

Cholesterol Content of Very-Low-Density Lipoproteins Is Associated with 1-Year Mortality in Acute Heart Failure Patients


 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Laboratory Procedures
2.3. Lipoprotein Profiling by Nuclear Magnetic Resonance (NMR) Spectroscopy
2.4. Statistics
3. Results
3.1. Clinical Characteristics, Medication, and Laboratory Parameters
3.2. Serum Levels and Lipid Content of VLDL Parameters
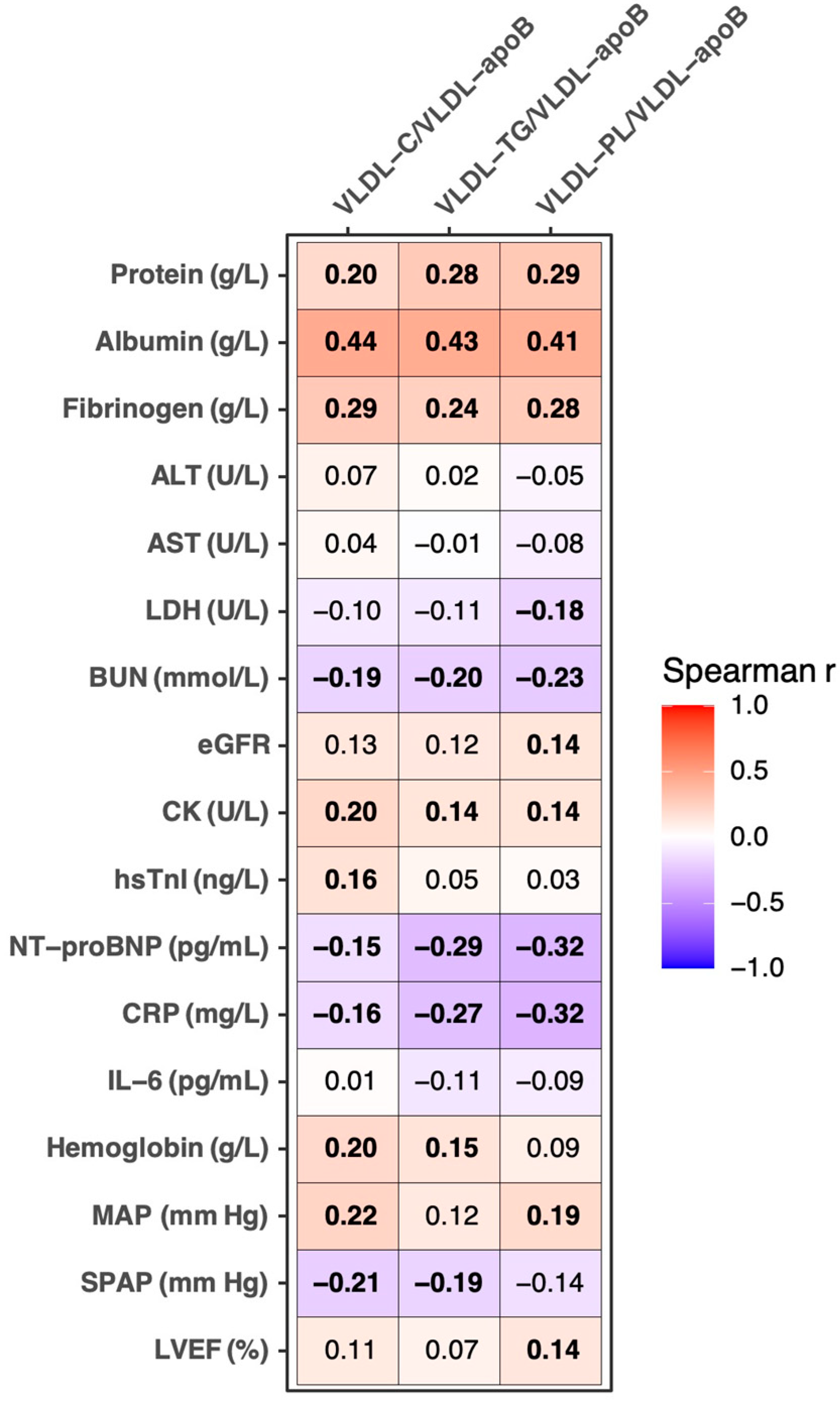
3.3. Correlation Analyses of VLDL-C/VLDL-apoB, VLDL-TG/VLDL-apoB, and VLDL-PL/VLDL-apoB Ratios with Clinical and Laboratory Parameters
3.4. VLDL-C/VLDL-apoB, VLDL-TG/VLDL-apoB, and VLDL-PL/VLDL-apoB Ratios in Various Groups of AHF Patients
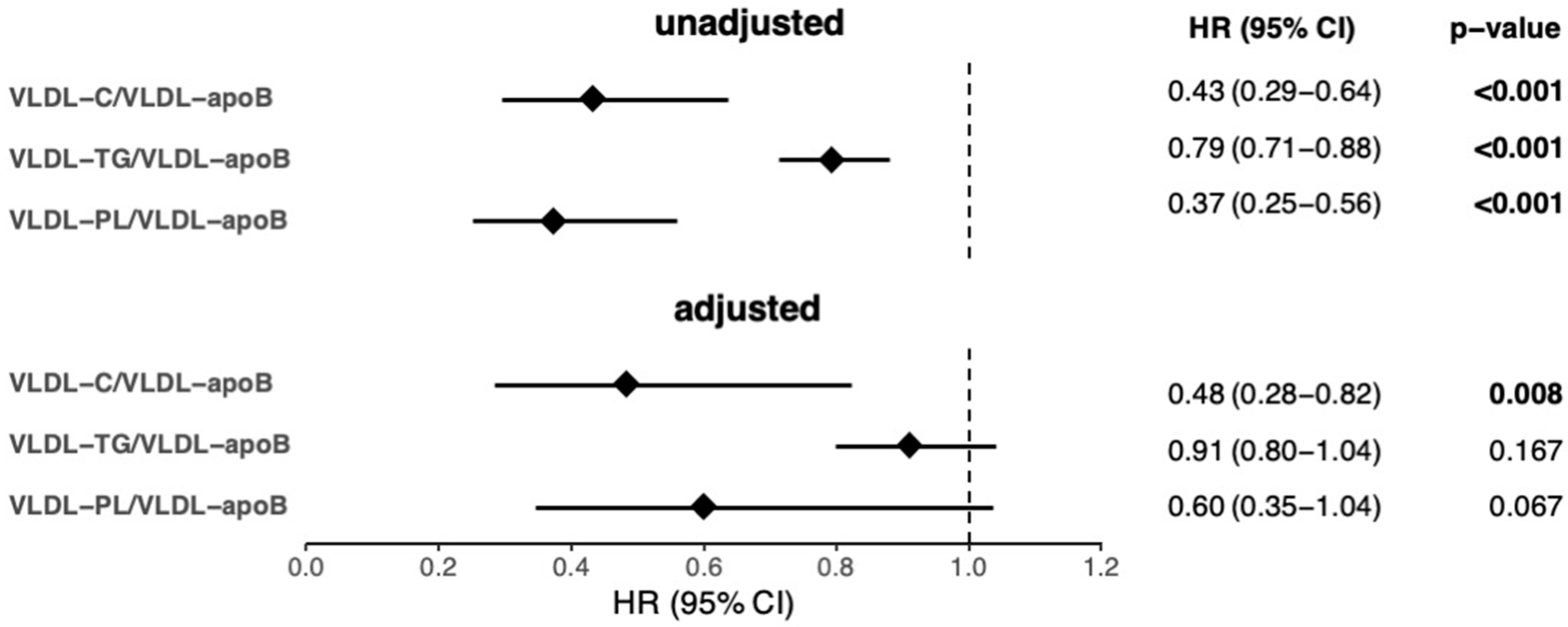
3.5. Association of the Estimators of VLDL Lipid Content with Mortality in AHF Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roger, V.L.; Weston, S.A.; Redfield, M.M.; Hellermann-Homan, J.P.; Killian, J.; Yawn, B.P.; Jacobsen, S.J. Trends in heart failure incidence and survival in a community-based population. Jama 2004, 292, 344–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; Gonzalez-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Rev. Esp. Cardiol. Engl. Ed. 2016, 69, 1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wende, A.R.; Brahma, M.K.; McGinnis, G.R.; Young, M.E. Metabolic Origins of Heart Failure. JACC Basic Transl. Sci. 2017, 2, 297–310. [Google Scholar] [CrossRef] [PubMed]
- Mentz, R.J.; O’Connor, C.M. Pathophysiology and clinical evaluation of acute heart failure. Nat. Rev. Cardiol. 2016, 13, 28–35. [Google Scholar] [CrossRef]
- Hunter, W.G.; Kelly, J.P.; McGarrah, R.W., 3rd; Kraus, W.E.; Shah, S.H. Metabolic Dysfunction in Heart Failure: Diagnostic, Prognostic, and Pathophysiologic Insights From Metabolomic Profiling. Curr. Heart Fail. Rep. 2016, 13, 119–131. [Google Scholar] [CrossRef] [Green Version]
- Gnanaraj, F.J.; von Haehling, S.; Anker, S.D.; Raj, D.S.; Radhakrishnan, J. The relevance of congestion in the cardio-renal syndrome. Kidney Int. 2013, 83, 384–391. [Google Scholar] [CrossRef] [Green Version]
- Mullens, W.; Abrahams, Z.; Francis, G.S.; Sokos, G.; Taylor, D.O.; Starling, R.C.; Young, J.B.; Tang, W.H. Importance of venous congestion for worsening of renal function in advanced decompensated heart failure. J. Am. Coll. Cardiol. 2009, 53, 589–596. [Google Scholar] [CrossRef] [Green Version]
- Boren, J.; Chapman, M.J.; Krauss, R.M.; Packard, C.J.; Bentzon, J.F.; Binder, C.J.; Daemen, M.J.; Demer, L.L.; Hegele, R.A.; Nicholls, S.J.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: Pathophysiological, genetic, and therapeutic insights: A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2020, 41, 2313–2330. [Google Scholar] [CrossRef] [Green Version]
- Packard, C.J.; Shepherd, J. Lipoprotein heterogeneity and apolipoprotein B metabolism. Arterioscler Thromb. Vasc. Biol. 1997, 17, 3542–3556. [Google Scholar] [CrossRef]
- Shelness, G.S.; Sellers, J.A. Very-low-density lipoprotein assembly and secretion. Curr. Opin. Lipidol. 2001, 12, 151–157. [Google Scholar] [CrossRef]
- Packard, C.J.; Demant, T.; Stewart, J.P.; Bedford, D.; Caslake, M.J.; Schwertfeger, G.; Bedynek, A.; Shepherd, J.; Seidel, D. Apolipoprotein B metabolism and the distribution of VLDL and LDL subfractions. J. Lipid. Res. 2000, 41, 305–318. [Google Scholar] [CrossRef]
- Prinsen, B.H.; Romijn, J.A.; Bisschop, P.H.; de Barse, M.M.; Barrett, P.H.; Ackermans, M.; Berger, R.; Rabelink, T.J.; de Sain-van der Velden, M.G. Endogenous cholesterol synthesis is associated with VLDL-2 apoB-100 production in healthy humans. J. Lipid. Res. 2003, 44, 1341–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barrows, B.R.; Parks, E.J. Contributions of different fatty acid sources to very low-density lipoprotein-triacylglycerol in the fasted and fed states. J. Clin. Endocrinol. Metab. 2006, 91, 1446–1452. [Google Scholar] [CrossRef] [Green Version]
- Packer, M. Pathophysiology of chronic heart failure. Lancet 1992, 340, 88–92. [Google Scholar] [CrossRef]
- Adam, R.C.; Mintah, I.J.; Alexa-Braun, C.A.; Shihanian, L.M.; Lee, J.S.; Banerjee, P.; Hamon, S.C.; Kim, H.I.; Cohen, J.C.; Hobbs, H.H.; et al. Angiopoietin-like protein 3 governs LDL-cholesterol levels through endothelial lipase-dependent VLDL clearance. J. Lipid. Res. 2020, 61, 1271–1286. [Google Scholar] [CrossRef] [PubMed]
- Packard, C.J.; Gaw, A.; Demant, T.; Shepherd, J. Development and application of a multicompartmental model to study very low density lipoprotein subfraction metabolism. J. Lipid. Res. 1995, 36, 172–187. [Google Scholar] [CrossRef]
- Loungani, R.S.; Teerlink, J.R.; Metra, M.; Allen, L.A.; Butler, J.; Carson, P.E.; Chen, C.W.; Cotter, G.; Davison, B.A.; Eapen, Z.J.; et al. Cause of Death in Patients With Acute Heart Failure: Insights From RELAX-AHF-2. JACC. Heart Fail. 2020, 8, 999–1008. [Google Scholar] [CrossRef]
- Ambrosy, A.P.; Fonarow, G.C.; Butler, J.; Chioncel, O.; Greene, S.J.; Vaduganathan, M.; Nodari, S.; Lam, C.S.P.; Sato, N.; Shah, A.N.; et al. The global health and economic burden of hospitalizations for heart failure: Lessons learned from hospitalized heart failure registries. J. Am. Coll. Cardiol. 2014, 63, 1123–1133. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; Januzzi, J.L., Jr. Established and Emerging Roles of Biomarkers in Heart Failure. Circ. Res. 2018, 123, 614–629. [Google Scholar] [CrossRef]
- Charach, G.; George, J.; Roth, A.; Rogowski, O.; Wexler, D.; Sheps, D.; Grosskopf, I.; Weintraub, M.; Keren, G.; Rubinstein, A. Baseline low-density lipoprotein cholesterol levels and outcome in patients with heart failure. Am. J. Cardiol. 2010, 105, 100–104. [Google Scholar] [CrossRef]
- Kahn, M.R.; Kosmas, C.E.; Wagman, G.; Serrao, G.W.; Fallahi, A.; Grady, K.M.; Vittorio, T.J. Low-density lipoprotein levels in patients with acute heart failure. Congest. Heart Fail. 2013, 19, 85–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charach, G.; Rabinovich, A.; Ori, A.; Weksler, D.; Sheps, D.; Charach, L.; Weintraub, M.; George, J. Low levels of low-density lipoprotein cholesterol: A negative predictor of survival in elderly patients with advanced heart failure. Cardiology 2014, 127, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Klobucar, I.; Degoricija, V.; Potocnjak, I.; Trbusic, M.; Pregartner, G.; Berghold, A.; Fritz-Petrin, E.; Habisch, H.; Madl, T.; Frank, S. HDL-apoA-II Is Strongly Associated with 1-Year Mortality in Acute Heart Failure Patients. Biomedicines 2022, 10, 1668. [Google Scholar] [CrossRef] [PubMed]
- World Medical, A. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Jama 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [Green Version]
- Schilcher, I.; Stadler, J.T.; Lechleitner, M.; Hrzenjak, A.; Berghold, A.; Pregartner, G.; Lhomme, M.; Holzer, M.; Korbelius, M.; Reichmann, F.; et al. Endothelial Lipase Modulates Paraoxonase 1 Content and Arylesterase Activity of HDL. Int. J. Mol. Sci. 2021, 22, 719. [Google Scholar] [CrossRef]
- Potocnjak, I.; Degoricija, V.; Trbusic, M.; Pregartner, G.; Berghold, A.; Marsche, G.; Frank, S. Serum Concentration of HDL Particles Predicts Mortality in Acute Heart Failure Patients. Sci. Rep. 2017, 7, 46642. [Google Scholar] [CrossRef] [Green Version]
- Hunter, W.G.; McGarrah, R.W., 3rd; Kelly, J.P.; Khouri, M.G.; Craig, D.M.; Haynes, C.; Felker, G.M.; Hernandez, A.F.; Velazquez, E.J.; Kraus, W.E.; et al. High-Density Lipoprotein Particle Subfractions in Heart Failure With Preserved or Reduced Ejection Fraction. J. Am. Coll. Cardiol. 2019, 73, 177–186. [Google Scholar] [CrossRef]
- Barter, P.J.; Rye, K.A. Cholesteryl ester transfer protein, high density lipoprotein and arterial disease. Curr. Opin. Lipidol. 2001, 12, 377–382. [Google Scholar] [CrossRef]
- Martinelli, A.E.M.; Maranhao, R.C.; Carvalho, P.O.; Freitas, F.R.; Silva, B.M.O.; Curiati, M.N.C.; Kalil Filho, R.; Pereira-Barretto, A.C. Cholesteryl ester transfer protein (CETP), HDL capacity of receiving cholesterol and status of inflammatory cytokines in patients with severe heart failure. Lipids Health Dis. 2018, 17, 242. [Google Scholar] [CrossRef] [Green Version]
- Flahault, A.; Metzger, M.; Chasse, J.F.; Haymann, J.P.; Boffa, J.J.; Flamant, M.; Vrtovsnik, F.; Houillier, P.; Stengel, B.; Thervet, E.; et al. Low Serum Creatine Kinase Level Predicts Mortality in Patients with a Chronic Kidney Disease. PLoS ONE 2016, 11, e0156433. [Google Scholar] [CrossRef]
- Yasuda, T.; Ishida, T.; Rader, D.J. Update on the role of endothelial lipase in high-density lipoprotein metabolism, reverse cholesterol transport, and atherosclerosis. Circ. J. 2010, 74, 2263–2270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sylvers-Davie, K.L.; Davies, B.S.J. Regulation of lipoprotein metabolism by ANGPTL3, ANGPTL4, and ANGPTL8. Am. J. Physiol. Endocrinol. Metab. 2021, 321, E493–E508. [Google Scholar] [CrossRef] [PubMed]
- Degoricija, V.; Trbusic, M.; Potocnjak, I.; Radulovic, B.; Teresak, S.D.; Pregartner, G.; Berghold, A.; Tiran, B.; Frank, S. Acute Heart Failure developed as worsening of Chronic Heart Failure is associated with increased mortality compared to de novo cases. Sci. Rep. 2018, 8, 9587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harada, M.; Van Wagoner, D.R.; Nattel, S. Role of inflammation in atrial fibrillation pathophysiology and management. Circ. J. 2015, 79, 495–502. [Google Scholar] [CrossRef] [Green Version]
- Balling, M.; Afzal, S.; Varbo, A.; Langsted, A.; Davey Smith, G.; Nordestgaard, B.G. VLDL Cholesterol Accounts for One-Half of the Risk of Myocardial Infarction Associated With apoB-Containing Lipoproteins. J. Am. Coll. Cardiol. 2020, 76, 2725–2735. [Google Scholar] [CrossRef]
- Horwich, T.B.; Fonarow, G.C. Reverse epidemiology beyond dialysis patients: Chronic heart failure, geriatrics, rheumatoid arthritis, COPD, and AIDS. Semin. Dial. 2007, 20, 549–553. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Alive (n = 197) | Deceased (n = 118) | All (n = 315) | p-Value | |
|---|---|---|---|---|
| Demographics | ||||
| Age (years) | 72.5 (10.4) | 77.0 (10.1) | 74.2 (10.5) | <0.001 |
| Sex, Female | 85 (43.1%) | 51 (43.2%) | 136 (43.2%) | 1.000 |
| Comorbidities | ||||
| Hypertension | 186 (94.4%) | 108 (91.5%) | 294 (93.3%) | 0.355 |
| T2DM | 76 (38.6%) | 56 (47.5%) | 132 (41.9%) | 0.127 |
| CAD | 100 (50.8%) | 56 (47.5%) | 156 (49.5%) | 0.642 |
| CMP | 173 (87.8%) | 115 (97.5%) | 288 (91.4%) | 0.003 |
| AF | 98 (49.7%) | 72 (61.0%) | 170 (54.0%) | 0.062 |
| CKD | 72 (36.5%) | 71 (60.2%) | 143 (45.4%) | <0.001 |
| MetS | 130 (66.0%) | 87 (73.7%) | 217 (68.9%) | 0.168 |
| Physical measures at admission | ||||
| MAP (mmHg) | 108.1 (24.2) | 96.0 (19.5) | 103.6 (23.3) | <0.001 |
| Heart rate (beats/min) | 103.8 (25.8) | 95.3 (27.5) | 100.6 (26.7) | 0.006 |
| Respiratory rate (breaths/min) | 29.3 (6.9) | 28.8 (6.0) | 29.1 (6.5) | 0.474 |
| BMI (kg/m2) | 27.4 (24.9, 30.7) | 29.1 (25.3, 32.8) | 28.0 (25.0, 31.6) | 0.067 |
| Signs and symptoms | ||||
| Symptom duration (days) | 5.0 (3.0, 5.0) | 5.0 (4.0, 5.0) | 5.0 (4.0, 5.0) | 0.022 |
| Rales or crackles | 193 (98.0%) | 118 (100.0%) | 311 (98.7%) | 0.301 |
| JVD | 97 (49.2%) | 77 (65.3%) | 174 (55.2%) | 0.007 |
| Enlarged liver | 95 (48.2%) | 81 (68.6%) | 176 (55.9%) | <0.001 |
| Ascites | 20 (10.2%) | 29 (24.6%) | 49 (15.6%) | 0.001 |
| Peripheral edema | 114 (57.9%) | 90 (76.3%) | 204 (64.8%) | <0.001 |
| NYHA class | 0.305 | |||
| 3 | 13 (6.6%) | 4 (3.4%) | 17 (5.4%) | |
| 4 | 184 (93.4%) | 114 (96.6%) | 298 (94.6%) | |
| AHF type | 0.003 | |||
| New onset AHF | 24 (12.2%) | 3 (2.5)% | 27 (8.6%) | |
| AHF following CHF | 173 (87.8%) | 115 (97.5%) | 288 (91.4%) | |
| Echocardiography | ||||
| LVEDd/BSA (mm/m2) | 29.1 (4.9) | 28.5 (5.2) | 28.8 (5.0) | 0.346 |
| LVEF (%) | 40.1 (11.9) | 39.1 (12.6) | 39.8 (12.1) | 0.455 |
| SPAP (mmHg) | 47.0 (42.0, 55.0) | 50.0 (45.0, 60.0) | 50.0 (45.0, 60.0) | 0.005 |
| AHF class | 0.575 | |||
| HFrEF, EF <40% | 88 (44.9%) | 55 (51.4%) | 143 (47.2%) | |
| HFmrEF, EF 41–49% | 55 (28.1%) | 26 (24.3%) | 81 (26.7%) | |
| HFpEF, EF ≥50% | 53 (27.3%) | 26 (24.3%) | 79 (26.1%) | |
| Laboratory test results at admission | ||||
| TC (mg/dL) | 145.0 (118.0, 188.0) | 128.5 (103.2, 156.8) | 134.0 (110.0, 173.0) | <0.001 |
| HDL-C (mg/dL) | 43.0 (35.0, 52.0) | 41.0 (31.0, 50.0) | 42.0 (34.0, 51.0) | 0.022 |
| LDL-C (mg/dL) | 78.0 (57.8, 109.2) | 66.5 (49.2, 91.5) | 73.0 (54.0, 102.0) | <0.001 |
| Triglycerides (mg/dL) | 90.0 (69.0, 121.0) | 84.0 (68.0, 103.8) | 88.0 (69.0, 113.5) | 0.099 |
| ApoB (mg/dL) | 77.8 (65.6, 97.8) | 75.7 (62.7, 89.9) | 77.6 (63.8, 95.0) | 0.045 |
| Albumin (g/L) | 38.2 (35.5, 42.0) | 36.7 (33.8, 39.7) | 37.8 (34.8, 41.3) | 0.009 |
| Total proteins (g/L) | 67.0 (62.0, 72.0) | 65.5 (61.0, 70.0) | 67.0 (61.0, 72.0) | 0.214 |
| Bilirubin (µmol/L) | 17.4 (11.0, 28.5) | 17.2 (11.9, 29.2) | 17.3 (11.1, 28.7) | 0.336 |
| AST (U/L) | 28.0 (22.0, 42.0) | 27.0 (18.2, 52.5) | 28.0 (20.0, 44.5) | 0.542 |
| ALT (U/L) | 25.0 (16.0, 41.0) | 21.0 (14.0, 46.5) | 25.0 (15.0, 42.0) | 0.226 |
| Glucose (mmol/L) | 7.7 (6.0, 10.8) | 8.1 (6.3, 11.6) | 7.9 (6.1, 11.2) | 0.267 |
| Sodium (mmol/L) | 140.0 (138.0, 142.0) | 138.0 (135.0, 141.0) | 140.0 (136.5, 142.0) | <0.001 |
| Potassium (mmol/L) | 4.5 (4.1, 4.8) | 4.5 (4.1, 5.0) | 4.5 (4.1, 4.8) | 0.194 |
| Chloride (mmol/L) | 104.0 (101.0, 107.0) | 100.0 (97.0, 104.0) | 103.0 (99.0, 106.0) | <0.001 |
| BUN (mmol/L) | 8.3 (6.3, 12.3) | 12.3 (8.9, 16.8) | 9.6 (6.9, 14.4) | <0.001 |
| Creatinine (µmol/L) | 107.0 (86.0, 144.0) | 131.5 (107.0, 164.0) | 117.0 (90.5, 152.5) | <0.001 |
| eGFR (ml/min/1.73 m2) | 54.0 (36.1, 70.5) | 38.4 (29.1, 52.1) | 46.6 (32.3, 65.0) | <0.001 |
| CK (U/L) | 105.0 (65.0, 174.0) | 78.0 (50.2, 147.5) | 93.0 (58.0, 165.5) | 0.007 |
| LDH (U/L) | 252.0 (217.0, 316.0) | 283.0 (230.8, 372.2) | 265.0 (218.5, 332.0) | 0.029 |
| hsTnI (ng/L) | 39.0 (17.5, 136.5) | 61.0 (30.0, 149.0) | 46.0 (20.0, 143.2) | 0.039 |
| NT-proBNP (pg/mL) | 5350.0 (3151.0, 10,691.0) | 10733.0 (5486.5, 18,385.5) | 6692.0 (3531.0, 14,395.5) | <0.001 |
| CRP (mg/L) | 10.3 (4.9, 21.9) | 24.9 (6.4, 47.3) | 12.2 (5.5, 33.1) | <0.001 |
| IL-6 (pg/mL) | 22.1 (11.3, 44.8) | 40.6 (17.1, 79.6) | 25.1 (12.9, 60.1) | <0.001 |
| Fibrinogen (g/L) | 4.0 (3.4, 4.7) | 4.0 (3.1, 4.9) | 4.0 (3.4, 4.8) | 0.469 |
| Erythrocytes (× 1012/L) | 4.7 (4.4, 5.1) | 4.4 (3.8, 4.9) | 4.6 (4.2, 5.1) | <0.001 |
| Hemoglobin (g/L) | 138.0 (124.0, 150.0) | 126.0 (111.0, 141.0) | 134.0 (119.0, 148.0) | <0.001 |
| pH | 7.4 (7.3, 7.5) | 7.4 (7.3, 7.4) | 7.4 (7.3, 7.5) | 0.709 |
| pO2 (kPa) | 8.8 (7.2, 10.4) | 8.8 (7.3, 10.4) | 8.8 (7.2, 10.4) | 0.803 |
| pCO2 (kPa) | 5.2 (4.4, 6.3) | 5.2 (4.5, 7.1) | 5.2 (4.5, 6.4) | 0.386 |
| HCO3 (mmol/L) | 23.9 (21.2, 27.0) | 24.4 (21.3, 28.9) | 23.9 (21.3, 27.4) | 0.368 |
| Alive (n = 197) | Deceased (n = 117) | All (n = 314) | p-Value | |
|---|---|---|---|---|
| VLDL-C (mg/dL) | 12.7 (8.4, 20.2) | 10.6 (7.7, 15.8) | 11.8 (7.9, 19.1) | 0.036 |
| VLDL-TG (mg/dL) | 39.7 (27.0, 65.7) | 34.7 (25.8, 49.6) | 37.3 (26.5, 58.4) | 0.021 |
| VLDL-PL (mg/dL) | 11.6 (8.1, 18.3) | 9.7 (7.1, 14.2) | 10.8 (7.5, 17.0) | 0.018 |
| VLDL-apoB (mg/dL) | 7.1 (5.0, 9.7) | 6.5 (5.1, 8.8) | 6.9 (5.0, 9.5) | 0.402 |
| VLDL-C/VLDL-apoB | 1.9 (1.6, 2.2) | 1.7 (1.5, 1.9) | 1.8 (1.5, 2.1) | <0.001 |
| VLDL-TG/VLDL-apoB | 6.4 (5.1, 7.9) | 5.4 (4.7, 6.3) | 5.9 (5.0, 7.3) | <0.001 |
| VLDL-PL/VLDL-apoB | 1.8 (1.5, 2.2) | 1.6 (1.3, 1.8) | 1.7 (1.4, 2.1) | <0.001 |
| VLDL-C/VLDL-apoB | VLDL-TG/VLDL-apoB | VLDL-PL/VLDL-apoB | ||
|---|---|---|---|---|
| T2D | no (n = 182) | 1.71 (1.51, 2.08) | 5.82 (4.83, 7.19) | 1.66 (1.39, 2.03) |
| yes (n = 132) | 1.88 (1.56, 2.21) | 6.10 (5.13, 7.35) | 1.80 (1.49, 2.08) | |
| p= 0.012 | p = 0.349 | p = 0.181 | ||
| CAD | no (n = 158) | 1.74 (1.51, 2.08) | 5.62 (4.57, 6.89) | 1.64 (1.41, 1.98) |
| yes (n = 156) | 1.82 (1.56, 2.20) | 6.34 (5.13, 7.73) | 1.82 (1.47, 2.16) | |
| p = 0.086 | p= 0.002 | p = 0.025 | ||
| AF | no (n = 144) | 1.89 (1.60, 2.26) | 6.53 (5.24, 8.12) | 1.86 (1.54, 2.19) |
| yes (n = 170) | 1.71 (1.49, 1.98) | 5.59 (4.73, 6.61) | 1.59 (1.37, 1.95) | |
| p< 0.001 | p< 0.001 | p< 0.001 | ||
| Statins | no (n = 196) | 1.78 (1.58, 2.15) | 5.76 (4.60, 7.15) | 1.67 (1.40, 2.02) |
| yes (n = 118) | 1.73 (1.48, 2.12) | 6.31 (5.17, 7.42) | 1.80 (1.49, 2.13) | |
| p = 0.296 | p= 0.012 | p = 0.095 | ||
| Venous overload * | no (n = 66) | 2.13 (1.82, 2.39) | 7.41 (5.97, 8.75) | 2.05 (1.73, 2.25) |
| yes (n = 248) | 1.72 (1.50, 2.03) | 5.70 (4.77, 7.03) | 1.64 (1.39, 1.97) | |
| p< 0.001 | p< 0.001 | p< 0.001 | ||
| AHF type | New onset AHF (n = 27) | 2.33 (2.08, 2.46) | 8.04 (6.65, 9.51) | 2.25 (1.96, 2.44) |
| AHF following CHF (n = 287) | 1.73 (1.51, 2.09) | 5.79 (4.86, 7.14) | 1.66 (1.41, 2.00) | |
| p< 0.001 | p< 0.001 | p< 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Degoricija, V.; Klobučar, I.; Potočnjak, I.; Dokoza Terešak, S.; Vidović, L.; Pregartner, G.; Berghold, A.; Habisch, H.; Madl, T.; Frank, S. Cholesterol Content of Very-Low-Density Lipoproteins Is Associated with 1-Year Mortality in Acute Heart Failure Patients. Biomolecules 2022, 12, 1542. https://doi.org/10.3390/biom12101542
Degoricija V, Klobučar I, Potočnjak I, Dokoza Terešak S, Vidović L, Pregartner G, Berghold A, Habisch H, Madl T, Frank S. Cholesterol Content of Very-Low-Density Lipoproteins Is Associated with 1-Year Mortality in Acute Heart Failure Patients. Biomolecules. 2022; 12(10):1542. https://doi.org/10.3390/biom12101542
Chicago/Turabian StyleDegoricija, Vesna, Iva Klobučar, Ines Potočnjak, Sanda Dokoza Terešak, Luka Vidović, Gudrun Pregartner, Andrea Berghold, Hansjörg Habisch, Tobias Madl, and Saša Frank. 2022. "Cholesterol Content of Very-Low-Density Lipoproteins Is Associated with 1-Year Mortality in Acute Heart Failure Patients" Biomolecules 12, no. 10: 1542. https://doi.org/10.3390/biom12101542
APA StyleDegoricija, V., Klobučar, I., Potočnjak, I., Dokoza Terešak, S., Vidović, L., Pregartner, G., Berghold, A., Habisch, H., Madl, T., & Frank, S. (2022). Cholesterol Content of Very-Low-Density Lipoproteins Is Associated with 1-Year Mortality in Acute Heart Failure Patients. Biomolecules, 12(10), 1542. https://doi.org/10.3390/biom12101542