
Effect of Antimicrobial Stewardship on Oral Quinolone Use and Resistance Patterns over 8 Years (2013–2020)

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Demographic Characteristics of Patients and Frequency of Oral Quinolone Prescriptions
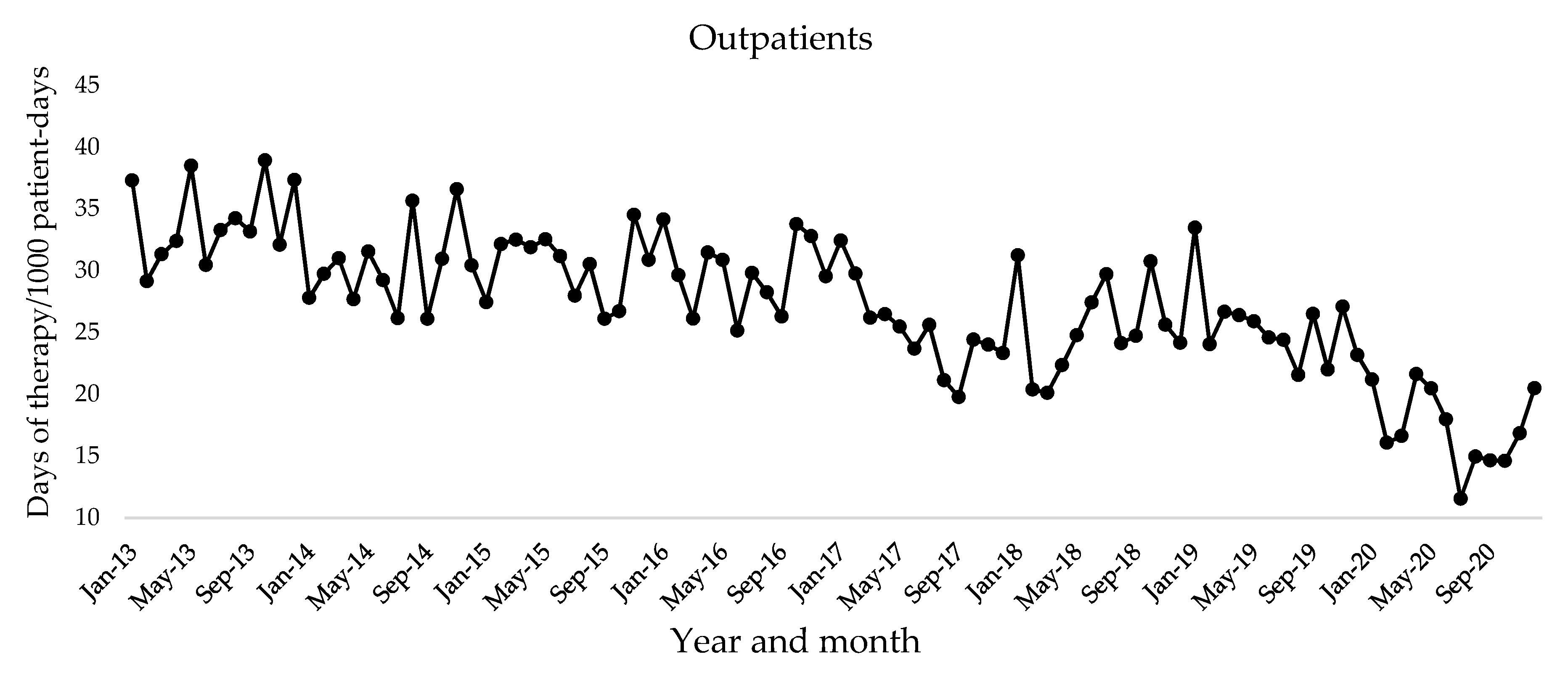
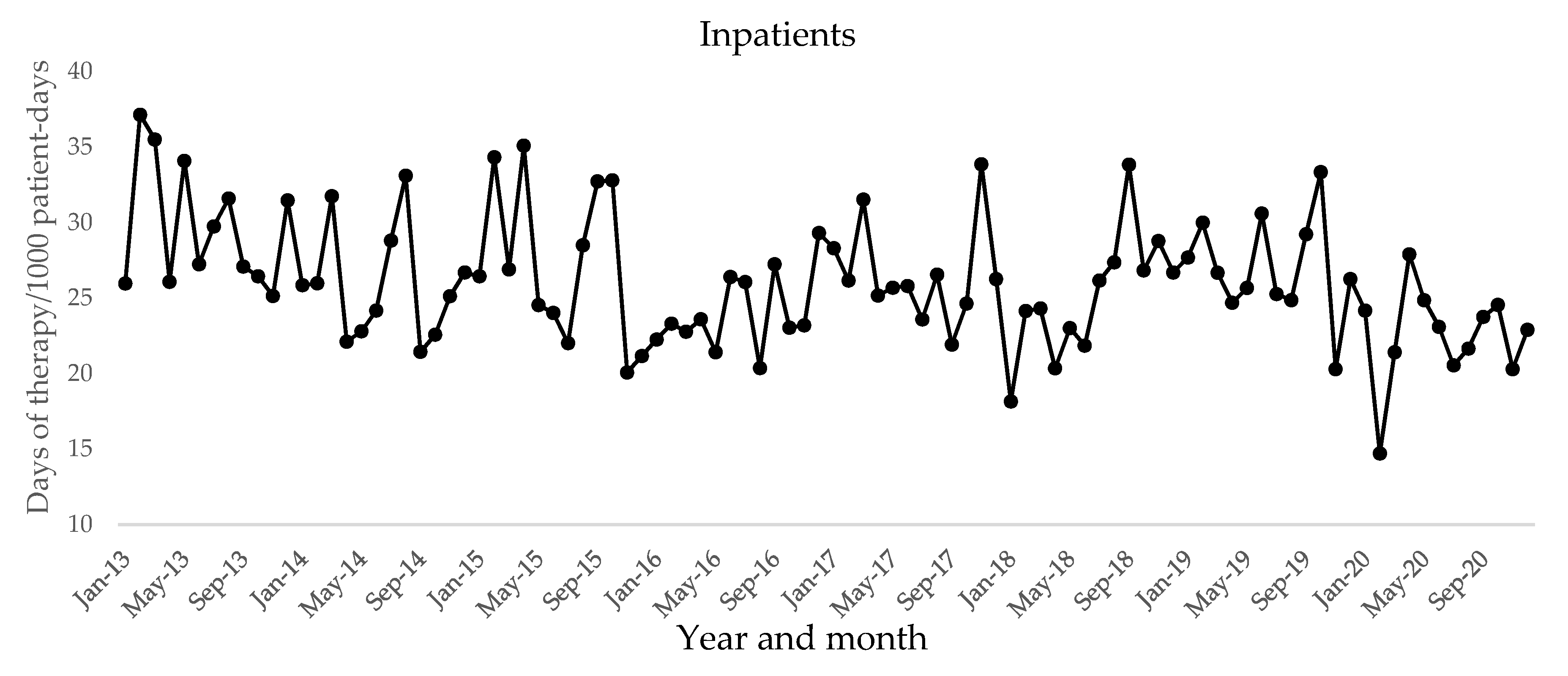
2.2. Antibiotic Use
2.3. Antibiotic Resistance
2.4. Clinical Outcomes for Outpatients
3. Discussion
4. Methods
4.1. Setting and Patients
4.2. Educational Intervention for Promoting Appropriate Antimicrobial Use
4.3. Outcomes
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations/the Review on Antimicrobial Resistance Chaired by Jim O’Neill. Available online: https://wellcomecollection.org/works/rdpck35v (accessed on 6 April 2021).
- World Health Organization, Regional Office for Europe. Global Action Plan on Antimicrobial Resistance; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Global Action Plan on Antimicrobial Resistance. 2015. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/antimicrobial-resistance/policy/global-action-plan-2015 (accessed on 2 September 2021).
- CDC U.S. National Action Plan for Combating Antibiotic-Resistant Bacteria (National Action Plan). Available online: https://www.cdc.gov/drugresistance/us-activities/national-action-plan.html (accessed on 2 September 2021).
- Japan: National Action Plan on Antimicrobial Resistance (AMR). Available online: https://www.who.int/publications/m/item/japan-national-action-plan-on-antimicrobial-resistance-(amr) (accessed on 26 August 2021).
- Manual of Antimicrobial Stewardship (1st Edition). Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/0000193504.pdf (accessed on 18 August 2021).
- Manual of Antimicrobial Stewardship (2nd Edition). Available online: https://www.mhlw.go.jp/content/10900000/000573655.pdf (accessed on 18 August 2021).
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Uda, A.; Shigemura, K.; Kitagawa, K.; Osawa, K.; Onuma, K.; Yan, Y.; Nishioka, T.; Fujisawa, M.; Yano, I.; Miyara, T. Risk factors for the acquisition of enterococcus faecium infection and mortality in patients with enterococcal bacteremia: A 5-year retrospective analysis in a tertiary care university hospital. Antibiotics 2021, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Aldred, K.J.; Kerns, R.J.; Osheroff, N. Mechanism of quinolone action and resistance. Biochemistry 2014, 53, 1565–1574. [Google Scholar] [CrossRef] [PubMed]
- Muraki, Y.; Yagi, T.; Tsuji, Y.; Nishimura, N.; Tanabe, M.; Niwa, T.; Watanabe, T.; Fujimoto, S.; Takayama, K.; Murakami, N.; et al. Japanese antimicrobial consumption surveillance: First report on oral and parenteral antimicrobial consumption in Japan (2009–2013). J. Glob. Antimicrob. Resist. 2016, 7, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Barlam, T.F.; Cosgrove, S.E.; Abbo, L.M.; MacDougall, C.; Schuetz, A.N.; Septimus, E.J.; Srinivasan, A.; Dellit, T.H.; Falck-Ytter, Y.T.; Fishman, N.O.; et al. Implementing an antibiotic stewardship program: Guidelines by the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Clin. Infect. Dis. 2016, 62, e51–e77. [Google Scholar] [CrossRef]
- Kimura, T.; Uda, A.; Sakaue, T.; Yamashita, K.; Nishioka, T.; Nishimura, S.; Ebisawa, K.; Nagata, M.; Ohji, G.; Nakamura, T.; et al. Long-term efficacy of comprehensive multidisciplinary antibiotic stewardship programs centered on weekly prospective audit and feedback. Infection 2018, 46, 215–224. [Google Scholar] [CrossRef] [Green Version]
- Lanbeck, P.; Ragnarson Tennvall, G.; Resman, F. A cost analysis of introducing an infectious disease specialist-guided antimicrobial stewardship in an area with relatively low prevalence of antimicrobial resistance. BMC Health Serv. Res. 2016, 16, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Uda, A.; Kimura, T.; Nishimura, S.; Ebisawa, K.; Ohji, G.; Kusuki, M.; Yahata, M.; Izuta, R.; Sakaue, T.; Nakamura, T.; et al. Efficacy of educational intervention on reducing the inappropriate use of oral third-generation cephalosporins. Infection 2019, 47, 1037–1045. [Google Scholar] [CrossRef]
- Guideline Committee for Practical Guidelines for the Appropriate Use of Prophylactic Antibiotics. Available online: http://www.chemotherapy.or.jp/guideline/jyutsugo_shiyou.html (accessed on 8 September 2021).
- Ling, M.L.; Apisarnthanarak, A.; Abbas, A.; Morikane, K.; Lee, K.Y.; Warrier, A.; Yamada, K. APSIC guidelines for the prevention of surgical site infections. Antimicrob. Resist. Infect. Control. 2019, 8, 174. [Google Scholar] [CrossRef]
- Kusumoto, J.; Uda, A.; Kimura, T.; Furudoi, S.; Yoshii, R.; Matsumura, M.; Miyara, T.; Akashi, M. Effect of educational intervention on the appropriate use of oral antimicrobials in oral and maxillofacial surgery: A retrospective secondary data analysis. BMC Oral Health 2021, 21, 20. [Google Scholar] [CrossRef]
- Mayumi, T.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Solomkin, J.S.; Schlossberg, D.; Pitt, H.A.; Yoshida, M.; Gomi, H.; Miura, F.; et al. Tokyo guidelines 2018: Management bundles for acute cholangitis and cholecystitis. J. Hepato-Biliary-Pancreat. Sci. 2018, 25, 96–100. [Google Scholar] [CrossRef] [PubMed]
- Sartelli, M.; Weber, D.G.; Ruppé, E.; Bassetti, M.; Wright, B.J.; Ansaloni, L.; Catena, F.; Coccolini, F.; Abu-Zidan, F.M.; Coimbra, R.; et al. Antimicrobials: A Global Alliance for Optimizing Their Rational Use in Intra-Abdominal Infections (AGORA). World J. Emerg. Surg. 2016, 11, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamasaki, D.; Tanabe, M.; Muraki, Y.; Kato, G.; Ohmagari, N.; Yagi, T. The first report of japanese antimicrobial use measured by national database based on health insurance claims data (2011–2013): Comparison with sales data, and trend analysis stratified by antimicrobial category and age group. Infection 2018, 46, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Talan, D.A.; Takhar, S.S.; Krishnadasan, A.; Abrahamian, F.M.; Mower, W.R.; Moran, G.J. Fluoroquinolone-Resistant and Extended-Spectrum β-Lactamase–Producing Escherichia Coli Infections in Patients with Pyelonephritis, United States1. Emerg. Infect. Dis. 2016, 22, 1594–1603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camins, B.C.; Marschall, J.; DeVader, S.R.; Maker, D.E.; Hoffman, M.W.; Fraser, V.J. The clinical impact of fluoroquinolone resistance in patients with E. Coli bacteremia. J. Hosp. Med. 2011, 6, 344–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, K.; Shigemura, K.; Nomi, M.; Takami, N.; Yamada, N.; Fujisawa, M. Use of oral third generation cephalosporins and quinolones and occurrence of antibiotic-resistant strains in the Neurogenic Bladder (NB) outpatient setting: A retrospective chart audit. Spinal Cord 2020, 58, 705–710. [Google Scholar] [CrossRef]
- Uda, A.; Tokimatsu, I.; Koike, C.; Osawa, K.; Shigemura, K.; Kimura, T.; Miyara, T.; Yano, I. Antibiotic de-escalation therapy in patients with community-acquired nonbacteremic pneumococcal pneumonia. Int. J. Clin. Pharm. 2019, 41, 1611–1617. [Google Scholar] [CrossRef]
- Wang, H.; Wang, H.; Yu, X.; Zhou, H.; Li, B.; Chen, G.; Ye, Z.; Wang, Y.; Cui, X.; Zheng, Y.; et al. Impact of antimicrobial stewardship managed by clinical pharmacists on antibiotic use and drug resistance in a Chinese hospital, 2010–2016: A retrospective observational study. BMJ Open 2019, 9, e026072. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, S.; Ishikawa, K.; Hayami, H.; Nakamura, T.; Miyairi, I.; Hoshino, T.; Hasui, M.; Tanaka, K.; Kiyota, H.; Arakawa, S. JAID/JSC guidelines for clinical management of infectious disease 2015—Urinary tract infection/male genital infection. J. Infect. Chemother. 2017, 23, 733–751. [Google Scholar] [CrossRef] [Green Version]
- Kitagawa, K.; Shigemura, K.; Yamamichi, F.; Alimsardjono, L.; Rahardjo, D.; Kuntaman, K.; Shirakawa, T.; Fujisawa, M. International comparison of causative bacteria and antimicrobial susceptibilities of urinary tract infections between Kobe, Japan, and Surabaya, Indonesia. Jpn. J. Infect. Dis. 2018, 71, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Gupta, K.; Hooton, T.M.; Naber, K.G.; Wullt, B.; Colgan, R.; Miller, L.G.; Moran, G.J.; Nicolle, L.E.; Raz, R.; Schaeffer, A.J.; et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: A 2010 update by the infectious diseases society of America and the European society for microbiology and infectious diseases. Clin. Infect. Dis. 2011, 52, e103–e120. [Google Scholar] [CrossRef] [Green Version]
- Gottesman, B.S.; Carmeli, Y.; Shitrit, P.; Chowers, M. Impact of quinolone restriction on resistance patterns of Escherichia Coli isolated from urine by culture in a community setting. Clin. Infect. Dis. 2009, 49, 869–875. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czeisler, M.É. Delay or Avoidance of Medical Care Because of COVID-19–Related Concerns — United States, June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1250. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Wordley, V.; Thompson, W. How Did COVID-19 Impact on Dental Antibiotic Prescribing across England? Br. Dent. J. 2020, 229, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Buehrle, D.J.; Wagener, M.M.; Nguyen, M.H.; Clancy, C.J. Trends in Outpatient Antibiotic Prescriptions in the United States During the COVID-19 Pandemic in 2020. JAMA Network Open 2021, 4, e2126114. [Google Scholar] [CrossRef]
- Uda, A.; Shigemura, K.; Kitagawa, K.; Osawa, K.; Onuma, K.; Inoue, S.; Kotani, J.; Yan, Y.; Nakano, Y.; Nishioka, T.; et al. How does antimicrobial stewardship affect inappropriate antibiotic therapy in urological patients? Antibiotics 2020, 9, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | December 2013 | December 2019 | December 2020 | p-Value 2013 vs. 2019 | p-Value 2013 vs. 2020 | p-Value 2019 vs. 2020 |
|---|---|---|---|---|---|---|
| Outpatients | n = 161 | n = 128 | n = 115 | |||
| Male sex, n (%) | 85 (53) | 81 (63) | 58 (50) | 0.19 | 0.79 | 0.18 |
| Age, median years (IQR) | 69 (52–79) | 70 (56–77) | 68 (56–76) | 1 | 1 | 1 |
| Medical ward, n (%) | 72 (45) | 48 (38) | 39 (34) | 0.53 | 0.28 | 0.65 |
| Inpatients | n = 134 | n = 77 | n = 61 | |||
| Male sex, n (%) | 90 (67) | 52 (68) | 36 (59) | 1 | 1 | 1 |
| Age, median years (IQR) | 69 (56–77) | 68 (57–77) | 73 (62–78) | 0.84 | 0.12 | 0.18 |
| Medical ward, n (%) | 66 (49) | 41 (53) | 31 (51) | 1 | 1 | 1 |
| Indications for use | December 2013 | December 2019 | December 2020 | p-Value 2013 vs. 2019 | p-Value 2013 vs. 2020 | p-Value 2019 vs. 2020 |
|---|---|---|---|---|---|---|
| Outpatients | ||||||
| Infections not requiring antibiotic prescriptions | 6.4 | 2.7 | 0.5 | 0.03 | <0.001 | 0.03 |
| Acute respiratory tract infections | 4.7 | 2.7 | 0.5 | 0.172 | <0.001 | 0.041 |
| Gastroenteritis | 1.7 | 0 | 0 | 0.032 | 0.032 | |
| Dental infections | 2.5 | 0.7 | 0.2 | 0.097 | 0.015 | 0.625 |
| Perioperative antibiotic prophylaxis | 10.9 | 8.5 | 6.1 | 0.47 | 0.069 | 0.47 |
| Surgical site infections | 0.7 | 0.2 | 0.2 | 1 | 1 | 1 |
| Prevention of febrile neutropenia | 4.2 | 4 | 6.8 | 1 | 0.32 | 0.32 |
| Otorhinolaryngology infections | 2 | 0.2 | 0.5 | 0.09 | 0.19 | 0.97 |
| Pneumonia | 2 | 1.3 | 1.6 | 1 | 0.58 | 1 |
| Skin and soft tissue infections | 2 | 0.2 | 0.7 | 0.09 | 0.39 | 0.59 |
| Intra-abdominal infections | 3 | 2 | 2.3 | 1 | 1 | 1 |
| Urinary tract infections | 4.7 | 11 | 8.7 | 0.006 | 0.079 | 0.33 |
| Other infections | 6 | 0.9 | 3 | <0.001 | 0.083 | 0.083 |
| Unknown infections | 6.2 | 5.4 | 3 | 0.72 | 0.15 | 0.27 |
| Inpatients | ||||||
| Perioperative antibiotic prophylaxis | 8.3 | 7.1 | 2.7 | 0.75 | 0.034 | 0.074 |
| Surgical site infections | 0.4 | 0.8 | 1.3 | 1 | 1 | 1 |
| Prevention of febrile neutropenia | 24.5 | 21.7 | 17.8 | 0.81 | 0.41 | 0.81 |
| Otorhinolaryngology infections | 0.8 | 2.1 | 0 | 0.82 | 0.82 | 0.26 |
| Pneumonia | 3.2 | 4.6 | 2.7 | 1 | 1 | 1 |
| Skin and soft tissue infections | 1.6 | 1.7 | 0 | 1 | 0.45 | 0.45 |
| Intra-abdominal infections | 9.1 | 3.8 | 3.6 | 0.034 | 0.038 | 1 |
| Urinary tract infections | 14.2 | 12.5 | 12.9 | 1 | 1 | 1 |
| Other infections | 4.8 | 0.8 | 7.6 | 0.03 | 0.26 | <0.001 |
| Unknown infections | 10.7 | 2.1 | 2.7 | 0.001 | 0.003 | 0.91 |
| Coef. | p | R-Squared | |
|---|---|---|---|
| Outpatients | −0.15655 | <0.001 | 0.5895 |
| Inpatients | −0.004825 | 0.0016 | 0.1015 |
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | |
|---|---|---|---|---|---|---|---|---|
| Outpatients | 34.0 (3.1) | 30.2 (3.2) * | 30.4 (2.6) * | 29.8 (2.8) * | 25.2 (3.3) *** | 25.5 (3.6) *** | 25.5 (3.0) *** | 17.3 (3.0) *** |
| Inpatients | 29.8 (3.9) | 25.9 (3.6) | 27.4 (5.1) | 24.1 (2.5) ** | 26.6 (3.1) | 25.1 (4.0) * | 27.1 (3.3) | 22.5 (3.1) *** |
| Bacteria | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | p |
|---|---|---|---|---|---|---|---|---|---|
| Pseudomonas aeruginosa | 194/229 (84.7) | 233/271 (86.0) | 249/267 (93.3) | 253/272 (93.0) | 232/250 (92.8) | 249/273 (91.2) | 314/334 (94.0) | 244/266 (91.7) | <0.001 |
| Escherichia coli | 312/396 (78.8) | 295/387 (76.2) | 329/419 (78.5) | 319/424 (75.2) | 320/438 (73.1) | 338/431 (78.4) | 378/499 (75.8) | 427/569 (75.0) | 0.24 |
| Klebsiella pneumoniae | 177/177 (100.0) | 182/188 (96.8) | 170/175 (97.1) | 200/201 (99.5) | 237/240 (98.8) | 237/242 (97.9) | 262/267 (98.1) | 277/280 (98.9) | 0.89 |
| 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | p | |
|---|---|---|---|---|---|---|---|---|---|
| Rate of intravenous antibiotic therapy | 258/2409 (10.7) | 240/2254 (10.6) | 248/2291 (10.8) | 279/2445 (11.4) | 260/2062 (12.6) | 232/2086 (11.1) | 193/2075 (9.3) | 161/1486 (10.8) | 0.71 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uda, A.; Shigemura, K.; Kitagawa, K.; Osawa, K.; Kusuki, M.; Yan, Y.; Yano, I.; Miyara, T. Effect of Antimicrobial Stewardship on Oral Quinolone Use and Resistance Patterns over 8 Years (2013–2020). Antibiotics 2021, 10, 1426. https://doi.org/10.3390/antibiotics10111426
Uda A, Shigemura K, Kitagawa K, Osawa K, Kusuki M, Yan Y, Yano I, Miyara T. Effect of Antimicrobial Stewardship on Oral Quinolone Use and Resistance Patterns over 8 Years (2013–2020). Antibiotics. 2021; 10(11):1426. https://doi.org/10.3390/antibiotics10111426
Chicago/Turabian StyleUda, Atsushi, Katsumi Shigemura, Koichi Kitagawa, Kayo Osawa, Mari Kusuki, Yonmin Yan, Ikuko Yano, and Takayuki Miyara. 2021. "Effect of Antimicrobial Stewardship on Oral Quinolone Use and Resistance Patterns over 8 Years (2013–2020)" Antibiotics 10, no. 11: 1426. https://doi.org/10.3390/antibiotics10111426
APA StyleUda, A., Shigemura, K., Kitagawa, K., Osawa, K., Kusuki, M., Yan, Y., Yano, I., & Miyara, T. (2021). Effect of Antimicrobial Stewardship on Oral Quinolone Use and Resistance Patterns over 8 Years (2013–2020). Antibiotics, 10(11), 1426. https://doi.org/10.3390/antibiotics10111426