Abstract
Background: Helicobacter pylori (HP) and Epstein–Barr virus (EBV) coinfection lead to chronic inflammation and contribute to the development of gastric cancer. However, studies examining the association between HP virulence factors and EBV infection in gastric cancer are limited. This study investigated the polymorphisms of HP virulence factors associated with EBV infection and their effects on clinical outcomes in EBV-associated gastric cancer (EBVaGC). Methods: A total of 96 HP isolates from 54 patients with gastric cancer were divided and analyzed based on EBV coinfection status. Polymerase chain reaction amplifications of virulence factors were conducted using DNA extracts from HP isolates cultured from gastric mucosal specimens. Results: EBV infection was significantly associated with gastric carcinoma with lymphoid stroma morphology and a proximal location in the stomach. Most HP strains from patients with gastric cancer were positive for cagA (100.0%), vacA (100.0%), and iceA1 (87.5%). Among HP isolates with EBV coinfection, the prevalence of iceA2 (21.7% vs. 0.0%, p < 0.001) and ureA (21.7% vs. 4.0%, p = 0.009) was significantly more frequent, and that of iceA1 (78.3% vs. 96.0%, p = 0.009) and vacA s1a (4.3% vs. 22.0%, p = 0.012) was less frequent than those of EBV– colonies. Multivariate analysis indicated that ureA (odds ratio, 6.148; 95% confidence interval [CI], 1.221 to 30.958; p = 0.028) was associated with EBVaGC. No significant difference in clinical outcomes was observed based on the presence of ureA expression in EBVaGC. Conclusions: In gastric cancer, regardless of EBV infection, most HP strains were highly virulent, testing positive for cagA, vacA, and iceA1. Although ureA was significantly associated with EBV infection, it did not influence the clinical outcomes of EBVaGC.
1. Introduction
Gastric cancer remains a significant global health concern, particularly in East Asia, where incidence and mortality rates are notably high. According to the Global Cancer Statistics (GLOBOCAN 2022), it ranks as the third-most commonly diagnosed cancer and the fourth leading cause of cancer mortality in South Korea [1]. While multiple genetic and environmental risk factors contribute to gastric carcinogenesis, infectious agents have emerged as crucial contributors [2,3].
Helicobacter pylori (HP), classified as a class I carcinogen by the World Health Organization in 1994, is recognized as a primary causative agent in the development of gastric cancer [4]. HP infection initiates a pathological cascade that progresses from chronic gastritis to atrophic gastritis, intestinal metaplasia, and dysplasia, ultimately leading to intestinal-type gastric cancer [5]. The pathogenicity of HP is influenced by various virulence factors, including cagA, vacA, iceA, oipA, and dupA, which show significant associations with gastric cancer development [6,7].
Recent studies have also identified Epstein–Barr virus (EBV) infection as a risk factor in gastric carcinogenesis [8]. Notably, coinfection with EBV and HP has been reported to significantly increase the risk of developing gastric cancer by synergistically inducing severe inflammatory responses in the gastric tissue [9]. Despite several studies examining the role of HP virulence factors in gastric carcinogenesis, limited research has addressed the relationship between these factors and EBV infection in gastric cancer.
Therefore, we aimed to analyze the genotypes of major HP virulence factors in patients with gastric cancer with EBV and HP coinfection, as well as the effects of these virulence factors on the clinical outcomes of EBV-associated gastric cancer (EBVaGC).
2. Results
2.1. Clinicopathologic Characteristics According to EBV Infection Status
Table 1 outlines the clinical characteristics of patients stratified by EBV status (EBV+ [n = 28], EBV– [n = 26]). The median age of all patients was 62 (IQR, 55–68) years, with males comprising 83.3% of all patients. HP eradication success rates were not significantly different between the EBV+ and EBV–groups (88.2% vs. 93.8%, p = 1.000). Tumors in the EBV+ group were more frequently located in the upper stomach compared to the EBV– group (28.6% vs. 7.7%, p = 0.034). Histologically, the GCLS type was significantly more prevalent in the EBV+ group (53.6% vs. 0.0%, p < 0.001). No significant differences were observed between the two groups in terms of recurrence-free survival (31.5 vs. 31.0 months, p = 0.075) or overall survival (32.0 vs. 32.5 months, p = 0.113).

Table 1.
Comparison of clinical characteristics between EBV+ and EBV− patients among HP-positive patients (n = 54).
2.2. Positivity of Virulence Factors According to EBV Infection Status
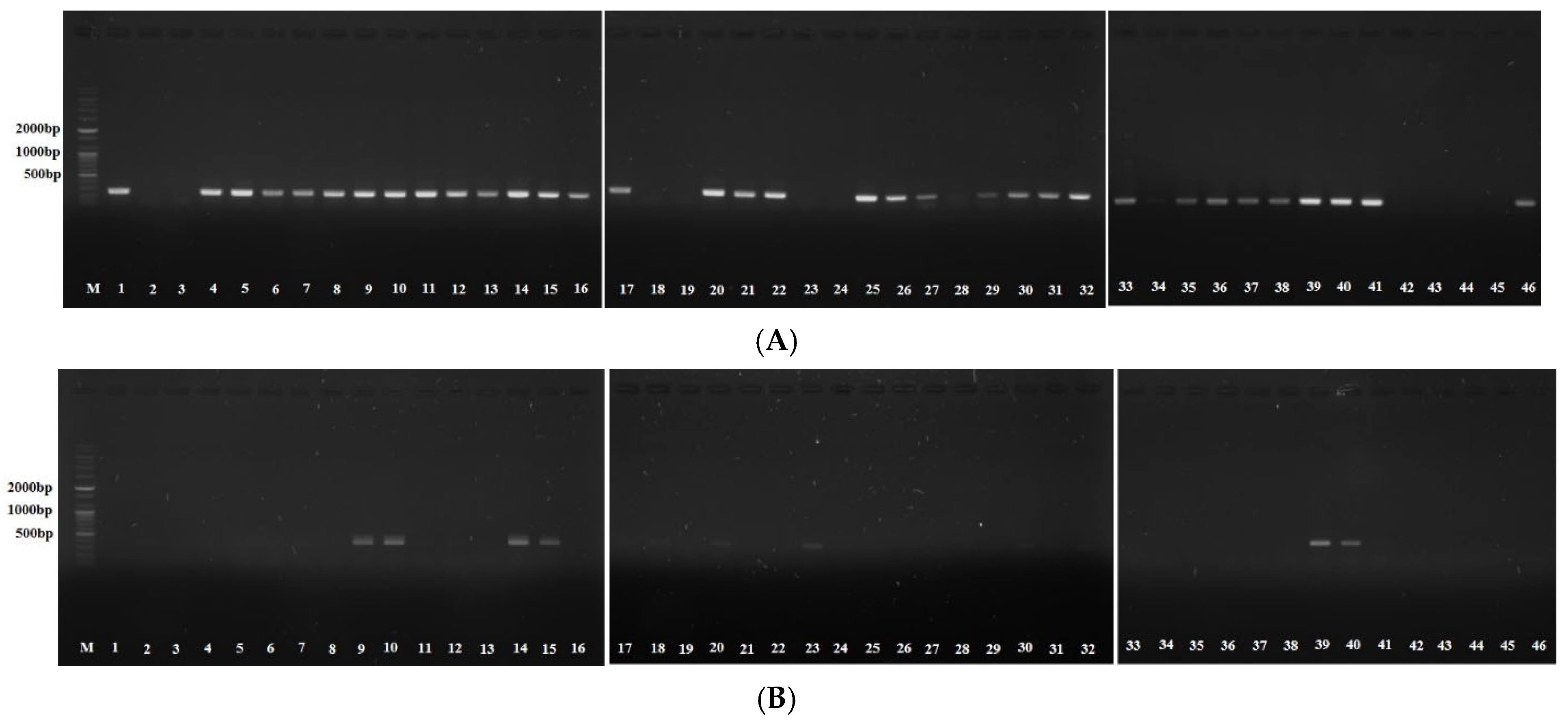
All HP isolates from patients with gastric cancer tested positive for cagA (100.0%) and vacA (100.0%), with iceA1 detected in 87.5% of isolates. Among HP isolates from patients with EBV coinfection, iceA2 (21.7% vs. 0.0%, p < 0.001) and ureA (21.7% vs. 4.0%, p = 0.009) were significantly more frequent, and iceA1 (78.3% vs. 96.0%, p = 0.009), JHP917 (0.0% vs. 18.0, p = 0.003), and vacA s1a (4.3% vs. 22.0%, p = 0.012) were less frequent compared to the EBV– group (Table 2). Multivariate analysis indicated that ureA (OR, 6.148; 95% CI, 1.221 to 30.958; p = 0.028) was significantly associated with EBVaGC (Table 3), whereas iceA1 showed an inverse association (OR, 0.163; 95% CI, 0.032 to 0.819; p = 0.028). Figure 1 presents the agarose gel electrophoresis results for iceA1 and ureA.
Table 2.
Positivity of virulence factors in EBV+ and EBV− HP colonies (n = 96).
Table 3.
Logistic regression analysis of the factors associated with EBV+ gastric cancer.
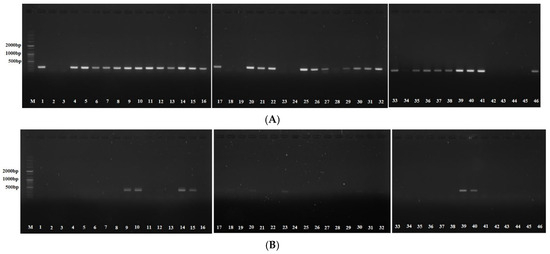
Figure 1.
Agarose gel electrophoresis for polymerase chain reaction products of Helicobacter pylori virulence factors in Epstein–Barr-virus-positive colonies. (A) iceA1 (247 bp) (−): 2/3/18/19/23/24/42/43/44/45. (B) ureA (411 bp) (+): 9/10/14/15/18/20/23/30/39/40. DNA size marker: 2000 bp, 1000 bp, 500 bp.
2.3. Clinical Outcomes According to Virulence Factors in EBV-Associated Gastric Cancer
We analyzed clinical outcomes based on the presence of ureA in patients with both EBV and HP coinfection (n = 46) (Table 4). Despite multivariate analysis confirming a significant association between ureA and EBVaGC, no significant differences in clinical outcomes were observed based on ureA expression. Supplemental Tables S1 and S2 summarize the comparisons of clinical outcomes based on the presence of iceA1 and iceA2. Similarly, no significant differences in clinical outcomes were detected with respect to the presence of iceA1 and iceA2.
Table 4.
Comparison of clinical characteristics according to presence of ureA in EBV+ HP colonies (n = 46).
3. Discussion
In this study, regardless of EBV infection, HP isolates from patients with gastric cancer exhibited highly virulent factors, including cagA, vacA, and iceA1. In cases of EBV and HP coinfection, the HP isolates displayed iceA2 and ureA virulence factors more frequently than those with HP infection alone, with ureA showing a significant association with EBVaGC. However, the presence of ureA did not lead to significant differences in the clinical outcomes of EBVaGC.
HP has been linked to various malignant conditions, including gastric carcinoma and mucosa-associated lymphoid tissue lymphoma of the stomach. Concurrently, EBV can induce oncogenic transformation in infected cells by activating multiple signaling pathways [10]. The coinfection of these two pathogens may exert synergistic effects, enhancing inflammatory responses in gastric tissues and increasing the risk of gastric cancer development [11,12,13]. We have reported previously that EBV and HP coinfection does not significantly influence clinical outcomes in patients with EBVaGC [14]. However, there is a lack of studies investigating which HP virulence factors are prominent in EBVaGC and their impact on clinical outcomes.
Consistent with prior studies, our study found that EBV+ gastric cancers were predominantly located in the proximal region of the stomach and exhibited GCLS histology more frequently than the EBV– group [14,15]. A notable finding from our study is that HP isolates from patients with gastric cancer, irrespective of EBV infection status, were predominantly highly virulent strains positive for cagA (100%), vacA (100%), and iceA1 (87.5%). This high prevalence of virulent strains supports the well-established association between HP virulence factors and increased gastric cancer risk [7,16,17,18]. Among these factors, cagA has been reported to enhance EBV-driven epigenetic modifications by increasing DNA methyltransferase expression and promoting gastric carcinogenesis through hypermethylation and silencing of tumor suppressor genes related to cell cycle regulation, apoptosis, and DNA repair [16].
Our study revealed significant differences in the distribution of virulence factors between the EBV+ and EBV– groups. EBV-coinfected HP isolates exhibited a significantly higher prevalence of iceA2 and ureA while demonstrating lower frequencies of iceA1, JHP917, and vacA s1a. These findings suggest that specific HP virulence profiles may interact differently with EBV infection, potentially contributing to distinct carcinogenic pathways. Furthermore, multivariate analysis identified ureA (OR 6.148) as significantly associated with EBV+ gastric cancer. The urease enzyme encoded by the ure gene cluster, including ureA, is essential for HP colonization by neutralizing gastric acid, thus creating a favorable microenvironment for bacterial survival [19,20,21,22]. Further studies are required to confirm whether this enhanced urease activity facilitates EBV infection or reactivation in the gastric mucosa. Despite the significant association between ureA and EBV+ gastric cancer, our analysis found no differences in clinical outcomes, including recurrence-free survival and overall survival, based on ureA expression status. This indicates that although these virulence factors may influence susceptibility to EBV and HP coinfection and the development of gastric cancer, they may not significantly affect disease progression or prognosis. Recent in vitro studies have demonstrated that EBV infection enhances phosphorylation-dependent CagA activity and amplifies the oncogenic potential of HP [23,24]. These findings suggest that EBV and HP coinfection may involve complex molecular interactions beyond simple co-colonization, indicating that the differential virulence factor profiles observed in this study are meaningful and warrant further investigation.
This study has certain limitations. First, the retrospective design and relatively small sample size may limit the generalizability of our findings and reduce statistical power, particularly for subgroup analyses. Second, the enrolled patients predominantly consisted of early gastric cancer cases (94.4% in the EBV+ and 92.3% in the EBV– groups), which may not represent the full spectrum of gastric cancer progression. Third, because HP isolates were analyzed from patients with diagnosed gastric cancer, it was not possible to evaluate the role of virulence factors in the early stages of carcinogenesis or the temporal relationship with EBV infection. It remains unclear whether specific HP virulence profiles predispose individuals to EBV infection or whether EBV infection exerts selective pressure favoring certain HP strains.
4. Materials and Methods
4.1. Study Population
We analyzed HP isolates obtained from patients with gastric cancer who visited Asan Medical Center between January 2018 and February 2021. The inclusion criteria were as follows: (1) age ≥ 19 years; (2) histologically confirmed gastric cancer; (3) HP infection confirmed by culture from endoscopic biopsy specimens; and (4) for the EBV+ group, EBV positivity confirmed by in situ hybridization in tumoral gastric mucosa. The exclusion criteria were as follows: (1) age < 19 years; and (2) cases without culture-confirmed HP infection. A total of 96 HP isolates obtained from 54 patients with gastric cancer were enrolled and analyzed. They were divided into two groups: patients with HP and EBV coinfection (28 patients, 46 isolates) and those with HP infection alone (26 patients, 50 isolates). Clinicopathological data for each patient were retrospectively collected from medical records. The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB No. 2020-0518).
4.2. H. pylori Culture
Gastric tissue samples were collected from the antrum and corpus regions during esophagogastroduodenoscopy and immediately transferred to sterile Eppendorf tubes, which were placed in a vacuum container with dry ice for transportation. Upon arrival at the laboratory, specimens were stored in a deep freezer at –80 °C until processing. Prior to culture, the tissue samples were equilibrated to room temperature. For bacterial isolation, the specimens were cultured on specialized HP-selective medium consisting of Brucella broth agar enriched with 5% sheep blood and supplemented with antimicrobial agents (vancomycin 10 µg/L, trimethoprim 5 µg/L, amphotericin B 5 µg/L, and polymyxin B 2.5 IU). The inoculated plates were maintained at 37 °C in a microaerophilic environment (5% O2, 10% CO2, and 85% N2) for 5–7 days. HP identification was based on colony morphology, positive Gram staining characteristics, and urease activity.
4.3. Genomic DNA Extraction
Harvested pellets were resuspended in 200 µL PBS. Genomic DNA (gDNA) was extracted using the DNeasy® (Qiagen, Hilden, Germany) kit. The mixture was incubated at 56 °C for 10 min after adding 20 µL proteinase K and 200 µL Buffer AL. Then, 200 µL ethanol was added and mixed by vortexing. The mixture was transferred to a DNeasy Mini spin column placed in a 2 mL collection tube and centrifuged at 6000× g for 1 min. A new 2 mL collection tube was used to add 500 µL Buffer AW1, followed by centrifugation for 1 min at 6000× g. A second new 2 mL collection tube was used to add 500 µL Buffer AW2, with centrifugation for 3 min at 20,000× g. For gDNA elution, 50 µL Buffer AE was added to the center of the spin column membrane and incubated for 1 min at room temperature. Centrifugation was then performed for 1 min at 6000× g. The gDNA was stored at –20 °C until required for polymerase chain reaction (PCR) amplification.
4.4. PCR Amplification
The PCR mixture included sense and antisense primers (Table 5), Taq PCR PreMix (AccuPower®, Daejeon, Republic of Korea), template DNA, and distilled water. PCR was performed under the following conditions: 10 min at 95 °C, followed by 30 cycles of 30 s at 95 °C, 30 s at each annealing temperature, and 30 s at 75 °C. After PCR, the products were run on 1% agarose gels, and bands were developed using an ultraviolet transilluminator and photographed.
Table 5.
PCR primers used to amplify the target sequences.
4.5. Statistical Analysis
Descriptive variables were summarized as the median and interquartile range (IQR) or the mean and standard deviation (SD). Differences in patient characteristics and HP virulence factors between the EBV+ and EBV− groups were compared using independent t-tests and chi-square tests. Logistic regression analyses were conducted to investigate factors associated with EBVaGC, and odds ratios (ORs) and corresponding confidence intervals (CIs) were calculated. p-values < 0.05 were considered statistically significant. All statistical analyses were performed using SPSS version 24 (IBM Corporation, Somers, NY, USA).
5. Conclusions
In conclusion, our study demonstrates that patients in Korea with gastric cancer predominantly harbor highly virulent HP strains positive for cagA, iceA1, and vacA. The ureA virulence factor was associated with EBVaGC; however, it did not significantly influence clinical outcomes. These findings contribute to our understanding of the complex interactions between infectious agents in gastric carcinogenesis and underscore the need for further investigation into the molecular mechanisms underlying the relationship between HP virulence factors and EBV infection in gastric cancer development.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/antibiotics14060580/s1. Table S1. Comparison of clinical characteristics according to presence of iceA1 in EBV+ HP colonies (n = 46). Table S2. Comparison of clinical characteristics according to presence of iceA2 in EBV+ HP colonies (n = 46).
Author Contributions
Conceptualization: J.Y.A. Methodology: J.H.N., J.Y.A., H.K.N., J.H.L., K.W.J., D.H.K., K.D.C., H.J.S., G.H.L., and H.-Y.J. Investigation: J.H.N. and J.Y.A. Writing—Original Draft: J.H.N. Writing—Review and Editing: J.H.N. and J.Y.A. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Korean College of Helicobacter and Upper Gastrointestinal Research Foundation Grant (grant number: KCHUGR–202002501).
Institutional Review Board Statement
The study protocol was approved by the Institutional Review Board of Asan Medical Center (IRB No. 2020-0518).
Informed Consent Statement
This study did not involve humans.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Gomceli, I.; Demiriz, B.; Tez, M. Gastric carcinogenesis. World J. Gastroenterol. 2012, 18, 5164–5170. [Google Scholar] [PubMed]
- Salvatori, S.; Marafini, I.; Laudisi, F.; Monteleone, G.; Stolfi, C. Helicobacter pylori and Gastric Cancer: Pathogenetic Mechanisms. Int. J. Mol. Sci. 2023, 24, 2895. [Google Scholar] [CrossRef] [PubMed]
- Schistosomes, liver flukes and Helicobacter pylori. In IARC Monographs on the Evaluation of Carcinogenic Risks to Humans; IARC: Lyon, France, 1994; Volume 61, pp. 1–241.
- Correa, P.; Piazuelo, M.B. The gastric precancerous cascade. J. Dig. Dis. 2012, 13, 2–9. [Google Scholar] [CrossRef]
- Wang, M.Y.; Liu, X.F.; Gao, X.Z. Helicobacter pylori virulence factors in development of gastric carcinoma. Future Microbiol. 2015, 10, 1505–1516. [Google Scholar] [CrossRef]
- Pormohammad, A.; Ghotaslou, R.; Leylabadlo, H.E.; Nasiri, M.J.; Dabiri, H.; Hashemi, A. Risk of gastric cancer in association with Helicobacter pylori different virulence factors: A systematic review and meta-analysis. Microb. Pathog. 2018, 118, 214–219. [Google Scholar] [CrossRef]
- Chen, X.Z.; Chen, H.; Castro, F.A.; Hu, J.K.; Brenner, H. Epstein-Barr virus infection and gastric cancer: A systematic review. Medicine 2015, 94, e792. [Google Scholar] [CrossRef]
- Cárdenas-Mondragón, M.G.; Torres, J.; Flores-Luna, L.; Camorlinga-Ponce, M.; Carreón-Talavera, R.; Gomez-Delgado, A.; Kasamatsu, E.; Fuentes-Pananá, E.M. Case–control study of Epstein–Barr virus and Helicobacter pylori serology in Latin American patients with gastric disease. Br. J. Cancer 2015, 112, 1866–1873. [Google Scholar] [CrossRef]
- Luo, Y.; Liu, Y.; Wang, C.; Gan, R. Signaling pathways of EBV-induced oncogenesis. Cancer Cell Int. 2021, 21, 93. [Google Scholar] [CrossRef]
- Singh, S.; Jha, H.C. Status of Epstein-Barr Virus Coinfection with Helicobacter pylori in Gastric Cancer. J. Oncol. 2017, 2017, 3456264. [Google Scholar] [CrossRef]
- Matsusaka, K.; Funata, S.; Fukayama, M.; Kaneda, A. DNA methylation in gastric cancer, related to Helicobacter pylori and Epstein-Barr virus. World J. Gastroenterol. 2014, 20, 3916–3926. [Google Scholar] [CrossRef] [PubMed]
- Dávila-Collado, R.; Jarquín-Durán, O.; Dong, L.T.; Espinoza, J.L. Epstein-Barr Virus and Helicobacter pylori Co-Infection in Non-Malignant Gastroduodenal Disorders. Pathogens 2020, 9, 104. [Google Scholar] [CrossRef]
- Noh, J.H.; Shin, J.Y.; Lee, J.H.; Park, Y.S.; Lee, I.S.; Kim, G.H.; Na, H.K.; Ahn, J.Y.; Jung, K.W.; Kim, D.H.; et al. Clinical Significance of Epstein-Barr Virus and Helicobacter pylori Infection in Gastric Carcinoma. Gut Liver 2023, 17, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Naseem, M.; Barzi, A.; Brezden-Masley, C.; Puccini, A.; Berger, M.D.; Tokunaga, R.; Battaglin, F.; Soni, S.; McSkane, M.; Zhang, W.; et al. Outlooks on Epstein-Barr virus associated gastric cancer. Cancer Treat. Rev. 2018, 66, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Pandey, S.; Jha, H.C.; Shukla, S.K.; Shirley, M.K.; Robertson, E.S. Epigenetic Regulation of Tumor Suppressors by Helicobacter pylori Enhances EBV-Induced Proliferation of Gastric Epithelial Cells. mBio 2018, 9, e00649-18. [Google Scholar] [CrossRef]
- Yong, X.; Tang, B.; Li, B.S.; Xie, R.; Hu, C.J.; Luo, G.; Qin, Y.; Dong, H.; Yang, S.-M. Helicobacter pylori virulence factor CagA promotes tumorigenesis of gastric cancer via multiple signaling pathways. Cell Commun. Signal. CCS 2015, 13, 30. [Google Scholar] [CrossRef]
- Huang, J.Q.; Zheng, G.F.; Sumanac, K.; Irvine, E.J.; Hunt, R.H. Meta-analysis of the relationship between cagA seropositivity and gastric cancer. Gastroenterology 2003, 125, 1636–1644. [Google Scholar] [CrossRef]
- Scott, D.R.; Marcus, E.A.; Weeks, D.L.; Sachs, G. Mechanisms of acid resistance due to the urease system of Helicobacter pylori. Gastroenterology 2002, 123, 187–195. [Google Scholar] [CrossRef]
- Clyne, M.; Labigne, A.; Drumm, B. Helicobacter pylori requires an acidic environment to survive in the presence of urea. Infect. Immun. 1995, 63, 1669–1673. [Google Scholar] [CrossRef]
- Scott, D.R.; Marcus, E.A.; Wen, Y.; Oh, J.; Sachs, G. Gene expression in vivo shows that Helicobacter pylori colonizes an acidic niche on the gastric surface. Proc. Natl. Acad. Sci. USA 2007, 104, 7235–7240. [Google Scholar] [CrossRef]
- Valenzuela-Valderrama, M.; Cerda-Opazo, P.; Backert, S.; González, M.F.; Carrasco-Véliz, N.; Jorquera-Cordero, C.; Wehinger, S.; Canales, J.; Bravo, D.; Quest, A.F.G. The Helicobacter pylori Urease Virulence Factor Is Required for the Induction of Hypoxia-Induced Factor-1α in Gastric Cells. Cancers 2019, 11, 799. [Google Scholar] [CrossRef]
- Wroblewski, L.E.; Peek, R.M., Jr. Clinical Pathogenesis, Molecular Mechanisms of Gastric Cancer Development. Curr. Top. Microbiol. Immunol. 2023, 444, 25–52. [Google Scholar]
- Bui, N.N.; Huang, S.C.; Tran, T.N.L.; Nguyen, N.H.; Do, H.N.; Chiu, Y.F.; Lai, C.-H. Association between Helicobacter pylori and Epstein-Barr virus co-infection and gastric cancer risk: A systematic review and meta-analysis. QJM Mon. J. Assoc. Physicians 2025, 118, hcaf092. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).