Illuminating Clues of Cancer Buried in Prostate MR Image: Deep Learning and Expert Approaches

 , , ,
, , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
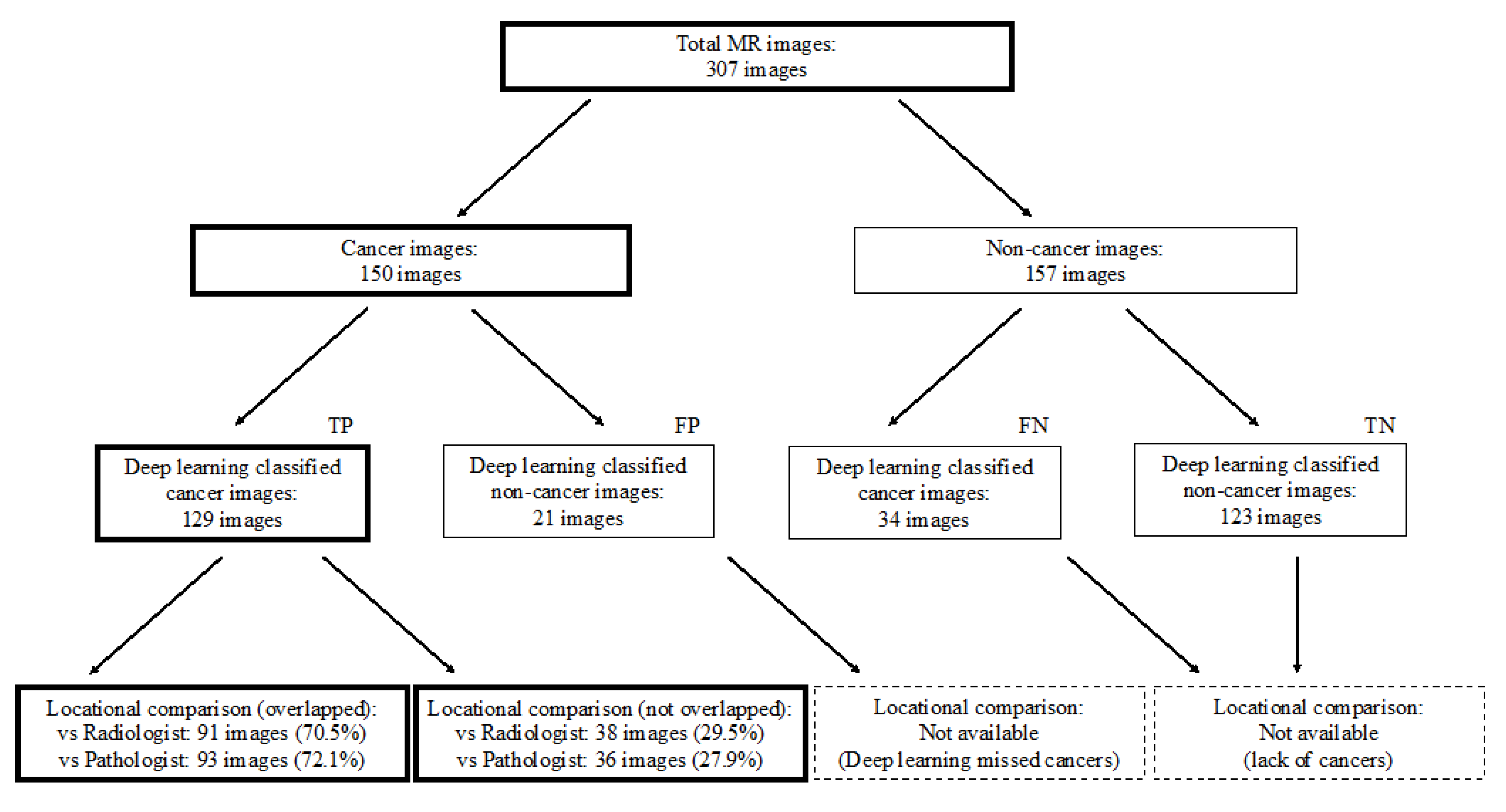
2.1. Outline of Study Design
2.2. Study Population
2.3. MR Image Preparation
2.4. MR Imaging Settings
2.5. Classification Using a Deep Neural Network (Preparation for an Explainable Deep Learning Model)
2.6. Clinicopathological Evaluations
2.7. Preparation of Pathology Images
2.8. Scoring on MR Images
2.9. Pathological Cancer Grading
2.10. Locational Comparison between Deep Learning-Focused Regions on MR Images and Expert-Identified Cancer Locations
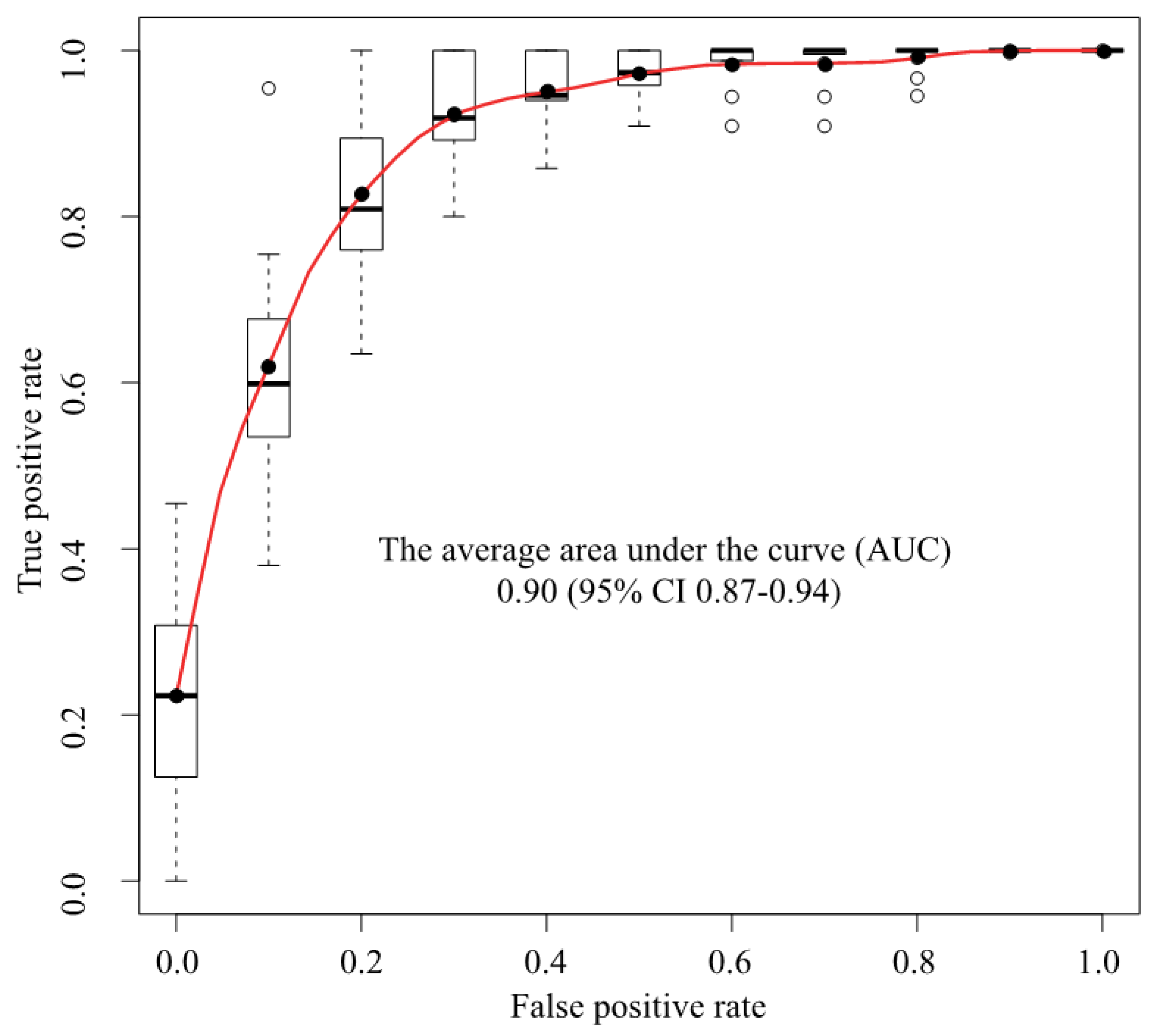
2.11. Statistical Analysis
3. Results
3.1. Image and Patient Characteristics
3.2. Classification Using a Deep Neural Network (Preparation for an Explainable Deep Learning Model)
3.3. Clinical Comparison of Cases Classified Using a Deep Neural Network
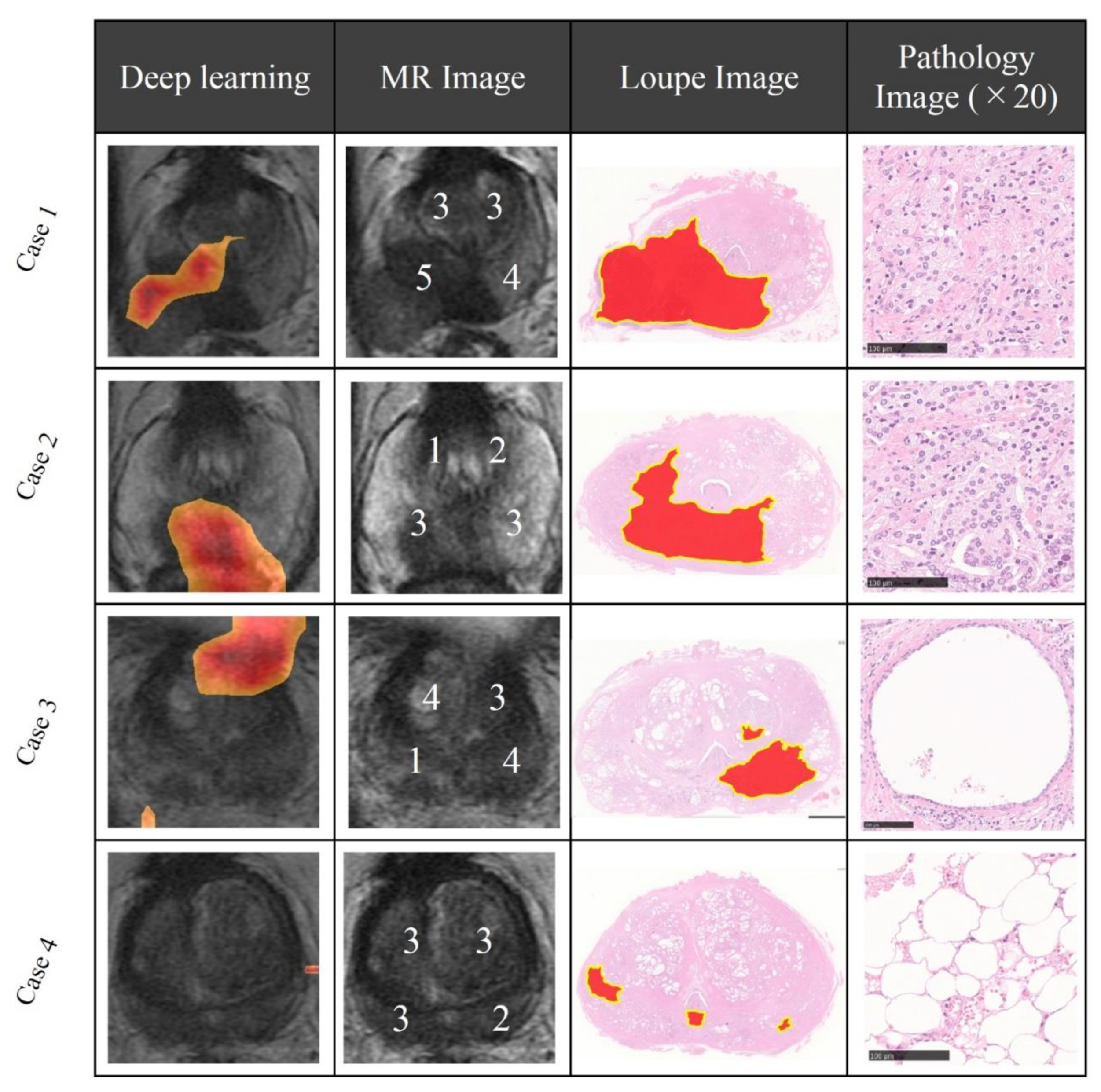
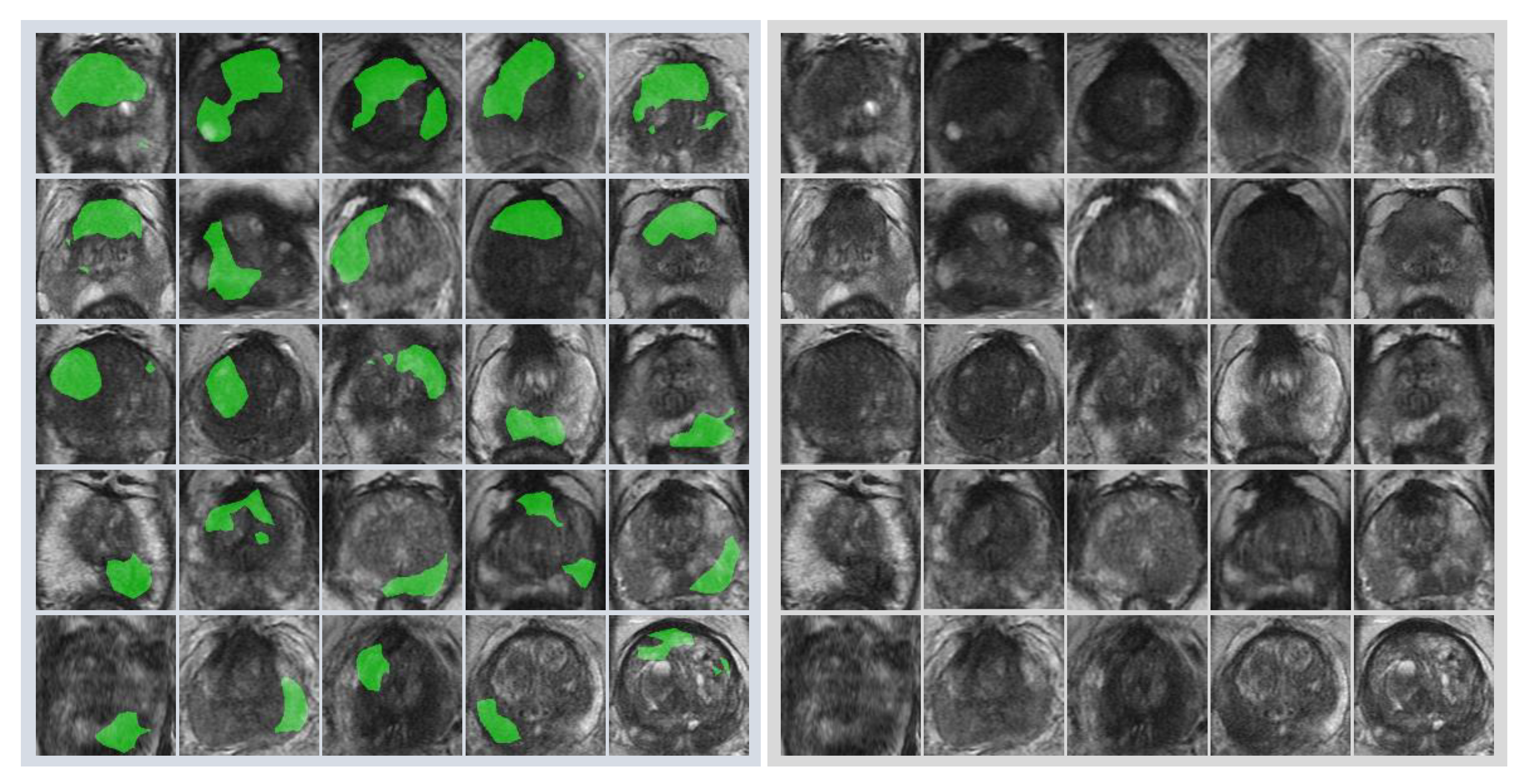
3.4. Locational Comparison between Deep Learning-Focused Regions on MR Images and Expert-Identified Cancer Locations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Walsh, S.L.F.; Calandriello, L.; Silva, M.; Sverzellati, N. Deep learning for classifying fibrotic lung disease on high-resolution computed tomography: a case-cohort study. Lancet Respir. Med. 2018, 6, 837–845. [Google Scholar] [CrossRef]
- De Fauw, J.; Ledsam, J.R.; Romera-Paredes, B.; Nikolov, S.; Tomasev, N.; Blackwell, S.; Askham, H.; Glorot, X.; O’Donoghue, B.; Visentin, D.; et al. Clinically applicable deep learning for diagnosis and referral in retinal disease. Nat. Med. 2018, 24, 1342–1350. [Google Scholar] [CrossRef] [PubMed]
- Bejnordi, B.E.; Veta, M.; Van Diest, P.J.; Van Ginneken, B.; Karssemeijer, N.; Litjens, G.; Van Der Laak, J.A.W.M.; Hermsen, M.; Manson, Q.F.; Balkenhol, M.; et al. Diagnostic Assessment of Deep Learning Algorithms for Detection of Lymph Node Metastases in Women with Breast Cancer. JAMA 2017, 318, 2199–2210. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Tsuzuki, T.; Akatsuka, J.; Ueki, M.; Morikawa, H.; Numata, Y.; Takahara, T.; Tsuyuki, T.; Shimizu, A.; Maeda, I.; et al. Automated acquisition of knowledge beyond pathologists. BioRxiv 2019, 539791. [Google Scholar]
- Group of Twenty. G20 AI Principles. Available online: https://g20.org/pdf/documents/en/annex_08.pdf (accessed on 6 September 2019).
- Mnih, V.; Heess, N.; Graves, A.; Kavukcuoglu, K. Recurrent Models of Visual Attention. Available online: https://arxiv.org/pdf/1406.6247 (accessed on 24 October 2019).
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-CAM: Visual Explanations from Deep Networks via Gradient-Based Localization. IEEE Int. Conf. on Comput. Vis. 2017, 618–626. [Google Scholar]
- Chattopadhyay, A.; Sarkar, A.; Howlader, P.; Balasubramanian, V.N. Grad-CAM++: Improved Visual Explanations for Deep Convolutional Networks. Available online: https://arxiv.org/abs/1710.11063 (accessed on 25 September 2019).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef]
- Arnold, M.; Karim-Kos, H.E.; Coebergh, J.W.; Byrnes, G.; Antilla, A.; Ferlay, J.; Renehan, A.G.; Forman, D.; Soerjomataram, I. Recent trends in incidence of five common cancers in 26 European countries since 1988: Analysis of the European Cancer Observatory. Eur. J. Cancer 2015, 51, 1164–1187. [Google Scholar] [CrossRef]
- Wang, X.; Yang, W.; Weinreb, J.; Han, J.; Li, Q.; Kong, X.; Yan, Y.; Ke, Z.; Luo, B.; Liu, T.; et al. Searching for prostate cancer by fully automated magnetic resonance imaging classification: deep learning versus non-deep learning. Sci. Rep. 2017, 7, 15415. [Google Scholar] [CrossRef]
- Ishioka, J.; Matsuoka, Y.; Uehara, S.; Yasuda, Y.; Kijima, T.; Yoshida, S.; Yokoyama, M.; Saito, K.; Kihara, K.; Numao, N.; et al. Computer-aided diagnosis of prostate cancer on magnetic resonance imaging using a convolutional neural network algorithm. BJU Int. 2018, 122, 411–417. [Google Scholar] [CrossRef]
- Ullrich, T.; Quentin, M.; Oelers, C.; Dietzel, F.; Sawicki, L.; Arsov, C.; Rabenalt, R.; Albers, P.; Antoch, G.; Blondin, D.; et al. Magnetic resonance imaging of the prostate at 1.5 versus 3.0 T: A prospective comparison study of image quality. Eur. J. Radiol. 2017, 90, 192–197. [Google Scholar] [CrossRef] [PubMed]
- Chollet, F. Xception: Deep Learning with Depthwise Separable Convolutions. In Proceedings of the 2017 IEEE Conference on Computer Vision and Pattern Recognition (CVPR), Honolulu, HI, USA, 21–26 July 2017; pp. 1800–1807. [Google Scholar]
- Szegedy, C.; Vanhoucke, V.; Ioffe, S.; Shlens, J.; Wojna, Z. Rethinking the Inception Architecture for Computer Vision. Available online: https://arxiv.org/abs/1512.00567 (accessed on 25 September 2019).
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. Available online: https://arxiv.org/abs/1409.1556 (accessed on 25 September 2019).
- Stone, M. Cross-Validatory Choice and Assessment of Statistical Predictions. J. R. Stat. Soc. Ser. B Methodol. 1974, 36, 111–133. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J. The Elements of Statistical Learning: Data Mining, Inference, and Prediction, 2nd ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Ledell, E.; Petersen, M.; Van Der Laan, M. Computationally efficient confidence intervals for cross-validated area under the ROC curve estimates. Electron. J. Stat. 2015, 9, 1583–1607. [Google Scholar] [CrossRef]
- Pirracchio, R.; Petersen, M.L.; Carone, M.; Rigon, M.R.; Chevret, S.; van der Laan, M.J. Mortality prediction in intensive care units with the Super ICU Learner Algorithm (SICULA): A population-based study. Lancet Respir Med. 2015, 3, 42–52. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Epstein, J.I.; Allsbrook, W.C., Jr.; Amin, M.B.; Egevad, L.L.; Committee, I.G. The 2005 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2005, 29, 1228–1242. [Google Scholar] [CrossRef]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Blank, K.; Broderick, G.A.; Schultz, D.; Tomaszewski, J.E.; Kaplan, I.; Beard, C.J.; Wein, A.; et al. Five years biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. Int. J. Radiat. Oncol. 1998, 42, 301. [Google Scholar] [CrossRef]
- Orczyk, C.; Villers, A.; Rusinek, H.; Lepennec, V.; Bazille, C.; Giganti, F.; Mikheev, A.; Bernaudin, M.; Emberton, M.; Fohlen, A.; et al. Prostate cancer heterogeneity: texture analysis score based on multiple magnetic resonance imaging sequences for detection, stratification and selection of lesions at time of biopsy. BJU Int. 2019, 124, 76–86. [Google Scholar] [CrossRef]
- Wang, L.; Mazaheri, Y.; Zhang, J.; Ishill, N.M.; Kuroiwa, K.; Hricak, H. Assessment of Biologic Aggressiveness of Prostate Cancer: Correlation of MR Signal Intensity with Gleason Grade after Radical Prostatectomy. Radiology 2008, 246, 168–176. [Google Scholar] [CrossRef]
- Cai, T.; Santi, R.; Tamanini, I.; Galli, I.C.; Perletti, G.; Johansen, T.E.B.; Nesi, G.; Johansen, T.B. Current Knowledge of the Potential Links between Inflammation and Prostate Cancer. Int. J. Mol. Sci. 2019, 20, 3833. [Google Scholar] [CrossRef] [PubMed]
- Miyai, K.; Mikoshi, A.; Hamabe, F.; Nakanishi, K.; Ito, K.; Tsuda, H.; Shinmoto, H. Histological differences in cancer cells, stroma, and luminal spaces strongly correlate with in vivo MRI-detectability of prostate cancer. Mod. Pathol. 2019, 32, 1536–1543. [Google Scholar] [CrossRef] [PubMed]
- Hinton, G.E.; Srivastava, N.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R.R. Improving neural networks by preventing co-adaptation of feature detectors. arXiv preprint 2012, arXiv:1207.0580. Available online: https://arxiv.org/abs/1207.0580 (accessed on 25 September 2019).
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. ImageNet Classification with Deep Convolutional Neural, NIPS’12. In Proceedings of the 25th International Conference on Neural Information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012; Volume 1, pp. 1097–1105. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Cases: N = 105 | Cancer Cases | Non-Cancer Cases | p Value |
|---|---|---|---|
| Number of cases, n | 54 | 51 | - |
| Age, year, mean ± SD | 67.4 ± 6.9 | 65.2 ± 8.6 | 0.09 |
| PSA, ng/mL, mean ± SD | 14.7 ± 12.1 | 8.1 ± 5.4 | <0.001 |
| TPV, mL, mean ± SD | 27.5 ± 10.6 | 42.5 ± 19.3 | <0.001 |
| PSAD, ng/mL/cm3, mean ± SD | 0.63 ± 0.66 | 0.22 ± 0.16 | <0.001 |
| Cancer Cases: N = 54 | Classified Cases | Misclassified Cases | Univariate (p Value) |
|---|---|---|---|
| Number of cases, (%) | 92.6 | 7.4 | |
| Age, years, mean ± SD | 67.4 ± 6.9 | 67.5 ± 7.3 | 0.96 |
| PSA, ng/mL, mean ± SD | 14.2 ± 11.9 | 21.6 ± 13.5 | 0.07 |
| TPV, mL, mean ± SD | 27.9 ± 10.7 | 23.0 ± 10.2 | 0.66 |
| PSAD, ng/mL/cm3, mean ± SD | 0.59 ± 0.64 | 1.17 ± 0.85 | 0.07 |
| Gleason score, (%) | 0.03 | ||
| <8 | 60.0 | 0.0 | |
| ≥8 | 40.0 | 100.0 | |
| Clinical stage, (%) | 0.21 | ||
| ≤T2 | 80.0 | 50.0 | |
| ≥T3 | 20.0 | 50.0 | |
| Pathological stage, (%) | 0.63 | ||
| ≤T2 | 44.0 | 25.0 | |
| ≥T3 | 56.0 | 75.0 | |
| WBC, 103/μL, mean ± SD | 6074 ± 1248 | 5150 ± 656 | 0.12 |
| Hb, g/dl, mean ± SD | 14.5 ± 1.2 | 13.8 ± 0.7 | 0.08 |
| Plt, 103/μL, mean ± SD | 21.8 ± 5.0 | 18.3 ± 2.5 | 0.14 |
| LDH, U/L, mean ± SD | 180 ± 34.9 | 179 ± 45.4 | 0.93 |
| ALP, U/L, mean ± SD | 208 ± 56 | 249 ± 161 | 0.75 |
| Ca, mg/dL, mean ± SD | 9.3 ± 0.43 | 9.1 ± 0.26 | 0.29 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akatsuka, J.; Yamamoto, Y.; Sekine, T.; Numata, Y.; Morikawa, H.; Tsutsumi, K.; Yanagi, M.; Endo, Y.; Takeda, H.; Hayashi, T.; et al. Illuminating Clues of Cancer Buried in Prostate MR Image: Deep Learning and Expert Approaches. Biomolecules 2019, 9, 673. https://doi.org/10.3390/biom9110673
Akatsuka J, Yamamoto Y, Sekine T, Numata Y, Morikawa H, Tsutsumi K, Yanagi M, Endo Y, Takeda H, Hayashi T, et al. Illuminating Clues of Cancer Buried in Prostate MR Image: Deep Learning and Expert Approaches. Biomolecules. 2019; 9(11):673. https://doi.org/10.3390/biom9110673
Chicago/Turabian StyleAkatsuka, Jun, Yoichiro Yamamoto, Tetsuro Sekine, Yasushi Numata, Hiromu Morikawa, Kotaro Tsutsumi, Masato Yanagi, Yuki Endo, Hayato Takeda, Tatsuro Hayashi, and et al. 2019. "Illuminating Clues of Cancer Buried in Prostate MR Image: Deep Learning and Expert Approaches" Biomolecules 9, no. 11: 673. https://doi.org/10.3390/biom9110673
APA StyleAkatsuka, J., Yamamoto, Y., Sekine, T., Numata, Y., Morikawa, H., Tsutsumi, K., Yanagi, M., Endo, Y., Takeda, H., Hayashi, T., Ueki, M., Tamiya, G., Maeda, I., Fukumoto, M., Shimizu, A., Tsuzuki, T., Kimura, G., & Kondo, Y. (2019). Illuminating Clues of Cancer Buried in Prostate MR Image: Deep Learning and Expert Approaches. Biomolecules, 9(11), 673. https://doi.org/10.3390/biom9110673