
Vitamin D Alleviates Anxiety and Depression in Elderly People with Prediabetes: A Randomized Controlled Study

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Intervention
2.3. Assessment of Anxiety and Depression Status
2.4. Ethical Considerations
2.5. Statistical Methods
3. Results
3.1. Study Population and Laboratory Markers
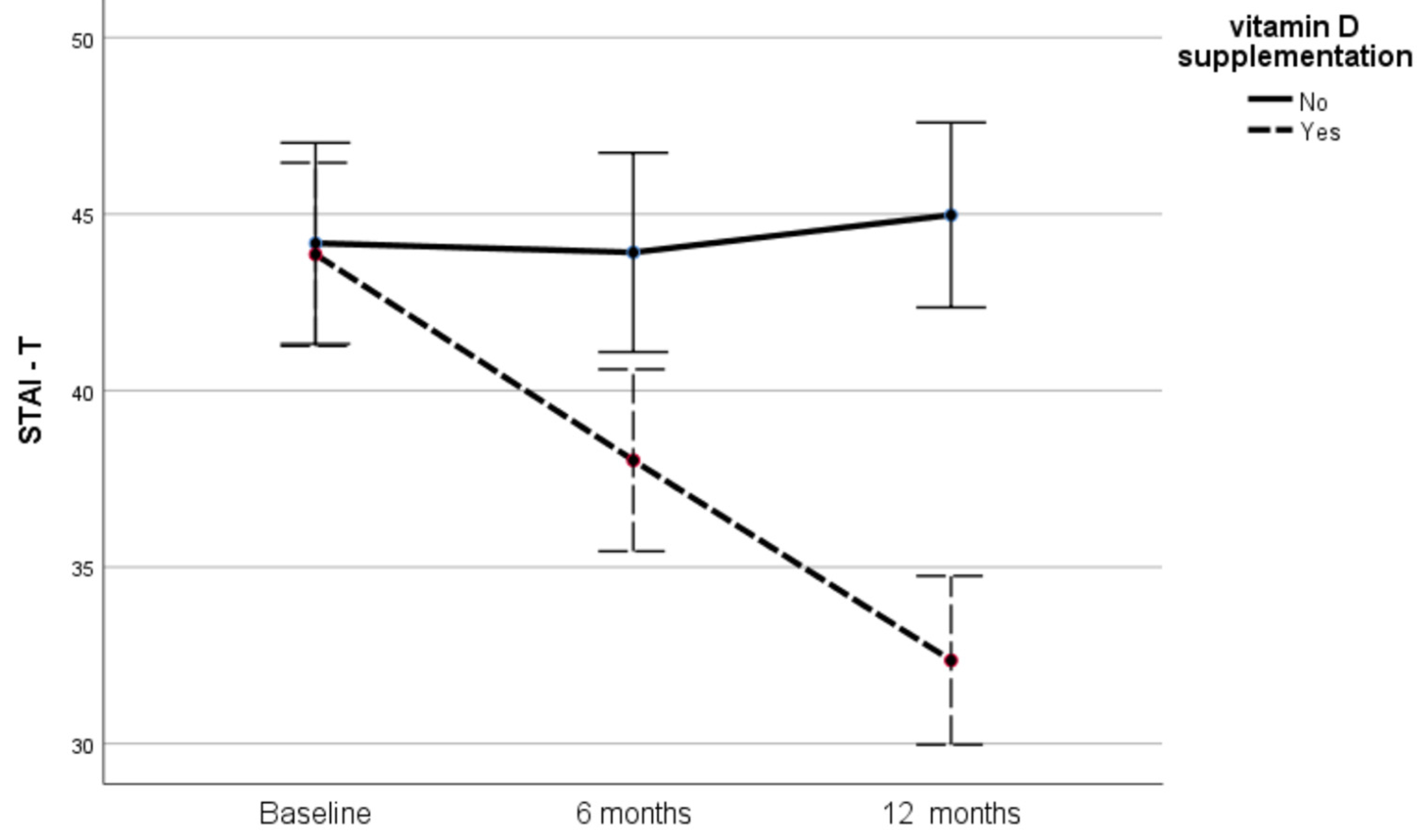
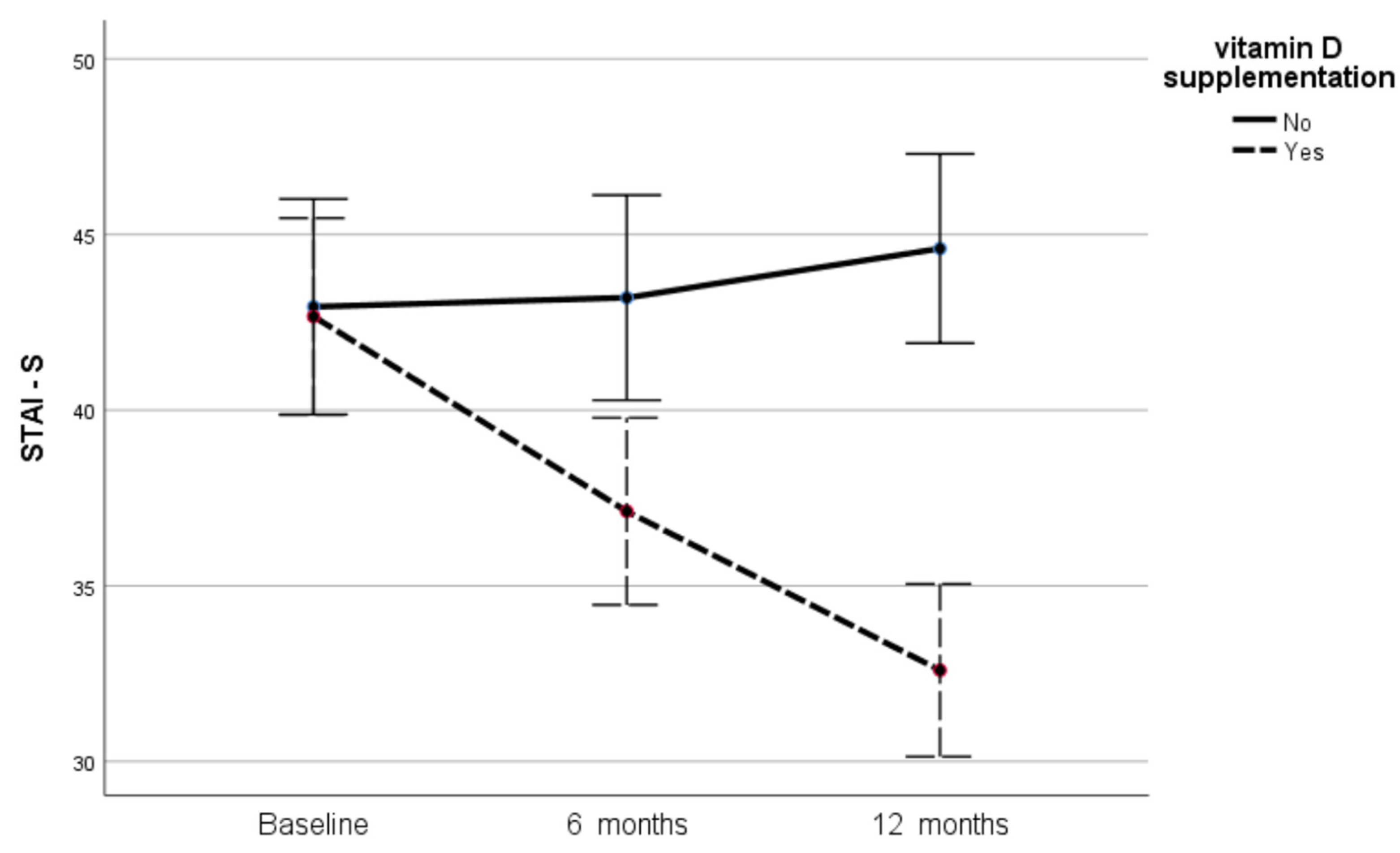
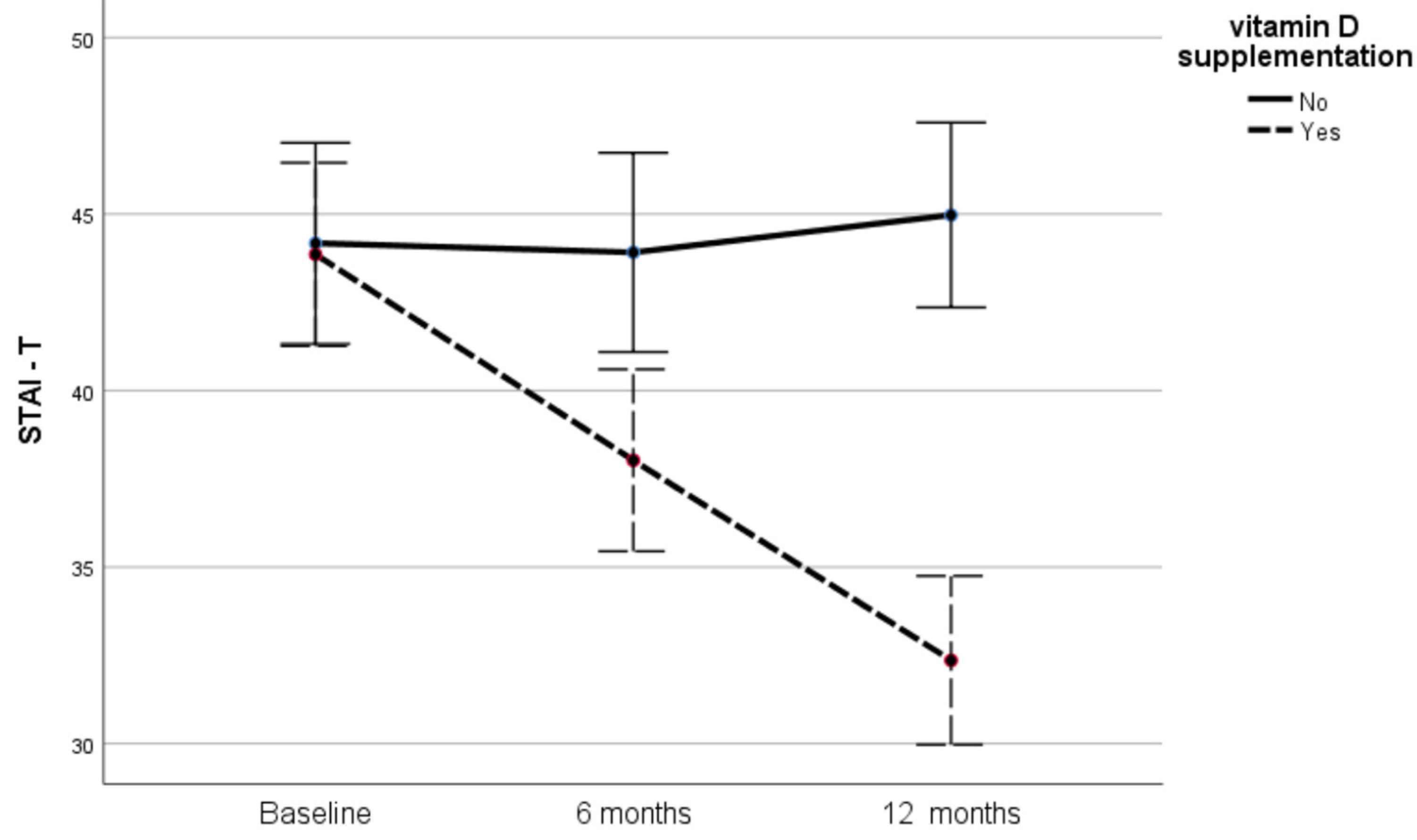
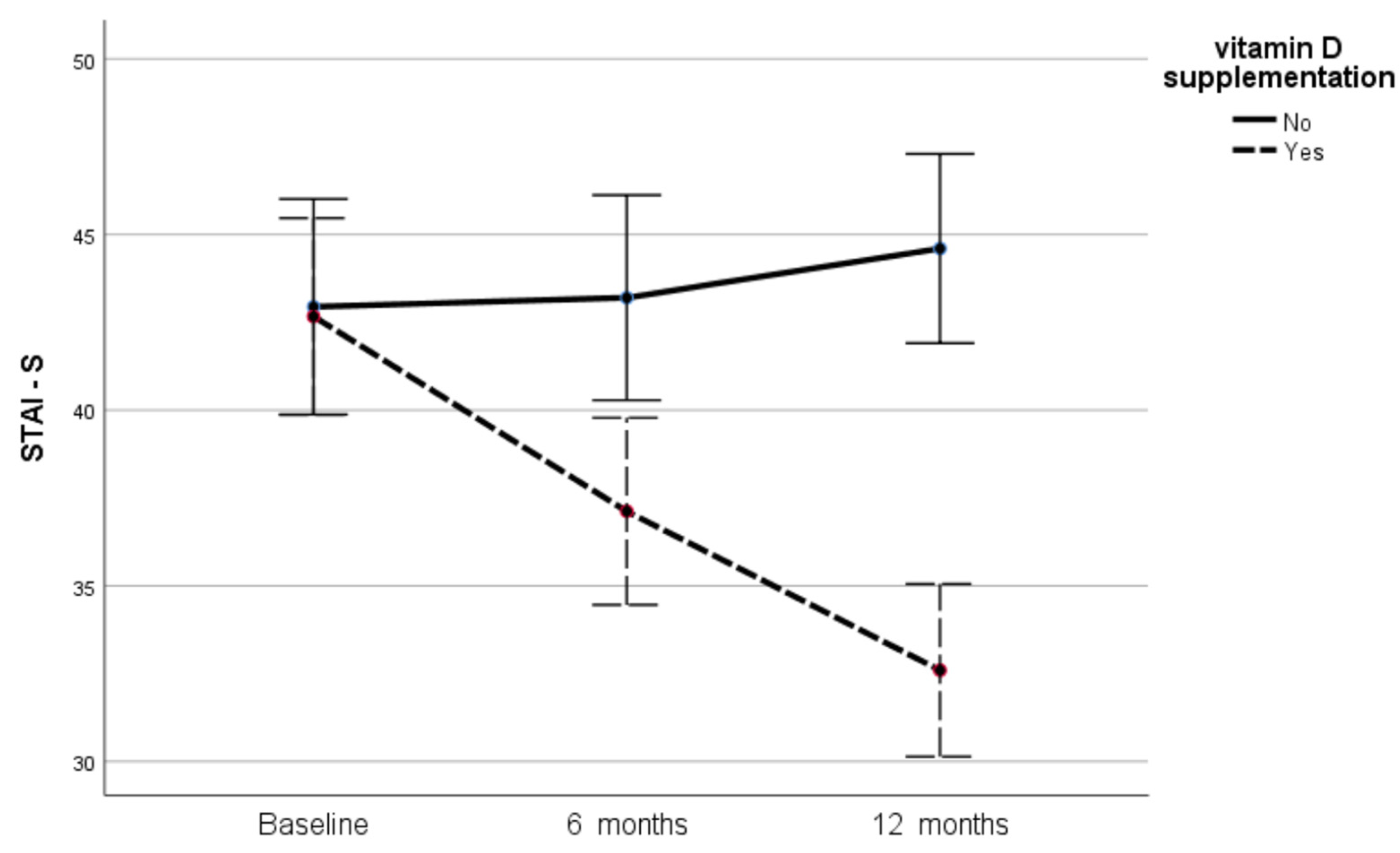
3.2. Effect of Vitamin D on Anxiety
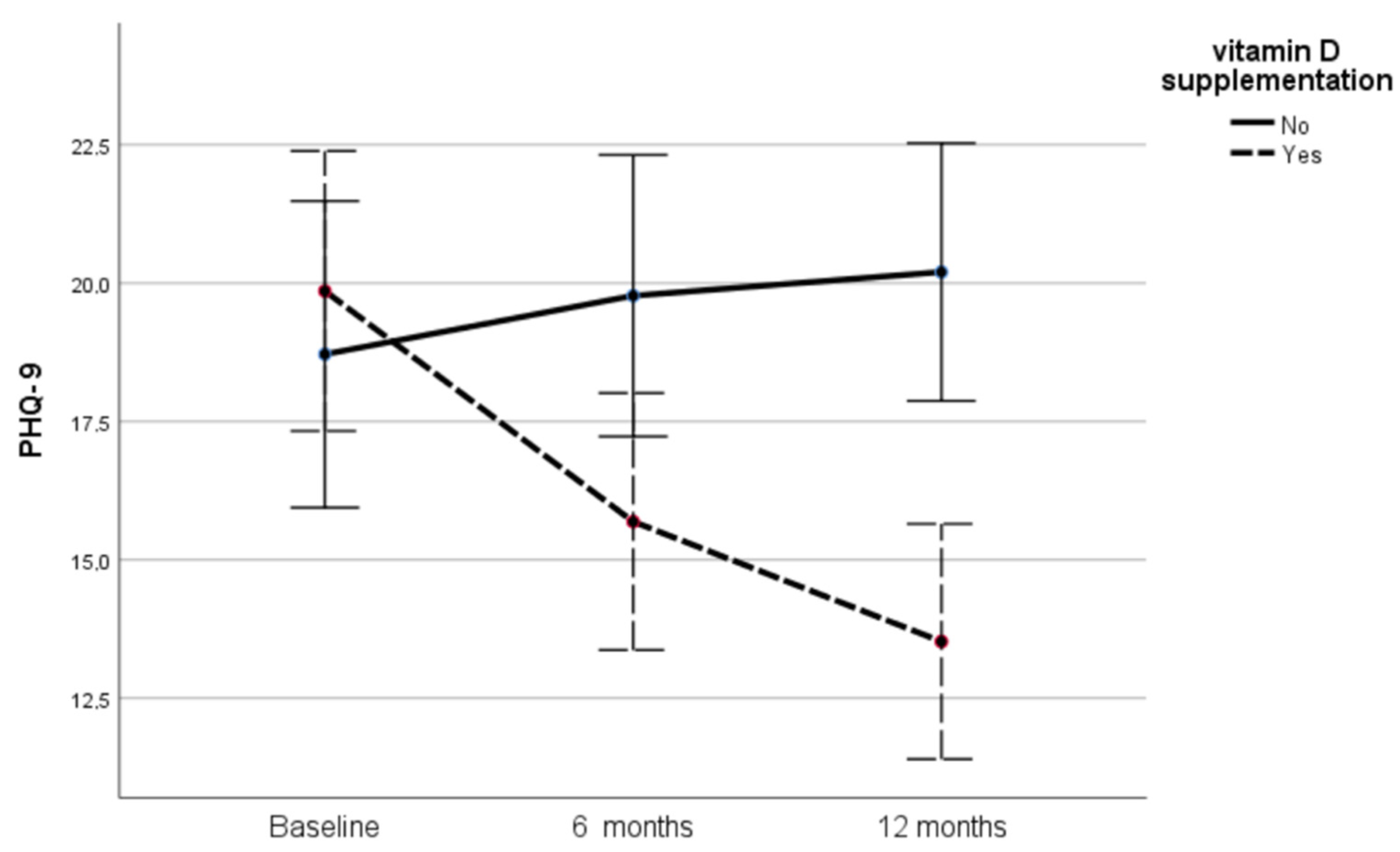
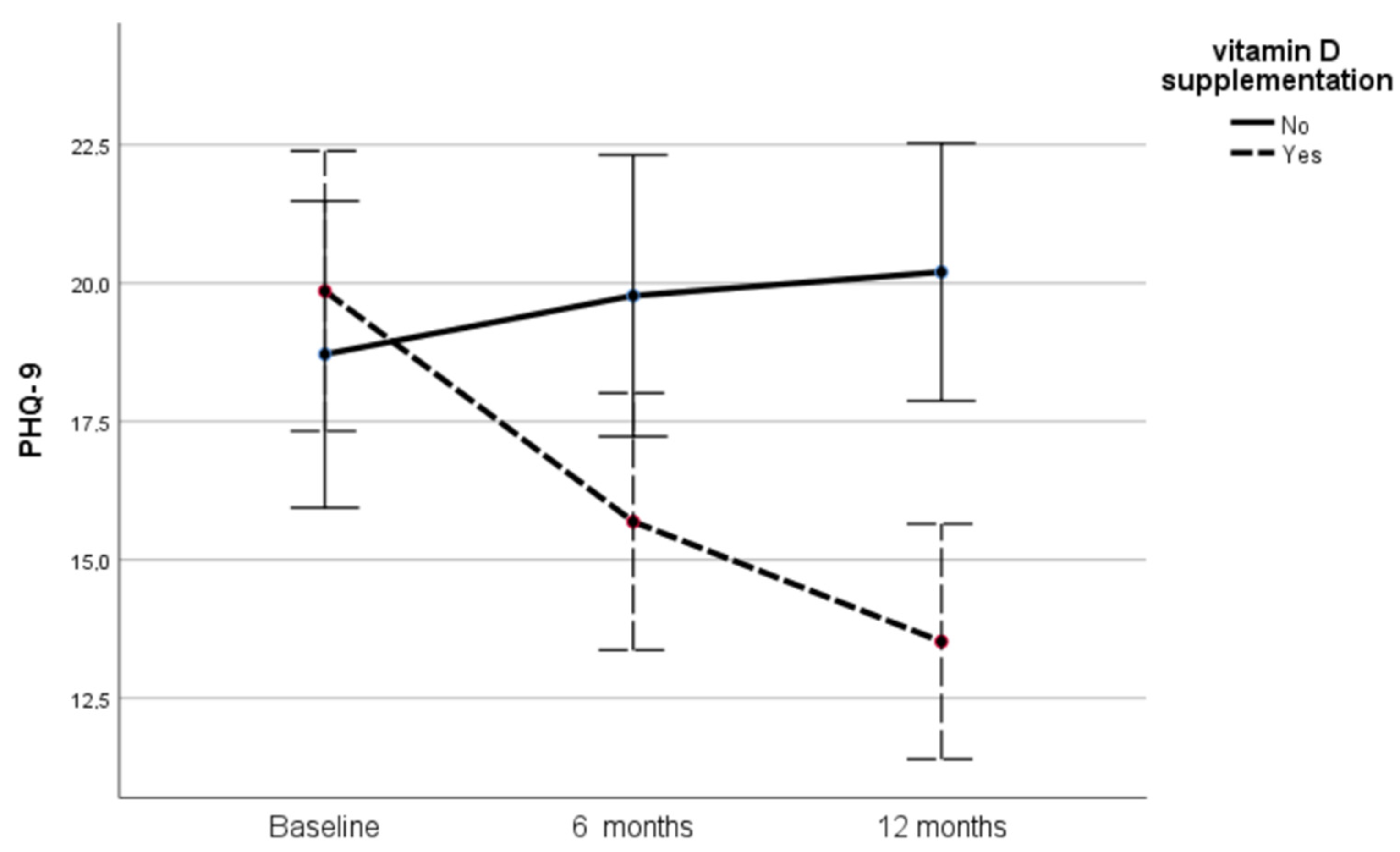
3.3. Effect of Vitamin D on Depression
3.4. Analysis According to 25(OH)D Status
3.5. Intention-to-Treat Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Bruyère, O.; Cavalier, E.; Souberbielle, J.-C.; Bischoff-Ferrari, H.A.; Beaudart, C.; Buckinx, F.; Reginster, J.-Y.; Rizzoli, R. Effects of vitamin D in the elderly population: Current status and perspectives. Arch. Public Health 2014, 72, 32. [Google Scholar] [CrossRef] [PubMed]
- Samefors, M.; Östgren, C.J.; Mölstad, S.; Lannering, C.; Midlöv, P.; Tengblad, A. Vitamin D deficiency in elderly people in Swedish nursing homes is associated with increased mortality. Eur. J. Endocrinol. 2014, 170, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Dhesi, J.K.; Jackson, S.H.D.; Bearne, L.; Moniz, C.; Hurley, M.V.; Swift, C.G.; Allain, T.J. Vitamin D supplementation improves neuromuscular function in older people who fall. Age Ageing 2004, 33, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Manousaki, D.; Rosen, C.; Trajanoska, K.; Rivadeneira, F.; Richards, J.B. The health effects of vitamin D supplementation: Evidence from human studies. Nat. Rev. Endocrinol. 2022, 18, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Lawal, Y.; Bello, F.; Kaoje, Y.S. Prediabetes Deserves More Attention: A Review. Clin. Diabetes 2020, 38, 328–338. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Lucas, M.; Sun, Q.; van Dam, R.; Franco, O.; Manson, J.E.; Willett, W.C.; Ascherio, A.; Hu, F.B. Bidirectional Association Between Depression and Type 2 Diabetes Mellitus in Women. Arch. Intern. Med. 2010, 170, 1884–1891. [Google Scholar] [CrossRef]
- Jiang, L.; Atasoy, S.; Johar, H.; Herder, C.; Peters, A.; Kruse, J.; Ladwig, K. Anxiety boosts progression of prediabetes to type 2 diabetes: Findings from the prospective Cooperative Health Research in the Region of Augsburg F4 and FF4 studies. Diabet. Med. 2020, 37, 1737–1741. [Google Scholar] [CrossRef]
- Bauer, M.E.; Teixeira, A.L. Inflammation in psychiatric disorders: What comes first? Ann. N. Y. Acad. Sci. 2019, 1437, 57–67. [Google Scholar] [CrossRef]
- Lin, E.H.B.; Katon, W.; Von Korff, M.; Rutter, C.; Simon, G.E.; Oliver, M.; Ciechanowski, P.; Ludman, E.J.; Bush, T.; Young, B. Relationship of Depression and Diabetes Self-Care, Medication Adherence, and Preventive Care. Diabetes Care 2004, 27, 2154–2160. [Google Scholar] [CrossRef]
- Koufakis, T.; Grammatiki, M.; Kotsa, K. Type 2 diabetes management in people aged over seventy-five years: Targets and treatment strategies. Maturitas 2021, 143, 118–126. [Google Scholar] [CrossRef]
- Zaromytidou, E.; Koufakis, T.; Dimakopoulos, G.; Drivakou, D.; Konstantinidou, S.; Antonopoulou, V.; Grammatiki, M.; Manthou, E.; Iakovou, I.; Gotzamani-Psarrakou, A.; et al. The effect of vitamin D supplementation on glycemic status of elderly people with prediabetes: A 12-month open-label, randomized-controlled study. Expert Rev. Clin. Pharmacol. 2022, 15, 89–97. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45 (Suppl. 1), S17–S38. [Google Scholar] [CrossRef] [PubMed]
- Joseph, J.J.; Deedwania, P.; Acharya, T.; Aguilar, D.; Bhatt, D.L.; Chyun, D.A.; Di Palo, K.E.; Golden, S.H.; Sperling, L.S. Comprehensive Management of Cardiovascular Risk Factors for Adults with Type 2 Diabetes: A Scientific Statement from the American Heart Association. Circulation 2022, 145, e722–e759. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Papadopoulou, M.; Kleanthous, S.; Papadopoulou, A.; Bizeli, V.; Nimatoudis, I.; Iacovides, A.; Kaprinis, G.S. Reliability and psychometric properties of the Greek translation of the State-Trait Anxiety Inventory form Y: Preliminary data. Ann. Gen. Psychiatry 2006, 5, 2. [Google Scholar] [CrossRef] [PubMed]
- Kayikcioglu, O.; Bilgin, S.; Seymenoglu, G.; Deveci, A. State and Trait Anxiety Scores of Patients Receiving Intravitreal Injections. Biomed. Hub 2017, 2, 1–5. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Karekla, M.; Pilipenko, N.; Feldman, J. Patient Health Questionnaire: Greek language validation and subscale factor structure. Compr. Psychiatry 2012, 53, 1217–1226. [Google Scholar] [CrossRef]
- Manea, L.; Gilbody, S.; McMillan, D. Optimal cut-off score for diagnosing depression with the Patient Health Questionnaire (PHQ-9): A meta-analysis. Can. Med. Assoc. J. 2011, 184, E191–E196. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Weaver, C.M. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Thanapluetiwong, S.; Chewcharat, A.; Takkavatakarn, K.; Praditpornsilpa, K.; Eiam-Ong, S.; Susantitaphong, P. Vitamin D sup-plement on prevention of fall and fracture: A Meta-analysis of Randomized Controlled Trials. Medicine 2020, 99, e21506. [Google Scholar] [CrossRef]
- Zheng, Y.T.; Cui, Q.Q.; Hong, Y.M.; Yao, W.G. A Meta-Analysis of High Dose, Intermittent Vitamin D Supplementation among Older Adults. PLoS ONE 2015, 10, e0115850. [Google Scholar] [CrossRef]
- Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of Daily, Weekly, and Monthly Vitamin D3 in Ethanol Dosing Protocols for Two Months in Elderly Hip Fracture Patients. J. Clin. Endocrinol. Metab. 2008, 93, 3430–3435. [Google Scholar] [CrossRef] [PubMed]
- Rooney, M.R.; Rawlings, A.M.; Pankow, J.S.; Tcheugui, J.B.E.; Coresh, J.; Sharrett, A.R.; Selvin, E. Risk of Progression to Diabetes Among Older Adults with Prediabetes. JAMA Intern. Med. 2021, 181, 511. [Google Scholar] [CrossRef] [PubMed]
- Anglin, R.E.; Samaan, Z.; Walter, S.D.; McDonald, S.D. Vitamin D deficiency and depression in adults: Systematic review and me-ta-analysis. Br. J. Psychiatry 2013, 202, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Menon, V.; Kar, S.K.; Suthar, N.; Nebhinani, N. Vitamin D and Depression: A Critical Appraisal of the Evidence and Future Directions. Indian J. Psychol. Med. 2020, 42, 11–21. [Google Scholar] [CrossRef]
- Alavi, N.M.; Khademalhoseini, S.; Vakili, Z.; Assarian, F. Effect of vitamin D supplementation on depression in elderly patients: A randomized clinical trial. Clin. Nutr. 2019, 38, 2065–2070. [Google Scholar] [CrossRef]
- Rajabi-Naeeni, M.; Dolatian, M.; Qorbani, M.; Vaezi, A.A. Effect of omega-3 and vitamin D co-supplementation on psychological distress in reproductive-aged women with pre-diabetes and hypovitaminosis D: A randomized controlled trial. Brain Behav. 2021, 11, e2342. [Google Scholar] [CrossRef]
- Cheng, Y.C.; Huang, Y.C.; Huang, W.L. The effect of vitamin D supplement on negative emotions: A systematic review and me-ta-analysis. Depress. Anxiety 2020, 37, 549–564. [Google Scholar] [CrossRef]
- Choukri, M.A.; Conner, T.S.; Haszard, J.J.; Harper, M.J.; Houghton, L.A. Effect of vitamin D supplementation on depressive symptoms and psychological wellbeing in healthy adult women: A double-blind randomised controlled clinical trial. J. Nutr. Sci. 2018, 7, e23. [Google Scholar] [CrossRef]
- Jorde, R.; Kubiak, J. No improvement in depressive symptoms by vitamin D supplementation: Results from a randomised con-trolled trial. J. Nutr. Sci. 2018, 7, e30. [Google Scholar] [CrossRef] [Green Version]
- Amani, R.; Fazelian, S.; Paknahad, Z.; Kheiri, S.; Khajehali, L. Effect of Vitamin D supplement on mood status and inflammation in Vitamin D deficient Type 2 diabetic women with anxiety: A randomized clinical trial. Int. J. Prev. Med. 2019, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Berridge, M.J. Vitamin D and Depression: Cellular and Regulatory Mechanisms. Pharmacol. Rev. 2017, 69, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.W.; Burt, A.; Edwards, T.L.; Züchner, S.; Scott, W.K.; Martin, E.R.; Vance, J.M.; Wang, L. Vitamin D Receptor Gene as a Candidate Gene for Parkinson Disease. Ann. Hum. Genet. 2010, 75, 201–210. [Google Scholar] [CrossRef] [PubMed]
- Neto, F.L.; Borges, G.; Torres-Sanchez, S.; Mico, J.A.; Berrocoso, E. Neurotrophins Role in Depression Neurobiology: A Review of Basic and Clinical Evidence. Curr. Neuropharmacol. 2011, 9, 530–552. [Google Scholar] [CrossRef]
- Save, R.; Petrofsky, J.; Alshammari, F.; Khowailed, I.A.; Rodrigues, S.; Potnis, P.; Akerkar, S.; Shah, J.; Chung, G. The effect of acute administration of Vitamin D on micro vascular endothelial function in Caucasians and South Asian Indians. Med. Sci. Monit. 2013, 19, 641–647. [Google Scholar] [CrossRef] [PubMed]
- Kresevic, D.M.; Denton, J.E.; Burant, C.J.; Pallaki, M. Racial Difference in Response to Vitamin D Supplementation. J. Natl. Med. Assoc. 2015, 107, 18–24. [Google Scholar] [CrossRef]
- Hunt, M.; Auriemma, J.; Cashaw, A.C.A. Self-Report Bias and Underreporting of Depression on the BDI-II. J. Pers. Assess. 2003, 80, 26–30. [Google Scholar] [CrossRef]
- Watson, K.T.; Simard, J.F.; Henderson, V.W.; Nutkiewicz, L.; Lamers, F.; Nasca, C.; Rasgon, N.; Penninx, B.W. Incident Major Depressive Disorder Predicted by Three Measures of Insulin Resistance: A Dutch Cohort Study. Am. J. Psychiatry 2021, 178, 914–920. [Google Scholar] [CrossRef]
- Zhuang, Q.; Wu, L.; Ting, W.; Jie, L.; Zou, J.; Du, J. Negative emotions in community-dwelling adults with prediabetes and hyper-tension. J. Int. Med. Res. 2020, 48, 300060520918411. [Google Scholar] [CrossRef]
- Blazer, D.; Burchett, B.; Service, C.; George, L.K. The association of age and depression among the elderly: An epidemiologic ex-ploration. J. Gerontol. 1991, 46, M210–M215. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameter | Vitamin D Supplementation | Mean | Std. Deviation | p-Value |
|---|---|---|---|---|
| Age (years) | No | 74.03 | 7.63 | 0.582 |
| Yes | 73.10 | 7.16 | ||
| Males:Females | No | 10:35 | - | 0.796 |
| Yes | 9:36 | - | ||
| 25(OH)D (ng/mL) | No | 19.85 | 5.72 | 0.931 |
| Yes | 19.98 | 6.73 | ||
| Fasting glucose (mg/dL) | No | 100.09 | 10.56 | 0.407 |
| Yes | 98.71 | 9.40 | ||
| Glycated hemoglobin (%) | No | 5.87 | 0.22 | 0.992 |
| Yes | 5.87 | 0.21 | ||
| Fasting insulin (μΙU/mL) | No | 12.71 | 13.46 | 0.819 |
| Yes | 12.11 | 9.66 | ||
| Weight (kg) | No | 77.22 | 12.96 | 0.428 |
| Yes | 74.86 | 12.97 | ||
| Height (cm) | No | 159.39 | 6.09 | 0.617 |
| Yes | 158.58 | 7.69 | ||
| Waist circumference (cm) | No | 97.91 | 11.26 | 0.795 |
| Yes | 97.17 | 13.46 | ||
| Total body fat (%) | No | 35.00 | 7.60 | 0.463 |
| Yes | 36.00 | 6.30 | ||
| Muscle mass (kg) | No | 46.69 | 9.12 | 0.240 |
| Yes | 44.24 | 8.99 | ||
| Body Mass Index (kg/m2) | No | 30.29 | 4.14 | 0.687 |
| Yes | 29.90 | 4.16 | ||
| Visceral fat (kg) | No | 12.77 | 4.19 | 0.399 |
| Yes | 11.90 | 4.68 |
| STAI-T | Vitamin D Supplementation | Mean | Std. Deviation | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Baseline | No | 44.17 | 5.94 | 41.32 | 47.01 |
| Yes | 43.85 | 9.40 | 41.25 | 46.45 | |
| 6 months | No | 43.91 | 7.18 | 41.09 | 46.73 |
| Yes | 38.02 | 9.03 | 35.44 | 40.60 | |
| 12 months | No | 44.97 | 7.78 | 42.35 | 47.59 |
| Yes | 32.35 | 7.77 | 29.96 | 34.74 | |
| Mean difference (No-Yes) | Sig. | Lower Bound | Upper Bound | ||
| Baseline | 0.31 | 0.87 | −3.54 | 4.16 | |
| 6 months | 5.89 | 0.003 | 2.06 | 9.71 | |
| 12 months | 12.61 | 0.000 | 9.06 | 16.15 | |
| STAI-S | Vitamin D Supplementation | Mean | Std. Deviation | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| baseline | No | 42.94 | 9.14 | 39.87 | 46.01 |
| Yes | 42.66 | 8.43 | 39.86 | 45.46 | |
| 6 months | No | 43.20 | 9.33 | 40.28 | 46.11 |
| Yes | 37.11 | 7.88 | 34.45 | 39.78 | |
| 12 months | No | 44.60 | 9.53 | 41.90 | 47.29 |
| Yes | 32.59 | 6.45 | 30.13 | 35.05 | |
| Mean difference (No-Yes) | Sig. | Lower Bound | Upper Bound | ||
| baseline | 0.27 | 0.89 | −3.87 | 4.42 | |
| 6 months | 6.08 | 0.003 | 2.12 | 10.03 | |
| 12 months | 12.00 | 0.000 | 8.35 | 15.65 | |
| PHQ-9 | Vitamin D Supplementation | Mean | Std. Deviation | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| Baseline | No | 18.71 | 9.01 | 15.94 | 21.48 |
| Yes | 19.85 | 7.37 | 17.32 | 22.38 | |
| 6 months | No | 19.77 | 8.96 | 17.22 | 22.31 |
| Yes | 15.69 | 6.15 | 13.36 | 18.01 | |
| 12 months | No | 20.20 | 8.67 | 17.87 | 22.52 |
| Yes | 13.52 | 5.01 | 11.39 | 15.65 | |
| Mean Difference (No-Yes) | Sig. | Lower Bound | Upper Bound | ||
| Baseline | −1.14 | 0.54 | −4.89 | 2.60 | |
| 6 months | 4.08 | 0.021 | 0.63 | 7.52 | |
| 12 months | 6.67 | 0.000 | 3.52 | 9.83 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zaromytidou, E.; Koufakis, T.; Dimakopoulos, G.; Drivakou, D.; Konstantinidou, S.; Rakitzi, P.; Grammatiki, M.; Manthou, E.; Notopoulos, A.; Iakovou, I.; et al. Vitamin D Alleviates Anxiety and Depression in Elderly People with Prediabetes: A Randomized Controlled Study. Metabolites 2022, 12, 884. https://doi.org/10.3390/metabo12100884
Zaromytidou E, Koufakis T, Dimakopoulos G, Drivakou D, Konstantinidou S, Rakitzi P, Grammatiki M, Manthou E, Notopoulos A, Iakovou I, et al. Vitamin D Alleviates Anxiety and Depression in Elderly People with Prediabetes: A Randomized Controlled Study. Metabolites. 2022; 12(10):884. https://doi.org/10.3390/metabo12100884
Chicago/Turabian StyleZaromytidou, Evangelia, Theocharis Koufakis, Georgios Dimakopoulos, Despina Drivakou, Stavroula Konstantinidou, Pantelitsa Rakitzi, Maria Grammatiki, Eleni Manthou, Athanasios Notopoulos, Ioannis Iakovou, and et al. 2022. "Vitamin D Alleviates Anxiety and Depression in Elderly People with Prediabetes: A Randomized Controlled Study" Metabolites 12, no. 10: 884. https://doi.org/10.3390/metabo12100884
APA StyleZaromytidou, E., Koufakis, T., Dimakopoulos, G., Drivakou, D., Konstantinidou, S., Rakitzi, P., Grammatiki, M., Manthou, E., Notopoulos, A., Iakovou, I., Gotzamani-Psarrakou, A., & Kotsa, K. (2022). Vitamin D Alleviates Anxiety and Depression in Elderly People with Prediabetes: A Randomized Controlled Study. Metabolites, 12(10), 884. https://doi.org/10.3390/metabo12100884