumu Suzuki, Motoyasu Yamashita, Arihisa Ohara, Yoshinori Hinokio, Hiroo Matsuoka, Yoshitomo Oka, and et al. 2007. Reliability and validity of the Japanese version of the World Health Organization-Five Well-Being Index in the context of detecting depression in diabetic patients. Psychiatry and Clinical Neurosciences 61: 112–19. [Google Scholar] [CrossRef] [PubMed]
- Benedict, Timothy O. 2018. Practicing Spiritual Care in the Japanese Hospice. Japanese Journal of Religious Studies 45: 175–200. [Google Scholar] [CrossRef]
- Boniol, Mathieu, Michelle McIsaac, Lihui Xu, Tana Wuliji, Khassoum Diallo, and Jim Campbell. 2019. Gender Equity in the Health Workforce: Analysis of 104 Countries. Working Paper 1. Geneva: World Health Organization. [Google Scholar]
- Cabinet Office. 2017. Annual Report on the Aging Society: 2017. Available online: https://www8.cao.go.jp/kourei/english/annualreport/2017/pdf/c1-2-1.pdf (accessed on 20 April 2025).
- Creswell, John W., and Vickil Plano Clark. 2007. Designing and Conducting Mixed Methods Research, 1st ed. Thousand Oaks: SAGE. [Google Scholar]
- Ferrant, Gaëlle, Luca Maria Pesando, and Keiko Nowacka. 2014. Unpaid Care Work: The Missing Link in the Analysis of Gender Gaps in Labour Outcomes. OECD Development Centre. Available online: https://www.oecd.org/content/dam/oecd/en/publications/reports/2014/12/unpaid-care-work-the-missing-link-in-the-analysis-of-gender-gaps-in-labour-outcomes_d26d4043/1f3fd03f-en.pdf (accessed on 27 April 2025).
- Ilmi, Ani Auli, Lisa McKenna, Maria Murphy, and Kusrini S. Kadar. 2024. Spiritual care for older people living in the community: A scoping review. Contemporary Nurse 9: 1–15. [Google Scholar] [CrossRef] [PubMed]
- Japan International Cooperation Agency (JICA). 2022. Community-Based Integrated Care in Japan—Suggestions for Developing Countries from Cases in Japan. Available online: https://openjicareport.jica.go.jp/pdf/1000048192.pdf (accessed on 20 April 2025).
- Jodo Shu. 2018. Jodo Shu Dictionary. Tsuki-Mairi. Available online: http://jodoshuzensho.jp/daijiten/index.php/%E6%9C%88%E5%8F%82%E3%82%8A (accessed on 20 April 2025).
- Ministry of Education, Culture, Sports, Science and Technology. 2016. Agency for Cultural Affairs. Religious Yearbook 2016. Available at s-STAT (Statistics Bureau of Ministry of Internal Affairs and Communications). Available online: http://www.e-stat.go.jp/SG1/estat/NewList.do?tid=000001018471 (accessed on 20 April 2025).
- National Police Agency. 2021. Police of Japan 2021. Human Resources. Available online: https://www.npa.go.jp/english/Police_of_Japan/2020/poj2020_p8-10.pdf (accessed on 27 April 2025).
- Neergaard, Mette Asbjoern, Frede Olesen, Rikke Sand Andersen, and Jens Sondergaard. 2009. Qualitative description—The poor cousin of health research? BMC Medical Research Methodology 9: 52. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Yukan, Akinori Takase, Masaya Shimmei, Chiaki Ura, Machiko Nakagawa, and Tsuyoshi Okamura. 2022a. Geography over doctrine? Factors affecting the role of Buddhist priests in a community-based integrated care system. International Journal of Geriatric Psychiatry 37: 5652. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Yukan, Akinori Takase, Masaya Shimmei, Shiho Toishiba, Chiaki Ura, Mari Yamashita, and Tsuyoshi Okamura. 2022b. Meaning of death among care workers of geriatric institutions in a death-avoidant culture: Qualitative descriptive analyses of in-depth interviews by Buddhist priests. PLoS ONE 17: e0276275. [Google Scholar] [CrossRef]
- Okamura, Tsuyoshi, Chiaki Ura, Mika Sugiyama, Hiroki Inagaki, Fumiko Miyamae, Ayako Edahiro, Tsutomu Taga, Shuji Tsuda, Riko Nakayama, Kae Ito, and et al. 2022. Factors associated with inability to attend a follow-up assessment, mortality, and institutionalization among community-dwelling older people with cognitive impairment during a 5-year period: Evidence from community-based participatory research. Psychogeriatrics 22: 332–42. [Google Scholar] [CrossRef] [PubMed]
- Okamura, Tsuyoshi, Masaya Shimmei, Akinori Takase, Shiho Toishiba, Kojun Hayashida, Tatsuya Yumiyama, and Yukan Ogawa. 2018. A positive attitude towards provision of end-of-life care may protect against burnout: Burnout and religion in a super-aging society. PLoS ONE 13: e0202277. [Google Scholar] [CrossRef] [PubMed]
- Rothenstein, Mikael. 2004. Science and Religion in the New Religions. In The Oxford Handbook of New Religions Movement. Edited by James R. Lewis. Oxford: Oxford University Press, pp. 99–118. [Google Scholar]
- Sano, Junko, Yuzuki Hirazawa, Kohei Komamura, and Shohei Okamoto. 2023. An overview of systems for providing integrated and comprehensive care for older people in Japan. Archives of Public Health 81: 81. [Google Scholar] [CrossRef] [PubMed]
- Schrimpf, Monika. 2018. Medical Discourses and Practices in Contemporary Japanese Religions. In Medicine—Religion—Spirituality. Edited by Dorothea Lüddeckens and Monika Schrimpf. New York: Columbia University Press, pp. 57–89. [Google Scholar]
- Shorten, Allison, and Joanna Smith. 2017. Mixed methods research: Expanding the evidence base. Evidence-Based Nursing 20: 74–75. [Google Scholar] [CrossRef] [PubMed]
- Smith, Robert John. 1974. Ancestor Worship in Contemporary Japan. Redwood City: Stanford University Press. [Google Scholar]
- Society for Interfaith Chaplaincy in Japan. n.d. Certified Interfaith Chaplaincy List. Available online: http://sicj.or.jp/uploads/2017/11/e223ec6887ddd317f4515a8167b7a33c.pdf (accessed on 27 April 2025).
- Takahashi, Hara. 2022. Buddhist Spiritual Caregivers in Japan. In The Routledge Handbook of Religion, Medicine, and Health. Edited by Dorothea Lüddeckens, Philipp Hetmanczyk, Pamela E. Klassen and Justin B. Stein. Oxford: Taylor and Francis, pp. 171–85. [Google Scholar]
- Taniyama, Rev Yozo, and Carl B. Becker. 2014. Religious Care by Zen Buddhist Monks: A Response to Criticism of “Funeral Buddhism”. Journal of Religion & Spirituality in Social Work: Social Thought 33: 49–60. [Google Scholar]
- Tashakkori, Abbas, and John W. Creswell. 2007. Exploring the Nature of Research Questions in Mixed Methods Research. Journal of Mixed Methods Research 1: 207–11. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).