
Somatic Copy-Number Alterations in Plasma Circulating Tumor DNA from Advanced EGFR-Mutated Lung Adenocarcinoma Patients

 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Patient Cohort and Sample Collection
2.2. Blood Collection and Cell-Free DNA Extraction from Plasma
2.3. ddPCR
2.4. Shallow Whole-Genome Plasma Sequencing
- Segment should be <20 Mb;
- Log2-ratio must be >0.2;
- Segment should contain a gene, but not >100 genes;
- Log2-ratio must be 0.2 higher than weighted mean of the log2-ratios of neighboring 20Mb on both the sides if it contains a known tumor driver gene;
- Log2-ratio must be 0.58 higher (Log2-ratio of 0.58 translates to about three copies) than weighted mean of the log2-ratios of neighboring 20Mb on both the sides if it does not contain a known tumor driver gene;
- Segment should not contain segmental duplications in >50% of its size;
- Segment should not overlap with known entries in DGVar.
- Segment should be <20 Mb;
- Log2-ratio must be lower than −0.2;
- Segment should contain a gene known to be affected by deletions;
- Segment should contain a gene but not >100 genes;
- Log2-ratio must be 0.2 lower than weighted mean of the log2-ratios of neighboring 20 Mb on both the sides;
- Segment should not contain segmental duplications in >50% of its size;
- Segment should not overlap with known entries in DGVar.
2.5. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Assessment of SCNAs in Plasma Samples
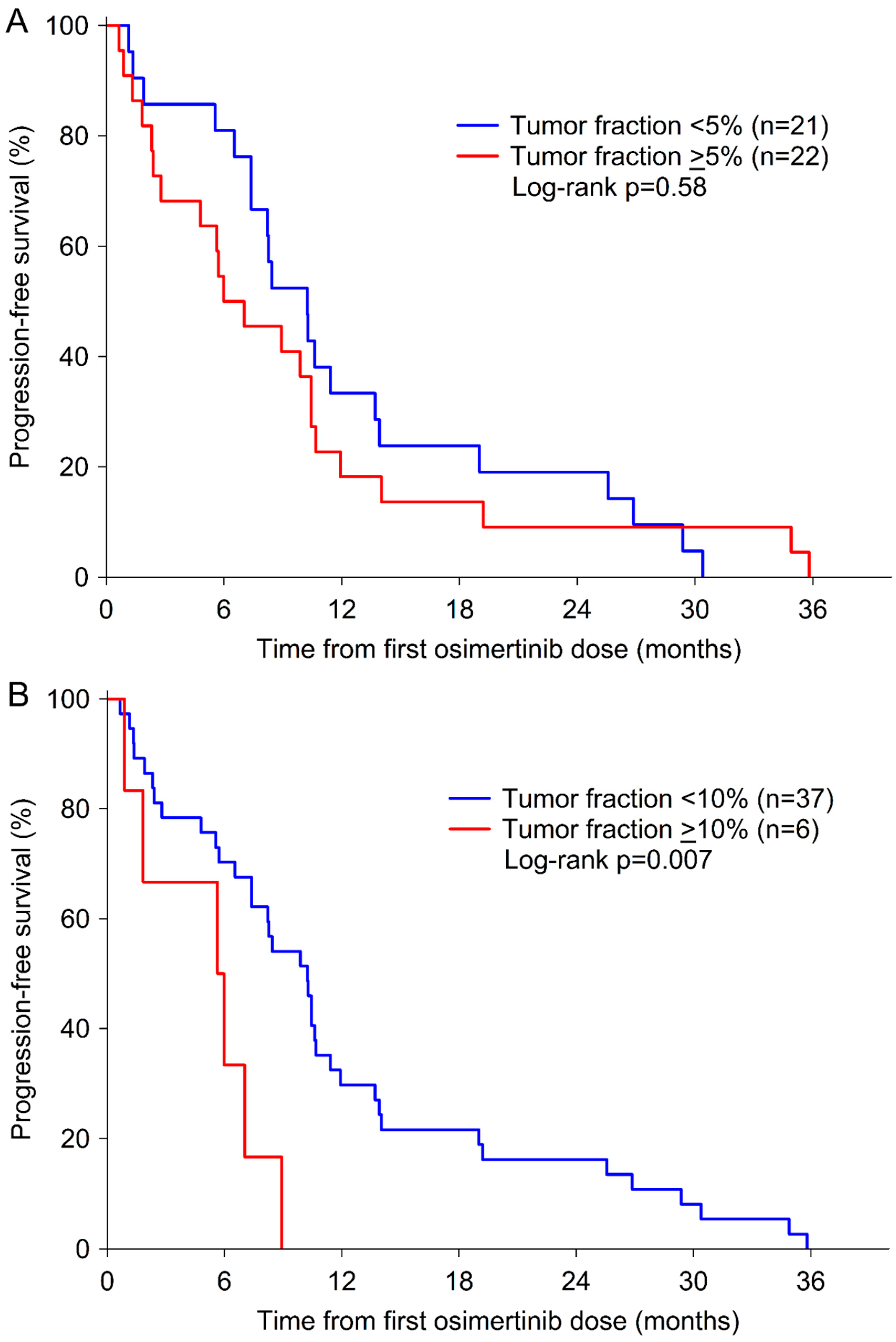
3.3. Clinical Relevance of rrSCNAs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Janne, P.A.; Yang, J.C.; Kim, D.W.; Planchard, D.; Ohe, Y.; Ramalingam, S.S.; Ahn, M.J.; Kim, S.W.; Su, W.C.; Horn, L.; et al. AZD9291 in EGFR inhibitor-resistant non-small-cell lung cancer. N. Engl. J. Med. 2015, 372, 1689–1699. [Google Scholar] [CrossRef]
- Mok, T.S.; Wu, Y.L.; Ahn, M.J.; Garassino, M.C.; Kim, H.R.; Ramalingam, S.S.; Shepherd, F.A.; He, Y.; Akamatsu, H.; Theelen, W.S.; et al. Osimertinib or Platinum-Pemetrexed in EGFR T790M-Positive Lung Cancer. N. Engl. J. Med. 2017, 376, 629–640. [Google Scholar] [CrossRef] [Green Version]
- Goss, G.; Tsai, C.M.; Shepherd, F.A.; Bazhenova, L.; Lee, J.S.; Chang, G.C.; Crino, L.; Satouchi, M.; Chu, Q.; Hida, T.; et al. Osimertinib for pretreated EGFR Thr790Met-positive advanced non-small-cell lung cancer (AURA2): A multicentre, open-label, single-arm, phase 2 study. Lancet Oncol. 2016, 17, 1643–1652. [Google Scholar] [CrossRef]
- Soria, J.C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef]
- Murtuza, A.; Bulbul, A.; Shen, J.P.; Keshavarzian, P.; Woodward, B.D.; Lopez-Diaz, F.J.; Lippman, S.M.; Husain, H. Novel Third-Generation EGFR Tyrosine Kinase Inhibitors and Strategies to Overcome Therapeutic Resistance in Lung Cancer. Cancer Res. 2019, 79, 689–698. [Google Scholar] [CrossRef] [Green Version]
- Thress, K.S.; Paweletz, C.P.; Felip, E.; Cho, B.C.; Stetson, D.; Dougherty, B.; Lai, Z.; Markovets, A.; Vivancos, A.; Kuang, Y.; et al. Acquired EGFR C797S mutation mediates resistance to AZD9291 in non-small cell lung cancer harboring EGFR T790M. Nat. Med. 2015, 21, 560–562. [Google Scholar] [CrossRef] [Green Version]
- Oxnard, G.R.; Hu, Y.; Mileham, K.F.; Husain, H.; Costa, D.B.; Tracy, P.; Feeney, N.; Sholl, L.M.; Dahlberg, S.E.; Redig, A.J.; et al. Assessment of Resistance Mechanisms and Clinical Implications in Patients With EGFR T790M-Positive Lung Cancer and Acquired Resistance to Osimertinib. JAMA Oncol. 2018, 4, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Planchard, D.; Boyer, M.J.; Lee, J.S.; Dechaphunkul, A.; Cheema, P.K.; Takahashi, T.; Gray, J.E.; Tiseo, M.; Ramalingam, S.S.; Todd, A.; et al. Postprogression Outcomes for Osimertinib versus Standard-of-Care EGFR-TKI in Patients with Previously Untreated EGFR-mutated Advanced Non-Small Cell Lung Cancer. Clin. Cancer Res. 2019, 25, 2058–2063. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Cheng, Y.; Zhou, C.; Ohe, Y.; Imamura, F.; Cho, B.C.; Lin, M.C.; Majem, M.; Shah, R.; Rukazenkov, Y.; et al. LBA50Mechanisms of acquired resistance to first-line osimertinib: Preliminary data from the phase III FLAURA study. Ann. Oncol. 2018, 29. [Google Scholar] [CrossRef]
- Yang, Z.; Yang, N.; Ou, Q.; Xiang, Y.; Jiang, T.; Wu, X.; Bao, H.; Tong, X.; Wang, X.; Shao, Y.W.; et al. Investigating Novel Resistance Mechanisms to Third-Generation EGFR Tyrosine Kinase Inhibitor Osimertinib in Non-Small Cell Lung Cancer Patients. Clin. Cancer Res. 2018, 24, 3097–3107. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; Zhang, X.C.; Yang, J.J.; Yang, Z.F.; Bai, Y.; Su, J.; Wang, Z.; Zhang, Z.; Shao, Y.; Zhou, Q.; et al. EGFR L792H and G796R: Two Novel Mutations Mediating Resistance to the Third-Generation EGFR Tyrosine Kinase Inhibitor Osimertinib. J. Thorac. Oncol. 2018, 13, 1415–1421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, D.; Hu, M.; Bai, Y.; Zhu, X.; Lu, X.; Wu, C.; Wang, J.; Liu, L.; Wang, Z.; Ni, J.; et al. EGFR G796D mutation mediates resistance to osimertinib. Oncotarget 2017, 8, 49671–49679. [Google Scholar] [CrossRef] [Green Version]
- Ramalingam, S.S.; Yang, J.C.; Lee, C.K.; Kurata, T.; Kim, D.W.; John, T.; Nogami, N.; Ohe, Y.; Mann, H.; Rukazenkov, Y.; et al. Osimertinib As First-Line Treatment of EGFR Mutation-Positive Advanced Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2018, 36, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Menon, R.; Muller, J.; Schneider, P.; Lakis, S.; Thress, K.; Wolf, J.; Heukamp, L.; Heuckmann, J.M.; Griesinger, F. A Novel EGFR(C797) Variant Detected in a Pleural Biopsy Specimen from an Osimertinib-Treated Patient Using a Comprehensive Hybrid Capture-Based Next-Generation Sequencing Assay. J. Thorac. Oncol. 2016, 11, e105–e107. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Loriot, Y.; Andre, F.; Gobert, A.; Auger, N.; Lacroix, L.; Soria, J.C. EGFR-independent mechanisms of acquired resistance to AZD9291 in EGFR T790M-positive NSCLC patients. Ann. Oncol. 2015, 26, 2073–2078. [Google Scholar] [CrossRef]
- Ortiz-Cuaran, S.; Scheffler, M.; Plenker, D.; Dahmen, L.; Scheel, A.H.; Fernandez-Cuesta, L.; Meder, L.; Lovly, C.M.; Persigehl, T.; Merkelbach-Bruse, S.; et al. Heterogeneous Mechanisms of Primary and Acquired Resistance to Third-Generation EGFR Inhibitors. Clin. Cancer Res. 2016, 22, 4837–4847. [Google Scholar] [CrossRef] [Green Version]
- Minari, R.; Bordi, P.; La Monica, S.; Squadrilli, A.; Leonetti, A.; Bottarelli, L.; Azzoni, C.; Lagrasta, C.A.M.; Gnetti, L.; Campanini, N.; et al. Concurrent Acquired BRAF V600E Mutation and MET Amplification as Resistance Mechanism of First-Line Osimertinib Treatment in a Patient with EGFR-Mutated NSCLC. J. Thorac. Oncol. 2018, 13, e89–e91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ou, S.I.; Agarwal, N.; Ali, S.M. High MET amplification level as a resistance mechanism to osimertinib (AZD9291) in a patient that symptomatically responded to crizotinib treatment post-osimertinib progression. Lung Cancer 2016, 98, 59–61. [Google Scholar] [CrossRef]
- Eberlein, C.A.; Stetson, D.; Markovets, A.A.; Al-Kadhimi, K.J.; Lai, Z.; Fisher, P.R.; Meador, C.B.; Spitzler, P.; Ichihara, E.; Ross, S.J.; et al. Acquired Resistance to the Mutant-Selective EGFR Inhibitor AZD9291 is Associated with Increased Dependence on RAS Signaling in Preclinical Models. Cancer Res. 2015, 75, 2489–2500. [Google Scholar] [CrossRef] [Green Version]
- Ho, C.C.; Liao, W.Y.; Lin, C.A.; Shih, J.Y.; Yu, C.J.; Yang, J.C. Acquired BRAF V600E Mutation as Resistant Mechanism after Treatment with Osimertinib. J. Thorac. Oncol. 2017, 12, 567–572. [Google Scholar] [CrossRef] [Green Version]
- Blakely, C.M.; Watkins, T.B.K.; Wu, W.; Gini, B.; Chabon, J.J.; McCoach, C.E.; McGranahan, N.; Wilson, G.A.; Birkbak, N.J.; Olivas, V.R.; et al. Evolution and clinical impact of co-occurring genetic alterations in advanced-stage EGFR-mutant lung cancers. Nat. Genet. 2017, 49, 1693–1704. [Google Scholar] [CrossRef]
- Minari, R.; Bordi, P.; Del Re, M.; Facchinetti, F.; Mazzoni, F.; Barbieri, F.; Camerini, A.; Comin, C.E.; Gnetti, L.; Azzoni, C.; et al. Primary resistance to osimertinib due to SCLC transformation: Issue of T790M determination on liquid re-biopsy. Lung Cancer 2018, 115, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.M.; Song, A.; Kim, D.W.; Kim, S.; Ahn, Y.O.; Keam, B.; Jeon, Y.K.; Lee, S.H.; Chung, D.H.; Heo, D.S. Mechanisms of Acquired Resistance to AZD9291: A Mutation-Selective, Irreversible EGFR Inhibitor. J. Thorac. Oncol. 2015, 10, 1736–1744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ham, J.S.; Kim, S.; Kim, H.K.; Byeon, S.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Park, K.; Choi, Y.L.; Han, J.; et al. Two Cases of Small Cell Lung Cancer Transformation from EGFR Mutant Adenocarcinoma During AZD9291 Treatment. J. Thorac. Oncol. 2016, 11, e1–e4. [Google Scholar] [CrossRef] [Green Version]
- Buder, A.; Tomuta, C.; Filipits, M. The potential of liquid biopsies. Curr. Opin. Oncol. 2016, 28, 130–134. [Google Scholar] [CrossRef]
- Heitzer, E.; Haque, I.S.; Roberts, C.E.S.; Speicher, M.R. Current and future perspectives of liquid biopsies in genomics-driven oncology. Nat. Rev. Genet. 2019, 20, 71–88. [Google Scholar] [CrossRef]
- Buder, A.; Hochmair, M.J.; Schwab, S.; Bundalo, T.; Schenk, P.; Errhalt, P.; Mikes, R.E.; Absenger, G.; Patocka, K.; Baumgartner, B.; et al. Cell-Free Plasma DNA-Guided Treatment With Osimertinib in Patients With Advanced EGFR-Mutated NSCLC. J. Thorac. Oncol. 2018, 13, 821–830. [Google Scholar] [CrossRef] [Green Version]
- Hochmair, M.J.; Buder, A.; Schwab, S.; Burghuber, O.C.; Prosch, H.; Hilbe, W.; Cseh, A.; Fritz, R.; Filipits, M. Liquid-Biopsy-Based Identification of EGFR T790M Mutation-Mediated Resistance to Afatinib Treatment in Patients with Advanced EGFR Mutation-Positive NSCLC, and Subsequent Response to Osimertinib. Target. Oncol. 2019, 14, 75–83. [Google Scholar] [CrossRef] [Green Version]
- Buder, A.; Setinek, U.; Hochmair, M.J.; Schwab, S.; Kirchbacher, K.; Keck, A.; Burghuber, O.C.; Pirker, R.; Filipits, M. EGFR Mutations in Cell-free Plasma DNA from Patients with Advanced Lung Adenocarcinoma: Improved Detection by Droplet Digital PCR. Target. Oncol. 2019, 14, 197–203. [Google Scholar] [CrossRef] [Green Version]
- Buder, A.; Hochmair, M.J.; Setinek, U.; Pirker, R.; Filipits, M. EGFR mutation tracking predicts survival in advanced EGFR-mutated non-small cell lung cancer patients treated with osimertinib. Transl. Lung Cancer Res. 2020, 9, 239–245. [Google Scholar] [CrossRef]
- Heitzer, E.; Ulz, P.; Belic, J.; Gutschi, S.; Quehenberger, F.; Fischereder, K.; Benezeder, T.; Auer, M.; Pischler, C.; Mannweiler, S.; et al. Tumor-associated copy number changes in the circulation of patients with prostate cancer identified through whole-genome sequencing. Genome Med. 2013, 5, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulz, P.; Belic, J.; Graf, R.; Auer, M.; Lafer, I.; Fischereder, K.; Webersinke, G.; Pummer, K.; Augustin, H.; Pichler, M.; et al. Whole-genome plasma sequencing reveals focal amplifications as a driving force in metastatic prostate cancer. Nat. Commun. 2016, 7, 12008. [Google Scholar] [CrossRef] [PubMed]
- Adalsteinsson, V.A.; Ha, G.; Freeman, S.S.; Choudhury, A.D.; Stover, D.G.; Parsons, H.A.; Gydush, G.; Reed, S.C.; Rotem, D.; Rhoades, J.; et al. Scalable whole-exome sequencing of cell-free DNA reveals high concordance with metastatic tumors. Nat. Commun. 2017, 8, 1324. [Google Scholar] [CrossRef] [Green Version]
- Belic, J.; Graf, R.; Bauernhofer, T.; Cherkas, Y.; Ulz, P.; Waldispuehl-Geigl, J.; Perakis, S.; Gormley, M.; Patel, J.; Li, W.; et al. Genomic alterations in plasma DNA from patients with metastasized prostate cancer receiving abiraterone or enzalutamide. Int. J. Cancer 2018, 143, 1236–1248. [Google Scholar] [CrossRef]
- Mohan, S.; Heitzer, E.; Ulz, P.; Lafer, I.; Lax, S.; Auer, M.; Pichler, M.; Gerger, A.; Eisner, F.; Hoefler, G.; et al. Changes in colorectal carcinoma genomes under anti-EGFR therapy identified by whole-genome plasma DNA sequencing. PLoS Genet. 2014, 10, e1004271. [Google Scholar] [CrossRef]
- Knebel, F.H.; Bettoni, F.; Shimada, A.K.; Cruz, M.; Alessi, J.V.; Negrao, M.V.; Reis, L.F.L.; Katz, A.; Camargo, A.A. Sequential liquid biopsies reveal dynamic alterations of EGFR driver mutations and indicate EGFR amplification as a new mechanism of resistance to osimertinib in NSCLC. Lung Cancer 2017, 108, 238–241. [Google Scholar] [CrossRef] [PubMed]
- Nukaga, S.; Yasuda, H.; Tsuchihara, K.; Hamamoto, J.; Masuzawa, K.; Kawada, I.; Naoki, K.; Matsumoto, S.; Mimaki, S.; Ikemura, S.; et al. Amplification of EGFR Wild-Type Alleles in Non-Small Cell Lung Cancer Cells Confers Acquired Resistance to Mutation-Selective EGFR Tyrosine Kinase Inhibitors. Cancer Res. 2017, 77, 2078–2089. [Google Scholar] [CrossRef] [Green Version]
- Shi, Y.; Xing, P.; Han, X.; Wang, S.; Liu, Y.; Liu, P.; Li, J.; Chang, L.; Guan, Y.; Zhang, Z.; et al. P1.13-18 Exploring the Resistance Mechanism of Osimertinib and Monitoring the Treatment Response Using Plasma ctDNA in Chinese NSCLC Patients. J. Thorac. Oncol. 2018, 13, S589. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.A.; Suzawa, K.; Jordan, E.; Zehir, A.; Ni, A.; Kim, R.; Kris, M.G.; Hellmann, M.D.; Li, B.T.; Somwar, R.; et al. Concurrent Alterations in EGFR-Mutant Lung Cancers Associated with Resistance to EGFR Kinase Inhibitors and Characterization of MTOR as a Mediator of Resistance. Clin. Cancer Res. 2018, 24, 3108–3118. [Google Scholar] [CrossRef] [Green Version]
- Le, X.; Puri, S.; Negrao, M.V.; Nilsson, M.B.; Robichaux, J.; Boyle, T.; Hicks, J.K.; Lovinger, K.L.; Roarty, E.; Rinsurongkawong, W.; et al. Landscape of EGFR-Dependent and -Independent Resistance Mechanisms to Osimertinib and Continuation Therapy Beyond Progression in EGFR-Mutant NSCLC. Clin. Cancer Res. 2018, 24, 6195–6203. [Google Scholar] [CrossRef] [Green Version]
- Drilon, A.; Cappuzzo, F.; Ou, S.I.; Camidge, D.R. Targeting MET in Lung Cancer: Will Expectations Finally Be MET? J. Thorac. Oncol. 2017, 12, 15–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noronha, V.; Patil, V.M.; Joshi, A.; Menon, N.; Chougule, A.; Mahajan, A.; Janu, A.; Purandare, N.; Kumar, R.; More, S.; et al. Gefitinib Versus Gefitinib Plus Pemetrexed and Carboplatin Chemotherapy in EGFR-Mutated Lung Cancer. J. Clin. Oncol. 2020, 38, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Hosomi, Y.; Morita, S.; Sugawara, S.; Kato, T.; Fukuhara, T.; Gemma, A.; Takahashi, K.; Fujita, Y.; Harada, T.; Minato, K.; et al. Gefitinib Alone Versus Gefitinib Plus Chemotherapy for Non-Small-Cell Lung Cancer With Mutated Epidermal Growth Factor Receptor: NEJ009 Study. J. Clin. Oncol. 2020, 38, 115–123. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Clinical Characteristics | No. of Patients n = 31 | No rrSCNAs n = 21 | rrSCNAs n = 10 | p-Value |
|---|---|---|---|---|
| Age | 0.88 | |||
| Median (range)—years | 66 (48–83) | 66 (48–83) | 65 (54–77) | |
| <65 years | 13 (42%) | 9 (43%) | 4 (40%) | |
| ≥65 years | 18 (58%) | 12 (57%) | 6 (60%) | |
| Sex | 0.21 | |||
| Female | 20 (65%) | 12 (57%) | 8 (80%) | |
| Male | 11 (35%) | 9 (43%) | 2 (20%) | |
| Metastases at diagnosis | 0.06 | |||
| M1a | 6 (19%) | 6 (29%) | 0 (0%) | |
| M1b | 25 (81%) | 15 (71%) | 10 (100%) | |
| EGFR tissue genotype | 0.77 | |||
| Exon 19 deletion | 21 (68%) | 15 (71%) | 6 (60%) | |
| L858R | 8 (26%) | 5 (24%) | 3 (30%) | |
| L861Q | 2 (7%) | 1 (5%) | 1 (10%) | |
| Previous EGFR-TKI therapy | 0.82 | |||
| Afatinib | 13 (42%) | 10 (48%) | 3 (30%) | |
| Erlotinib | 3 (10%) | 2 (10%) | 1 (10%) | |
| Gefitinib | 10 (32%) | 6 (28%) | 4 (40%) | |
| >1 EGFR-TKI | 5 (16%) | 3 (14%) | 2 (20%) | |
| Tumor fraction | <0.0001 | |||
| Median (range) | 5.7 (1.6–42.4) | 5.1 (1.6–8.7) | 17.0 (6.9–42.4) |
| Patient | Pre-Osimertinib | Osimertinib Resistance | ||||
|---|---|---|---|---|---|---|
| EGFR Mutation | rrSCNAs | Tumor Fraction | EGFR Mutation | rrSCNAs | Tumor Fraction | |
| Case 1 | L858R, T790M | No rrSCNAs | 4.5% | L858R, T790M | MET | 7.4% |
| Case 2 | del19, T790M | No rrSCNAs | 3.0% | del19, T790M | No rrSCNAs | 4.1% |
| Case 3 | T790M | No rrSCNAs | 4.5% | - | No rrSCNAs | 4.5% |
| Case 4 | del19, T790M | MDM2 | 7.2% | del19, T790M | No rrSCNAs | 5.0% |
| Case 5 | T790M | No rrSCNAs | 5.0% | del19, C797S | No rrSCNAs | 3.9% |
| Case 6 | del19, T790M | No rrSCNAs | 4.1% | - | No rrSCNAs | 3.9% |
| Case 7 | T790M | No rrSCNAs | 3.6% | del19 | No rrSCNAs | 5.0% |
| Case 8 | L858R, T790M | CDK4, MDM2 | 7.6% | L858R, T790M | CDK4, MDM2, ERBB2, PIK3CA | 10.1% |
| Case 9 | T790M | No rrSCNAs | <3.0% | - | No rrSCNAs | 3.4% |
| Case 10 | del19, T790M | EGFR, CDK4, MDM2 | 19.4% | del19, T790M, C797S | CDK4, MDM2 | 3.4% |
| Case 11 | T790M | EGFR | 22.5% | del19 | EGFR | 6.7% |
| Case 12 | del19, T790M | No rrSCNAs | 5.6% | del19, T790M, C797S | EGFR, CDK4 | 5.9% |
| Case 13 | del19, T790M | No rrSCNAs | 5.3% | del19 | No rrSCNAs | 10.2% |
| Case 14 | del19, T790M | No rrSCNAs | 4.0% | del19, T790M, C797S | No rrSCNAs | 3.3% |
| Case 15 | T790M | No rrSCNAs | 3.1% | - | No rrSCNAs | 3.3% |
| Case 16 | L858R, T790M | ERBB2, CDKN2A | 42.4% | L858R, T790M | ERBB2 | 23.7% |
| Case 17 | L858R, T790M | No rrSCNAs | 4.8% | L858R | No rrSCNAs | 4.1% |
| Case 18 | del19, T790M | No rrSCNAs | 4.9% | - | No rrSCNAs | 4.8% |
| Case 19 | T790M | No rrSCNAs | 8.7% | - | No rrSCNAs | 9.9% |
| Case 20 | del19, T790M | No rrSCNAs | 4.9% | del19 | No rrSCNAs | 4.7% |
| Case 21 | del19, T790M | No rrSCNAs | 5.1% | del19 | No rrSCNAs | 4.9% |
| Case 22 | del19, T790M | No rrSCNAs | 3.7% | - | No rrSCNAs | 3.2% |
| Case 23 | del19, T790M | EGFR | 21.0% | del19, T790M, C797S | EGFR | 15.3% |
| Case 24 | T790M | No rrSCNAs | 3.3% | - | No rrSCNAs | 4.5% |
| Case 25 | del19, T790M | No rrSCNAs | <3.0% | del19, T790M | No rrSCNAs | 15.5% |
| Case 26 | del19, T790M | AKT2, RB1 | 23.8% | T790M | AKT2, RB1 | 42.6% |
| Case 27 | L858R, T790M | No rrSCNAs | 3.2% | L858R, T790M, C797S | No rrSCNAs | 3.7% |
| Case 28 | L858R, T790M | No rrSCNAs | 7.5% | L858R, T790M, C797S | No rrSCNAs | 4.4% |
| Case 29 | L858R, T790M | EGFR, CDK6 | 14.6% | L858R, T790M | No rrSCNAs | 5.3% |
| Case 30 | del19, T790M | EGFR | 6.9% | del19 | No rrSCNAs | 30.8% |
| Case 31 | L858R, T790M | No rrSCNAs | 3.0% | L858R | No rrSCNAs | 4.1% |
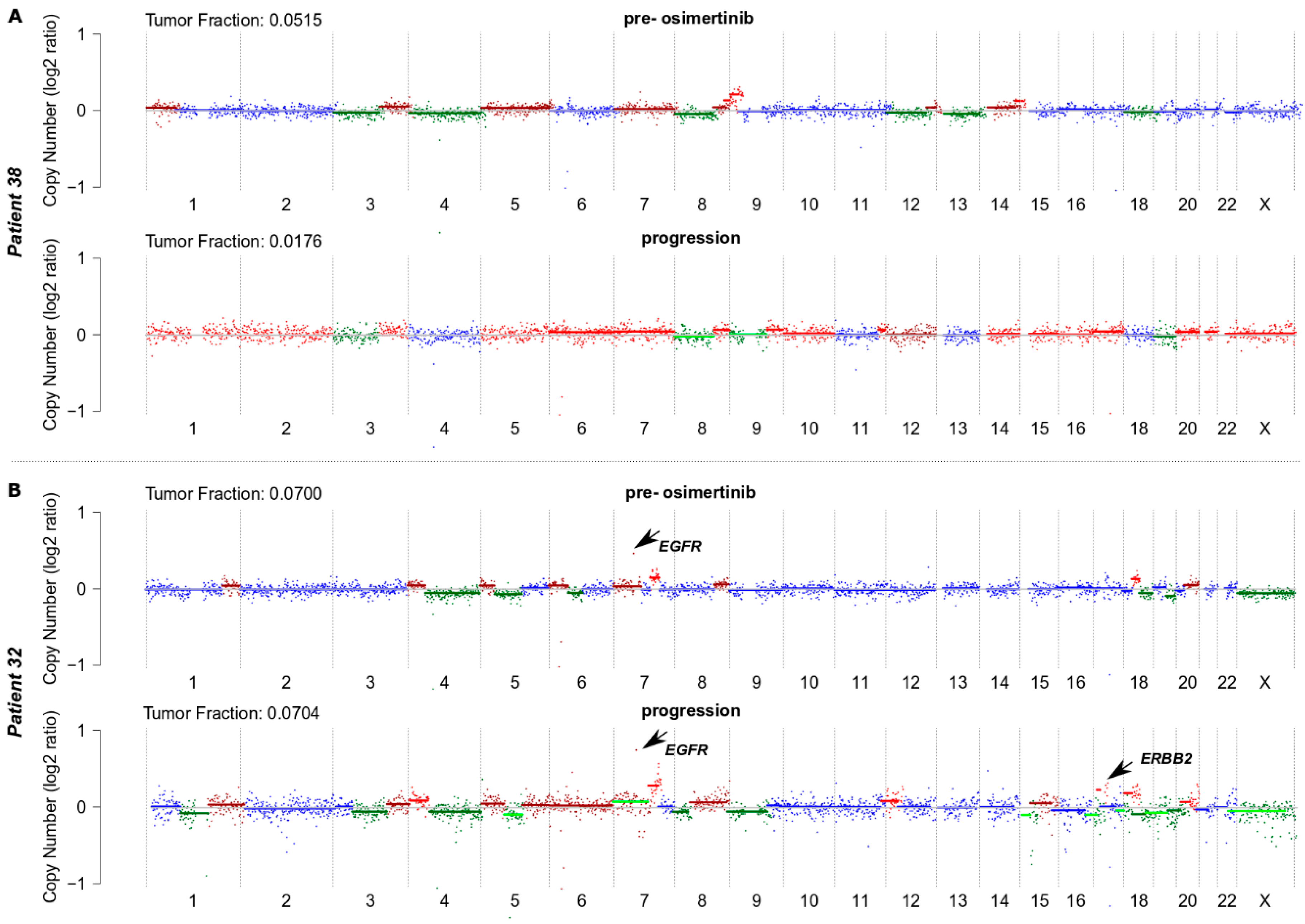
| Case 32 | L861Q, T790M | EGFR | 7.0% | L861Q | EGFR, ERBB2 | 7.0% |
| Case 33 | del19, T790M | No rrSCNAs | 6.2% | del19, T790M, C797S | No rrSCNAs | 4.3% |
| Case 34 | L858R, T790M | No rrSCNAs | 3.9% | - | No rrSCNAs | 4.0% |
| Case 35 | T790M | No rrSCNAs | 5.7% | - | No rrSCNAs | 4.2% |
| Case 36 | del19, T790M | No rrSCNAs | 5.9% | - | No rrSCNAs | 4.0% |
| Case 37 | del19, T790M | No rrSCNAs | 3.9% | del19 | No rrSCNAs | 7.8% |
| Case 38 | del19, T790M | No rrSCNAs | 5.1% | del19 | No rrSCNAs | <3.0% |
| Case 39 | L858R, T790M | No rrSCNAs | 3.8% | L858R | No rrSCNAs | <3.0% |
| Case 40 | L861Q, T790M | No rrSCNAs | 7.9% | L861Q | EGFR | 4.5% |
| Case 41 | del19, T790M | No rrSCNAs | 4.1% | del19, T790M | No rrSCNAs | 4.5% |
| Case 42 | del19, T790M | No rrSCNAs | <3.0% | - | CDKN2A | 8.3% |
| Case 43 | del19, T790M | No rrSCNAs | 5.1% | del19, T790M | No rrSCNAs | 5.0% |
| Patient | EGFR-Activating Mutation (copies/mL) | EGFR T790M (copies/mL) | Tumor Fraction (ichorCNA) | SCNAs ** |
|---|---|---|---|---|
| Case 1 | 6.7 | 6.9 | 4.5% | Yes |
| Case 2 * | 73.1 | 50.4 | 3.0% | No |
| Case 3 * | 0 | 5.2 | 4.5% | No |
| Case 4 | 179.2 | 86.0 | 7.2% | Yes |
| Case 5 | 0 | 2.9 | 5.0% | No |
| Case 6 * | 173.9 | 10.1 | 4.1% | No |
| Case 7 * | 0 | 6.4 | 3.6% | No |
| Case 8 | 166.3 | 38.1 | 7.6% | Yes |
| Case 9 * | 0 | 1.6 | <3.0% | No |
| Case 10 | 33,559.8 | 38,092.5 | 19.4% | Yes |
| Case 11 | 0 | 2.1 | 22.5% | Yes |
| Case 12 | 20.9 | 14.5 | 5.6% | No |
| Case 13 | 5.1 | 2.5 | 5.3% | Yes |
| Case 14 | 710.1 | 124.6 | 4.0% | Yes |
| Case 15 | 0 | 2.3 | 3.1% | Yes |
| Case 16 | 21,119.3 | 7.9 | 42.4% | Yes |
| Case 17 * | 7.6 | 52.0 | 4.8% | No |
| Case 18 | 2.7 | 2.3 | 4.9% | Yes |
| Case 19 | 0 | 7.9 | 8.7% | No |
| Case 20 * | 122.6 | 1.9 | 4.9% | No |
| Case 21 | 8.4 | 5.2 | 5.1% | No |
| Case 22 * | 763.6 | 10.2 | 3.7% | No |
| Case 23 | 5010.5 | 3354.0 | 21.0% | Yes |
| Case 24 * | 0 | 1.9 | 3.3% | No |
| Case 25 | 156.8 | 52.4 | <3.0% | Yes |
| Case 26 | 1571.9 | 254.5 | 23.8% | Yes |
| Case 27 * | 341.6 | 111.9 | 3.2% | No |
| Case 28 | 966.8 | 261.2 | 7.5% | No |
| Case 29 | 3891.9 | 444.3 | 14.6% | Yes |
| Case 30 | 4217.9 | 649.8 | 6.9% | Yes |
| Case 31 | 125.3 | 17.0 | 3.0% | Yes |
| Case 32 | 12660.3 | 1.8 | 7.0% | Yes |
| Case 33 | 201.6 | 39.2 | 6.2% | Yes |
| Case 34 * | 5.5 | 1.8 | 3.9% | No |
| Case 35 | 0 | 75.8 | 5.7% | No |
| Case 36 | 164.1 | 52.0 | 5.9% | No |
| Case 37 | 29.3 | 9.6 | 3.9% | Yes |
| Case 38 | 373.1 | 91.1 | 5.1% | No |
| Case 39 | 38.0 | 9.0 | 3.8% | Yes |
| Case 40 | 8373.2 | 6.0 | 7.9% | No |
| Case 41 | 231.1 | 93.8 | 4.1% | Yes |
| Case 42 * | 1.1 | 1.9 | <3.0% | No |
| Case 43 | 1540.7 | 379.8 | 5.1% | No |
| No rrSCNAs | rrSCNAs | p-Value | |
|---|---|---|---|
| Complete/Partial Response | 17 (81%) | 5 (50%) | 0.08 |
| Stable/Progressive Disease | 4 (19%) | 5 (50%) |
| Progression-Free Survival | Overall Survival | |||
|---|---|---|---|---|
| Univariate | Multivariate ** | Univariate | Multivariate ** | |
| HR * (95% CI); p Value | HR (95% CI); p Value | HR (95% CI); p Value | HR (95% CI); p Value | |
| Age | 0.99 (0.95–1.04); 0.74 | - | 0.99 (0.94–1.03); 0.58 | - |
| Gender | 1.58 (0.74–3.40); 0.24 | - | 1.51 (0.64–3.53); 0.35 | - |
| Metastases | 1.09 (0.44–2.71); 0.86 | - | 1.58 (0.54–4.65); 0.41 | - |
| EGFR tissue genotype | 2.19 (1.29–3.72); 0.004 | - | 2.49 (1.44–4.31); 0.001 | - |
| Previous EGFR-TKI therapy | 1.06 (0.77–1.45); 0.74 | - | 1.16 (0.81–1.65); 0.43 | - |
| Tumor fraction | 1.03 (0.99–1.07); 0.13 | - | 1.02 (0.98–1.06);0.38 | - |
| rrSCNAs | 3.33 (1.37–8.10); 0.008 | 3.33 (1.37–8.10); 0.008 | 2.54 (1.09–5.92); 0.03 | 2.54 (1.09–5.92); 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buder, A.; Heitzer, E.; Waldispühl-Geigl, J.; Weber, S.; Moser, T.; Hochmair, M.J.; Hackner, K.; Errhalt, P.; Setinek, U.; Filipits, M. Somatic Copy-Number Alterations in Plasma Circulating Tumor DNA from Advanced EGFR-Mutated Lung Adenocarcinoma Patients. Biomolecules 2021, 11, 618. https://doi.org/10.3390/biom11050618
Buder A, Heitzer E, Waldispühl-Geigl J, Weber S, Moser T, Hochmair MJ, Hackner K, Errhalt P, Setinek U, Filipits M. Somatic Copy-Number Alterations in Plasma Circulating Tumor DNA from Advanced EGFR-Mutated Lung Adenocarcinoma Patients. Biomolecules. 2021; 11(5):618. https://doi.org/10.3390/biom11050618
Chicago/Turabian StyleBuder, Anna, Ellen Heitzer, Julie Waldispühl-Geigl, Sabrina Weber, Tina Moser, Maximilian J. Hochmair, Klaus Hackner, Peter Errhalt, Ulrike Setinek, and Martin Filipits. 2021. "Somatic Copy-Number Alterations in Plasma Circulating Tumor DNA from Advanced EGFR-Mutated Lung Adenocarcinoma Patients" Biomolecules 11, no. 5: 618. https://doi.org/10.3390/biom11050618