Abstract
Aim: The objective of this study was to explore the effects of fixed orthodontic appliances on enamel structure by assessing microfractures, surface roughness, and alterations in color. Methods: This review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. A systematic search of online databases was conducted using the keywords ‘enamel’ AND ‘orthodontic debonding’. Eligibility criteria included both in vivo and ex vivo clinical trials conducted on human teeth. Results and Discussion: A total of 14 relevant papers were analyzed. Various instruments and techniques were utilized across different studies to assess surface roughness, color change, and surface fractures. Conclusions: The findings of this study suggest that ceramic brackets may lead to an increase in enamel fractures, particularly during bracket removal. The surface roughness of enamel exhibits variability depending on the adhesive substance and polishing methods used post-removal. Fixed orthodontic appliances could induce changes in enamel color, which may be alleviated by the use of nano-hydroxyapatite or specific polishing techniques. Further research is necessary to identify effective strategies for managing these color changes and improving the overall outcomes of fixed orthodontic treatment.
Keywords:
orthodontic debonding; enamel appearance; brackets; retainer; crack; roughness; discoloration 1. Introduction
The field of clinical orthodontic procedures has experienced notable evolution with the introduction of bracket bonding onto the enamel surface. This adhesive method not only accelerates the process considerably but also facilitates more accurate positioning of attachments on specific teeth, thus improving patient comfort [1].
The adhesive technique utilizes the bonding capability of the adhesive to establish a connection between the enamel surface and the base of the attachment [2].
While the aim is for this type of bonding to remain robust throughout orthodontic treatment, it often does not. Masticatory forces or inadequate isolation of the tooth during bonding are two common reasons for brackets to detach from teeth [3,4,5,6].
The removal of orthodontic attachments is a primary concern for clinicians during orthodontic treatment. The objective of this final step is to fully eliminate the composite and adhesive from the enamel surface, thereby restoring the enamel to its original condition [7,8,9,10,11,12].
The separation forces exerted by orthodontic pliers can lead to the development of fracture lines and/or enamel fissures, particularly when ceramic brackets debond [13,14,15,16,17,18].
To prevent irreversible iatrogenic harm like enamel surface loss, enamel cracks, pulp necrosis, or lingering adhesive remnants, it is vital to employ an appropriate debonding approach [19,20,21,22].
The gentleness of the debonding process is affected by various factors, including:
- -
- The type of brackets used.
- -
- The instruments used for bracket removal and the technique applied.
- -
- The tools used for removing residual adhesive remnants from the enamel surface.
1.1. Type of Brackets Used
Frequently, the orthodontist’s choice to use ceramic brackets over metal ones is driven by the patient’s preference for aesthetics [23,24]. Ceramics possess inherent characteristics that lead to clinical limitations, including high brittleness (low resistance to fracture) and challenges in forming chemical bonds with adhesive materials [25,26,27,28].
Odegaard illustrated how ceramic attachments often detach at the enamel–adhesive substance contact [29,30]. Separation from metal attachments, conversely, usually happens at the interface between the bracket and adhesive substance, posing a lower risk to the integrity of the enamel [31,32,33].
1.2. The Tools Used for Attachment Removal
In contemporary practice, a variety of debonding techniques are utilized. Mechanical, thermal, and ultrasonic methods represent some examples. Mechanical debonding involves employing different types of forceps like How’s forceps, Weingart’s forceps, straight cutters, or specialized debonding forceps. Research has shown that the latter is the most effective in minimizing damage to the enamel surface.
Thermal debonding presents an alternative for removing ceramic attachments by utilizing the heat generated by a laser, reducing the force required to detach the brackets. However, drawbacks of this method include the bulky nature of the handpiece, the potential irritation to surrounding mucosal tissues, and the discomfort caused by increased warmth [34,35].
Ultimately, studies have shown that ultrasonic debonding drastically decreases adhesion strength, reducing it from 9.2 MPa to 0.28 MPa. However, drawbacks of this method include prolonged operation, leading to patient discomfort and the risk of causing pain if ultrasonic tips make contact with the ceramic attachment [36].
Despite the validity of all three debonding techniques, the mechanical one achieves much more satisfactory results.
1.3. The Technique Employed
The literature describes two debonding techniques: the wing approach and the base method (Figure 1). The wing approach involves gripping the mesial and distal wings of the bracket using forceps, whereas the base method requires inserting the forceps between the bracket’s base and the tooth surface. Brosh’s latest research indicates an overlap between these two debonding procedures [37].
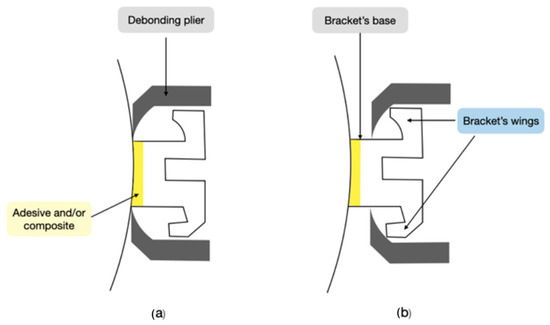
Figure 1.
Two debonding techniques: (a) base method; (b) wings method. Figure created by author R.M.
1.4. The Instruments Used
Another relevant factor is the protocol for removing the adhesive material at the enamel level [38,39,40]. Even in present times, diverse viewpoints exist in the literature, but it is possible to draw the following conclusions:
- -
- Debonding forceps or scalers are inadequate as they can result in significant enamel loss.
- -
- Diamond burs cause permanent damage to enamel.
- -
- Arkansas stones do not completely eliminate composite residue.
- -
- Green stones alone are insufficient in fully removing bonding material.
- -
- Ultrasonic methods necessitate extended chair time and may lead to the loss of small enamel fragments.
- -
- It is recommended that a tungsten carbide bur is used for the primary removal of composite, followed by a disk to eliminate the remaining adhesive residue.
Theoretically, scratches and grooves on enamel could potentially lead to the development of stains and reduce resistance to organic acids found in plaque, thereby increasing the risk of demineralization for teeth [9,41,42].
Regardless, the debonding procedure almost always leads to some degree of enamel damage, even if it is not readily visible to the naked eye and might not always be clinically significant [43,44,45,46].
The objective of this systematic investigation was to analyze alterations in enamel color and roughness resulting from debonding, irrespective of the bracket type or removal techniques utilized. The aim was to explore the most efficient methods to prevent damage and improve the final appearance of enamel after orthodontic treatment. Due to limited research availability in the literature, clinical studies conducted both in vivo and on extracted teeth were assessed.
2. Materials and Methods
2.1. Protocol and Registration
This research adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and was registered with PROSPERO (International Prospective Register of Reviews) under registration number 473047 [47].
2.2. Search Processing
On 15 September 2023, searches were conducted across the PubMed, Scopus, and Web of Science databases using the Boolean keywords “enamel” AND “orthodontic debonding” as part of our search strategy, for an analysis of texts from the past 10 years (2013–2023). These keywords were selected as they closely aligned with the objective of our study, which aimed to assess changes in enamel color and roughness resulting from debonding, irrespective of the bracket type or removal procedures employed. The primary focus was to explore the most effective approaches for minimizing damage and enhancing the overall appearance of enamel following orthodontic treatment.
2.3. Eligibility Criteria and Study Selection
The evaluation of the title and abstract, as well as the entire content, were the two phases of the selection procedure. Any item that met the following parameters was considered: (a) in vivo and ex vivo clinical studies; (b) free full text; (c) human participants of any age; and (d) English language. Publications that lacked original data (such as meta-analyses, research techniques, conference presentations, in vitro or animal studies) were excluded. The preliminary search yielded titles and abstracts that were appraised for relevance. Full publications from relevant studies were obtained for additional examination. Two distinct reviewers (R.M. and L.R.) evaluated the retrieved studies for inclusion using the aforementioned criteria.
2.4. Data Processing
Two reviewers, R.M. and L.R., independently assessed the quality of the studies based on selection criteria that fit the purpose of the review, after conducting a database search to extrapolate the findings. The selected articles were downloaded in the 6.0.15 version for usage with Zotero. To resolve any differences between the two writers, a senior reviewer (F.I.) was contacted. The screening process allowed the exclusion of any publications that did not fit the themes examined. After being found to meet the predefined inclusion criteria, the full text of the publications was read.
2.5. PICOS Requirements
The PICOS (Population, Intervention, Comparison, Outcome, Study Design) criteria, which were used in this evaluation, encompass population, intervention, comparison, outcomes, and study design (Table 1).

Table 1.
PICOS criteria.
Quality Assessment
The quality of the included papers was assessed by two reviewers, R.F. and E.I., using the ROBINS, which is a tool developed to assess risk of bias in the results of non-randomized studies that compare health effects of two or more interventions. Seven points were evaluated and each was assigned a degree of bias. A third reviewer (FI) was consulted in the event of a disagreement until an agreement was reached.
3. Results
3.1. Selection and Characteristics of This Study
A total of 949 papers were found in the online databases (Web of Science n = 282, PubMed n = 337, and Scopus n = 329) using the Boolean keywords “enamel” AND “orthodontic debonding” as the search string; After removing 450 duplicates, 499 studies were taken into consideration by reading the title and abstract, focusing on the different techniques and the variation in enamel structure after the debonding procedure. This analysis led to the selection of 40 records out of 499 papers, whereas 459 articles were excluded for different reasons (229 off topic, 20 reviews, 150 in vitro, 20 on animals). Subsequently, 21 non-retrieved records were excluded because texts were not available. After reading the full texts of the remaining 19 reports eligible, 5 more reports were excluded (1 was not free and 4 were off topic). Finally, 14 papers were chosen for the systematic review. Figure 2 summarizes the selection procedure. The study data were selected by analyzing the study design, patients, type of intervention, and outcomes (Table 2).
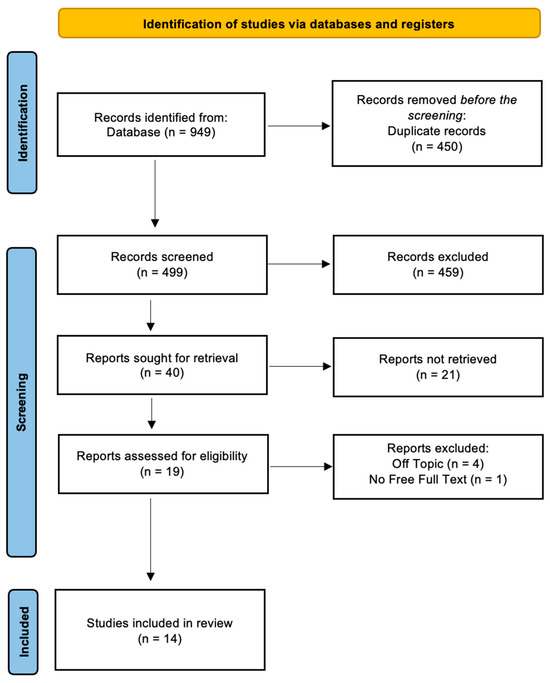
Figure 2.
PRISMA ScR flowchart diagram of the inclusion process.
Table 2.
Descriptive summary of the included studies.
Quality Assessment and Risk of Bias
The risk of bias in the included studies is reported in Figure 3. Regarding the bias due to confounding, most studies had a high risk. The bias arising from measurement was a parameter with a low risk of bias. Many studies had a low risk of bias due to bias in their selection of participants. Bias due to post-exposure could not be calculated due to high heterogeneity. The bias due to missing data was low in many studies. Bias arising from measurement of the outcome was low. Bias in the selection of the reported results was high in most studies. The final results showed that 10 studies had a high risk of bias, 3 had a very high risk of bias, and 8 had a low risk of bias.
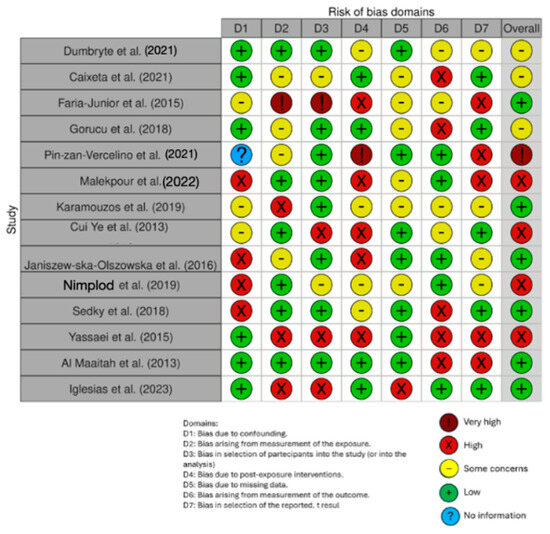
Figure 3.
Evaluation of bias by ROBINS: Dumbryte et al. (2021) [48]; Caixeta et al. (2021) [49]; Faria-Junior et al. (2015) [50]; Gorucu et al. (2018) [51]; Pin-zan-Vercelino et al. (2021) [52]; Malekpour et al. (2022) [53]; Karamouzos et al (2019) [54]; Cui Ye et al. (2013) [55]; Janiszew-ska-Olszowska et al. (2016) [56]; Nimplod et al (2019) [57]; Sedky et al (2018) [58]; Yassaei et al. (2015) [59]; Al Maaitah et al. (2013) [60]; Iglesias et al. (2023) [61].
4. Discussion
The application of fixed orthodontic devices requires a tooth surface preparation procedure that inevitably modifies the enamel structure. This alteration includes the formation of cracks, the loss of the fluoride-rich surface layer, the presence of residual adhesive residue, and surface roughening, leading to the accumulation of plaque [62,63,64,65,66].
4.1. Microcracks
Due to the challenging clinical detection of enamel fractures, controlled surface cracks were intentionally created before attaching brackets to explore the impact of debonding shear stress on cracks associated with both metal and ceramic brackets, with or without indentations. Despite utilizing the same loading method, variations were observed in the size and configuration of the controlled microcracks in this investigation, encompassing features such as crack branching, fracture bridging, and crack bifurcation. This diversity might have been influenced by the distinct mechanical behaviors at the dentin–enamel junction-to-enamel surface and enamel prism orientations.
According to the studies, enamel fractures occurred in 13.3% of debonded ceramic brackets, particularly in samples exhibiting an exceptionally high debonding strength exceeding 40 MPa. The elevated shear bond strength noted in this investigation could be attributed to the preparation of the enamel surface. It seems that polishing enamel before installing or repositioning ceramic brackets should be avoided, as it led to a higher incidence of enamel fractures upon the removal of ceramic brackets compared to metal brackets.
The spontaneous repair of enamel microcracks is a common phenomenon in live teeth, safeguarding against crack propagation to the dentin and dental pulp, and this reparative process was also observed in extracted teeth, as mentioned in the studies [57,58,59,60,61,62,63,64,65,66,67,68].
In a clinical trial conducted in 2021, Dumbryte et al. investigated the presence of enamel microcracks (EMCs) on teeth during debonding. The study involved 13 participants who displayed visible EMCs before the initiation of therapy and 13 individuals who did not have EMCs before undergoing treatment with metal brackets. Following the debonding process, 25% of the teeth exhibited apparent EMCs. Notably, patients who had pre-existing EMCs before treatment experienced three times the level of cold sensitivity compared to those without EMCs prior to therapy [48,69,70].
4.2. Surface Roughness
Physiologically, the microstructure of teeth determines their micro-roughness [8,71].
In 2021, Caixeta et al. conducted an in vivo study involving 15 patients undergoing fixed orthodontic treatment. Brackets were bonded using traditional composite resin in some subjects and resin-modified glass ionomer cement (RMGIC) in others. Examination of epoxy resin models of the teeth before and after debonding revealed that, following polishing, both the composite and RMGIC groups exhibited comparable surface roughness (SR). The choice between composite and RMGIC materials did not impact enamel SR in either group, but the values were significantly reduced after polishing compared to the initial condition. In both instances, the smoother surfaces post-polishing were more apparent than at the beginning of the treatment [49,72].
In a study conducted in 2015, Faria-Junior et al. assessed the surface roughness (SR) and morphology of enamel after the polishing and removal of metal brackets, utilizing an SR tester and scanning electron microscopy. Ten orthodontic patients were included in the study. Upon completing their orthodontic treatment, metal brackets were removed, and a randomly selected tooth underwent finishing and polishing with either aluminum oxide disks or multi-laminated carbide burs. Dental replicas of teeth, both before and after polishing, were created using epoxy resin. Statistical methods were employed to analyze the data obtained from various SR measurements, and scanning electron microscopy was utilized to examine three samples from each group.
In comparison with aluminum oxide, the carbide bur group exhibited a significantly higher average roughness [50,73].
Using a confocal laser microscope at a magnification of 1080×, the buccal surfaces of 45 extracted human third molars were scrutinized, and 3D roughness characteristics were ascertained. Molar tubes were affixed after a 20 s etching, and the teeth were subsequently immersed in a 0.9% saline solution for 24 h before undergoing debonding. In 15 different specimens, any remaining adhesive was eliminated using a 12-fluted tungsten carbide bur, a one-step finisher and polisher, and adhesive residue remover. Subsequently, the analysis of surface roughness (SR) was repeated.
The roughness of enamel was found to increase due to orthodontic debonding and the removal of adhesive residue. The adhesive residue remover resulted in the smoothest surfaces, while the tungsten carbide bur yielded the roughest surfaces [56].
The assessment of the Adhesive Remnant Index (ARI) under the surgical microscope in Sedky et al.’s study revealed that employing the Er,Cr:YSGG laser (2.78 μm, 6 W, 20 Hz, 60 μs pulse duration) compared to traditional bracket removal techniques (using a specialized plier), despite necessitating longer application times and treatment durations, resulted in more effective bracket removal. This was achieved by minimizing the amount of adhesive residue and expediting the finishing and polishing phase [58].
In Yassaei’s study, the Er:YAG laser operating at 2.94 μm, 20 Hz, 125 mJ, and 2.5 W, and positioned at a distance of 5 mm, was utilized post-debonding with pliers to eliminate excess adhesive. This was compared to the use of a tungsten carbide bur or a zircon-rich glass-fiber-reinforced composite bur. Ninety teeth were treated using one of these three methods. SEM observations revealed that, contrary to findings reported by Almeida et al., the laser produced the most uneven surface after adhesive removal, while the composite bur resulted in the absolute smoothest surface [14,73,74,75,76]. While the tungsten carbide bur removed adhesive residue more rapidly than the other two methods, though not significantly faster, it caused a temperature increase of 5.5 °C at a significantly slower rate compared to the reinforced composite bur. The laser method resulted in the smallest temperature increase [59,77].
Forty-five extracted premolars were categorized into three groups based on the polishing bur used after debonding, with four specimens serving as the control group. A gold chain measuring 0.038 by 0.015 inches was bonded and subsequently extracted between the premolars. Group 1 utilized a white stone at high speed, Group 2 employed a high-speed handpiece with a 30-blade tungsten carbide bur, and Group 3 utilized a low-speed handpiece and a 30-blade tungsten bur to eliminate adhesive residue. All samples underwent examination using a confocal microscope to assess surface roughness (SR) characteristics after debonding and polishing.
The debonded enamel surface exhibited increased roughness compared to the enamel of control teeth, irrespective of the polishing bur used. There was variability in enamel roughness after debonding based on the polishing technique, with the 30-blade tungsten carbide bur, particularly when used at a low speed, resulting in a smoother surface. For the purpose of maintaining long-term teeth alignment, the binding strength between the tooth and the composite pad, as well as the retention wire, was deemed optimal. Given that each approach examined increased the SR of the treated enamel, further research into remineralization processes is warranted [61].
4.3. Color Changes
Enamel color alterations represent one of the most common and undesirable outcomes of fixed orthodontic treatment. The fluctuation in tooth surface color is intricately linked to the employed surface cleaning and polishing procedure designed to eliminate residual materials. Nevertheless, the use of various rotary instruments, particularly diamond burs in grinding, inevitably leads to enamel surface reduction and subsequent color changes [33,78,79].
In a clinical study conducted by Gorucu et al. in 2018, the appearance of enamel post-debonding was evaluated by categorizing a sample of 59 patients into four groups. Various enamel etching techniques and two distinct tungsten carbide burs were employed across these groups. The study’s results are noteworthy: despite the use of different etching and adhesive removal methods, observable and clinically undesirable changes in tooth color were noted following orthodontic treatment. Neither conventional nor self-etching techniques exhibited statistically significant differences in altering tooth color [51].
The introduction of increasingly high-performance polishing systems appears to yield promising outcomes. In their 2020 clinical study, Pinzan-Vercelino et al. assessed the surface roughness (SR) and color change of enamel following bracket detachment and polishing with two different systems. A 12-blade tungsten carbide bur on a low-speed handpiece was utilized for adhesive removal, followed by the application of Sof-Lex spiral wheels and disks in a random polishing process. Dental replicas were created using epoxy resin, polished, and attached with adhesive. Neither system significantly harmed dental enamel, as both color and roughness were equally affected. Both methods successfully restored the enamel, bringing it as close as possible to its initial state [52].
The 2022 study conducted by Malekpour et al. investigated the influence of nano-hydroxyapatite serum and various polishing and finishing methods on enamel discoloration resulting from post-orthodontic debonding procedures. The study compared the use of carbide burs alone (the standard procedure) with the combined use of carbide burs and Sof-Lex disks, followed by 10 days of nano-hydroxyapatite application post-debonding. Enamel coloration was then measured using a spectrophotometer. Clinically notable color changes were observed on average across all groups and intervals. Unlike Sof-Lex disks, which were found to significantly reduce tooth color changes shortly after debonding, the use of nano-hydroxyapatite showed no appreciable impact in terms of slowing these changes [53].
A total of 120 extracted teeth were subjected to coffee immersion after bracket removal. Subsequently, they underwent random polishing using four different techniques and were examined using a spectrophotometer. Teeth treated solely with a diamond bur exhibited a higher level of discoloration, attributed to increased aggressiveness and residual surface roughness (SR), leading to enhanced retention of potentially pigmented substances. The combination of the bur with other tools significantly reduced the discoloration rate. The most favorable outcomes were achieved when employing diamond burs in conjunction with polymerized urethane dimethacrylate resin, fine diamond powder, and silicon oxide (PoGo) cups, disks, and tips, followed by disks reverted by aluminum oxide. In contrast, the combination of burs and the OneGloss Polisher did not yield excellent results compared to the other two combined protocols [33,55].
Al Maaitah’s study aimed to evaluate the impact of fixed orthodontic treatment, etching techniques (self-etching and conventional), and various parameters (age, gender, tooth type) on tooth color. The Commission Internationale de l’Eclairage color scheme was employed to determine instrumental tooth shade before and after orthodontic treatment. The researchers identified statistically significant changes in color characteristics post-treatment, with teeth darkening and trending towards reddish–yellowish hues. The choice of etching technique (self-etching or conventional) did not affect the observed color alterations. Male patients and teenagers exhibited more pronounced color changes, possibly linked to their dietary habits, dental hygiene practices, and enamel characteristics [60,79].
The 2019 clinical study by Karamouzos et al. also showed that teeth undergo color change at the end of fixed orthodontic therapy; in particular, the greatest change was found during the first 3 months in teeth on which high-speed rotary instruments were used during debonding [48,54].
The studies that we reviewed had various limitations:
Heterogeneity in study designs: The studies analyzed encompass a diverse range of designs, including case–control, observational, retrospective, and prospective studies. Dental element analysis was conducted in vivo or after extraction. The incorporation of different designs may introduce heterogeneity, potentially compromising the reliability of the review’s findings.
Small sample sizes: Some of the included research has small sample sizes, which may limit the statistical power and generalizability of the results.
Lack of quality assessment: The review does not specify whether the included studies underwent quality assessment. Evaluating the methodological quality of the studies is crucial to determine the overall dependability of the evidence.
Limited scope of analysis: The review primarily focuses on enamel modification after debonding, analyzing various techniques and procedures. However, it does not address other potential complications affecting the tooth, such as variations in temperature within the pulpar chamber.
Further studies are essential to establish standardized and increasingly effective debonding protocols.
5. Conclusions
In conclusion, the use of fixed orthodontic appliances has several adverse effects on dental enamel, including the development of microcracks, surface roughness, and alterations in color. Ceramic brackets, particularly when excessive tooth surface preparation precedes bonding, are often linked to a higher incidence of enamel fracture.
Surface roughness in enamel can be affected by various factors, such as the type of adhesive material used and the polishing procedure after debonding. While the use of a low-speed tungsten carbide bur has shown effectiveness in reducing roughness, all polishing methods contribute to increased roughness, highlighting the need for further investigation into remineralization techniques.
Fixed orthodontic treatment may also result in undesirable changes in tooth color. Some studies have explored methods to mitigate these changes, such as the application of nano-hydroxyapatite or specific polishing systems, although success is not always guaranteed.
Age, gender, tooth type, and patient behaviors collectively influence the degree of color change during orthodontic treatment. These findings emphasize the importance of carefully evaluating the materials and techniques used in orthodontic procedures to minimize adverse effects on tooth enamel, such as microcracks, surface roughness, and color alterations. Further research is essential to discover approaches that mitigate these side effects while maintaining therapeutic effectiveness.
Author Contributions
Conceptualization, A.P., A.M.I. and A.D.I.; methodology, F.I., G.D. and D.D.V.; software, R.M., L.R. and R.S.; validation, A.P., M.C. and F.I.; formal analysis, A.M.I. and D.D.V.; investigation, A.D.I. and D.D.V.; resources, G.D.; data curation, L.R. and R.M.; writing—original draft preparation, R.S. and D.D.V.; writing—review and editing, F.I.; visualization, A.D.I.; supervision, A.P., F.I. and M.C; project administration, A.M.I., M.C. and D.D.V.; funding acquisition, A.P., L.R., R.M. and R.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ARI | Adhesive Remnant Index |
| EMC | enamel microcrack |
| RMGIC | Resin-modified glass ionomer cement |
| SR | surface roughness |
References
- Campbell, P.M. Enamel Surfaces after Orthodontic Bracket Debonding. Angle Orthod. 1995, 65, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Herrera-Barraza, V.; Arroyo-Larrondo, S.; Fernández-Córdova, M.; Catricura-Cerna, D.; Garrido-Urrutia, C.; Ferrer-Valdivia, N. Complications Post Simple Exodontia: A Systematic Review. Dent. Med. Probl. 2022, 59, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.E.; Way, D.C. Enamel Loss Due to Prophylaxis and Multiple Bonding/Debonding of Orthodontic Attachments. Am. J. Orthod. 1981, 79, 282–295. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Abenavoli, F.M.; Marrelli, M.; Inchingolo, A.D.; Palladino, A.; Inchingolo, A.M.; Dipalma, G. Oral Piercing and Oral Diseases: A Short Time Retrospective Study. Int. J. Med. Sci. 2011, 8, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Ronsivalle, V.; Cicciù, M. Children Oral Health and Parents Education Status: A Cross Sectional Study. BMC Oral Health 2023, 23, 787. [Google Scholar] [CrossRef]
- Osorio, R.; Toledano, M.; García-Godoy, F. Enamel Surface Morphology after Bracket Debonding. ASDC J. Dent. Child. 1998, 65, 313–317+354. [Google Scholar]
- Eslamian, L.; Borzabadi-Farahani, A.; Tavakol, P.; Tavakol, A.; Amini, N.; Lynch, E. Effect of Multiple Debonding Sequences on Shear Bond Strength of New Stainless Steel Brackets. J. Orthod. Sci. 2015, 4, 37. [Google Scholar] [CrossRef]
- Fjeld, M.; Øgaard, B. Scanning Electron Microscopic Evaluation of Enamel Surfaces Exposed to 3 Orthodontic Bonding Systems. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Malcangi, G.; Sardano, R.; Mastrodonato, A.; Garofoli, G.; Mancini, A.; Inchingolo, A.D.; Di Venere, D.; Inchingolo, F.; Dipalma, G.; et al. White Spots: Prevention in Orthodontics-Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2023, 20, 5608. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. The Association between Parent Education Level, Oral Health, and Oral-Related Sleep Disturbance. An Observational Crosssectional Study. Eur. J. Paediatr. Dent. 2023, 24, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Ulusoy, C. Comparison of Finishing and Polishing Systems for Residual Resin Removal after Debonding. J. Appl. Oral Sci. Rev. 2009, 17, 209–215. [Google Scholar] [CrossRef]
- Zaher, A.R.; Abdalla, E.M.; Abdel Motie, M.A.; Rehman, N.A.; Kassem, H.; Athanasiou, A.E. Enamel Colour Changes after Debonding Using Various Bonding Systems. J. Orthod. 2012, 39, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Eslamian, L.; Borzabadi-Farahani, A.; Mousavi, N.; Ghasemi, A. A Comparative Study of Shear Bond Strength between Metal and Ceramic Brackets and Artificially Aged Composite Restorations Using Different Surface Treatments. Eur. J. Orthod. 2012, 34, 610–617. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Marangoni, R.D.; Flint, W. In Vitro Comparison of Debonding Force and Intrapulpal Temperature Changes during Ceramic Orthodontic Bracket Removal Using a Carbon Dioxide Laser. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Janiszewska-Olszowska, J.; Tandecka, K.; Szatkiewicz, T.; Sporniak-Tutak, K.; Grocholewicz, K. Three-Dimensional Quantitative Analysis of Adhesive Remnants and Enamel Loss Resulting from Debonding Orthodontic Molar Tubes. Head Face Med. 2014, 10, 37. [Google Scholar] [CrossRef] [PubMed]
- Ryf, S.; Flury, S.; Palaniappan, S.; Lussi, A.; van Meerbeek, B.; Zimmerli, B. Enamel Loss and Adhesive Remnants following Bracket Removal and Various Clean-Up Procedures In Vitro. Eur. J. Orthod. 2012, 34, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Patano, A.; Malcangi, G.; De Santis, M.; Morolla, R.; Settanni, V.; Piras, F.; Inchingolo, A.D.; Mancini, A.; Inchingolo, F.; Dipalma, G.; et al. Conservative Treatment of Dental Non-Carious Cervical Lesions: A Scoping Review. Biomedicines 2023, 11, 1530. [Google Scholar] [CrossRef]
- Giorgini, E.; Sabbatini, S.; Conti, C.; Rubini, C.; Rocchetti, R.; Fioroni, M.; Memè, L.; Orilisi, G. Fourier Transform Infrared Imaging Analysis of Dental Pulp Inflammatory Diseases. Oral Dis. 2017, 23, 484–491. [Google Scholar] [CrossRef]
- Almeida, L.E.; Cicciù, M.; Doetzer, A.; Beck, M.L.; Cervino, G.; Minervini, G. Mandibular Condylar Hyperplasia and Its Correlation with Vascular Endothelial Growth Factor. J. Oral Rehabil. 2023, 50, 845–851. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Fiorillo, L.; Cervino, G.; Cicciù, M. Post-traumatic Stress, Prevalence of Temporomandibular Disorders in War Veterans: Systematic Review with Meta-analysis. J. Oral Rehabil. 2023, 50, 1101–1109. [Google Scholar] [CrossRef]
- Burapavong, V.; Marshall, G.W.; Apfel, D.A.; Perry, H.T. Enamel Surface Characteristics on Removal of Bonded Orthodontic Brackets. Am. J. Orthod. 1978, 74, 176–187. [Google Scholar] [CrossRef]
- Alessandri Bonetti, G.; Zanarini, M.; Incerti Parenti, S.; Lattuca, M.; Marchionni, S.; Gatto, M.R. Evaluation of Enamel Surfaces after Bracket Debonding: An In-Vivo Study with Scanning Electron Microscopy. Am. J. Orthod. Dentofac. Orthop. 2011, 140, 696–702. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Almeida, L.E.; Ronsivalle, V.; Cicciù, M. Prevalence of Temporomandibular Disorders (TMD) in Obesity Patients: A Systematic Review and Meta-Analysis. J. Oral Rehabil. 2023, 50, 1544–1553. [Google Scholar] [CrossRef] [PubMed]
- miHabibi, M.; Nik, T.H.; Hooshmand, T. Comparison of Debonding Characteristics of Metal and Ceramic Orthodontic Brackets to Enamel: An In-Vitro Study. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 675–679. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.M.; Joseph, V.P.; Rossouw, P.E. Shear Peel Bond Strengths of Esthetic Orthodontic Brackets. Am. J. Orthod. Dentofac. Orthop. 1992, 102, 215–219. [Google Scholar] [CrossRef]
- Joseph, V.P.; Rossouw, E. The Shear Bond Strengths of Stainless Steel and Ceramic Brackets Used with Chemically and Light-Activated Composite Resins. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Di Blasio, M.; Isola, G.; Cicciù, M. Conservative Treatment of Temporomandibular Joint Condylar Fractures: A Systematic Review Conducted According to PRISMA Guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. J. Oral Rehabil. 2023, 50, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef]
- Odegaard, J.; Segner, D. Shear Bond Strength of Metal Brackets Compared with a New Ceramic Bracket. Am. J. Orthod. Dentofac. Orthop. 1988, 94, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Kitahara-Céia, F.M.F.; Mucha, J.N.; Marques dos Santos, P.A. Assessment of Enamel Damage after Removal of Ceramic Brackets. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 548–555. [Google Scholar] [CrossRef]
- Wang, W.N.; Meng, C.L.; Tarng, T.H. Bond Strength: A Comparison between Chemical Coated and Mechanical Interlock Bases of Ceramic and Metal Brackets. Am. J. Orthod. Dentofac. Orthop. 1997, 111, 374–381. [Google Scholar] [CrossRef]
- Lucchese, A.; Porcù, F.; Dolci, F. Effects of Various Stripping Techniques on Surface Enamel. J. Clin. Orthod. 2001, 35, 691–695. [Google Scholar] [PubMed]
- Bishara, S.E.; Olsen, M.E.; VonWald, L.; Jakobsen, J.R. Comparison of the Debonding Characteristics of Two Innovative Ceramic Bracket Designs. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Marrapodi, M.M.; Cicciù, M. Online Bruxism-related Information: Can People Understand What They Read? A Cross-Sectional Study. J. Oral Rehabil. 2023, 50, 1211–1216. [Google Scholar] [CrossRef] [PubMed]
- Janiszewska-Olszowska, J.; Szatkiewicz, T.; Tomkowski, R.; Tandecka, K.; Grocholewicz, K. Effect of Orthodontic Debonding and Adhesive Removal on the Enamel–Current Knowledge and Future Perspectives—A Systematic Review. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2014, 20, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Boyer, D.B.; Engelhardt, G.; Bishara, S.E. Debonding Orthodontic Ceramic Brackets by Ultrasonic Instrumentation. Am. J. Orthod. Dentofac. Orthop. 1995, 108, 262–266. [Google Scholar] [CrossRef]
- Brosh, T.; Kaufman, A.; Balabanovsky, A.; Vardimon, A.D. In Vivo Debonding Strength and Enamel Damage in Two Orthodontic Debonding Methods. J. Biomech. 2005, 38, 1107–1113. [Google Scholar] [CrossRef]
- Oliver, R.G.; Griffiths, J. Different Techniques of Residual Composite Removal Following Debonding--Time Taken and Surface Enamel Appearance. Br. J. Orthod. 1992, 19, 131–137. [Google Scholar] [CrossRef]
- Almudhi, A.; Aldeeri, A.; Aloraini, A.A.A.; Alomar, A.I.M.; Alqudairi, M.S.M.; Alzahrani, O.A.A.; Eldwakhly, E.; AlMugairin, S. Comparison of Enamel Surface Integrity after De-Bracketing as Affected by Seven Different Orthodontic Residual Cement Removal Systems. Diagnostics 2023, 13, 3284. [Google Scholar] [CrossRef]
- Isacco, C.G.; Ballini, A.; De Vito, D.; Nguyen, K.C.D.; Cantore, S.; Bottalico, L.; Quagliuolo, L.; Boccellino, M.; Di Domenico, M.; Santacroce, L.; et al. Rebalancing the Oral Microbiota as an Efficient Tool in Endocrine, Metabolic and Immune Disorders. Endocr. Metab. Immune Disord.-Drug Targets 2021, 21, 777–784. [Google Scholar] [CrossRef]
- Malcangi, G.; Patano, A.; Morolla, R.; De Santis, M.; Piras, F.; Settanni, V.; Mancini, A.; Di Venere, D.; Inchingolo, F.; Inchingolo, A.D.; et al. Analysis of Dental Enamel Remineralization: A Systematic Review of Technique Comparisons. Bioengineering 2023, 10, 472. [Google Scholar] [CrossRef]
- Malcangi, G.; Inchingolo, A.D.; Patano, A.; Coloccia, G.; Ceci, S.; Garibaldi, M.; Inchingolo, A.M.; Piras, F.; Cardarelli, F.; Settanni, V.; et al. Impacted Central Incisors in the Upper Jaw in an Adolescent Patient: Orthodontic-Surgical Treatment—A Case Report. Appl. Sci. 2022, 12, 2657. [Google Scholar] [CrossRef]
- Eichenberger, M.; Iliadi, A.; Koletsi, D.; Eliades, G.; Verna, C.; Eliades, T. Enamel Surface Roughness after Lingual Bracket Debonding: An In Vitro Study. Materials 2019, 12, 4196. [Google Scholar] [CrossRef]
- Webb, B.J.; Koch, J.; Hagan, J.L.; Ballard, R.W.; Armbruster, P.C. Enamel Surface Roughness of Preferred Debonding and Polishing Protocols. J. Orthod. 2016, 43, 39–46. [Google Scholar] [CrossRef]
- Goldoni, R.; Dolci, C.; Boccalari, E.; Inchingolo, F.; Paghi, A.; Strambini, L.; Galimberti, D.; Tartaglia, G.M. Salivary Biomarkers of Neurodegenerative and Demyelinating Diseases and Biosensors for Their Detection. Ageing Res. Rev. 2022, 76, 101587. [Google Scholar] [CrossRef]
- Heravi, F.; Shafaee, H.; Abdollahi, M.; Rashed, R. How Is the Enamel Affected by Different Orthodontic Bonding Agents and Polishing Techniques? J. Dent. 2015, 12, 188. [Google Scholar]
- The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/19622552/ (accessed on 12 October 2023).
- Dumbryte, I.; Malinauskas, M. In Vivo Examination of Enamel Microcracks after Orthodontic Debonding: Is There a Need for Detailed Analysis? Am. J. Orthod. Dentofac. Orthop. 2021, 159, e103–e111. [Google Scholar] [CrossRef]
- Caixeta, R.V.; Berger, S.B.; Lopes, M.B.; Paloco, E.A.C.; Faria, É.M., Jr.; Contreras, E.F.R.; Gonini-Júnior, A.; Guiraldo, R.D. Evaluation of Enamel Roughness after the Removal of Brackets Bonded with Different Materials: In Vivo Study. Braz. Dent. J. 2021, 32, 34–40. [Google Scholar] [CrossRef]
- Faria, É.M., Jr.; Guiraldo, R.D.; Berger, S.B.; Correr, A.B.; Correr-Sobrinho, L.; Contreras, E.F.R.; Lopes, M.B. In-Vivo Evaluation of the Surface Roughness and Morphology of Enamel after Bracket Removal and Polishing by Different Techniques. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 324–329. [Google Scholar] [CrossRef]
- Gorucu-Coskuner, H.; Atik, E.; Taner, T. Tooth Color Change Due to Different Etching and Debonding Procedures. Angle Orthod. 2018, 88, 779–784. [Google Scholar] [CrossRef]
- Pinzan-Vercelino, C.R.M.; Souza Costa, A.C.; Gurgel, J.A.; Salvatore Freitas, K.M. Comparison of Enamel Surface Roughness and Color Alteration after Bracket Debonding and Polishing with 2 Systems: A Split-Mouth Clinical Trial. Am. J. Orthod. Dentofac. Orthop. 2021, 160, 686–694. [Google Scholar] [CrossRef]
- Malekpour, B.; Ajami, S.; Salehi, P.; Hamedani, S. Use of Nano-Hydroxyapatite Serum and Different Finishing/Polishing Techniques to Reduce Enamel Staining of Debonding after Orthodontic Treatment: A Randomized Clinical Trial. J. Orofac. Orthop./Fortschritte Der Kieferorthopädie 2022, 83, 205–214. [Google Scholar] [CrossRef]
- Karamouzos, A.; Zafeiriadis, A.A.; Kolokithas, G.; Papadopoulos, M.A.; Athanasiou, A.E. In Vivo Evaluation of Tooth Colour Alterations during Orthodontic Retention: A Split-Mouth Cohort Study. Orthod. Craniofac. Res. 2019, 22, 124–130. [Google Scholar] [CrossRef]
- Ye, C.; Zhao, Z.; Zhao, Q.; Du, X.; Ye, J.; Wei, X. Comparison of Enamel Discoloration Associated with Bonding with Three Different Orthodontic Adhesives and Cleaning-up with Four Different Procedures. J. Dent. 2013, 41 (Suppl. S5), e35–e40. [Google Scholar] [CrossRef]
- Janiszewska-Olszowska, J.; Tomkowski, R.; Tandecka, K.; Stepien, P.; Szatkiewicz, T.; Sporniak-Tutak, K.; Grocholewicz, K. Effect of Orthodontic Debonding and Residual Adhesive Removal on 3D Enamel Microroughness. PeerJ 2016, 4, e2558. [Google Scholar] [CrossRef]
- Nimplod, P.; Tansalarak, R.; Sornsuwan, T. Effect of the Different Debonding Strength of Metal and Ceramic Brackets on the Degree of Enamel Microcrack Healing. Dent. Press J. Orthod. 2021, 26, e2119177. [Google Scholar] [CrossRef]
- Sedky, Y.; Gutknecht, N. The Effect of Using Er,Cr:YSGG Laser in Debonding Stainless Steel Orthodontic Brackets: An in Vitro Study. Lasers Dent. Sci. 2018, 2, 13–18. [Google Scholar] [CrossRef]
- Yassaei, S.; Aghili, H.; Joshan, N. Effects of Removing Adhesive from Tooth Surfaces by Er:YAG Laser and a Composite Bur on Enamel Surface Roughnessand Pulp Chamber Temperature. Dent. Res. J. 2015, 12, 254–259. [Google Scholar]
- Al Maaitah, E.F.; Abu Omar, A.A.; Al-Khateeb, S.N. Effect of Fixed Orthodontic Appliances Bonded with Different Etching Techniques on Tooth Color: A Prospective Clinical Study. Am. J. Orthod. Dentofac. Orthop. 2013, 144, 43–49. [Google Scholar] [CrossRef]
- Iglesias, A.; Flores, T.; Moyano, J.; Artés, M.; Botella, N.; Gil, J.; Puigdollers, A. Enamel Evaluation after Debonding of Fixed Retention and Polishing Treatment with Three Different Methods. Materials 2023, 16, 2403. [Google Scholar] [CrossRef]
- Rix, D.; Foley, T.F.; Mamandras, A. Comparison of Bond Strength of Three Adhesives: Composite Resin, Hybrid GIC, and Glass-Filled GIC. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 36–42. [Google Scholar] [CrossRef]
- Merone, G.; Valletta, R.; De Santis, R.; Ambrosio, L.; Martina, R. A novel bracket base design: Biomechanical stability. Eur. J. Orthod. 2009, 32, 219–223. [Google Scholar] [CrossRef]
- Al Shamsi, A.H.; Cunningham, J.L.; Lamey, P.J.; Lynch, E. Three-Dimensional Measurement of Residual Adhesive and Enamel Loss on Teeth after Debonding of Orthodontic Brackets: An in-Vitro Study. Am. J. Orthod. Dentofac. Orthop. 2007, 131, e9–e15. [Google Scholar] [CrossRef] [PubMed]
- Karan, S.; Kircelli, B.H.; Tasdelen, B. Enamel Surface Roughness after Debonding. Angle Orthod. 2010, 80, 1081–1088. [Google Scholar] [CrossRef] [PubMed]
- Bollen, C.M.; Lambrechts, P.; Quirynen, M. Comparison of Surface Roughness of Oral Hard Materials to the Threshold Surface Roughness for Bacterial Plaque Retention: A Review of the Literature. Dent. Mater. 1997, 13, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Ijbara, M.; Wada, K.; Tabata, M.J.; Wada, J.; Inoue, G.; Miyashin, M. Enamel Microcracks Induced by Simulated Occlusal Wear in Mature, Immature, and Deciduous Teeth. Biomed. Res. Int. 2018, 2018, 5658393. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Suliman, S.N.; Trojan, T.M.; Tantbirojn, D.; Versluis, A. Enamel Loss Following Ceramic Bracket Debonding: A Quantitative Analysis in Vitro. Angle Orthod. 2015, 85, 651–656. [Google Scholar] [CrossRef]
- Cesur, E.; Arslan, C.; Orhan, A.I.; Bilecenoğlu, B.; Orhan, K. Effect of Different Resin Removal Methods on Enamel after Metal and Ceramic Bracket Debonding: An in Vitro Micro-Computed Tomography Study. J. Orofac. Orthop./Fortschritte Der Kieferorthopädie 2022, 83, 157–171. [Google Scholar] [CrossRef]
- Ghafari, J. Problems Associated with Ceramic Brackets Suggest Limiting Use to Selected Teeth. Angle Orthod. 1992, 62, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature–PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/35883998/ (accessed on 29 November 2023).
- Anaraki, S.N.; Shahabi, S.; Chiniforush, N.; Nokhbatolfoghahaei, H.; Assadian, H.; Yousefi, B. Evaluation of the Effects of Conventional versus Laser Bleaching Techniques on Enamel Microroughness. Lasers Med. Sci. 2015, 30, 1013–1018. [Google Scholar] [CrossRef] [PubMed]
- Pont, H.B.; Özcan, M.; Bagis, B.; Ren, Y. Loss of Surface Enamel after Bracket Debonding: An In-Vivo and Ex-Vivo Evaluation. Am. J. Orthod. Dentofac. Orthop. 2010, 138, 387.e1–387.e9. [Google Scholar] [CrossRef]
- Grzech-Leśniak, K.; Matys, J.; Żmuda-Stawowiak, D.; Mroczka, K.; Dominiak, M.; Brugnera Junior, A.; Gruber, R.; Romanos, G.E.; Sculean, A. Er:YAG Laser for Metal and Ceramic Bracket Debonding: An In Vitro Study on Intrapulpal Temperature, SEM, and EDS Analysis. Photomed. Laser Surg. 2018, 36, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Almeida, H.C.; Vedovello Filho, M.; Vedovello, S.A.S.; Young, A.A.A.; Ramirez-Yañez, G.O. ER: YAG Laser for Composite Removal after Bracket Debonding: A Qualitative SEM Analysis. Int. J. Orthod. 2009, 20, 9–13. [Google Scholar]
- Dostalova, T.; Jelinkova, H.; Remes, M.; Šulc, J.; Němec, M. The Use of the Er:YAG Laser for Bracket Debonding and Its Effect on Enamel Damage. Photomed. Laser Surg. 2016, 34, 394–399. [Google Scholar] [CrossRef]
- Mesaroș, A.; Mesaroș, M.; Buduru, S. Orthodontic Bracket Removal Using LASER-Technology-A Short Systematic Literature Review of the Past 30 Years. Materials 2022, 15, 548. [Google Scholar] [CrossRef] [PubMed]
- Marchi, R.; De-Marchi, L.; Terada, R.; Terada, H. Comparison between Two Methods for Resin Removing after Bracket Debonding. Dent. Press. J. Orthod. 2012, 17, 130–136. [Google Scholar] [CrossRef]
- Al Shamsi, A.; Cunningham, J.L.; Lamey, P.J.; Lynch, E. Shear Bond Strength and Residual Adhesive after Orthodontic Bracket Debonding. Angle Orthod. 2006, 76, 694–699. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).