
Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations



Abstract
:1. Introduction
2. Melatonin: The Basics
2.1. Synthesis and Secretion of Melatonin
2.2. Childhood and Melatonin
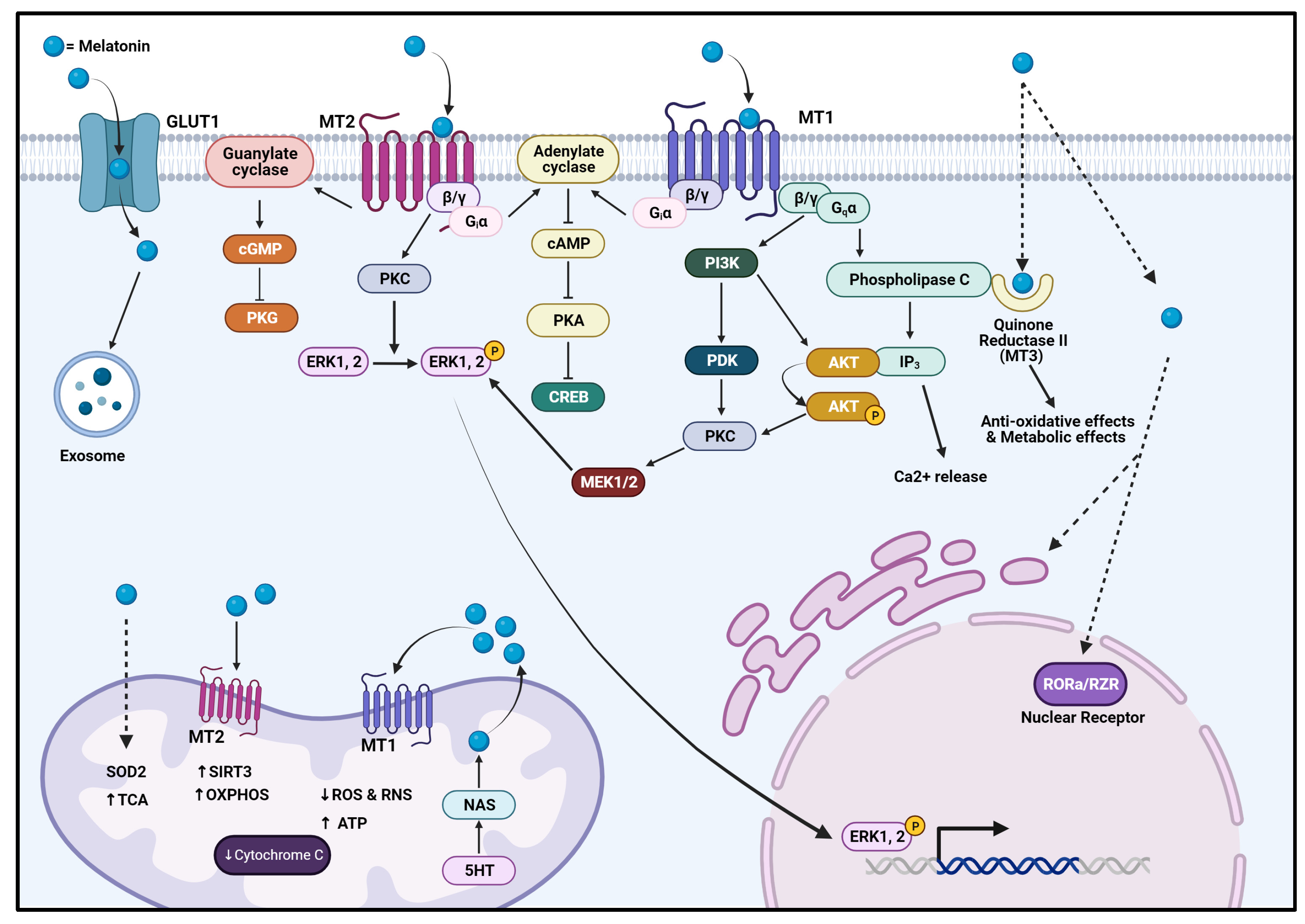
2.3. Mechanism of Action and Physiology
2.4. Melatonin in Bone Metabolism and Remodeling
3. Osteosarcoma: Where Are We Now?
3.1. Osteosarcoma: The Facts
3.2. Cancer Cell Populations
3.3. Genomic Nature
3.4. Signaling Pathways


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Signaling Pathway Involved | Expression in OS | Function | References |
|---|---|---|---|
| SOX-9 via JNK Pathway | ↑ | ↑ Tumor progression | [43,90,91] |
| Wnt Pathway | ↑ (↑ in CSC) | ↑ Cell proliferation ↑ Cancer cell survival ↑ Tumor metastasis ↑ EMT ↑ Chemoresistance | [43,70] |
| NOTCH Pathway | ↑ | ↑ Tumor metastasis ↑ Drug resistance ↑ EMT ↑ Cancer relapse | [43,66] |
| Hedgehog Pathway | ↑ | ↑ Tumor metastasis | [82] |
| SDF1-CXCR4 Pathway | ↑ | ↑ MMP9 expression leading to invasion | [43] |
| PI3K/Akt/mTOR Pathway | ↑ | OS progression ↑ Angiogenesis ↑ Proliferation ↑ Invasion ↑ EMT ↑ Metastasis | [41,43,83,85] |
| JAK2/Stat3 Pathway | ↑ | ↑ Tumor cell survival ↑ EMT ↑ Metastasis | [43,81] |
| RANK Pathway | ↑ | ↑ Cancer cell migration ↑ Lung metastasis ↑ Pathological bone destruction | [43,51,81,92] |
| Hippo Pathway | ↑ | ↑ Chemoresistance | [43,92] |
| ERK/MAPK Pathway | ↑ | ↑ Angiogenesis ↑ Proliferation ↑ Inflammatory microenvironment | [43,69] |
| NF-κB Pathway | ↑ | Cancer proliferation Immune response | [52,93] |
| Fas/Fas ligand Pathway | ↓ | Caspase cascade Apoptosis regulation | [94] |
3.5. Cancer Cell Survival: Cytokines, Growth, and Transcription Factors
3.6. Microenvironment, Angiogenesis, and Tumor Metabolism
3.7. Cancer Resistance
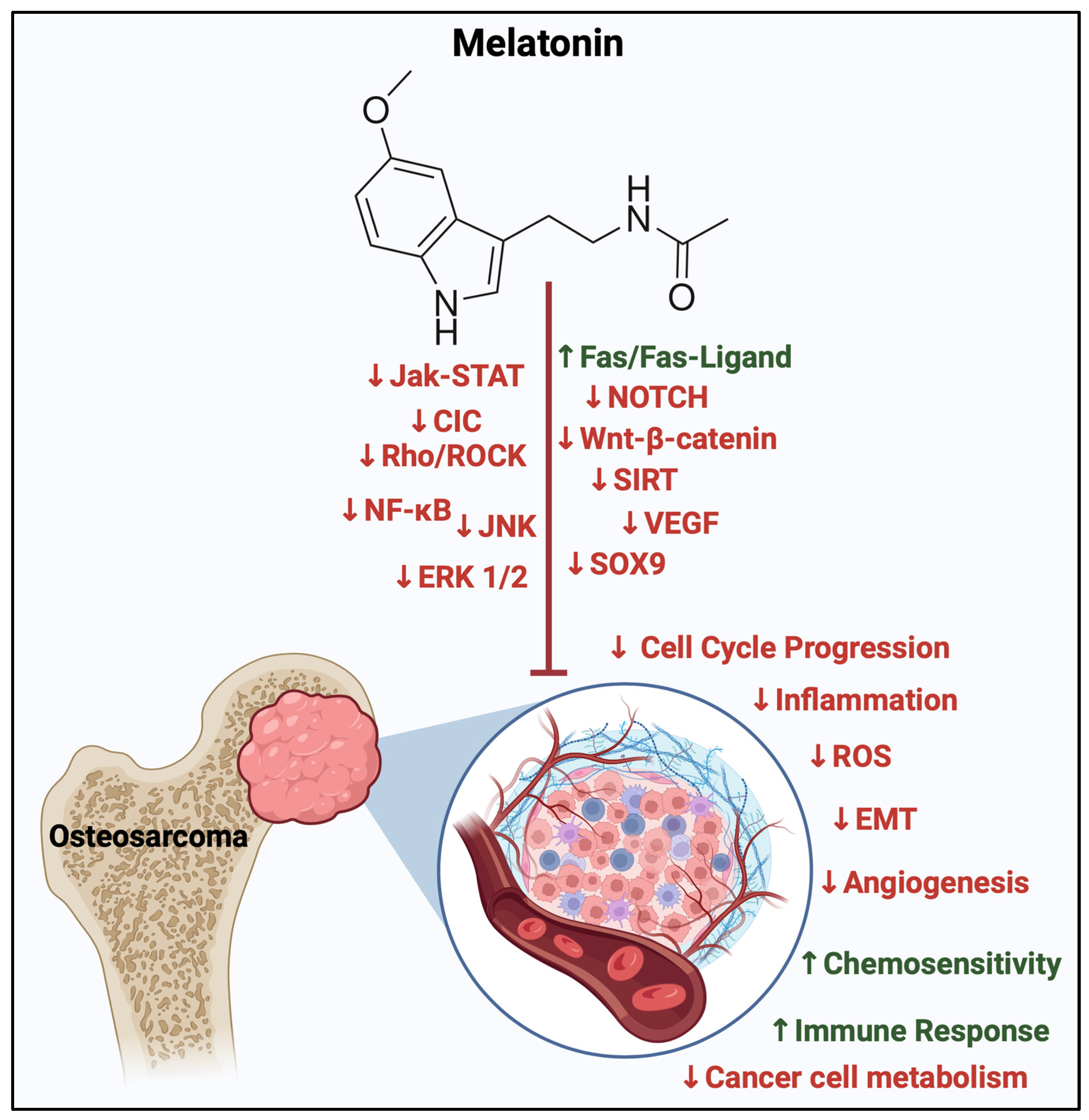
4. Melatonin in OS
4.1. Melatonin in Malignancy
4.2. Melatonin, the Cell Cycle, and Cell Signaling
| Signaling Cascade | Study Model | Type of Model | Melatonin Concentration | Effects | References |
|---|---|---|---|---|---|
| Cell Cycle Modulation | Cell Study | MG-63 cells | 4–10 mM | ↑ Cells in G0/G1 phase ↓ G1 phase progression via (↓ cyclin D1 and CDK4) ↓ G2/M phases progression via (↓ cyclin B1 and CDK1) | [137] |
| Cell Cycle Modulation | Cell Study | MG-63 cells | 0–0.1 M | ↓ G0/G1 cell cycle phase at 9 mM | [138] |
| SOX9 suppression EMT Pathway | Cell Study | HOS, MG-63, and U2 | 1 mM | ↓ Migration ↓ Invasion ↓ Sarcosphere formation OS-CSC ↓ EMT markers | [133] |
| Animal Study | Mice | 100 mg/kg | ↓ Initiation and metastasis | ||
| JNK/ERK Pathway | Cell Study | U2OS, HOS | 0.25, 0.5, 1.0, 2.0 mmol/L | No effect of melatonin after 24 h exposure ↓ Cell motility after 48 h ↑ Phosphorylation of ERK1/2 ↓ Phosphorylation of JNK1/2 in U2OS and HOS cells | [132] |
| JPX-Wnt/β-catenin | Cell Study | Saos-2, MG63, and U2OS | 0.1, 0.5, 1, 1.5, and 2 mM | ↓ Cell survival rate ↓ Cell viability in a concentration-dependent manner (more evident from 1, 1.5, 2), dose-dependent ↓ Migration ↓ Metastasis | [62] |
| SIRT1 inhibition | Cell Study | 9607 | 250 µM 500 µM 1000 µM | ↓ Cell growth ↑ Apoptotic index ↓ Adhesion ability ↓ Migration ability ↓ Glutathione (GSH) levels | [134] |
| miR-424-5p/VEGFA | Cell Study | SaOS-2 and MG-63 cells | 1–1000 μM | ↓ Cell viability beyond 50 μM ↓ VEGFA mRNA ↓ Protein expression ↓ Secreted levels of VEGFA ↑ miR-424-5p expression in microenvironment. | [65] |
| CIC, Rho/ROCK cAMP/PKA | Cell Study | U2OS, 143b, hFOB1.1, MG63, HOS, OS patient tissue samples, VX2 | 1 mM | ↓ OS development ↓ CIC activity ↓ Mitochondrial biogenesis ↓ Mitochondrial function | [136] |
| Animal Study | Rabbit |
4.3. Tumor Microenvironment, Immune Response, and Oxidative Stress
4.4. Melatonin and Cancer Metabolism
4.5. Melatonin and Synergistic Effects with Therapeutics
5. Melatonin in the Clinical Setting
Clinical Studies on Melatonin’s Effects on OS: Prospects and Limitations
6. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| AANAT | Aralkylamine N-acetyltransferase |
| ABC | ATP-binding cassette transporter |
| ACTH | Adrenocorticotropic hormone |
| AD | Autosomal dominant |
| Akt | Protein kinase B |
| APC | Adenomatous polyposis coli |
| AR | Autosomal recessive |
| ATP | Adenosine triphosphate |
| Bcl2 | B-cell lymphoma 2 |
| Bcl-xL | B-cell lymphoma-extra large |
| BLM | Bloom syndrome protein |
| BMI | Body mass index |
| CDK2/4 | Cyclin-dependant kinase 2/4 |
| CDKN2A | Cyclin-dependant kinase inhibitor 2A |
| cGMP | Guanosine 3′,5′-cyclic monophosphate |
| CIC | Capicua transcriptional repressor |
| circRNA | Circular RNA |
| CK1 | Casein kinase 1 |
| c-Myc | Cellular myc |
| Co-F | Co-factor |
| COX | Cyclooxygenase |
| CREB | cAMP-response element binding protein |
| CSC | Cancer stem cell |
| CTGF | Connective tissue growth factor |
| DNMT | DNA methyltransferase |
| Dvl | Dishevelled protein |
| ECV | Extracellular vesicles |
| EGF | Epidermal growth factor |
| EMT | Epithelial–mesenchymal transition |
| ERK | Extracellular signal-regulated kinase |
| FGF | Fibroblast growth factor |
| GnRH | Gonadotropin hormone-releasing hormone |
| GSK-3β | Glycogen synthase kinase 3β |
| HIF-1α | Hypoxia-inducible factor 1 subunit alpha |
| HPβCD | 2-Hydroxypropyl-beta-cyclodextrin. |
| IGF | Insulin growth factor |
| IL-2/6/12/34 | Interleukin |
| INFγ | Interferon gamma |
| INK4A | CDK inhibitors superfamily |
| INOS | Inducible nitric oxide synthase |
| IP3 | Inositol trisphosphate |
| JNK | Jun N-terminal kinase |
| Kif7 | Kinesin family member 7 |
| LA | Linoleic acid |
| LH | Luteinizing hormone |
| lncRNA | Long non-coding RNA |
| MAPK | Mitogen-activated protein kinase |
| M-CSF | Macrophage colony-stimulating factor |
| MCT1/4 | Monocarboxylate transporter 1/4 |
| MDM2 | Murine double minute 2 |
| MDR | Multidrug resistance |
| MeCP2 | Methyl CpG binding protein 2 |
| miR | MicroRNA |
| MMP-9 | Matrix metallopeptidase-9 |
| MSC | Mesenchymal stem cell |
| MT1 | Melatonin receptor 1 |
| MT2 | Melatonin receptor 2 |
| mTOR | Mechanistic (formerly “mammalian”) target of rapamycin |
| NCID | NOTCH intracellular domain |
| NF-κB | Nuclear factor kappa B |
| NOS | Nitric oxide synthases |
| OPG | Osteoprotegerin |
| OS | Osteosarcoma |
| OS-CSC | Osteosarcoma–cancer stem cell |
| OXPHOS | Oxidative phosphorylation |
| PDK | Pyruvate dehydrogenase kinase |
| PEDF | Pigment epithelium-derived factor |
| PGE2 | Prostaglandin E2 |
| P-gp | P-glycoprotein |
| PI3K | Phosphoinositide 3 kinase |
| PKC | Protein kinase C |
| PKG | Protein kinase G |
| PTEN | Phosphotase and tensin homolog |
| PTH | Parathyroid hormone |
| PTHR | Parathyroid hormone receptor |
| PTH-rp | Parathyroid-related peptide |
| RANKL | Receptor activator of nuclear factor kappa beta |
| Rb1 | Retinoblastoma 1 |
| RCT | Randomized clinical trial |
| RecQ | Recombination Q helicases |
| Rh0/ROCK | Rho-associated protein kinase |
| RNA | Ribonucleic acid |
| ROR | Retinoic acid receptor-related orphan receptor |
| ROS | Reactive oxygen species |
| R-SMAD | Receptor-regulated Smad |
| RUNX2 | Runt-related transcription factor 2 |
| SIRT3 | Sirtuin 3 |
| SMAD | Suppressor of mothers against decapentaplegic |
| SOD2 | Superoxide dismutase 2 |
| SOX5 | S RY-Box transcription factor 5 |
| STAT | Signal transducers and activators of transcription |
| SUFU | Suppressor of fused homolog |
| TCA | Tricarboxylic acid cycle |
| TCF/LEF | T-cell factor/lymphoid enhancer factor |
| TET | Ten-eleven translocation |
| TF | Transcription factor |
| TGF | Transforming growth factor |
| TGFβ | Transforming growth factor beta |
| TNFα | Tumor necrosis factor alpha |
| TP53 | Tumor protein p53 |
| TSC 1/2 | Tuberous sclerosis 1/2 |
| VEGF | Vascular endothelial growth factor |
| Wnt | Wingless/Integrated |
| WWOX | WW domain-containing oxidoreductase |
References
- Arendt, J.; Aulinas, A. Physiology of the Pineal Gland and Melatonin. In Endotext; Feingold, K.R., Anawalt, B., Blackman, M.R., Boyce, A., Chrousos, G., Corpas, E., de Herder, W.W., Dhatariya, K., Dungan, K., Hofland, J., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Claustrat, B.; Brun, J.; Chazot, G. The basic physiology and pathophysiology of melatonin. Sleep Med. Rev. 2005, 9, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Lin, R.C.; Yang, J.S.; Yang, W.E.; Reiter, R.J.; Yang, S.F. Molecular and Cellular Mechanisms of Melatonin in Osteosarcoma. Cells 2019, 8, 1618. [Google Scholar] [CrossRef] [PubMed]
- Lu, X.; Yu, S.; Chen, G.; Zheng, W.; Peng, J.; Huang, X.; Chen, L. Insight into the roles of melatonin in bone tissue and bone-related diseases (Review). Int. J. Mol. Med. 2021, 47, 82. [Google Scholar] [CrossRef] [PubMed]
- Waldhauser, F.; Boepple, P.A.; Schemper, M.; Mansfield, M.J.; Crowley, W.F., Jr. Serum melatonin in central precocious puberty is lower than in age-matched prepubertal children. J. Clin. Endocrinol. Metab. 1991, 73, 793–796. [Google Scholar] [CrossRef] [PubMed]
- Langer, M.; Hartmann, J.; Turkof, H.; Waldhauser, F. Melatonin in the human—an overview. Wien. Klin. Wochenschr. 1997, 109, 707–713. [Google Scholar]
- Tordjman, S.; Chokron, S.; Delorme, R.; Charrier, A.; Bellissant, E.; Jaafari, N.; Fougerou, C. Melatonin: Pharmacology, Functions and Therapeutic Benefits. Curr. Neuropharmacol. 2017, 15, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Cassone, V.M.; Warren, W.S.; Brooks, D.S.; Lu, J. Melatonin, the pineal gland, and circadian rhythms. J. Biol. Rhythms 1993, 8, S73–S81. [Google Scholar] [PubMed]
- Lindsey, B.A.; Markel, J.E.; Kleinerman, E.S. Osteosarcoma Overview. Rheumatol. Ther. 2017, 4, 25–43. [Google Scholar] [CrossRef]
- Gupta, D. The pineal gland in relation to growth and development in children. J. Neural Transm. Suppl. 1986, 21, 217–232. [Google Scholar]
- Waldhauser, F.; Steger, H. Changes in melatonin secretion with age and pubescence. J. Neural Transm. Suppl. 1986, 21, 183–197. [Google Scholar]
- Cecon, E.; Oishi, A.; Jockers, R. Melatonin receptors: Molecular pharmacology and signalling in the context of system bias. Br. J. Pharmacol. 2018, 175, 3263–3280. [Google Scholar] [CrossRef] [PubMed]
- Slominski, R.M.; Reiter, R.J.; Schlabritz-Loutsevitch, N.; Ostrom, R.S.; Slominski, A.T. Melatonin membrane receptors in peripheral tissues: Distribution and functions. Mol. Cell Endocrinol. 2012, 351, 152–166. [Google Scholar] [CrossRef] [PubMed]
- Reiter, R.J.; Ma, Q.; Sharma, R. Melatonin in Mitochondria: Mitigating Clear and Present Dangers. Physiology 2020, 35, 86–95. [Google Scholar] [CrossRef]
- Carrillo-Vico, A.; Lardone, P.J.; Alvarez-Sánchez, N.; Rodríguez-Rodríguez, A.; Guerrero, J.M. Melatonin: Buffering the immune system. Int. J. Mol. Sci. 2013, 14, 8638–8683. [Google Scholar] [CrossRef] [PubMed]
- Carlberg, C.; Wiesenberg, I. The orphan receptor family RZR/ROR, melatonin and 5-lipoxygenase: An unexpected relationship. J. Pineal Res. 1995, 18, 171–178. [Google Scholar] [CrossRef]
- Ma, H.; Kang, J.; Fan, W.; He, H.; Huang, F. ROR: Nuclear Receptor for Melatonin or Not? Molecules 2021, 26, 2693. [Google Scholar] [CrossRef]
- Tan, D.X.; Manchester, L.C.; Qin, L.; Reiter, R.J. Melatonin: A Mitochondrial Targeting Molecule Involving Mitochondrial Protection and Dynamics. Int. J. Mol. Sci. 2016, 17, 2124. [Google Scholar] [CrossRef]
- Millet-Boureima, C.; Ennis, C.C.; Jamison, J.; McSweeney, S.; Park, A.; Gamberi, C. Empowering Melatonin Therapeutics with Drosophila Models. Diseases 2021, 9, 67. [Google Scholar] [CrossRef]
- Tarocco, A.; Caroccia, N.; Morciano, G.; Wieckowski, M.R.; Ancora, G.; Garani, G.; Pinton, P. Melatonin as a master regulator of cell death and inflammation: Molecular mechanisms and clinical implications for newborn care. Cell Death Dis. 2019, 10, 317. [Google Scholar] [CrossRef]
- Marqueze, E.C.; Nogueira, L.F.R.; Vetter, C.; Skene, D.J.; Cipolla-Neto, J.; Moreno, C.R.C. Exogenous melatonin decreases circadian misalignment and body weight among early types. J. Pineal Res. 2021, 71, e12750. [Google Scholar] [CrossRef]
- Mohammadi-Sartang, M.; Ghorbani, M.; Mazloom, Z. Effects of melatonin supplementation on blood lipid concentrations: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2018, 37, 1943–1954. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.; Van Montfrans, G.A.; van Someren, E.J.; Mairuhu, G.; Buijs, R.M. Daily nighttime melatonin reduces blood pressure in male patients with essential hypertension. Hypertension 2004, 43, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Owino, S.; Buonfiglio, D.D.C.; Tchio, C.; Tosini, G. Melatonin Signaling a Key Regulator of Glucose Homeostasis and Energy Metabolism. Front. Endocrinol. 2019, 10, 488. [Google Scholar] [CrossRef] [PubMed]
- Ali, T.; Rahman, S.U.; Hao, Q.; Li, W.; Liu, Z.; Ali Shah, F.; Murtaza, I.; Zhang, Z.; Yang, X.; Liu, G.; et al. Melatonin prevents neuroinflammation and relieves depression by attenuating autophagy impairment through FOXO3a regulation. J. Pineal Res. 2020, 69, e12667. [Google Scholar] [CrossRef] [PubMed]
- Potes, Y.; Cachán-Vega, C.; Antuña, E.; García-González, C.; Menéndez-Coto, N.; Boga, J.A.; Gutiérrez-Rodríguez, J.; Bermúdez, M.; Sierra, V.; Vega-Naredo, I.; et al. Benefits of the Neurogenic Potential of Melatonin for Treating Neurological and Neuropsychiatric Disorders. Int. J. Mol. Sci. 2023, 24, 4803. [Google Scholar] [CrossRef] [PubMed]
- Liebmann, P.M.; Wölfler, A.; Felsner, P.; Hofer, D.; Schauenstein, K. Melatonin and the immune system. Int. Arch. Allergy Immunol. 1997, 112, 203–211. [Google Scholar] [CrossRef]
- Srinivasan, V.; Maestroni, G.J.; Cardinali, D.P.; Esquifino, A.I.; Perumal, S.R.; Miller, S.C. Melatonin, immune function and aging. Immun. Ageing 2005, 2, 17. [Google Scholar] [CrossRef]
- Zhou, Y.; Wang, C.; Si, J.; Wang, B.; Zhang, D.; Ding, D.; Zhang, J.; Wang, H. Melatonin up-regulates bone marrow mesenchymal stem cells osteogenic action but suppresses their mediated osteoclastogenesis via MT2-inactivated NF-κB pathway. Br. J. Pharmacol. 2020, 177, 2106–2122. [Google Scholar] [CrossRef]
- Cardinali, D.P.; Ladizesky, M.G.; Boggio, V.; Cutrera, R.A.; Mautalen, C. Melatonin effects on bone: Experimental facts and clinical perspectives. J. Pineal Res. 2003, 34, 81–87. [Google Scholar] [CrossRef]
- Munmun, F.; Witt-Enderby, P.A. Melatonin effects on bone: Implications for use as a therapy for managing bone loss. J. Pineal Res. 2021, 71, e12749. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, H.J.; Bae, M.K.; Kim, Y.D. Suppression of Osteoclastogenesis by Melatonin: A Melatonin Receptor-Independent Action. Int. J. Mol. Sci. 2017, 18, 1142. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, I.J.; Tsai, H.C.; Chang, A.C.; Huang, C.C.; Yang, S.F.; Tang, C.H. Melatonin Inhibits Osteoclastogenesis and Osteolytic Bone Metastasis: Implications for Osteoporosis. Int. J. Mol. Sci. 2021, 22, 9435. [Google Scholar] [CrossRef] [PubMed]
- Everson, C.A.; Folley, A.E.; Toth, J.M. Chronically inadequate sleep results in abnormal bone formation and abnormal bone marrow in rats. Exp. Biol. Med. 2012, 237, 1101–1109. [Google Scholar] [CrossRef] [PubMed]
- Roth, J.A.; Kim, B.G.; Lin, W.L.; Cho, M.I. Melatonin promotes osteoblast differentiation and bone formation. J. Biol. Chem. 1999, 274, 22041–22047. [Google Scholar] [CrossRef] [PubMed]
- Swanson, C.M.; Kohrt, W.M.; Buxton, O.M.; Everson, C.A.; Wright, K.P., Jr.; Orwoll, E.S.; Shea, S.A. The importance of the circadian system & sleep for bone health. Metabolism 2018, 84, 28–43. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.; Pan, Q.; Guo, L. Chronic Sleep Deprivation Impaired Bone Formation in Growing Rats and Down-Regulated PI3K/AKT Signaling in Bone Tissues. Nat. Sci. Sleep 2022, 14, 697–710. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Wang, L.; Chen, L.; Su, T.; Zhang, Y.; Wang, T.; Ma, W.; Yang, F.; Zhai, W.; Xie, Y.; et al. Effects of chronic sleep deprivation on bone mass and bone metabolism in rats. J. Orthop. Surg. Res. 2016, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- Broadhead, M.L.; Clark, J.C.; Myers, D.E.; Dass, C.R.; Choong, P.F. The molecular pathogenesis of osteosarcoma: A review. Sarcoma 2011, 2011, 959248. [Google Scholar] [CrossRef]
- Rossi, M.; Del Fattore, A. Molecular and Translational Research on Bone Tumors. Int. J. Mol. Sci. 2023, 24, 1946. [Google Scholar] [CrossRef]
- de Azevedo, J.W.V.; de Medeiros Fernandes, T.A.A.; Fernandes, J.V., Jr.; de Azevedo, J.C.V.; Lanza, D.C.F.; Bezerra, C.M.; Andrade, V.S.; de Araújo, J.M.G.; Fernandes, J.V. Biology and pathogenesis of human osteosarcoma. Oncol. Lett. 2020, 19, 1099–1116. [Google Scholar] [CrossRef]
- Eaton, B.R.; Schwarz, R.; Vatner, R.; Yeh, B.; Claude, L.; Indelicato, D.J.; Laack, N. Osteosarcoma. Pediatr. Blood Cancer 2021, 68 (Suppl. S2), e28352. [Google Scholar] [CrossRef] [PubMed]
- Todosenko, N.; Khlusov, I.; Yurova, K.; Khaziakhmatova, O.; Litvinova, L. Signal Pathways and microRNAs in Osteosarcoma Growth and the Dual Role of Mesenchymal Stem Cells in Oncogenesis. Int. J. Mol. Sci. 2023, 24, 8993. [Google Scholar] [CrossRef] [PubMed]
- Corre, I.; Verrecchia, F.; Crenn, V.; Redini, F.; Trichet, V. The Osteosarcoma Microenvironment: A Complex But Targetable Ecosystem. Cells 2020, 9, 976. [Google Scholar] [CrossRef] [PubMed]
- Nørregaard, K.S.; Jürgensen, H.J.; Gårdsvoll, H.; Engelholm, L.H.; Behrendt, N.; Søe, K. Osteosarcoma and Metastasis Associated Bone Degradation-A Tale of Osteoclast and Malignant Cell Cooperativity. Int. J. Mol. Sci. 2021, 22, 6865. [Google Scholar] [CrossRef] [PubMed]
- Tang, N.; Song, W.X.; Luo, J.; Haydon, R.C.; He, T.C. Osteosarcoma development and stem cell differentiation. Clin. Orthop. Relat. Res. 2008, 466, 2114–2130. [Google Scholar] [CrossRef]
- Urlić, I.; Jovičić, M.; Ostojić, K.; Ivković, A. Cellular and Genetic Background of Osteosarcoma. Curr. Issues Mol. Biol. 2023, 45, 4344–4358. [Google Scholar] [CrossRef]
- Abarrategi, A.; Tornin, J.; Martinez-Cruzado, L.; Hamilton, A.; Martinez-Campos, E.; Rodrigo, J.P.; González, M.V.; Baldini, N.; Garcia-Castro, J.; Rodriguez, R. Osteosarcoma: Cells-of-Origin, Cancer Stem Cells, and Targeted Therapies. Stem Cells Int. 2016, 2016, 3631764. [Google Scholar] [CrossRef]
- Gianferante, D.M.; Mirabello, L.; Savage, S.A. Germline and somatic genetics of osteosarcoma—Connecting aetiology, biology and therapy. Nat. Rev. Endocrinol. 2017, 13, 480–491. [Google Scholar] [CrossRef]
- Wu, C.C.; Beird, H.C.; Andrew Livingston, J.; Advani, S.; Mitra, A.; Cao, S.; Reuben, A.; Ingram, D.; Wang, W.L.; Ju, Z.; et al. Immuno-genomic landscape of osteosarcoma. Nat. Commun. 2020, 11, 1008. [Google Scholar] [CrossRef]
- Panez-Toro, I.; Munoz-Garcia, J.; Vargas-Franco, J.W.; Renodon-Corniere, A.; Heymann, M.F.; Lezot, F.; Heymann, D. Advances in Osteosarcoma. Curr. Osteoporos. Rep. 2023, 21, 330–343. [Google Scholar] [CrossRef]
- Gong, T.; Su, X.; Xia, Q.; Wang, J.; Kan, S. Expression of NF-κB and PTEN in osteosarcoma and its clinical significance. Oncol. Lett. 2017, 14, 6744–6748. [Google Scholar] [CrossRef] [PubMed]
- Del Mare, S.; Husanie, H.; Iancu, O.; Abu-Odeh, M.; Evangelou, K.; Lovat, F.; Volinia, S.; Gordon, J.; Amir, G.; Stein, J.; et al. WWOX and p53 Dysregulation Synergize to Drive the Development of Osteosarcoma. Cancer Res. 2016, 76, 6107–6117. [Google Scholar] [CrossRef] [PubMed]
- Hameed, M.; Mandelker, D. Tumor Syndromes Predisposing to Osteosarcoma. Adv. Anat. Pathol. 2018, 25, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zhao, L.; Tian, W.; Liao, Z.; Zheng, H.; Wang, G.; Chen, K. Correlation of WWOX, RUNX2 and VEGFA protein expression in human osteosarcoma. BMC Med. Genom. 2013, 6, 56. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, G.P.; Burns, K.L.; Rosenberg, A.E.; Louis, D.N. CDKN2A gene deletions and loss of p16 expression occur in osteosarcomas that lack RB alterations. Am. J. Pathol. 1998, 153, 159–163. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.; Aboussekhra, A. p16(INK4A) inhibits the pro-metastatic potentials of osteosarcoma cells through targeting the ERK pathway and TGF-β1. Mol. Carcinog. 2016, 55, 525–536. [Google Scholar] [CrossRef] [PubMed]
- Wei, G.; Lonardo, F.; Ueda, T.; Kim, T.; Huvos, A.G.; Healey, J.H.; Ladanyi, M. CDK4 gene amplification in osteosarcoma: Reciprocal relationship with INK4A gene alterations and mapping of 12q13 amplicons. Int. J. Cancer 1999, 80, 199–204. [Google Scholar] [CrossRef]
- Dujardin, F.; Binh, M.B.; Bouvier, C.; Gomez-Brouchet, A.; Larousserie, F.; Muret, A.; Louis-Brennetot, C.; Aurias, A.; Coindre, J.M.; Guillou, L.; et al. MDM2 and CDK4 immunohistochemistry is a valuable tool in the differential diagnosis of low-grade osteosarcomas and other primary fibro-osseous lesions of the bone. Mod. Pathol. 2011, 24, 624–637. [Google Scholar] [CrossRef]
- Han, G.; Wang, Y.; Bi, W. C-Myc overexpression promotes osteosarcoma cell invasion via activation of MEK-ERK pathway. Oncol. Res. 2012, 20, 149–156. [Google Scholar] [CrossRef]
- Wang, Q.; Liu, H.; Wang, Q.; Zhou, F.; Liu, Y.; Zhang, Y.; Ding, H.; Yuan, M.; Li, F.; Chen, Y. Involvement of c-Fos in cell proliferation, migration, and invasion in osteosarcoma cells accompanied by altered expression of Wnt2 and Fzd9. PLoS ONE 2017, 12, e0180558. [Google Scholar] [CrossRef]
- Li, Y.; Zou, J.; Li, B.; Du, J. Anticancer effects of melatonin via regulating lncRNA JPX-Wnt/β-catenin signalling pathway in human osteosarcoma cells. J. Cell Mol. Med. 2021, 25, 9543–9556. [Google Scholar] [CrossRef] [PubMed]
- Hattinger, C.M.; Patrizio, M.P.; Fantoni, L.; Casotti, C.; Riganti, C.; Serra, M. Drug Resistance in Osteosarcoma: Emerging Biomarkers, Therapeutic Targets and Treatment Strategies. Cancers 2021, 13, 2878. [Google Scholar] [CrossRef] [PubMed]
- Otoukesh, B.; Boddouhi, B.; Moghtadaei, M.; Kaghazian, P.; Kaghazian, M. Novel molecular insights and new therapeutic strategies in osteosarcoma. Cancer Cell Int. 2018, 18, 158. [Google Scholar] [CrossRef] [PubMed]
- Vimalraj, S.; Saravanan, S.; Raghunandhakumar, S.; Anuradha, D. Melatonin regulates tumor angiogenesis via miR-424-5p/VEGFA signaling pathway in osteosarcoma. Life Sci. 2020, 256, 118011. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Wu, W.; Shao, Z. NOTCH Signaling in Osteosarcoma. Curr. Issues Mol. Biol. 2023, 45, 2266–2283. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Zheng, S.; He, Q.; Li, Y. Recent Advances of Circular RNAs as Biomarkers for Osteosarcoma. Int. J. Gen. Med. 2023, 16, 173–183. [Google Scholar] [CrossRef]
- Abdraboh, M.E.; El-Missiry, M.A.; Othman, A.I.; Taha, A.N.; Elhamed, D.S.A.; Amer, M.E. Constant light exposure and/or pinealectomy increases susceptibility to trichloroethylene-induced hepatotoxicity and liver cancer in male mice. Environ. Sci. Pollut. Res. Int. 2022, 29, 60371–60384. [Google Scholar] [CrossRef]
- Chandhanayingyong, C.; Kim, Y.; Staples, J.R.; Hahn, C.; Lee, F.Y. MAPK/ERK Signaling in Osteosarcomas, Ewing Sarcomas and Chondrosarcomas: Therapeutic Implications and Future Directions. Sarcoma 2012, 2012, 404810. [Google Scholar] [CrossRef]
- Fang, F.; VanCleave, A.; Helmuth, R.; Torres, H.; Rickel, K.; Wollenzien, H.; Sun, H.; Zeng, E.; Zhao, J.; Tao, J. Targeting the Wnt/β-catenin pathway in human osteosarcoma cells. Oncotarget 2018, 9, 36780–36792. [Google Scholar] [CrossRef]
- Hu, K.; Dai, H.B.; Qiu, Z.L. mTOR signaling in osteosarcoma: Oncogenesis and therapeutic aspects (Review). Oncol. Rep. 2016, 36, 1219–1225. [Google Scholar] [CrossRef]
- Ji, Z.; Shen, J.; Lan, Y.; Yi, Q.; Liu, H. Targeting signaling pathways in osteosarcoma: Mechanisms and clinical studies. MedComm 2023, 4, e308. [Google Scholar] [CrossRef] [PubMed]
- Kopustinskiene, D.M.; Bernatonienė, J. Molecular Mechanisms of Melatonin-Mediated Cell Protection and Signaling in Health and Disease. Pharmaceutics 2021, 13, 129. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xiao, Q.; Xiao, J.; Niu, C.; Li, Y.; Zhang, X.; Zhou, Z.; Shu, G.; Yin, G. Wnt/β-catenin signalling: Function, biological mechanisms, and therapeutic opportunities. Signal Transduct. Target. Ther. 2022, 7, 3. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Wang, X.; Chen, Z.; Zhou, H.; Xiao, Y. The role and mechanism of JAK2/STAT3 signaling pathway regulated by m6A methyltransferase KIAA1429 in osteosarcoma. J. Bone Oncol. 2023, 39, 100471. [Google Scholar] [CrossRef] [PubMed]
- Mihanfar, A.; Yousefi, B.; Azizzadeh, B.; Majidinia, M. Interactions of melatonin with various signaling pathways: Implications for cancer therapy. Cancer Cell Int. 2022, 22, 420. [Google Scholar] [CrossRef] [PubMed]
- Truong, D.D.; Lamhamedi-Cherradi, S.E.; Ludwig, J.A. Targeting the IGF/PI3K/mTOR pathway and AXL/YAP1/TAZ pathways in primary bone cancer. J. Bone Oncol. 2022, 33, 100419. [Google Scholar] [CrossRef] [PubMed]
- Verrecchia, F.; Rédini, F. Transforming Growth Factor-β Signaling Plays a Pivotal Role in the Interplay Between Osteosarcoma Cells and Their Microenvironment. Front. Oncol. 2018, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Z.; Zhang, S.F.; Yang, Z.H.; Ye, Z.W.; Liu, J. Punicalagin suppresses osteosarcoma growth and metastasis by regulating NF-κB signaling. J. Biol. Regul. Homeost. Agents 2020, 34, 1699–1708. [Google Scholar] [CrossRef]
- Wei, M.; Zhang, C.; Tian, Y.; Du, X.; Wang, Q.; Zhao, H. Expression and Function of WNT6: From Development to Disease. Front. Cell Dev. Biol. 2020, 8, 558155. [Google Scholar] [CrossRef]
- Yan, J.; Wang, Q.; Zou, K.; Wang, L.; Schwartz, E.B.; Fuchs, J.R.; Zheng, Z.; Wu, J. Inhibition of the JAK2/STAT3 signaling pathway exerts a therapeutic effect on osteosarcoma. Mol. Med. Rep. 2015, 12, 498–502. [Google Scholar] [CrossRef]
- Yao, Z.; Han, L.; Chen, Y.; He, F.; Sun, B.; Kamar, S.; Zhang, Y.; Yang, Y.; Wang, C.; Yang, Z. Hedgehog signalling in the tumourigenesis and metastasis of osteosarcoma, and its potential value in the clinical therapy of osteosarcoma. Cell Death Dis. 2018, 9, 701. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Yu, X.H.; Yan, Y.G.; Wang, C.; Wang, W.J. PI3K/Akt signaling in osteosarcoma. Clin. Chim. Acta 2015, 444, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Liu, Y.; Wang, X.; Wang, J.; Xi, G. lncRNA SNHG10 Promotes the Proliferation and Invasion of Osteosarcoma via Wnt/β-Catenin Signaling. Mol. Ther. Nucleic Acids 2020, 22, 957–970. [Google Scholar] [CrossRef] [PubMed]
- Xia, K.; Huang, X.; Zhao, Y.; Yang, I.; Guo, W. SERPINH1 enhances the malignancy of osteosarcoma via PI3K-Akt signaling pathway. Transl. Oncol. 2023, 39, 101802. [Google Scholar] [CrossRef] [PubMed]
- Carbajo-Pescador, S.; Ordoñez, R.; Benet, M.; Jover, R.; García-Palomo, A.; Mauriz, J.L.; González-Gallego, J. Inhibition of VEGF expression through blockade of Hif1α and STAT3 signalling mediates the anti-angiogenic effect of melatonin in HepG2 liver cancer cells. Br. J. Cancer 2013, 109, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Chong, Z.X.; Yeap, S.K.; Ho, W.Y. Unraveling the roles of miRNAs in regulating epithelial-to-mesenchymal transition (EMT) in osteosarcoma. Pharmacol. Res. 2021, 172, 105818. [Google Scholar] [CrossRef]
- Gong, H.; Tao, Y.; Xiao, S.; Li, X.; Fang, K.; Wen, J.; Zeng, M.; Liu, Y.; Chen, Y. Identification of an EMT-related gene-based prognostic signature in osteosarcoma. Cancer Med. 2023, 12, 12912–12928. [Google Scholar] [CrossRef]
- Hinton, K.; Kirk, A.; Paul, P.; Persad, S. Regulation of the Epithelial to Mesenchymal Transition in Osteosarcoma. Biomolecules 2023, 13, 398. [Google Scholar] [CrossRef]
- Zhu, H.; Tang, J.; Tang, M.; Cai, H. Upregulation of SOX9 in osteosarcoma and its association with tumor progression and patients’ prognosis. Diagn. Pathol. 2013, 8, 183. [Google Scholar] [CrossRef]
- Ruan, H.; Hu, S.; Zhang, H.; Du, G.; Li, X.; Li, X.; Li, X. Upregulated SOX9 expression indicates worse prognosis in solid tumors: A systematic review and meta-analysis. Oncotarget 2017, 8, 113163–113173. [Google Scholar] [CrossRef]
- Wang, D.Y.; Wu, Y.N.; Huang, J.Q.; Wang, W.; Xu, M.; Jia, J.P.; Han, G.; Mao, B.B.; Bi, W.Z. Hippo/YAP signaling pathway is involved in osteosarcoma chemoresistance. Chin. J. Cancer 2016, 35, 47. [Google Scholar] [CrossRef]
- Mongre, R.K.; Sodhi, S.S.; Ghosh, M.; Kim, J.H.; Kim, N.; Sharma, N.; Jeong, D.K. A New Paradigm to Mitigate Osteosarcoma by Regulation of MicroRNAs and Suppression of the NF-κB Signaling Cascade. Dev. Reprod. 2014, 18, 197–212. [Google Scholar] [CrossRef]
- Durfee, R.A.; Mohammed, M.; Luu, H.H. Review of Osteosarcoma and Current Management. Rheumatol. Ther. 2016, 3, 221–243. [Google Scholar] [CrossRef] [PubMed]
- De Martino, V.; Rossi, M.; Battafarano, G.; Pepe, J.; Minisola, S.; Del Fattore, A. Extracellular Vesicles in Osteosarcoma: Antagonists or Therapeutic Agents? Int. J. Mol. Sci. 2021, 22, 12586. [Google Scholar] [CrossRef]
- Perut, F.; Roncuzzi, L.; Baldini, N. The Emerging Roles of Extracellular Vesicles in Osteosarcoma. Front. Oncol. 2019, 9, 1342. [Google Scholar] [CrossRef]
- Wang, R.X.; Liu, H.; Xu, L.; Zhang, H.; Zhou, R.X. Melatonin downregulates nuclear receptor RZR/RORγ expression causing growth-inhibitory and anti-angiogenesis activity in human gastric cancer cells in vitro and in vivo. Oncol. Lett. 2016, 12, 897–903. [Google Scholar] [CrossRef]
- Yang, Q.; Liu, J.; Wu, B.; Wang, X.; Jiang, Y.; Zhu, D. Role of extracellular vesicles in osteosarcoma. Int. J. Med. Sci. 2022, 19, 1216–1226. [Google Scholar] [CrossRef]
- Sun, C.; Li, S. PTHR1 in osteosarcoma: Specific molecular mechanisms and comprehensive functional perspective. J. Cell Mol. Med. 2021, 25, 3175–3181. [Google Scholar] [CrossRef]
- Mori, T.; Sato, Y.; Miyamoto, K.; Kobayashi, T.; Shimizu, T.; Kanagawa, H.; Katsuyama, E.; Fujie, A.; Hao, W.; Tando, T.; et al. TNFα promotes osteosarcoma progression by maintaining tumor cells in an undifferentiated state. Oncogene 2014, 33, 4236–4241. [Google Scholar] [CrossRef]
- Xu, B.; Jin, X.; Yang, T.; Zhang, Y.; Liu, S.; Wu, L.; Ying, H.; Wang, Z. Upregulated lncRNA THRIL/TNF-α Signals Promote Cell Growth and Predict Poor Clinical Outcomes of Osteosarcoma. Onco Targets Ther. 2020, 13, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Itoh, H.; Kadomatsu, T.; Tanoue, H.; Yugami, M.; Miyata, K.; Endo, M.; Morinaga, J.; Kobayashi, E.; Miyamoto, T.; Kurahashi, R.; et al. TET2-dependent IL-6 induction mediated by the tumor microenvironment promotes tumor metastasis in osteosarcoma. Oncogene 2018, 37, 2903–2920. [Google Scholar] [CrossRef]
- Zhao, H.; Wu, Y.; Chen, Y.; Liu, H. Clinical significance of hypoxia-inducible factor 1 and VEGF-A in osteosarcoma. Int. J. Clin. Oncol. 2015, 20, 1233–1243. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.S.; Liu, Q.; Tian, J.; He, H.B.; Luo, W. Angiogenesis Process in Osteosarcoma: An Updated Perspective of Pathophysiology and Therapeutics. Am. J. Med. Sci. 2019, 357, 280–288. [Google Scholar] [CrossRef] [PubMed]
- Sotgia, F.; Martinez-Outschoorn, U.E.; Lisanti, M.P. The reverse Warburg effect in osteosarcoma. Oncotarget 2014, 5, 7982–7983. [Google Scholar] [CrossRef] [PubMed]
- Bonuccelli, G.; Avnet, S.; Grisendi, G.; Salerno, M.; Granchi, D.; Dominici, M.; Kusuzaki, K.; Baldini, N. Role of mesenchymal stem cells in osteosarcoma and metabolic reprogramming of tumor cells. Oncotarget 2014, 5, 7575–7588. [Google Scholar] [CrossRef] [PubMed]
- Prudowsky, Z.D.; Yustein, J.T. Recent Insights into Therapy Resistance in Osteosarcoma. Cancers 2020, 13, 83. [Google Scholar] [CrossRef]
- Marchandet, L.; Lallier, M.; Charrier, C.; Baud’huin, M.; Ory, B.; Lamoureux, F. Mechanisms of Resistance to Conventional Therapies for Osteosarcoma. Cancers 2021, 13, 683. [Google Scholar] [CrossRef]
- Jones, M.E.; Schoemaker, M.J.; McFadden, E.C.; Wright, L.B.; Johns, L.E.; Swerdlow, A.J. Night shift work and risk of breast cancer in women: The Generations Study cohort. Br. J. Cancer 2019, 121, 172–179. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Schulmeister, K. Melatonin and cancer risk: Does light at night compromise physiologic cancer protection by lowering serum melatonin levels? Br. J. Cancer 2004, 90, 941–943. [Google Scholar] [CrossRef]
- Spiegel, D.; Sephton, S. Re: Night Shift Work, Light at Night, and Risk of Breast Cancer. JNCI J. Natl. Cancer Inst. 2002, 94, 530. [Google Scholar] [CrossRef]
- Tamarkin, L.; Cohen, M.; Roselle, D.; Reichert, C.; Lippman, M.; Chabner, B. Melatonin inhibition and pinealectomy enhancement of 7,12-dimethylbenz(a)anthracene-induced mammary tumors in the rat. Cancer Res. 1981, 41, 4432–4436. [Google Scholar]
- Benítez-King, G.; Hernández, M.E.; Tovar, R.; Ramírez, G. Melatonin activates PKC-alpha but not PKC-epsilon in N1E-115 cells. Neurochem. Int. 2001, 39, 95–102. [Google Scholar] [CrossRef]
- Gurunathan, S.; Qasim, M.; Kang, M.H.; Kim, J.H. Role and Therapeutic Potential of Melatonin in Various Type of Cancers. OncoTargets Ther. 2021, 14, 2019–2052. [Google Scholar] [CrossRef]
- Kubatka, P.; Zubor, P.; Busselberg, D.; Kwon, T.K.; Adamek, M.; Petrovic, D.; Opatrilova, R.; Gazdikova, K.; Caprnda, M.; Rodrigo, L.; et al. Melatonin and breast cancer: Evidences from preclinical and human studies. Crit. Rev. Oncol. Hematol. 2018, 122, 133–143. [Google Scholar] [CrossRef]
- Li, Y.; Li, S.; Zhou, Y.; Meng, X.; Zhang, J.J.; Xu, D.P.; Li, H.B. Melatonin for the prevention and treatment of cancer. Oncotarget 2017, 8, 39896–39921. [Google Scholar] [CrossRef]
- Panzer, A.; Lottering, M.L.; Bianchi, P.; Glencross, D.K.; Stark, J.H.; Seegers, J.C. Melatonin has no effect on the growth, morphology or cell cycle of human breast cancer (MCF-7), cervical cancer (HeLa), osteosarcoma (MG-63) or lymphoblastoid (TK6) cells. Cancer Lett. 1998, 122, 17–23. [Google Scholar] [CrossRef]
- Zare, H.; Shafabakhsh, R.; Reiter, R.J.; Asemi, Z. Melatonin is a potential inhibitor of ovarian cancer: Molecular aspects. J. Ovarian Res. 2019, 12, 26. [Google Scholar] [CrossRef]
- González, A.; González-González, A.; Alonso-González, C.; Menéndez-Menéndez, J.; Martínez-Campa, C.; Cos, S. Melatonin inhibits angiogenesis in SH-SY5Y human neuroblastoma cells by downregulation of VEGF. Oncol. Rep. 2017, 37, 2433–2440. [Google Scholar] [CrossRef] [PubMed]
- Marques, J.H.M.; Mota, A.L.; Oliveira, J.G.; Lacerda, J.Z.; Stefani, J.P.; Ferreira, L.C.; Castro, T.B.; Aristizábal-Pachón, A.F.; Zuccari, D. Melatonin restrains angiogenic factors in triple-negative breast cancer by targeting miR-152-3p: In vivo and in vitro studies. Life Sci. 2018, 208, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Gui, S.; Zhou, Q.; Wang, Y. Melatonin inhibits the migration of human lung adenocarcinoma A549 cell lines involving JNK/MAPK pathway. PLoS ONE 2014, 9, e101132. [Google Scholar] [CrossRef] [PubMed]
- Park, E.J.; Woo, S.M.; Min, K.J.; Kwon, T.K. Transcriptional and post-translational regulation of Bim controls apoptosis in melatonin-treated human renal cancer Caki cells. J. Pineal Res. 2014, 56, 97–106. [Google Scholar] [CrossRef]
- Talib, W.H.; Alsayed, A.R.; Abuawad, A.; Daoud, S.; Mahmod, A.I. Melatonin in Cancer Treatment: Current Knowledge and Future Opportunities. Molecules 2021, 26, 2506. [Google Scholar] [CrossRef] [PubMed]
- Jung-Hynes, B.; Nihal, M.; Zhong, W.; Ahmad, N. Role of sirtuin histone deacetylase SIRT1 in prostate cancer. A target for prostate cancer management via its inhibition? J. Biol. Chem. 2009, 284, 3823–3832. [Google Scholar] [CrossRef] [PubMed]
- Sohn, E.J.; Won, G.; Lee, J.; Lee, S.; Kim, S.H. Upregulation of miRNA3195 and miRNA374b Mediates the Anti-Angiogenic Properties of Melatonin in Hypoxic PC-3 Prostate Cancer Cells. J. Cancer 2015, 6, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Targhazeh, N.; Reiter, R.J.; Rahimi, M.; Qujeq, D.; Yousefi, T.; Shahavi, M.H.; Mir, S.M. Oncostatic activities of melatonin: Roles in cell cycle, apoptosis, and autophagy. Biochimie 2022, 200, 44–59. [Google Scholar] [CrossRef] [PubMed]
- Leon-Blanco, M.M.; Guerrero, J.M.; Reiter, R.J.; Calvo, J.R.; Pozo, D. Melatonin inhibits telomerase activity in the MCF-7 tumor cell line both in vivo and in vitro. J. Pineal Res. 2003, 35, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Lu, K.H.; Lin, C.W.; Hsieh, Y.H.; Su, S.C.; Reiter, R.J.; Yang, S.F. New insights into antimetastatic signaling pathways of melatonin in skeletomuscular sarcoma of childhood and adolescence. Cancer Metastasis Rev. 2020, 39, 303–320. [Google Scholar] [CrossRef]
- Reiter, R.J.; Sharma, R.; Rosales-Corral, S. Anti-Warburg Effect of Melatonin: A Proposed Mechanism to Explain its Inhibition of Multiple Diseases. Int. J. Mol. Sci. 2021, 22, 764. [Google Scholar] [CrossRef]
- Samec, M.; Liskova, A.; Koklesova, L.; Zhai, K.; Varghese, E.; Samuel, S.M.; Šudomová, M.; Lucansky, V.; Kassayova, M.; Pec, M.; et al. Metabolic Anti-Cancer Effects of Melatonin: Clinically Relevant Prospects. Cancers 2021, 13, 3018. [Google Scholar] [CrossRef]
- Sánchez-Hidalgo, M.; Guerrero, J.M.; Villegas, I.; Packham, G.; de la Lastra, C.A. Melatonin, a natural programmed cell death inducer in cancer. Curr. Med. Chem. 2012, 19, 3805–3821. [Google Scholar] [CrossRef]
- Lu, K.H.; Su, S.C.; Lin, C.W.; Hsieh, Y.H.; Lin, Y.C.; Chien, M.H.; Reiter, R.J.; Yang, S.F. Melatonin attenuates osteosarcoma cell invasion by suppression of C-C motif chemokine ligand 24 through inhibition of the c-Jun N-terminal kinase pathway. J. Pineal Res. 2018, 65, e12507. [Google Scholar] [CrossRef] [PubMed]
- Qu, H.; Xue, Y.; Lian, W.; Wang, C.; He, J.; Fu, Q.; Zhong, L.; Lin, N.; Lai, L.; Ye, Z.; et al. Melatonin inhibits osteosarcoma stem cells by suppressing SOX9-mediated signaling. Life Sci. 2018, 207, 253–264. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Cai, L.; Jiang, P.; Wang, J.; Gao, C.; Feng, H.; Wang, C.; Pan, H.; Yang, Y. SIRT1 inhibition by melatonin exerts antitumor activity in human osteosarcoma cells. Eur. J. Pharmacol. 2013, 715, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Xia, Y.; Cai, X.; Fan, J.; Zhang, L.; Li, Z.; Ren, J.; Wu, G.; Zhu, F. RhoA/ROCK pathway inhibition by fasudil suppresses the vasculogenic mimicry of U2OS osteosarcoma cells in vitro. Anticancer. Drugs 2017, 28, 514–521. [Google Scholar] [CrossRef]
- Zhang, W.; Zhao, W.; Li, Q.; Zhao, D.; Qu, J.; Yuan, Z.; Cheng, Z.; Zhu, X.; Zhuang, X.; Zhang, Z. 3D-printing magnesium-polycaprolactone loaded with melatonin inhibits the development of osteosarcoma by regulating cell-in-cell structures. J. Nanobiotechnol. 2021, 19, 263. [Google Scholar] [CrossRef]
- Liu, L.; Xu, Y.; Reiter, R.J. Melatonin inhibits the proliferation of human osteosarcoma cell line MG-63. Bone 2013, 55, 432–438. [Google Scholar] [CrossRef]
- Topal, B.; Çetin Altındal, D.; Gümüşderelioğlu, M. Melatonin/HPβCD complex: Microwave synthesis, integration with chitosan scaffolds and inhibitory effects on MG-63CELLS. Int. J. Pharm. 2015, 496, 801–811. [Google Scholar] [CrossRef]
- Cascini, C.; Chiodoni, C. The Immune Landscape of Osteosarcoma: Implications for Prognosis and Treatment Response. Cells 2021, 10, 1668. [Google Scholar] [CrossRef]
- Heymann, M.F.; Lézot, F.; Heymann, D. The contribution of immune infiltrates and the local microenvironment in the pathogenesis of osteosarcoma. Cell Immunol. 2019, 343, 103711. [Google Scholar] [CrossRef]
- Prieto-Domínguez, N.; Ordóñez, R.; Fernández, A.; Méndez-Blanco, C.; Baulies, A.; Garcia-Ruiz, C.; Fernández-Checa, J.C.; Mauriz, J.L.; González-Gallego, J. Melatonin-induced increase in sensitivity of human hepatocellular carcinoma cells to sorafenib is associated with reactive oxygen species production and mitophagy. J. Pineal Res. 2016, 61, 396–407. [Google Scholar] [CrossRef]
- Dhupper, V.; Yadav, U.; Verma, M.; Dahiya, K.; Chahal, A.; Kumar, S.; Kumar, R.; Yadav, N. Oxidative Stress in Primary Bone Tumors: A Comparative Analysis. Cureus 2022, 14, e25335. [Google Scholar] [CrossRef] [PubMed]
- Bejarano, I.; Espino, J.; Barriga, C.; Reiter, R.J.; Pariente, J.A.; Rodríguez, A.B. Pro-oxidant effect of melatonin in tumour leucocytes: Relation with its cytotoxic and pro-apoptotic effects. Basic. Clin. Pharmacol. Toxicol. 2011, 108, 14–20. [Google Scholar] [CrossRef]
- Clapp-Lilly, K.L.; Smith, M.A.; Perry, G.; Harris, P.L.; Zhu, X.; Duffy, L.K. Melatonin acts as antioxidant and pro-oxidant in an organotypic slice culture model of Alzheimer’s disease. Neuroreport 2001, 12, 1277–1280. [Google Scholar] [CrossRef]
- Girish, K.S.; Paul, M.; Thushara, R.M.; Hemshekhar, M.; Shanmuga Sundaram, M.; Rangappa, K.S.; Kemparaju, K. Melatonin elevates apoptosis in human platelets via ROS mediated mitochondrial damage. Biochem. Biophys. Res. Commun. 2013, 438, 198–204. [Google Scholar] [CrossRef]
- Medina-Navarro, R.; Duran-Reyes, G.; Hicks, J.J. Pro-oxidating properties of melatonin in the in vitro interaction with the singlet oxygen. Endocr. Res. 1999, 25, 263–280. [Google Scholar] [CrossRef]
- Osseni, R.A.; Rat, P.; Bogdan, A.; Warnet, J.M.; Touitou, Y. Evidence of prooxidant and antioxidant action of melatonin on human liver cell line HepG2. Life Sci. 2000, 68, 387–399. [Google Scholar] [CrossRef]
- Wölfler, A.; Caluba, H.C.; Abuja, P.M.; Dohr, G.; Schauenstein, K.; Liebmann, P.M. Prooxidant activity of melatonin promotes fas-induced cell death in human leukemic Jurkat cells. FEBS Lett. 2001, 502, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.M.; Zhang, Y. Melatonin: A well-documented antioxidant with conditional pro-oxidant actions. J. Pineal Res. 2014, 57, 131–146. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.M.; Zhang, Y.; Zhang, B.X. The role of mitochondrial complex III in melatonin-induced ROS production in cultured mesangial cells. J. Pineal Res. 2011, 50, 78–82. [Google Scholar] [CrossRef]
- Liberti, M.V.; Locasale, J.W. The Warburg Effect: How Does it Benefit Cancer Cells? Trends Biochem. Sci. 2016, 41, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Giang, A.H.; Raymond, T.; Brookes, P.; de Mesy Bentley, K.; Schwarz, E.; O’Keefe, R.; Eliseev, R. Mitochondrial dysfunction and permeability transition in osteosarcoma cells showing the Warburg effect. J. Biol. Chem. 2013, 288, 33303–33311. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Jin, Y.; Fan, Z. The Mechanism of Warburg Effect-Induced Chemoresistance in Cancer. Front. Oncol. 2021, 11, 698023. [Google Scholar] [CrossRef] [PubMed]
- Feng, Z.; Ou, Y.; Hao, L. The roles of glycolysis in osteosarcoma. Front. Pharmacol. 2022, 13, 950886. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Yue, X.; Luo, Q. Metabolic reprogramming in osteosarcoma. Pediatr. Discov. 2023, 1, e18. [Google Scholar] [CrossRef]
- Blask, D.E.; Sauer, L.A.; Dauchy, R.T.; Holowachuk, E.W.; Ruhoff, M.S.; Kopff, H.S. Melatonin Inhibition of Cancer Growth in Vivo Involves Suppression of Tumor Fatty Acid Metabolism via Melatonin Receptor-mediated Signal Transduction Events1. Cancer Res. 1999, 59, 4693–4701. [Google Scholar] [PubMed]
- Lissoni, P.; Barni, S.; Mandalà, M.; Ardizzoia, A.; Paolorossi, F.; Vaghi, M.; Longarini, R.; Malugani, F.; Tancini, G. Decreased toxicity and increased efficacy of cancer chemotherapy using the pineal hormone melatonin in metastatic solid tumour patients with poor clinical status. Eur. J. Cancer 1999, 35, 1688–1692. [Google Scholar] [CrossRef]
- Lissoni, P.; Tancini, G.; Barni, S.; Paolorossi, F.; Ardizzoia, A.; Conti, A.; Maestroni, G. Treatment of cancer chemotherapy-induced toxicity with the pineal hormone melatonin. Support. Care Cancer 1997, 5, 126–129. [Google Scholar] [CrossRef]
- Ma, Z.; Xu, L.; Liu, D.; Zhang, X.; Di, S.; Li, W.; Zhang, J.; Reiter, R.J.; Han, J.; Li, X.; et al. Utilizing Melatonin to Alleviate Side Effects of Chemotherapy: A Potentially Good Partner for Treating Cancer with Ageing. Oxid. Med. Cell Longev. 2020, 2020, 6841581. [Google Scholar] [CrossRef]
- Ghielmini, M.; Pagani, O.; de Jong, J.; Pampallona, S.; Conti, A.; Maestroni, G.; Sessa, C.; Cavalli, F. Double-blind randomized study on the myeloprotective effect of melatonin in combination with carboplatin and etoposide in advanced lung cancer. Br. J. Cancer 1999, 80, 1058–1061. [Google Scholar] [CrossRef]
- Niu, G.; Yousefi, B.; Qujeq, D.; Marjani, A.; Asadi, J.; Wang, Z.; Mir, S.M. Melatonin and doxorubicin co-delivered via a functionalized graphene-dendrimeric system enhances apoptosis of osteosarcoma cells. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 119, 111554. [Google Scholar] [CrossRef]
- Wang, Y.P.; Yang, Z.P. Effects of melatonin combined with Cis-platinum or methotrexate on the proliferation of osteosarcoma cell line SaOS-2. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2015, 37, 215–220. [Google Scholar] [CrossRef]
- Hosseini, F.; Shanehbandi, D.; Soleimanpour, J.; Yousefi, B.; Alemi, F. Melatonin Increases the Sensitivity of Osteosarcoma Cells to Chemotherapy Drug Cisplatin. Drug Res. 2022, 72, 312–318. [Google Scholar] [CrossRef]
- Lawlor, P.G.; McNamara-Kilian, M.T.; MacDonald, A.R.; Momoli, F.; Tierney, S.; Lacaze-Masmonteil, N.; Dasgupta, M.; Agar, M.; Pereira, J.L.; Currow, D.C.; et al. Melatonin to prevent delirium in patients with advanced cancer: A double blind, parallel, randomized, controlled, feasibility trial. BMC Palliat. Care 2020, 19, 163. [Google Scholar] [CrossRef]
- Hrushesky, W.J.M.; Lis, C.G.; Levin, R.D.; Grutsch, J.F.; Birdsall, T.; Wood, P.A.; Huff, D.F.Q.; Reynolds, J.L.; Pearl, D.K.; Shen, X.; et al. Daily evening melatonin prolongs survival among patients with advanced non-small-cell lung cancer. Biol. Rhythm. Res. 2022, 53, 1043–1057. [Google Scholar] [CrossRef]
- Lévi, F. Circadian chronotherapy for human cancers. Lancet Oncol. 2001, 2, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, N.; Ozturk, D.; Kavakli, I.H.; Okyar, A. Molecular Aspects of Circadian Pharmacology and Relevance for Cancer Chronotherapy. Int. J. Mol. Sci. 2017, 18, 2168. [Google Scholar] [CrossRef] [PubMed]
- Ramos, E.; Egea, J.; López-Muñoz, F.; Gil-Martín, E.; Romero, A. Therapeutic Potential of Melatonin Counteracting Chemotherapy-Induced Toxicity in Breast Cancer Patients: A Systematic Review. Pharmaceutics 2023, 15, 1616. [Google Scholar] [CrossRef]
- Zhou, J.; Wang, J.; Zhang, X.; Tang, Q. New Insights Into Cancer Chronotherapies. Front. Pharmacol. 2021, 12, 741295. [Google Scholar] [CrossRef]
- Wang, L.; Wang, C.; Choi, W.S. Use of Melatonin in Cancer Treatment: Where Are We? Int. J. Mol. Sci. 2022, 23, 3779. [Google Scholar] [CrossRef]



| Pathology | Effects of Melatonin | References |
|---|---|---|
| Lipid Metabolism | ↓ Dyslipidemia by ↓ levels of triglycerides and ↓ total cholesterol. Exogenous melatonin has secondary effects in ↓ Waist circumference ↓ BMI | [21,22] |
| Reproductive Health | ↓ GnRH release ↓ LH levels. ↓ Melatonin was associated with hypothalamic amenorrhea and precocious puberty. | [1] |
| Cardiovascular | ↓ Blood pressure | [7,23] |
| Energy Metabolism | ↑ Glucose tolerance ↑ Insulin sensitivity ↓ Body weight | [24] |
| Thermoregulation | ↓ Body temperature | [1] |
| Neurodegenerative Diseases and Dementia | ↑ Cognitive thinking ↑ Neurogenesis ↑ Anti-aging effects | [1,25,26] |
| Stroke | ↓ Infarction volume | [7] |
| Psychiatric Conditions | ↓ Melatonin in depression, anxiety, schizophrenia, and autism | [26] |
| Immunity | ↑ Anti-inflammatory cytokines ↓ Proinflammatory cytokine production (COX and iNOS) | [27,28] |
| Familial Syndrome | Gene | Inheritance Pattern | Function | References |
|---|---|---|---|---|
| Li–Fraumeni | p53 | AD | ↓ Cell growth ↓ Differentiation ↑ Cell apoptosis | [41,46,52,53,54] |
| Retinoblastoma | RB1 | AD | Cell cycle regulation | [43,46,54] |
| Bloom | BLM | AR | DNA helicase | [54] |
| Werner | WRN | AR | DNA helicase | [54] |
| Rothmund Thompson | RECQL4 | AR | RecQ helicase | [54] |
| Gene | Expression in OS | Function | References |
|---|---|---|---|
| PTEN | ↓ | ↓ Cell growth ↓ Differentiation ↑ Cell apoptosis | [52] |
| WWOX | ↓ | Tumor suppressor gene | [41,53,55] |
| SOX5 | ↑ | ↑ Transcription factor synthesis ↑EMT, invasion, and migration | [41] |
| CDKN2A | ↓ | Cyclin-dependant kinase | [41,56] |
| INK4A | ↓ | CDK4 Cell cycle | [57,58] |
| MDM2 | ↑ | Oncogene | [41,59] |
| c-Myc | ↑ | Oncogene | [41,60] |
| C-fos | ↑ | Protooncogene | [61] |
| RUNX2 | ↑ | Oncogenesis | [41,55] |
| Non-Coding RNA Type | Non-Coding RNA | Effect | References |
|---|---|---|---|
| miR | miR-101, miR-574–3P, mi-R-20a, mi-R-19a, miR-16, miR-140, miR-150, miR-29, miR-133a, miR26a, miR-29b-1, miR-200b, miR-181, miR-205, miR-424, miR-106, miR-519 | CSC formation and proliferation Activation of PI3K/Akt pathway Activation of JAK/STAT pathway Cell invasion ↓ IL-2 Lung metastasis | [41,63,64,65,66] |
| lncRNA | MALAT1, HOXD-AS1, TUG-1, LINC00161, SNHG16RO, NEAT1, SARCC, MIR17HG, OIP5, FENDRR | Tumor initiation Tumor proliferation Migration Invasion | |
| circRNA | hsa_circRNA_103801, hsa-miR-370-3p, hsa-miR-338-3p, hsa-miR-877-3p, CircTCF25, CircMMP9, Circ001621, CircEPSTI1, Circ0001658, Circ-LARP4 | Cell proliferation Hinder cell death Tumor invasion | [41,67] |
| Cytokine | Effect | References |
|---|---|---|
| IL-6 | ↑ Glycolytic metabolism in OS cells ↑ Lung metastasis ↑ MEK/ERK1/2/hypoxia-inducible transcription factor-1α (HIF-1α) | [52,102] |
| TNFα | ↑ Undifferentiated cells ↑ Neo-angiogenesis ↑ M2 macrophage recruitment | [52,100,101] |
| IL-34 | ↑ Neo-angiogenesis ↑ M2 macrophage recruitment | [52,101] |
| Malignancy | Effects | References |
|---|---|---|
| Neuron Malignancy | ↓ Neuroblastoma via ↓ VGEF | [113,119] |
| Breast Cancer | ↓ Risk of breast cancer ↓ CDK2, CDK4 ↓ IGFR ↓ HIF-1α ↓ VEGF ↑ miR-152-3p | [45,114,115,116,117,120] |
| Ovarian | ↓ Oxidative stress ↓ CDK2, CDK4 ↓ Risk of ovarian cancer ↓ Akt/ERK/JNK pathway ↓ NF-κB pathway | [114,116,118] |
| Lymphoproliferative Pathologies | Cell cycle arrest ↓ Bcl-2 Mitochondrial membrane depolarization Cytochrome c release activation of caspase-3 in lymphoproliferative disease. | [9,114] |
| Lung Cancer | ↑ Cancer cell migration and variability 2/2 ↑ JNK/MAPK pathway (6) | [114,121] |
| Renal Cancer | ↑ Bim → ↑ apoptosis | [122] |
| Gastric Cancer | ↓ RZR/RORγ → ↓ angiogenesis | [97] |
| Colon Cancer | ↑ Apoptosis ↓ TGF | [114,123] |
| Prostate | ↓ Cell growth of both androgen-dependent and androgen-independent prostate cancer ↑ miRNA3195 and miRNA374b | [124,125] |
| Treatment | Melatonin Concentration | Cell Type(s) | Effects in OS | References |
|---|---|---|---|---|
| Doxorubicin | 10 mg of the MLT-nanocarrier | Saos-2 MG-63 human bone marrow mesenchymal stem cell, (hBM-MSC) | Improved DOX efficacy in cancer treatment and reduced toxicity. | [161] |
| Melatonin/HPβCD inclusion complex-loaded chitosan scaffolds | 9 mM | MG-63 | Time-dependant ↑ Apoptosis | [138] |
| Methotrexate | 0.5 mmol/L 1 mmol/L 2 mmol/L 4 mmol/L 5 mmol/L | SaOS-2 | ↓ Cell activity ↑ Cells at G1 Cycle ↑ Apoptosis | [162] |
| Cisplatin-Methotrexate | ||||
| Cisplatin | 19.74 µg/mL 179.1 µg/mL 7.72 µg/mL | MG-63 | ↑ Sensitivity ↓ BCL2 ↓ miR-181b ↑ CYLD ↑ CBX-7 ↑ p53 ↑ Apoptosis | [163] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Ansari, N.; Samuel, S.M.; Büsselberg, D. Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations. Biomolecules 2024, 14, 145. https://doi.org/10.3390/biom14020145
Al-Ansari N, Samuel SM, Büsselberg D. Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations. Biomolecules. 2024; 14(2):145. https://doi.org/10.3390/biom14020145
Chicago/Turabian StyleAl-Ansari, Nojoud, Samson Mathews Samuel, and Dietrich Büsselberg. 2024. "Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations" Biomolecules 14, no. 2: 145. https://doi.org/10.3390/biom14020145
APA StyleAl-Ansari, N., Samuel, S. M., & Büsselberg, D. (2024). Unveiling the Protective Role of Melatonin in Osteosarcoma: Current Knowledge and Limitations. Biomolecules, 14(2), 145. https://doi.org/10.3390/biom14020145