
Reference Architectures, Platforms, and Pilots for European Smart and Healthy Living—Analysis and Comparison

 ,
,  , ,
, ,  , , , ,
, , , ,  and
and
Abstract
:1. Introduction
2. Background
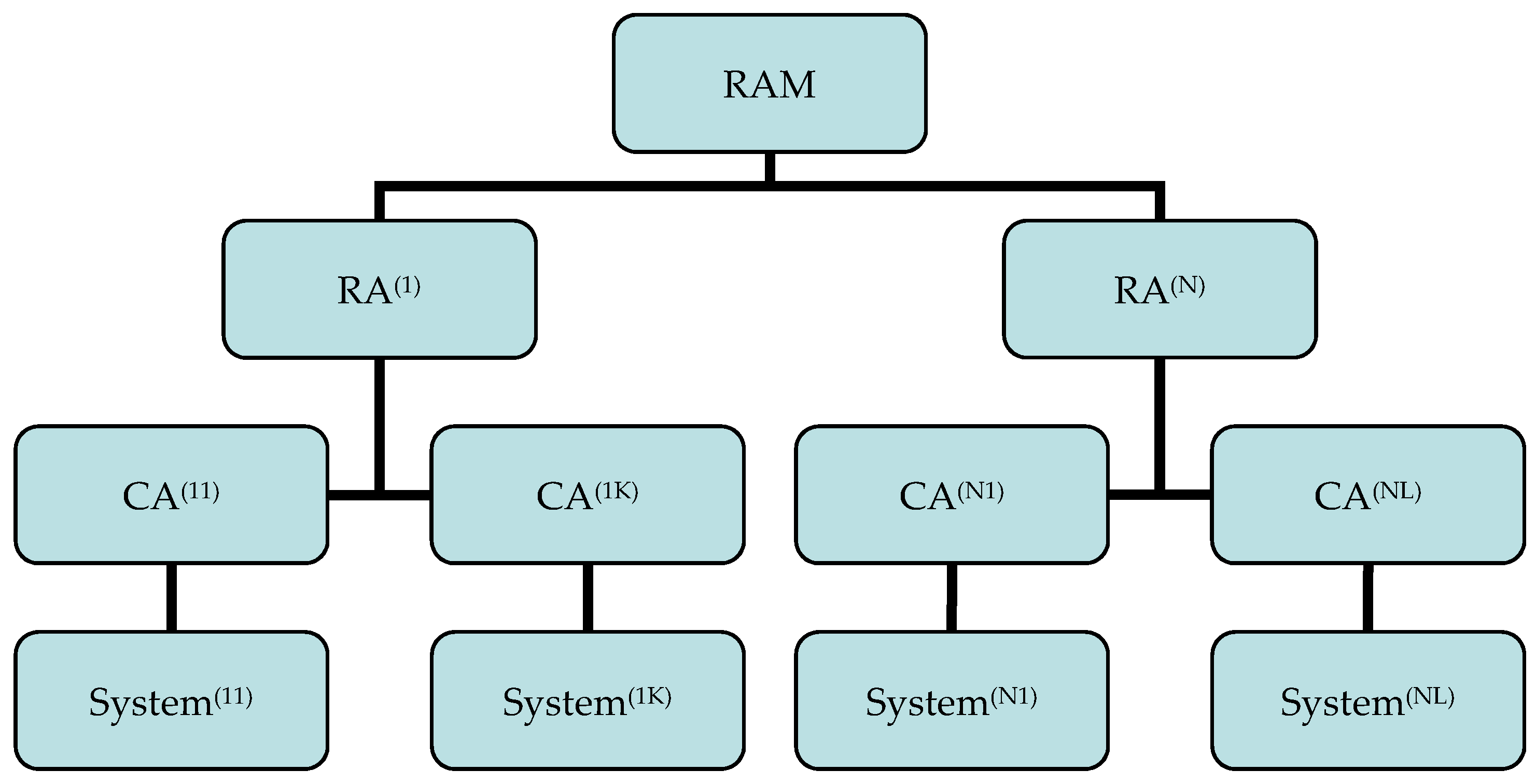
2.1. Reference Architecture Model (RAM), Reference Architecture (RA), Concrete Architecture (CA), System
- System stakeholders (including users, operators, owners, developers, maintainers);
- Fundamental concerns (including the purpose of the system, suitability of the architecture to fulfill the set objective, feasibility, risks, maintainability, evolution);
- Architecture views (representing a related set of concerns as seen from a perspective a view is taken, a viewpoint); and
- The rationale for each important architecture decision.
2.2. Architectures in eHealth Systems
2.3. Architectures in AAL systems
3. Selected Health and Care Projects in A Nutshell
3.1. Activage Large Scale Pilots
3.2. Adlife Large Scale Pilots
3.3. Gatekeeper Large Scale Pilots
3.4. Pharaon Large Scale Pilots
3.5. Shapes Large Scale Pilots
3.6. Sphinx Pilots
3.7. Smart Bear Large Scale Pilots
4. Analysis Method Definition
4.1. Selection of Established Taxonomies
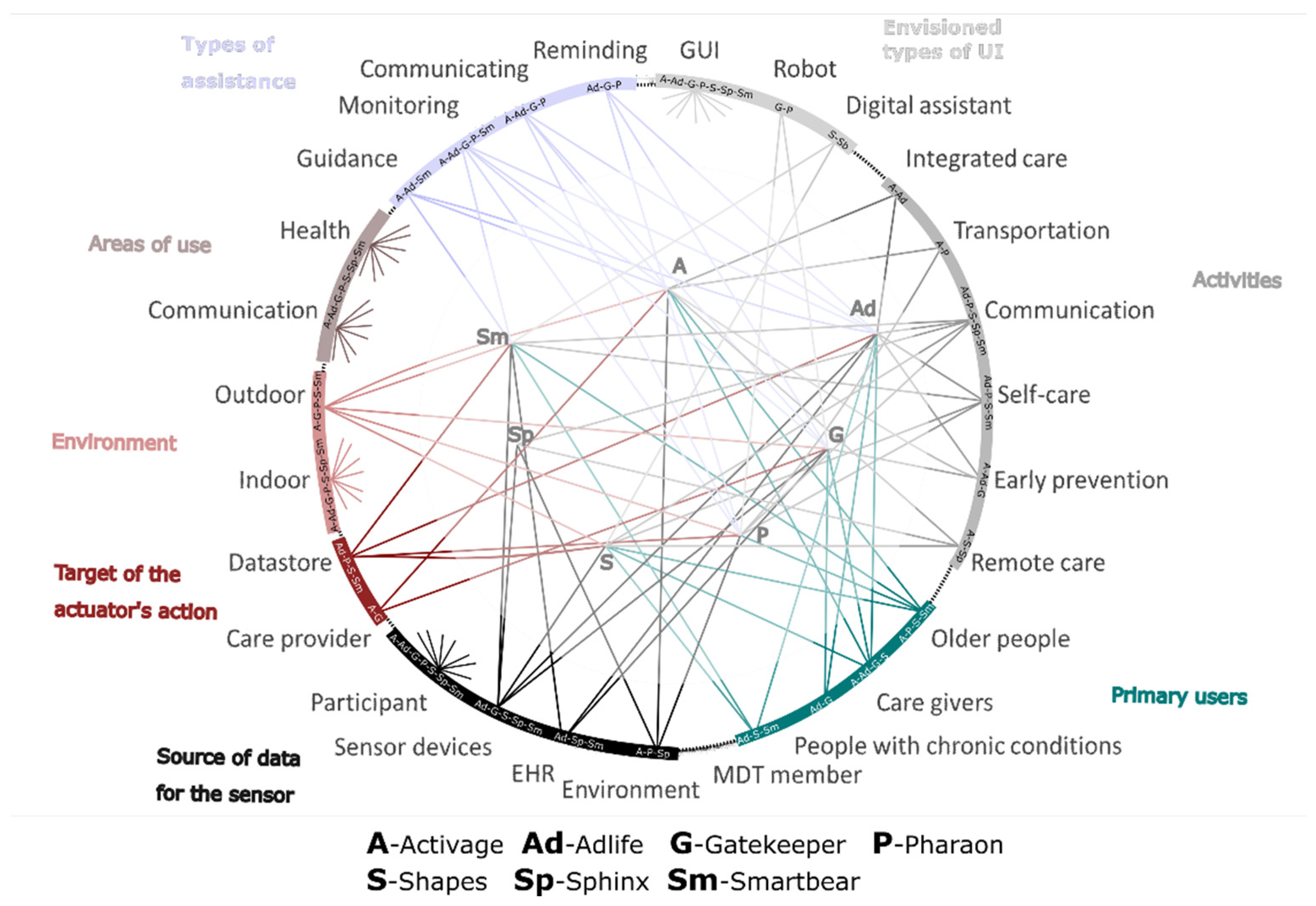
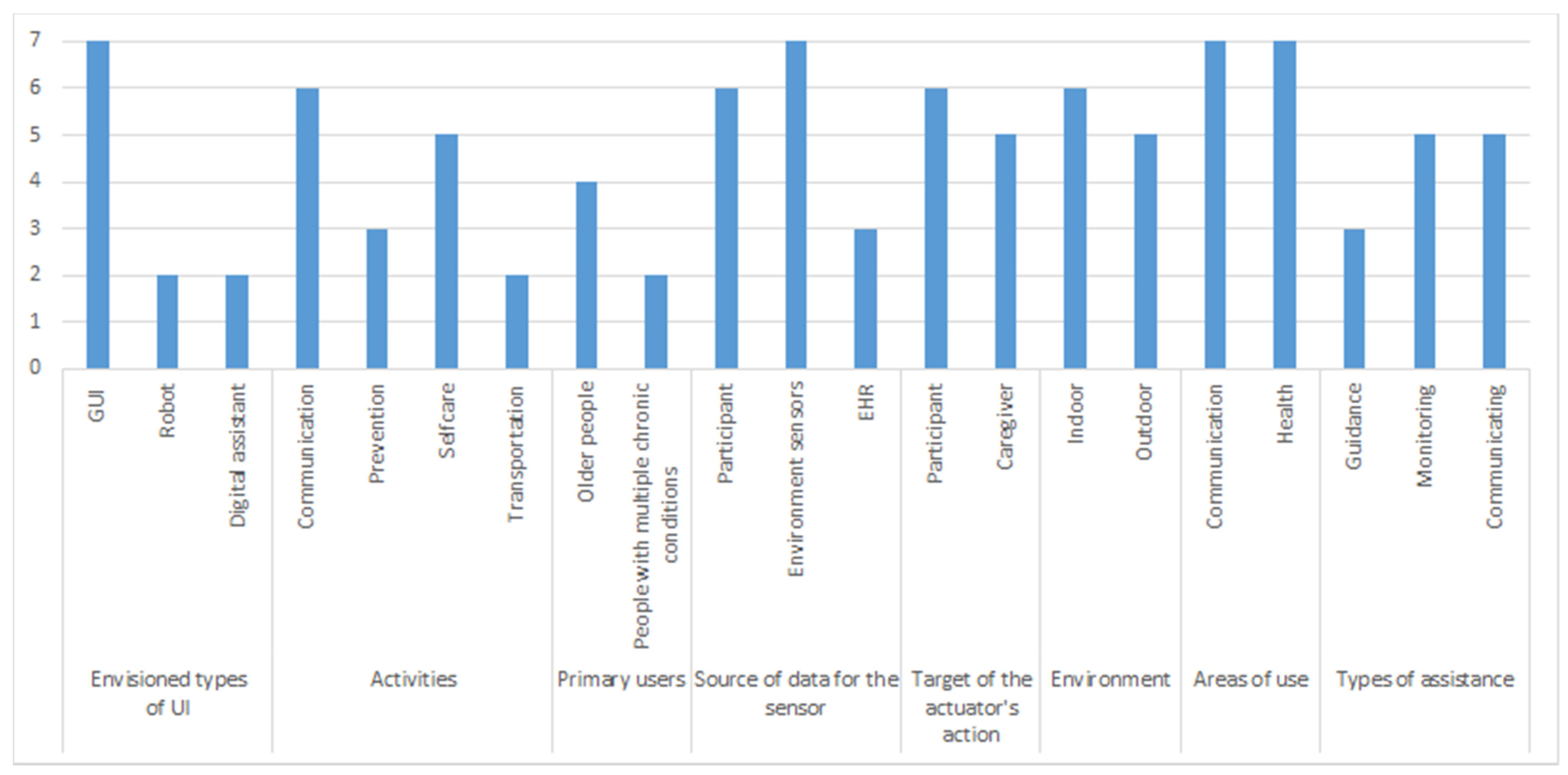
4.1.1. Pervasive Healthcare Systems (PHS) Taxonomy
- Body functions (including mental, sensory, voice and speech, movement-related, cardiovascular, respiratory, immunological), to imply the appropriate User Interface (UI);
- Activities and participation (including general tasks, communication, mobility, self-care, domestic life), indicating tasks that the user cannot manage;
- Support (including participants, caregiver, vicinity), to imply who may benefit from the system;
- Source of data for sensor (including participant, object, environment, time), to mean the kind of data that triggers the action;
- The target of actuator’s action (including participant, caregiver, object, data store), to imply identity or object a device’s outcome is executed;
- Environment (including indoors and outdoors), to indicate where the pervasive system is used;
- Products and technology, to imply areas of use (including use in daily living, indoor and outdoor mobility, communication, protection, health) and types of assistance (including localization, guidance, reminding, communicating, monitoring, assisting).
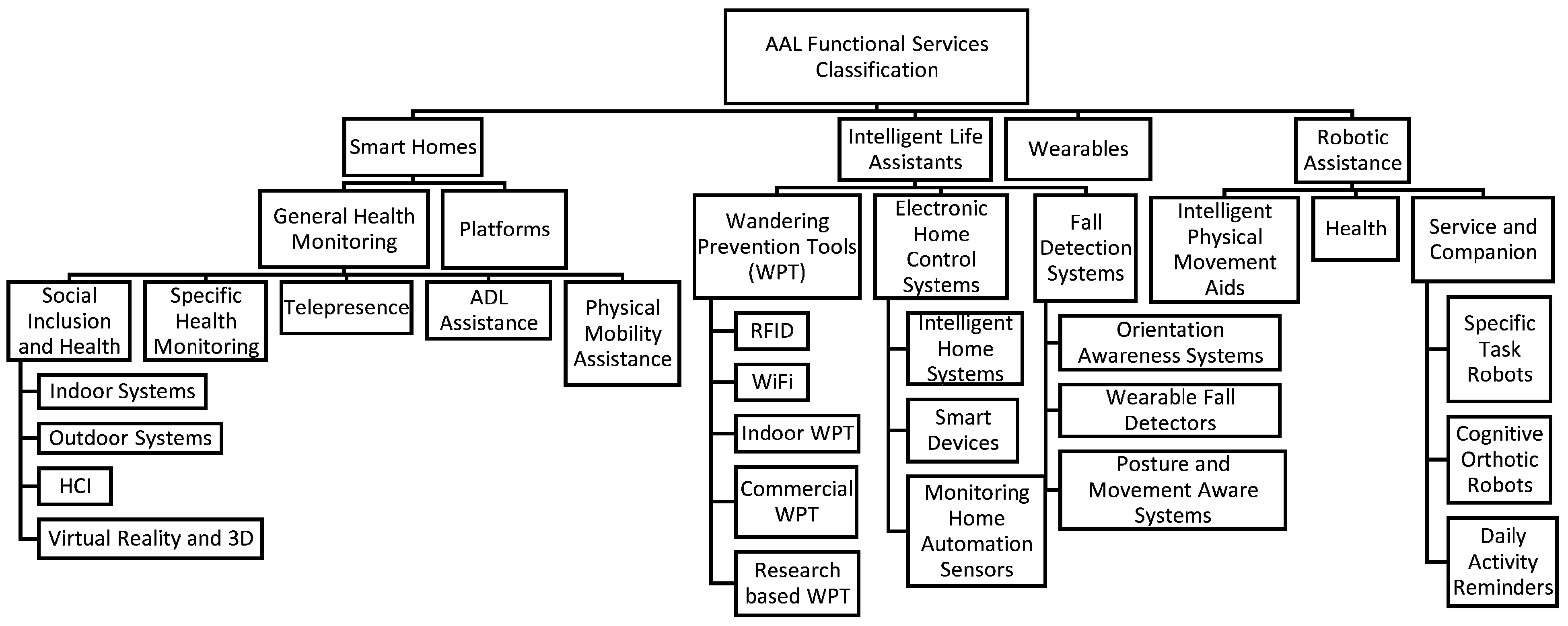
4.1.2. AAL Taxonomy
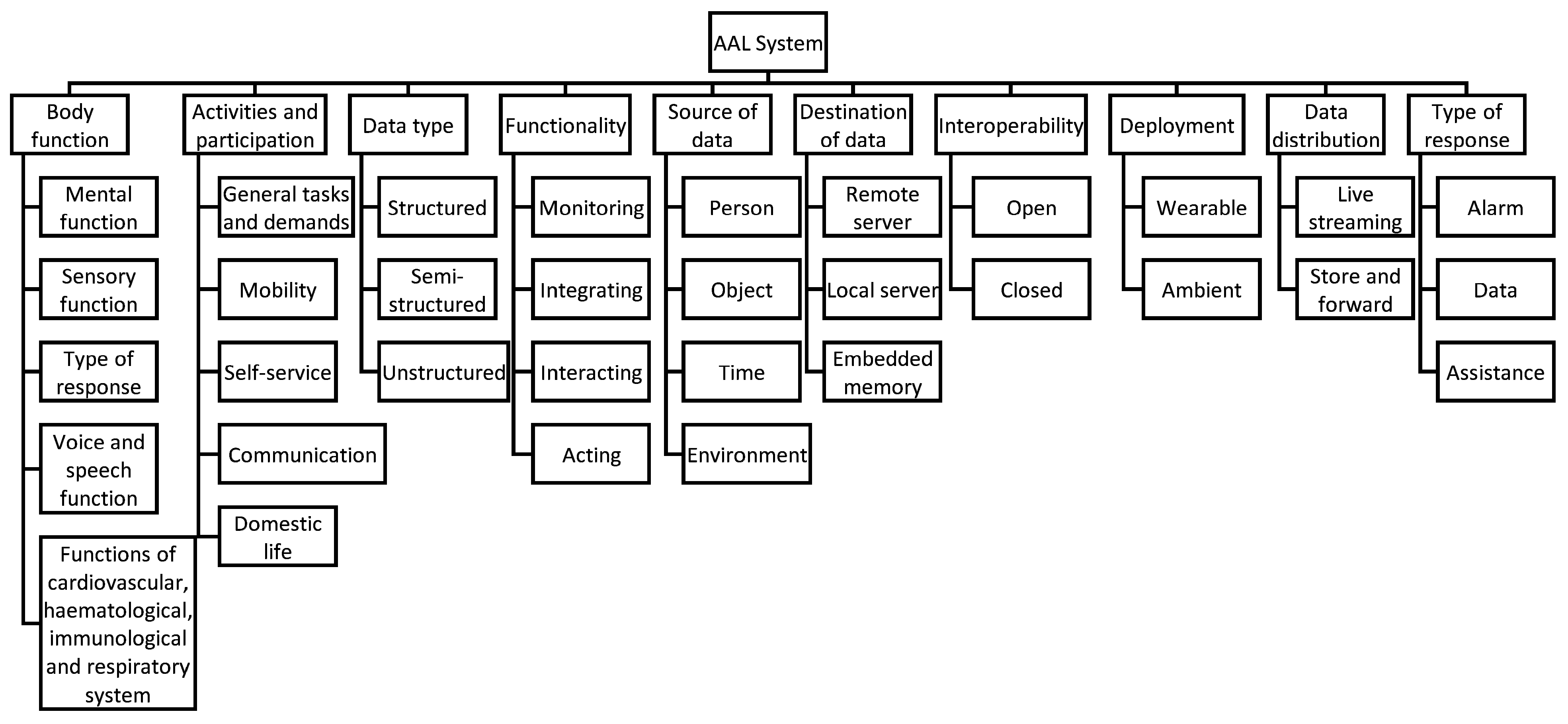
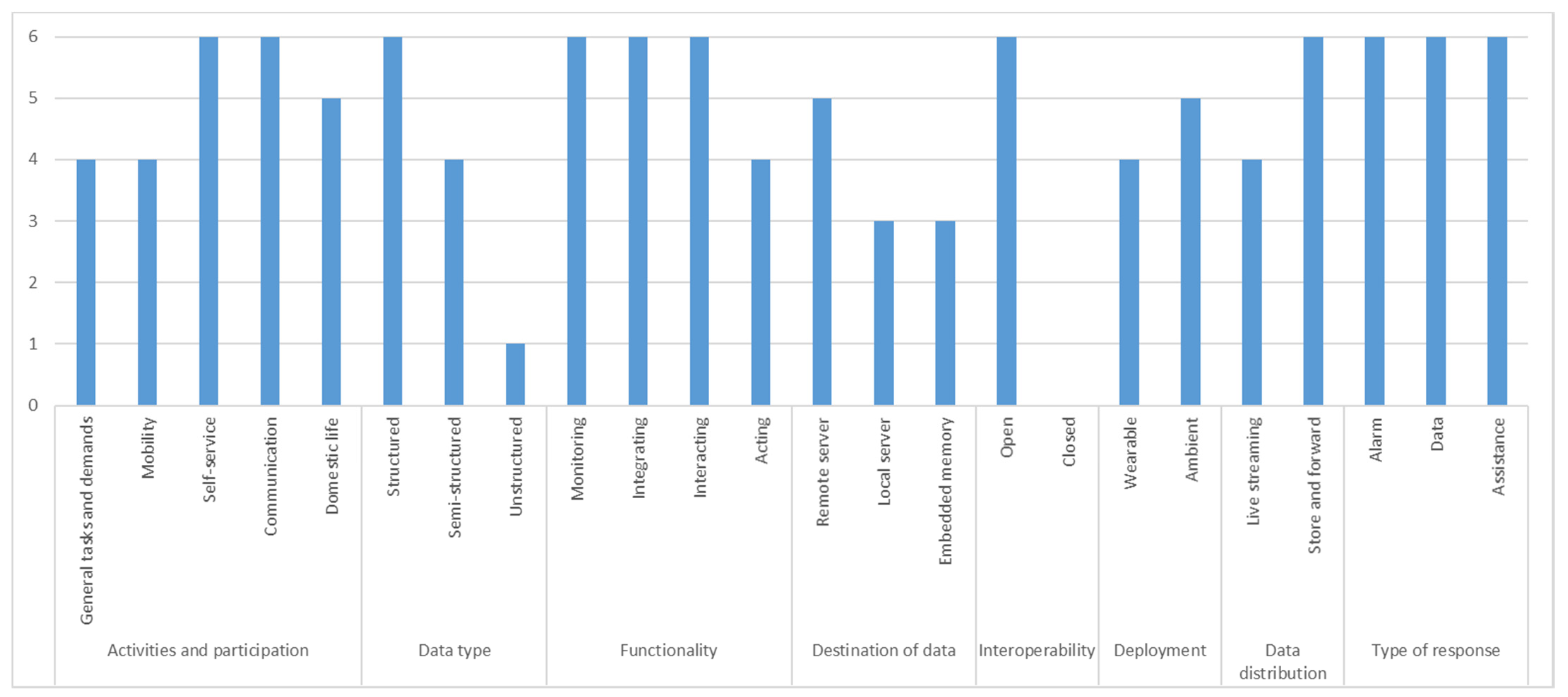
4.1.3. Data Quality-Oriented AAL Taxonomy
4.2. Selection of Reference Architecture Model (RAM)
- IDS RAM (International Data Spaces Association, Reference Architecture Model) 3.0 [44];
- IIRA (Industrial Internet Reference Architecture) [45];
- IoT reference model by ITU-T Y.2060 [46];
- CREATE-IoT 3D RAM [47];
- RAMI4.0 (Reference Architecture Model Industrie) [48];
- ISO/IEC 30141: 2018 IoT RA [49]; and
- None.
4.2.1. IDS RAM 3.0
4.2.2. CREATE-IoT 3D RAM
5. Presentation of Results
5.1. Classification Based on Selected Taxonomies
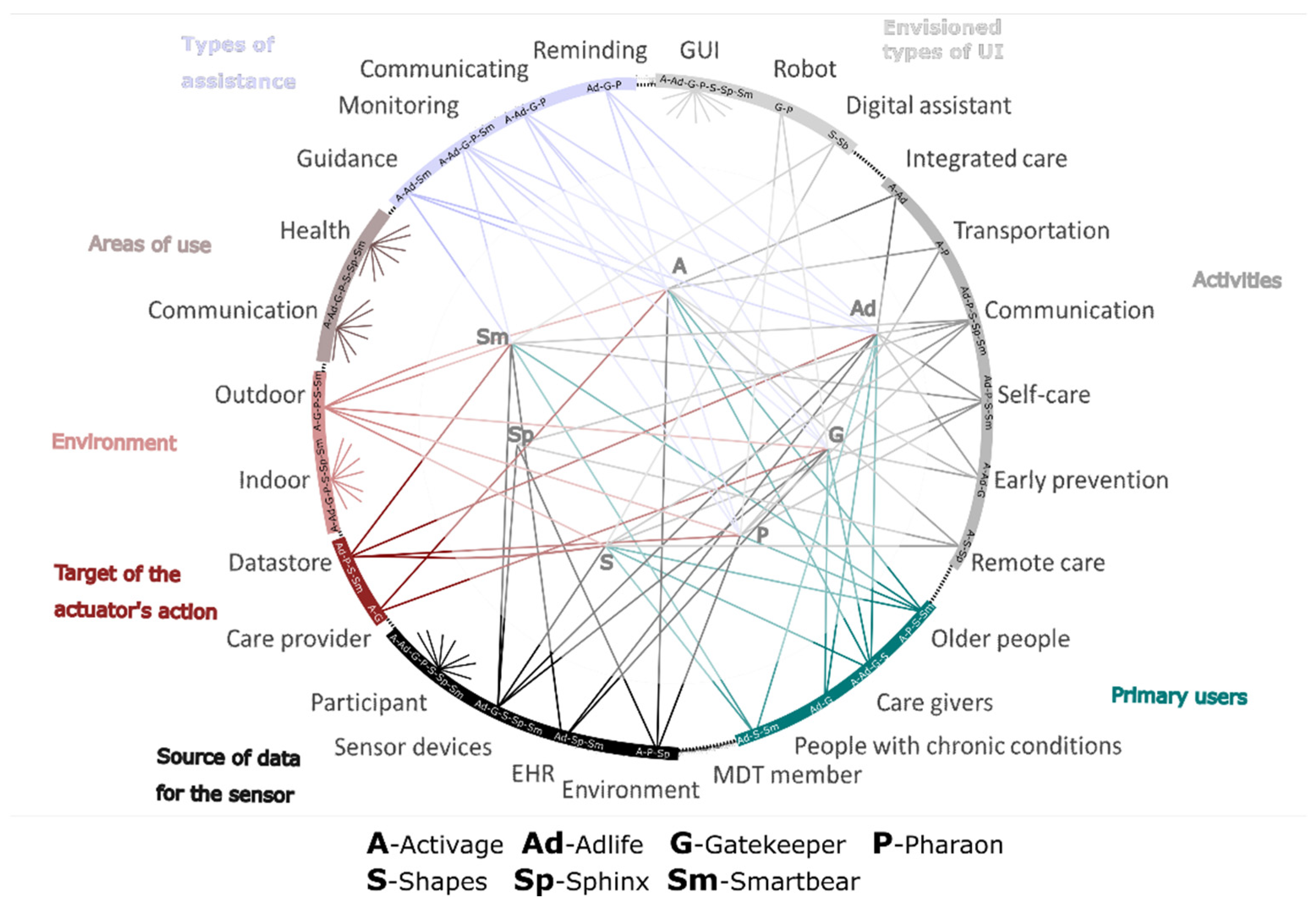
5.1.1. PHS Taxonomy-Based Classification
5.1.2. AAL Taxonomy-Based Classification
5.1.3. Data Quality-Oriented AAL Taxonomy-Based Classification
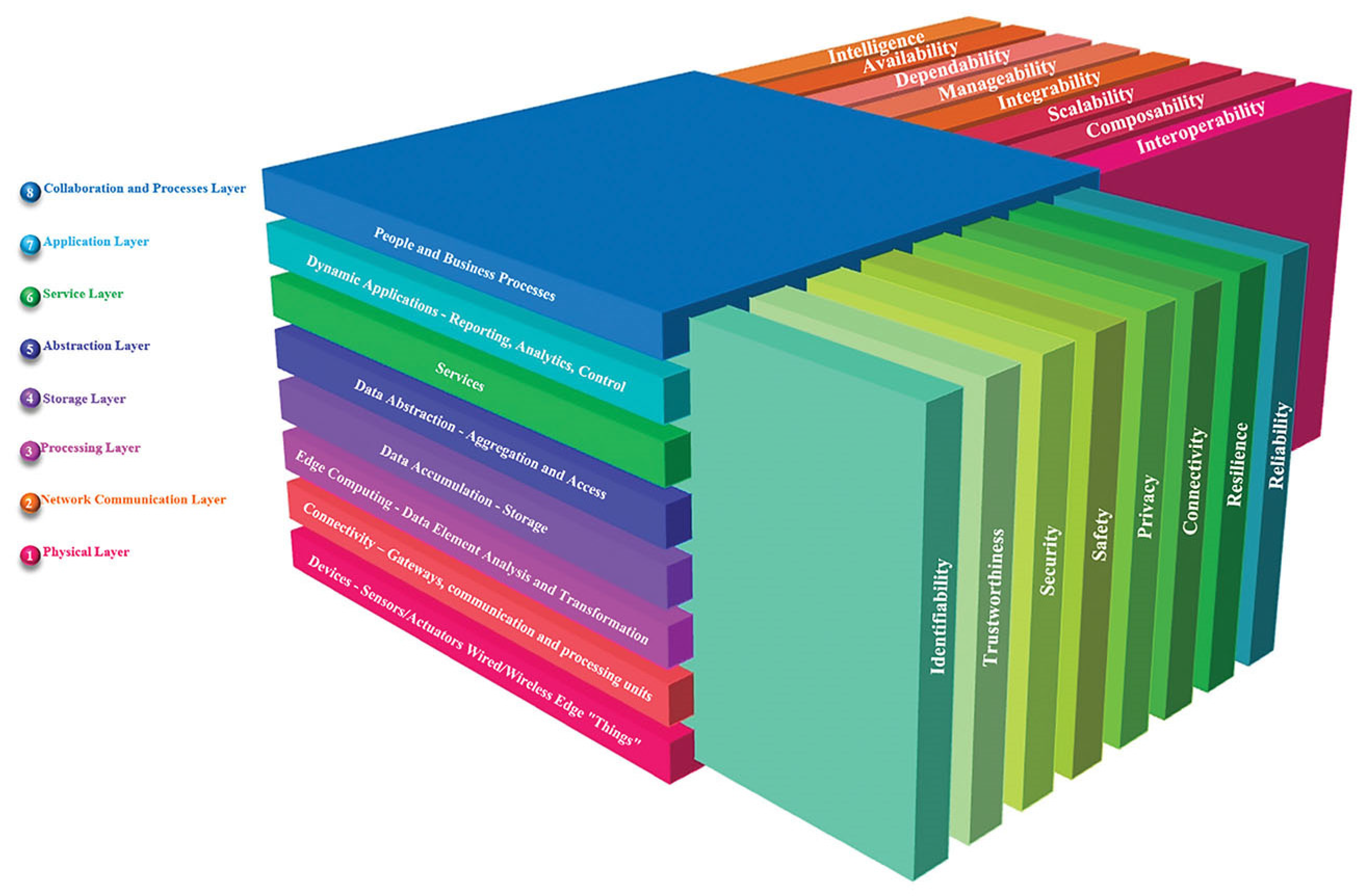
5.2. Mapping to Selected RAM
- Collaboration and Process layer (People and Business Processes), which focuses on enabling integration with external systems;
- Application Layer (Dynamic Applications), which focuses on visualizing the device data;
- Service Layer (Services), which focuses on the development environment, service orchestration, advanced analytics;
- Abstraction Layer (Data Abstraction), which focuses on event and action management, basic data normalization, reformatting, and cleaning;
- Storage Layer (Data Accumulation), which focuses on storing data in databases;
- Processing Layer (Edge Computing), which focuses on device management and data processing at the edge;
- Network Communication Layer (Connectivity), which focuses on network connectivity and bridges from IoT gateways to Cloud;
- Physical Layer (Devices), which focuses on operating systems, drivers, sensors, and actuators.
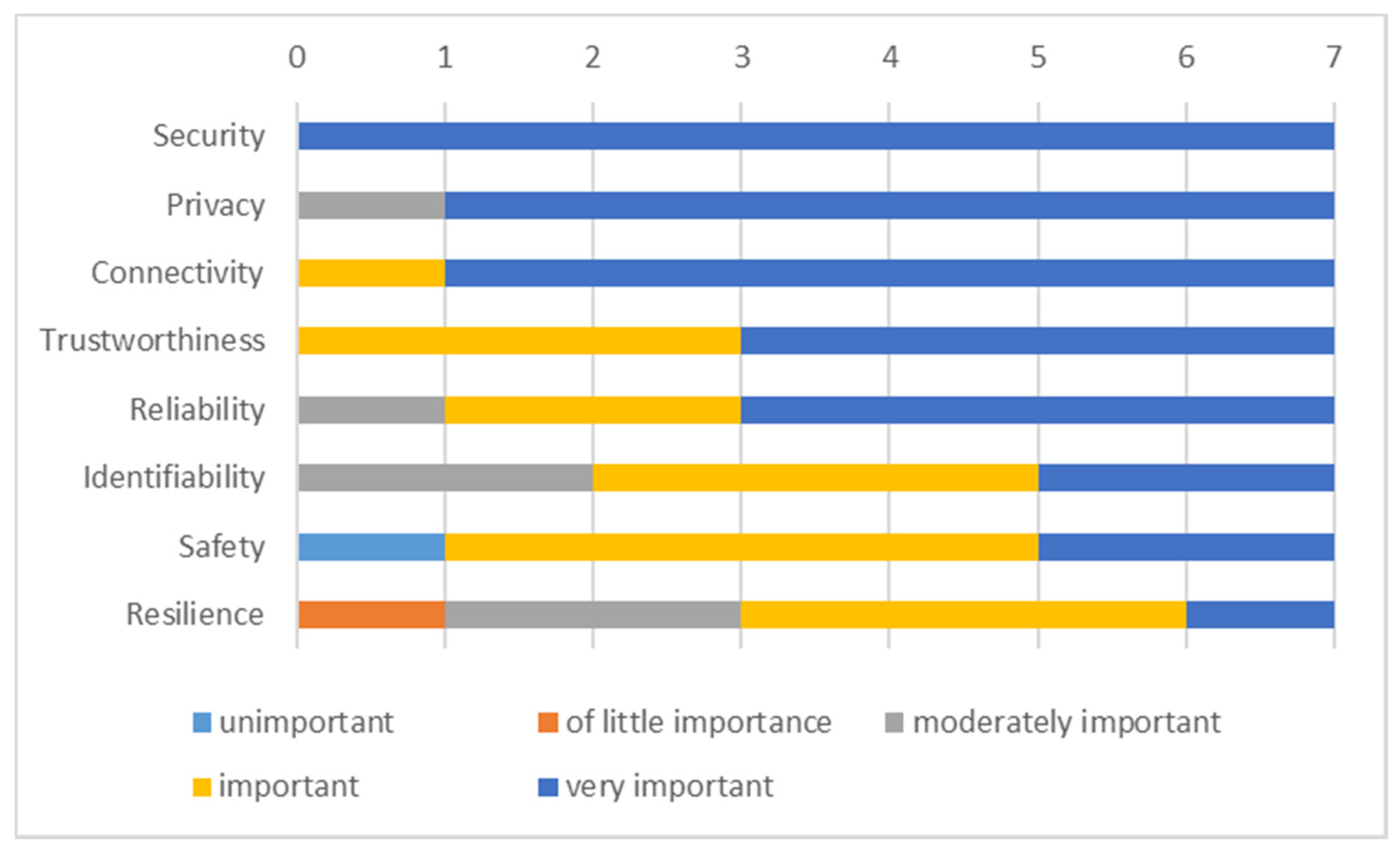
- Identifiability—enables the system to uniquely identify an entity such as device, application, service, communication interface or session, location, or data instance.
- Trustworthiness—reflects confidence and faith in the system. It builds on the reputation of the vendor organization, level of adherence to regulation, law, ethical principle, standards, and essential requirements related to cybersecurity, safety, reliability, and privacy.
- Security—of devices, communication networks, data, and the system is of pivotal importance. The security dimensions (such as access control, authentication, non-repudiation, data confidentiality, communication security, data integrity, availability, and privacy) must be applied to provide end-to-end security.
- Safety—as the ability of a system not to harm persons or objects is strictly regulated and prescribed by standards.
- Privacy—is about enabling the chosen information to stay private. Privacy concerns, such as profiling, localization, tracking, secure data transmission, self-adaptive dynamic data management, and confidentiality have to be adequately addressed. Here, one of the requirements is to follow the European General Data Protection Regulation (GDPR).
- Connectivity—is about connecting the system, composing different devices, and a communication network(s).
- Resilience—is about system reaction and recovery from damaging effects or states caused by power shortage, cyberattack, hardware, or software malfunction.
- Reliability—is about delivering the service following the defined performance specification for a specified period.
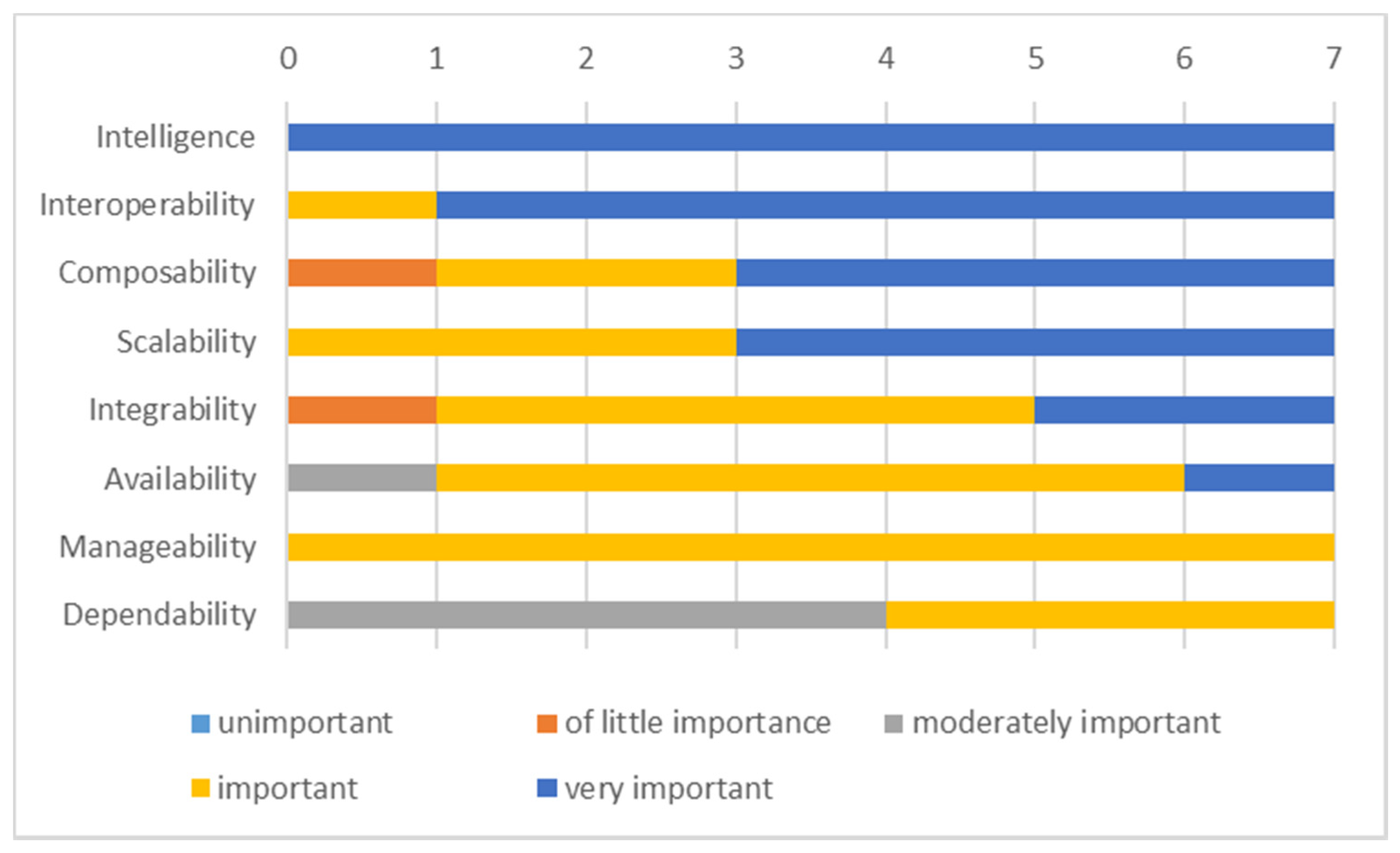
- Interoperability—is the ability of a system to exchange information with other systems.
- Composability—is a design principle promoting the reusability and composition of new services by reusing the existing ones.
- Scalability—is the ability of a system to manage increasing demand, such as new devices or data throughput.
- Integrability—as a degree of effectiveness, the system can be integrated with other systems developed separately.
- Manageability—is a system’s ability to be maintained to perform and run smoothly (thus facilitating reliability, availability, and serviceability).
- Dependability—is the ability to avoid or quickly fix service failures.
- Availability—as a degree to which the system is operational and accessible.
- Intelligence—in terms of Artificial Intelligence (AI) features, functions, and behaviors.
5.3. Discussion
6. Conclusions
7. Future Directions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Byrne, C.A.; Collier, R.; O’Hare, G.M.P. A Review and Classification of Assisted Living Systems. Information 2018, 9, 182. [Google Scholar] [CrossRef] [Green Version]
- Dobre, C.; Mavromoustakis, C.X.; Garcia, N.; Mastorakis, G.; Goleva, R.I. Introduction to the AAL and ELE Systems; Dobre, C., Mavromoustakis, C.X., Garcia, N., Goleva, R.I., Mastorakis, G., Eds.; Ambient Assisted Living and Enhanced Living Environments: Principles, Technologies and Control; Butterworth-Heinemann: Newton, MA, USA, 2016; ISBN 978-0-12-805195-5. [Google Scholar]
- Cicirelli, G.; Marani, R.; Petitti, A.; Milella, A.; D’Orazio, T. Ambient Assisted Living: A Review of Technologies, Methodologies and Future Perspectives for Healthy Aging of Population. Sensors 2021, 21, 3549. [Google Scholar] [CrossRef]
- The Green Paper on Aging, Fostering Solidarity and Responsibility between Generations. Available online: https://ec.europa.eu/info/sites/default/files/1_en_act_part1_v8_0.pdf (accessed on 9 June 2021).
- Expert Group on Health System Performance Assessment. An Overview of Current Approaches and Opportunities for Improvement. Available online: https://ec.europa.eu/health/sites/default/files/systems_performance_assessment/docs/2019_efficiency_en.pdf (accessed on 1 June 2021).
- Oh, H.; Jadad, A.; Rizo, C.; Enkin, M.; Powell, J.; Pagliari, C. What Is eHealth (3): A Systematic Review of Published Definitions. J. Med. Internet Res. 2005, 7, e1. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, D.; Salimi, N. Qualitative and Quantitative Analysis of Definitions of e-Health and m-Health. Health Inform. Res. 2020, 26, 119–128. [Google Scholar] [CrossRef] [PubMed]
- ISO; IEC; IEEE. Systems and software engineering—Architecture description. ISO/IEC/IEEE 2012, 42010, 1–46. [Google Scholar] [CrossRef]
- Reference Model for Service Oriented Architecture 1.0. OASIS Stand. 2006, 12, 18.
- Bass, L.; Clements, P.; Kazman, R. Software Architecture in Practice; Addison-Wesley Professional: Boston, MA, USA, 2003. [Google Scholar]
- Nakagawa, E.Y.; Oquendo, F.; Becker, M. RAModel: A Reference Model for Reference Architectures. In Proceedings of the 2012 Joint Working IEEE/IFIP Conference on Software Architecture and European Conference on Software Architecture, Helsinki, Finland, 20–24 August 2012. [Google Scholar]
- Merilampi, S.; Sirkka, A. Introduction to Smart eHealth and eCare Technologies; CRC Press: London, UK, 2020; pp. 3–84. ISBN 9780367655860. [Google Scholar]
- Islam, S.M.R.; Kwak, D.; Kabir, H.; Hossain, M.; Kwak, K.-S. The Internet of Things for Health Care: A Comprehensive Survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Kodali, R.K.; Swamy, G.; Lakshmi, B. An implementation of IoT for healthcare. IEEE Recent Adv. Intell. Comput. Syst. 2015, 411–416. [Google Scholar] [CrossRef]
- Dang, L.M.; Piran, J.; Han, D.; Min, K.; Moon, H. A Survey on Internet of Things and Cloud Computing for Healthcare. Electronics 2019, 8, 768. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, H.; Arji, G.; Shahmoradi, L.; Safdari, R.; Nilashi, M.; Alizadeh, M. The application of internet of things in healthcare: A systematic literature review and classification. Univers. Access Inf. Soc. 2019, 18, 837–869. [Google Scholar] [CrossRef]
- Greco, L.; Percannella, G.; Ritrovato, P.; Tortorella, F.; Vento, M. Trends in IoT based solutions for health care: Moving AI to the edge. Pattern Recognit. Lett. 2020, 135, 346–353. [Google Scholar] [CrossRef]
- Birje, M.N.; Hanji, S.S. Internet of things based distributed healthcare systems: A review. J. Data Inf. Manag. 2020, 2, 149–165. [Google Scholar] [CrossRef]
- Naresh, V.S.; Pericherla, S.S.; Murty, P.S.R.; Reddi, S. Internet of Things in Healthcare: Architecture, Applications, Challenges, and Solutions. Comput. Syst. Sci. Eng. 2020, 35, 411–421. [Google Scholar] [CrossRef]
- Continua Design Guidelines, Version 2019. Available online: https://members.pchalliance.org/document/dl/2148 (accessed on 6 January 2020).
- Markakis, E.; Nikoloudakis, Y.; Pallis, E.; Manso, M. Security Assessment as a Service Cross-Layered System for the Adoption of Digital, Personalised and Trusted Healthcare. WF-IoT 2019, 91–94. [Google Scholar] [CrossRef]
- Chehri, A.; Mouftah, H.; Jeon, G. A Smart Network Architecture for e-Health Applications. In Intelligent Interactive Multimedia Systems and Services; Tsihrintzis, G.A., Damiani, E., Virvou, M., Howlett, R.J., Jain, L.C., Eds.; Smart Innovation, Systems and Technologies; Springer: Berlin/Heidelberg, Germany, 2010; pp. 157–166. ISBN 978-3-642-14619-0. [Google Scholar]
- Lee, E.A. The Past, Present and Future of Cyber-Physical Systems: A Focus on Models. Sensors 2015, 15, 4837–4869. [Google Scholar] [CrossRef]
- Monostori, L. Cyber-Physical Systems. In CIRP Encyclopedia of Production Engineering; Chatti, S., Tolio, T., Eds.; Springer: Berlin/Heidelberg, Germany, 2018; pp. 1–8. ISBN 978-3-642-35950-7. [Google Scholar]
- Plaza, A.M.; Díaz, J.; Pérez, J. Software architectures for health care cyber-physical systems: A systematic literature review. J. Softw. Evol. Process. 2018, 30, e1930. [Google Scholar] [CrossRef]
- El Murabet, A.; Abtoy, A.; Touhafi, A.; Tahiri, A. Ambient Assisted living system’s models and architectures: A survey of the state of the art. J. King Saud Univ. Comput. Inf. Sci. 2020, 32, 1–10. [Google Scholar] [CrossRef]
- Kara, M.; Lamouchi, O.; Ramdane-Cherif, A. A Quality Model for the Evaluation AAL Systems. Procedia Comput. Sci. 2017, 113, 392–399. [Google Scholar] [CrossRef]
- Di Martino, B.; Rak, M.; Ficco, M.; Esposito, A.; Maisto, S.; Nacchia, S. Internet of things reference architectures, security and interoperability: A survey. Internet Things 2018, 1–2, 99–112. [Google Scholar] [CrossRef]
- Memon, M.; Wagner, S.R.; Pedersen, C.F.; Beevi, F.H.A.; Hansen, F.O. Ambient Assisted Living Healthcare Frameworks, Platforms, Standards, and Quality Attributes. Sensors 2014, 14, 4312–4341. [Google Scholar] [CrossRef] [PubMed]
- Calvaresi, D.; Cesarini, D.; Sernani, P.; Marinoni, M.; Dragoni, A.F.; Sturm, A. Exploring the ambient assisted living domain: A systematic review. J. Ambient. Intell. Humaniz. Comput. 2017, 8, 239–257. [Google Scholar] [CrossRef]
- Nikoloudakis, Y.; Panagiotakis, S.; Markakis, E.; Pallis, E.; Mastorakis, G.; Mavromoustakis, C.X.; Dobre, C. A Fog-Based Emergency System for Smart Enhanced Living Environments. IEEE Cloud Comput. 2016, 3, 54–62. [Google Scholar] [CrossRef]
- Rodriguez, L.M.G.; Ampatzoglou, A.; Avgeriou, P.; Nakagawa, E.Y. A Comparative Analysis of Reference Architectures for Healthcare in the Ambient Assisted Living Domain. In Proceedings of the 2015 IEEE 28th International Symposium on Computer-Based Medical Systems, Sao Carlos, Brazil, 22–25 June 2015. [Google Scholar]
- OpenDei Health and Care Cluster Projects. Available online: https://www.opendei.eu/healthcare-sector/ (accessed on 11 March 2021).
- Project Activage (#732679) Homepage. Available online: https://www.activageproject.eu/ (accessed on 21 May 2021).
- Project Adlife (#875209) Homepage. Available online: https://adlifeproject.com/ (accessed on 21 May 2021).
- Project Gatekeeper (#857223) Homepage. Available online: https://www.gatekeeper-project.eu/ (accessed on 21 May 2021).
- Project Pharaon (#857188) Homepage. Available online: https://www.pharaon.eu/ (accessed on 21 May 2021).
- Project Shapes (#857159) Homepage. Available online: https://shapes2020.eu/ (accessed on 21 May 2021).
- Project Sphinx (#826183) Homepage. Available online: https://sphinx-project.eu/ (accessed on 21 May 2021).
- Project Smart Bear (#857172) Homepage. Available online: https://www.smart-bear.eu/ (accessed on 21 May 2021).
- Muras, J.A.; Cahill, V.; Stokes, E.K. A Taxonomy of Pervasive Healthcare Systems. In Proceedings of the 2006 Pervasive Health Conference and Workshops, Innsbruck, Austria, 29 November–1 December 2006. [Google Scholar]
- Beevi, F.H.A.; Wagner, S.; Hallerstede, S.; Pedersen, C.F. Data Quality Oriented Taxonomy of Ambient Assisted Living Systems. In Proceedings of the IET International Conference on Technologies for Active and Assisted Living (TechAAL), London, UK, 5 November 2015. [Google Scholar]
- CSA OpenDei (#857065) Homepage. Available online: https://www.opendei.eu/ (accessed on 5 March 2021).
- International Data Spaces Association, Reference Architecture Model, Version 3.0. April 2019. Available online: https://www.internationaldataspaces.org/wp-content/uploads/2019/03/IDS-Reference-Architecture-Model-3.0.pdf (accessed on 8 March 2021).
- Industrial Internet Consortium, The Industrial Internet of Things Volume G1: Reference Architecture, v1.9. June 2019. Available online: https://www.iiconsortium.org/IIRA.htm (accessed on 8 March 2021).
- Recommendation ITU-T Y.2060: Next Generation Networks-Frameworks and Functional Architecture Models, Overview of the Internet of Things. Available online: https://www.itu.int/rec/dologin_pub.asp?lang=e&id=T-REC-Y.2060-201206-I!!PDF-E&type=items (accessed on 8 March 2021).
- CREATE-IoT EU H2020 Project. Grant Agreement no. 732929: CREATE-IoT 3D Reference Architecture Model. Available online: https://european-iot-pilots.eu/wp-content/uploads/2019/06/IoT-_European-_Large-Scale_Pilots_Programme_eBook_CREATE-IoT_V02.pdf (accessed on 8 March 2021).
- Reference Architecture Model Industrie 4.0 (RAMI4.0)-DIN SPEC 91345:2016-04. 2016. Available online: https://www.din.de/en/wdc-beuth:din21:250940128 (accessed on 8 March 2021).
- ISO/IEC 30141:2018, Internet of Things (loT)—Reference Architecture. Available online: https://www.iso.org/standard/65695.html (accessed on 8 March 2021).
- CREATE-IoT (#732929) Homepage. Available online: https://european-iot-pilots.eu/project/create-iot/ (accessed on 5 March 2021).
- Vermesan, O.; Eisenhauer, M.; Serrano, M.; Guillemin, P.; Sundmaeker, H.; Tragos, E.Z. The Next Generation Internet of Things–Hyperconnectivity and Embedded Intelligence at the Edge. In Next Generation Internet of Things. Distributed Intelligence at the Edge and Human Machine-to-Machine Cooperation; River Publishers: Gistrup, Denmark, 2019. [Google Scholar]
- Joshi, A.; Kale, S.; Chandel, S.; Pal, D.K. Likert Scale: Explored and Explained. Br. J. Appl. Sci. Technol. 2015, 7, 396–403. [Google Scholar] [CrossRef]
- Nehra, V.; Rungta, U.; Choudhury, B. Blockchain enabled Ambient Assisted living for Critically ill Patients. In Proceedings of the 2021 11th International Conference on Cloud Computing, Data Science & Engineering (Confluence), online, 28–29 January 2021; pp. 575–581. [Google Scholar]
- Arachchige, P.C.M.; Bertok, P.; Khalil, I.; Liu, D.; Camtepe, S.; Atiquzzaman, M. Local Differential Privacy for Deep Learning. IEEE Internet Things J. 2019. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.I.; Butler, K.R.B. Secure Multiparty Computation and Trusted Hardware: Examining Adoption Challenges and Opportunities. Secur. Commun. Netw. 2019. [Google Scholar] [CrossRef] [Green Version]
- Yang, Q.; Liu, Y.; Chen, T.; Tong, Y. Federated Machine Learning: Concept and Applications. ACM Trans. Intell. Syst. Technol. 2019, 10, 12:1–12:19. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Activage | Adlife | Gatekeeper | Pharaon | Shapes | Sphinx | Smart Bear |
|---|---|---|---|---|---|---|---|
| Envisioned types of UI | Mobile, web, embedded | GUI | GUI, robot | GUI, robot | GUI, Digital Assistant | GUI | GUI, Digital Assistant |
| Activities | Daily living, integrated care, monitoring outdoor, emergency triggers, fall prevention, cognitive decline, social isolation, transportation | Communication, self-care, multidisciplinary care team coordination | Early prevention and intervention at a different level | Communication, self-care, transportation | Communication, Self-care, Remote care, Homecare | Communications, Remote care | Communication, Self-care |
| Primary users | Older people, caregivers | People with multiple chronic conditions, informal caregivers, Multidisciplinary care team members | People with multiple chronic conditions (High and moderate risk), general population. | Older people | Elders, Care practitioners, | ICT personnel, General hospital visitors | Elders, medical research teams |
| Source of data for the sensor | Participant, Environment, care provider | Participant, EHR, sensor devices | Participant, EHR, sensor devices | Participant, environment, time | Participants, Sensors devices | Home environment, Medical Sensors devices | Participant, EHR, mobile devices, Smart home sensors |
| The target of the actuator’s action | Participant, caregiver | Participant, caregiver, datastore | Patients, Citizens, caregiver, healthcare provider | Participant, caregiver, datastore | Participant, caregiver, datastore | ICT infrastructure | Participant, datastore |
| Environment | Indoor, Outdoor | Indoor | Indoor, outdoor | Indoor, outdoor | Indoor, outdoor | ICT infrastructure | Indoor, outdoor |
| Areas of use | Communication, health | Communication, health | Communication, health | Communication, health | Communication, health | Communication, health | Communication, health |
| Types of assistance | Training, guidance, monitoring, communicating | Guidance, reminding, communicating, monitoring | Reminding, communicating, monitoring | Reminding, communicating, monitoring | Voice | Guidance, reminding, monitoring |
| Category | Primary Function | Activage | Adlife | Gatekeeper | Pharaon | Shapes | Smart Bear |
|---|---|---|---|---|---|---|---|
| Smart Homes | General Health Monitoring | + | + | + | + | + | |
| Platforms | + | + | + | + | |||
| Intelligent life assistants | Wandering Prevention tools | + | |||||
| Electronic Home Control Systems | + | + | + | + | |||
| Fall Detection Systems | + | + | + | ||||
| Wearables | On-the-body sensors | + | + | + | + | + | + |
| Robotic Assistance | Intelligent Physical Movement Aids | + | |||||
| Health | + | ||||||
| Service and Companion | + | + | + |
| Dimension | Function | Activage | Adlife | Gatekeeper | Pharaon | Shapes | Smart Bear |
|---|---|---|---|---|---|---|---|
| Activities and participation | General tasks and demands | + | + | + | + | ||
| Mobility | + | + | + | + | |||
| Self-service | + | + | + | + | + | + | |
| Communication | + | + | + | + | + | + | |
| Domestic life | + | + | + | + | + | ||
| Data type | Structured | + | + | + | + | + | + |
| Semi-structured | + | + | + | + | |||
| Unstructured | + | ||||||
| Functionality | Monitoring | + | + | + | + | + | + |
| Integrating | + | + | + | + | + | + | |
| Interacting | + | + | + | + | + | + | |
| Acting | + | + | + | + | |||
| Destination of data | Remote server | + | + | + | + | + | |
| Local server | + | + | + | ||||
| Embedded memory | + | + | + | ||||
| Interoperability | Open | + | + | + | + | + | + |
| Closed | |||||||
| Deployment | Wearable | + | + | + | + | ||
| Ambient | + | + | + | + | + | ||
| Data distribution | Live streaming | + | + | + | + | ||
| Store and forward | + | + | + | + | + | + | |
| Type of response | Alarm | + | + | + | + | + | + |
| Data | + | + | + | + | + | + | |
| Assistance | + | + | + | + | + | + |
| CREATE-IoT RAM Layer | Activage Layer | Adlife Layer | Gatekeeper Layer | Pharaon Layer | Shapes Layer | Sphinx Layer | Smart Bear Layer |
|---|---|---|---|---|---|---|---|
| Collaboration and Process layer | Market place, ACTIVAGE Ecosystem, IPSM Alignments | Change Management for Personalised Integrated Care Delivery | GK Layer 5 COMPOSE | Collaboration and Process layer | Market place | A knowledge repository, Common Cybersecurity Toolkit | Continuous cross-pilot collaboration with other projects (Smart4Health, HoloBalance). Management of personalized interventions for six comorbidities. |
| Application Layer | Data Layer | Personalized Care Plan Management and Patient Empowerment Platforms | GK Layer 4 SHARE | Application layer | Front-end Applications | Cybersecurity oriented applications | Web-based front-end for visualizing data and performing data analytics. Mobile application for visualizing participant’s personal data and interventions. |
| Service Layer | Service Layer: Developer tools, Data analytics, Deployer tools | Pilot Design and Implementation | GK Layer 3 FIND | Service layer | Service layer | Service layer | Identification, Authorization, Privacy Management, Data Analytics, Intervention Generation, Data Visualization. |
| Abstraction Layer | Semantic Interoperability layer: AHA ont., AIOTES Core Ont. | Semantic Interoperability Suite | GK Layer 3 FIND | Platform layer | SYMBIOTE, FHIR | STIX 2.1 | Common data model: FHIR; Semantic annotation (SNOMED-CT) |
| Storage Layer | Data Lake, Metadata storage server | FHIR Repository (onFHIR.io) | GK Layer 2 ACCESS | Platform layer | Data Lake, Metadata storage server | - | FHIR compatible repository |
| Processing Layer | Deployment manager, SIL-GW | Clinical Decision Support Services | GK Layer 2 ACCESS | Platform layer | Platform layer | Platform layer, Anonymization | Mobile phone processing; Home-hub server processing. Cloud-servers processing. Pseudo-anonymization. |
| Network Communication Layer | SIL Bridges | Technical Interoperability Suite | GK Networked Things | Device and Network Layer | Device and Network Layer | Device and Network Layer | Device and Network Layer |
| Physical Layer | IoT Platform/device Layer | Medical Devices | GK Networked Things | Device and Network Layer | Device and Network Layer | Device and Network Layer | Device and Network Layer |
| CREATE-IoT RAM Cross-Cutting Functions | Activage | Adlife | Gatekeeper | Pharaon | Shapes | Sphinx | Smart Bear |
|---|---|---|---|---|---|---|---|
| Identifiability | ++ | 0 | 0 | ++ | + | + | + |
| Trustworthiness | + | ++ | ++ | + | ++ | ++ | + |
| Security | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
| Safety | + | + | + | + | ++ | ++ | -- |
| Privacy | ++ | 0 | ++ | ++ | ++ | ++ | ++ |
| Connectivity | ++ | + | ++ | ++ | ++ | ++ | + |
| Resilience | 0 | - | ++ | 0 | + | + | + |
| Reliability | 0 | ++ | ++ | + | ++ | ++ | + |
| CREATE-IoT RAM Property | Activage | Adlife | Gatekeeper | Pharaon | Shapes | Sphinx | Smart Bear |
|---|---|---|---|---|---|---|---|
| Interoperability | ++ | ++ | ++ | ++ | ++ | ++ | + |
| Composability | + | ++ | ++ | ++ | + | ++ | - |
| Scalability | ++ | + | ++ | + | ++ | ++ | + |
| Integrability | + | ++ | + | + | + | ++ | - |
| Manageability | + | + | + | + | + | + | + |
| Dependability | + | + | 0 | 0 | 0 | 0 | + |
| Availability | + | 0 | ++ | + | + | + | + |
| Intelligence | ++ | ++ | ++ | ++ | ++ | ++ | ++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grguric, A.; Khan, O.; Ortega-Gil, A.; Markakis, E.K.; Pozdniakov, K.; Kloukinas, C.; Medrano-Gil, A.M.; Gaeta, E.; Fico, G.; Koloutsou, K. Reference Architectures, Platforms, and Pilots for European Smart and Healthy Living—Analysis and Comparison. Electronics 2021, 10, 1616. https://doi.org/10.3390/electronics10141616
Grguric A, Khan O, Ortega-Gil A, Markakis EK, Pozdniakov K, Kloukinas C, Medrano-Gil AM, Gaeta E, Fico G, Koloutsou K. Reference Architectures, Platforms, and Pilots for European Smart and Healthy Living—Analysis and Comparison. Electronics. 2021; 10(14):1616. https://doi.org/10.3390/electronics10141616
Chicago/Turabian StyleGrguric, Andrej, Omar Khan, Ana Ortega-Gil, Evangelos K. Markakis, Konstantin Pozdniakov, Christos Kloukinas, Alejandro M. Medrano-Gil, Eugenio Gaeta, Giuseppe Fico, and Konstantina Koloutsou. 2021. "Reference Architectures, Platforms, and Pilots for European Smart and Healthy Living—Analysis and Comparison" Electronics 10, no. 14: 1616. https://doi.org/10.3390/electronics10141616