
Comparison of Different Green Space Measures and Their Impact on Dementia Cases in South Korea: A Spatial Panel Analysis


Abstract
1. Introduction
2. Materials and Methods
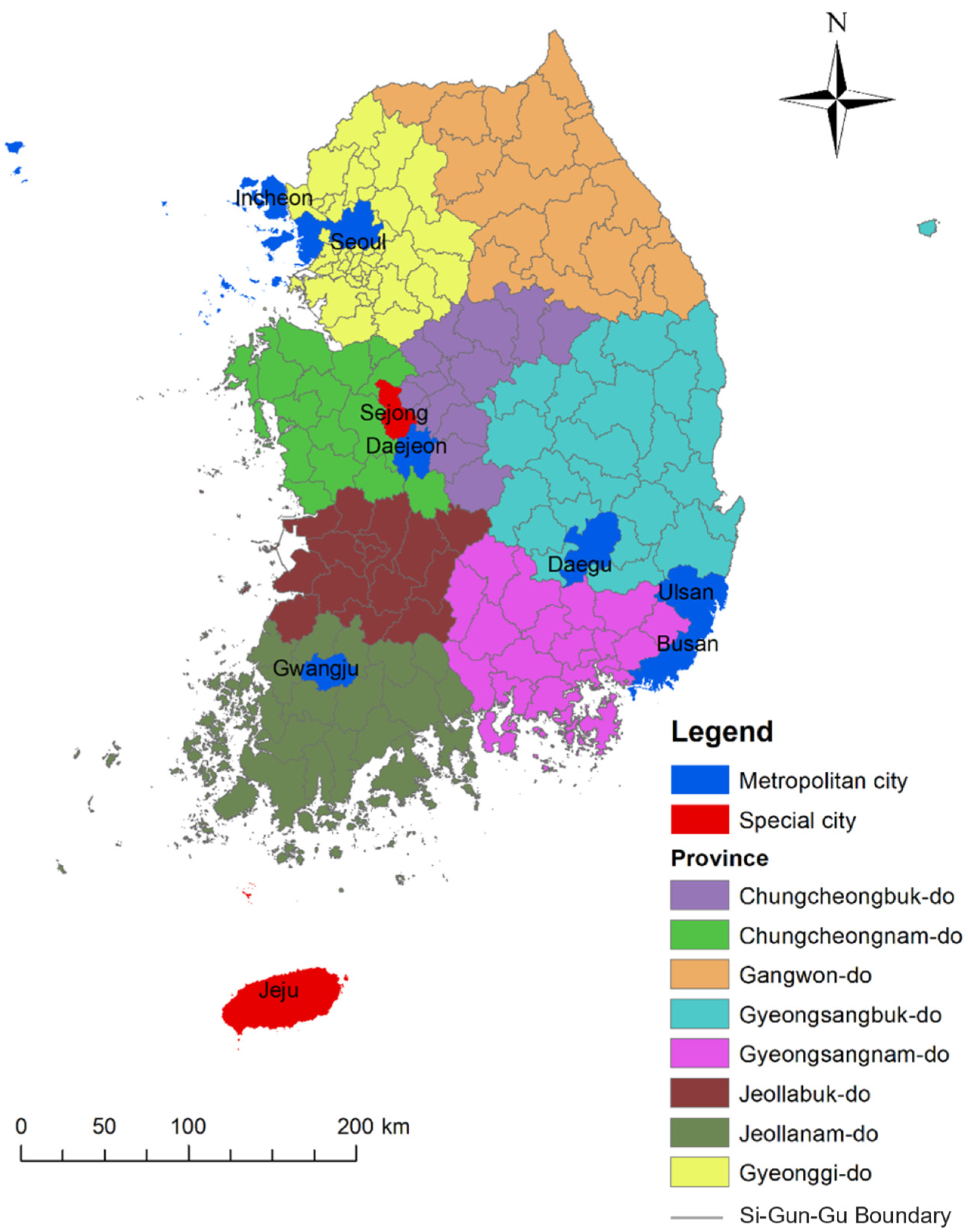
2.1. Study Area
2.2. Data Collection
Greenspace Measures
2.3. Analysis
2.3.1. Panel Model Estimation
2.3.2. Spatial Autocorrelation
2.3.3. Spatial Panel Regression
3. Results
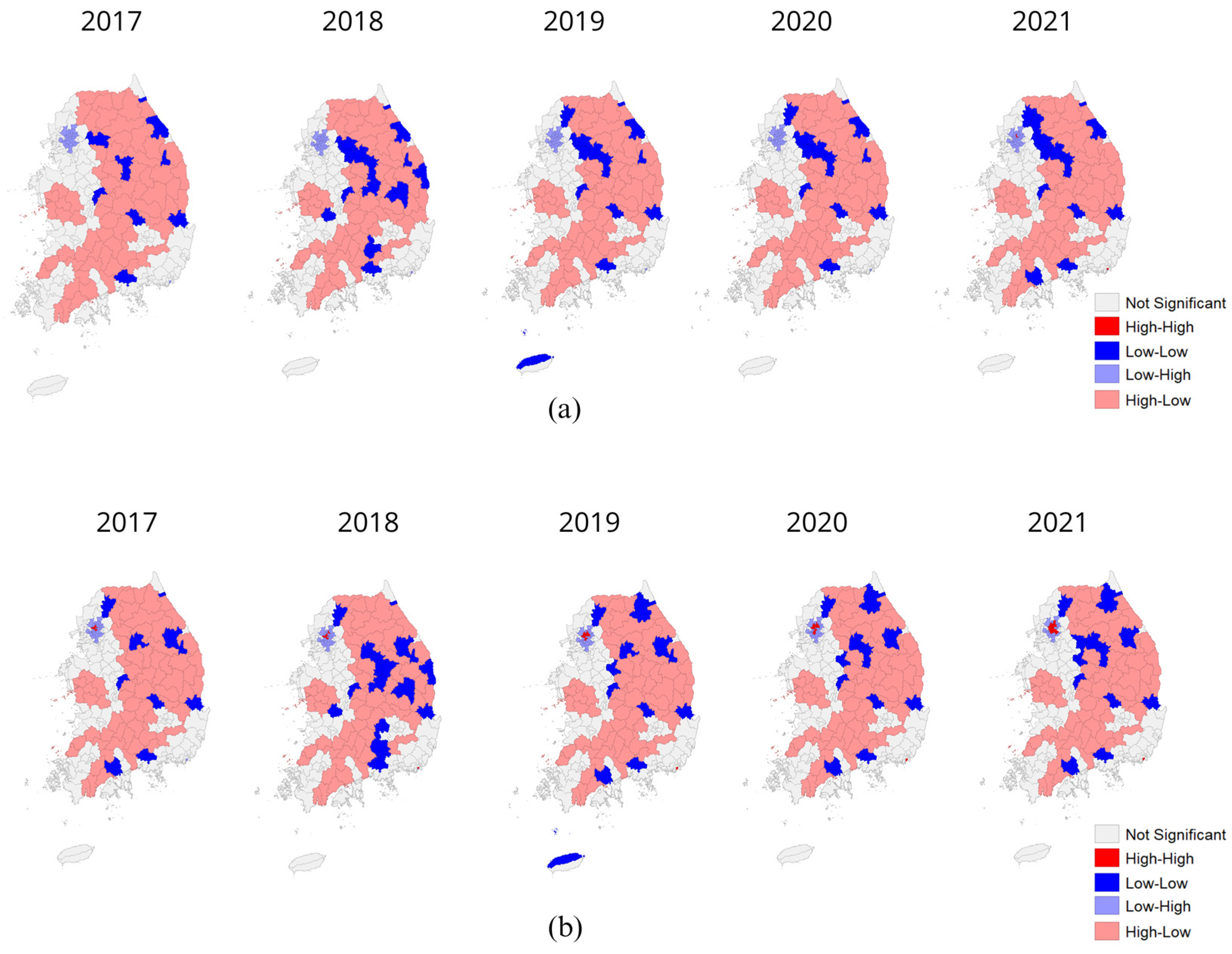
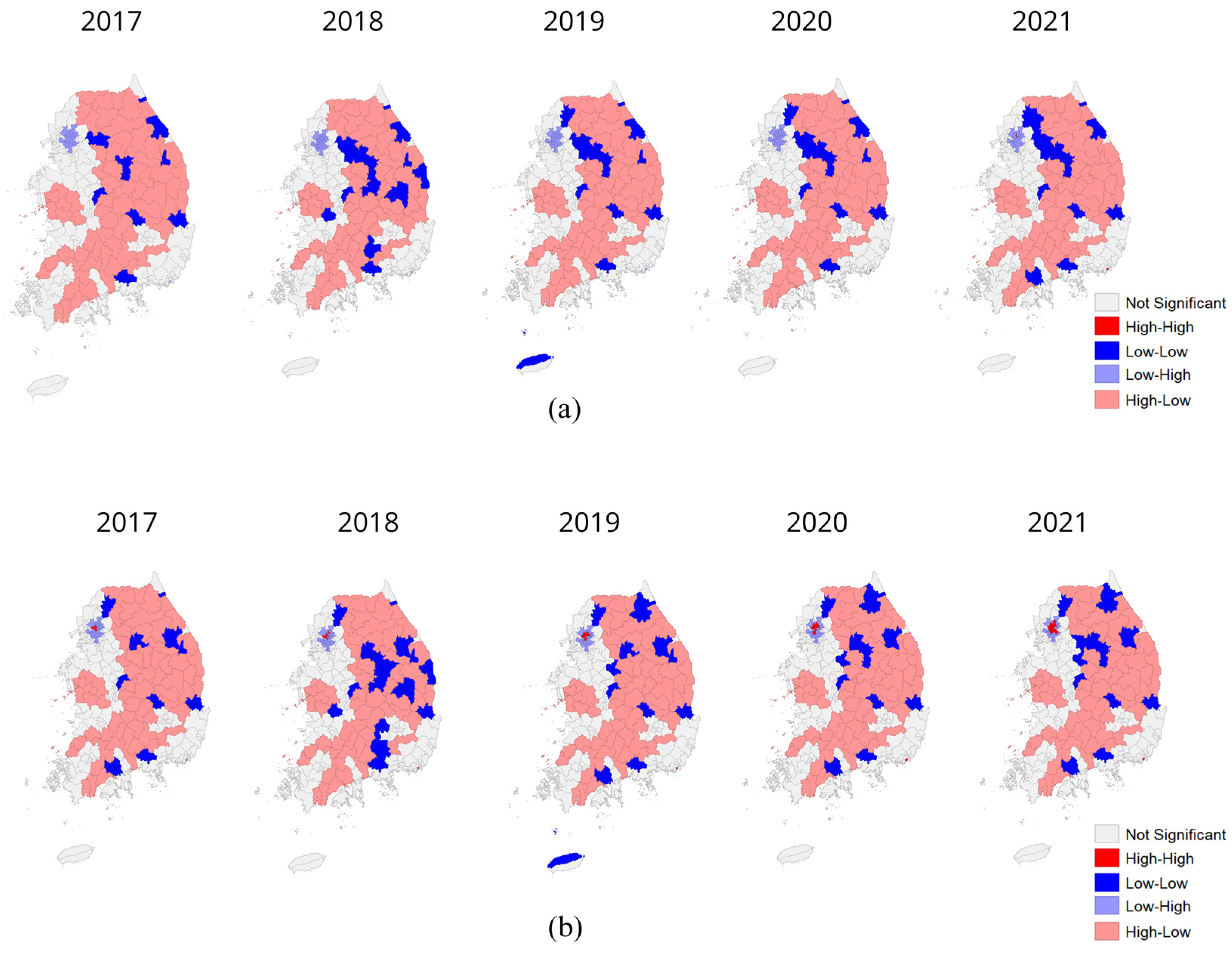
3.1. Spatial Autocorrelation
3.2. Panel Regression
3.3. Spatial Panel Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Van Der Flier, W.M.; Scheltens, P. Epidemiology and Risk Factors of Dementia. J. Neurol. Neurosurg. Psychiatry 2005, 76, V2–V7. [Google Scholar] [CrossRef] [PubMed]
- Dhana, K.; Evans, D.A.; Rajan, K.B.; Bennett, D.A.; Morris, M.C. Healthy Lifestyle and the Risk of Alzheimer Dementia: Findings from 2 Longitudinal Studies. Neurology 2020, 95, e374–e383. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Park, J.-H. Predictive Model of Regional Dementia Prevalence Using Geographic Weighted Regression Analysis. J. Pers. Med. 2022, 12, 1388. [Google Scholar] [CrossRef] [PubMed]
- Besser, L. Outdoor Green Space Exposure and Brain Health Measures Related to Alzheimer’s Disease: A Rapid Review. BMJ Open 2021, 11, e043456. [Google Scholar] [CrossRef] [PubMed]
- Shon, C.; Yoon, H. Health-Economic Burden of Dementia in South Korea. BMC Geriatr. 2021, 21, 54. [Google Scholar] [CrossRef] [PubMed]
- Zagnoli, F.; Filippini, T.; Jimenez, M.P.; Wise, L.A.; Hatch, E.E.; Vinceti, M. Is Greenness Associated with Dementia? A Systematic Review and Dose–Response Meta-Analysis. Curr. Environ. Health Rep. 2022, 9, 574–590. [Google Scholar] [CrossRef] [PubMed]
- Astell-Burt, T.; Navakatikyan, M.A.; Feng, X. Urban Green Space, Tree Canopy and 11-Year Risk of Dementia in a Cohort of 109,688 Australians. Environ. Int. 2020, 145, 106102. [Google Scholar] [CrossRef]
- Rodriguez-Loureiro, L.; Gadeyne, S.; Bauwelinck, M.; Lefebvre, W.; Vanpoucke, C.; Casas, L. Long-Term Exposure to Residential Greenness and Neurodegenerative Disease Mortality among Older Adults: A 13-Year Follow-up Cohort Study. Environ. Health A Glob. Access Sci. Source 2022, 21, 49. [Google Scholar] [CrossRef]
- Hu, H.Y.; Ma, Y.H.; Deng, Y.T.; Ou, Y.N.; Cheng, W.; Feng, J.F.; Tan, L.; Yu, J.T. Residential Greenness and Risk of Incident Dementia: A Prospective Study of 375,342 Participants. Environ. Res. 2023, 216, 114703. [Google Scholar] [CrossRef]
- Browning, M.; Lee, K. Within What Distance Does “Greenness” Best Predict Physical Health? A Systematic Review of Articles with Gis Buffer Analyses across the Lifespan. Int. J. Environ. Res. Public Health 2017, 14, 675. [Google Scholar] [CrossRef]
- Dhana, K.; Franco, O.H.; Ritz, E.M.; Ford, C.N.; Desai, P.; Krueger, K.R.; Holland, T.M.; Dhana, A.; Liu, X.; Aggarwal, N.T.; et al. Healthy Lifestyle and Life Expectancy with and without Alzheimer’s Dementia: Population Based Cohort Study. BMJ 2022, 377, e068390. [Google Scholar] [CrossRef] [PubMed]
- Younan, D.; Wang, X.; Millstein, J.; Petkus, A.J.; Beavers, D.P.; Espeland, M.A.; Chui, H.C.; Resnick, S.M.; Gatz, M.; Kaufman, J.D.; et al. Air Quality Improvement and Cognitive Decline in Community-Dwelling Older Women in the United States: A Longitudinal Cohort Study. PLoS Med. 2022, 19, e1003893. [Google Scholar] [CrossRef] [PubMed]
- Mmako, N.J.; Courtney-Pratt, H.; Marsh, P. Green Spaces, Dementia and a Meaningful Life in the Community: A Mixed Studies Review. Health Place 2020, 63, 102344. [Google Scholar] [CrossRef]
- Choi, H.G.; Kim, J.H.; Kim, J.H.; Kim, E.S.; Park, H.Y.; Min, K.W.; Kwon, M.J. Associations between Proton Pump Inhibitors and Alzheimer’s Disease: A Nested Case–Control Study Using a Korean Nationwide Health Screening Cohort. Alzheimer’s Res. Ther. 2022, 14, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. Spatial and Socioeconomic Inequalities in Accessibility to Healthcare Services in South Korea. Healthcare 2022, 10, 2049. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kwon, L.; Lim, H.; Chun, H. Gender-Based Analysis of Risk Factors for Dementia Using Senior Cohort. Int. J. Environ. Res. Public Health 2020, 17, 7274. [Google Scholar] [CrossRef]
- Sun, H.; Wang, A.; He, S. Temporal and Spatial Analysis of Alzheimer’s Disease Based on an Improved Convolutional Neural Network and a Resting-State FMRI Brain Functional Network. Int. J. Environ. Res. Public Health 2022, 19, 4508. [Google Scholar] [CrossRef] [PubMed]
- Firouraghi, N.; Kiani, B.; Jafari, H.T.; Learnihan, V.; Salinas-Perez, J.A.; Raeesi, A.; Furst, M.A.; Salvador-Carulla, L.; Bagheri, N. The Role of Geographic Information System and Global Positioning System in Dementia Care and Research: A Scoping Review. Int. J. Health Geogr. 2022, 21, 8. [Google Scholar] [CrossRef] [PubMed]
- Scerpella, D.L.; Adam, A.; Marx, K.; Gitlin, L.N. Implications of Geographic Information Systems (GIS) for Targeted Recruitment of Older Adults with Dementia and Their Caregivers in the Community: A Retrospective Analysis. Contemp. Clin. Trials Commun. 2019, 14, 100338. [Google Scholar] [CrossRef]
- Su, C.; Lee, K.; Yen, C.; Wu, L.; Huang, C.; Lu, M. Use of Spatial Panel-Data Models to Investigate Factors Related to Incidence of End-Stage Renal Disease: A Nationwide Longitudinal Study in Taiwan. BMC Public Health. 2023, 23, 247. [Google Scholar] [CrossRef]
- Lee, K.; Browning, M.H.E.M.; Park, Y.M. Spatiotemporal Non-Stationarity in Green Space and Stress Relationships: Recent Evidence from South Korea. Environ. Res. 2023, 220, 115214. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, J.A.; Michael, Y.L.; Moore, K.A.; Melly, S.; Hughes, T.M.; Hayden, K.; Luchsinger, J.A.; Jimenez, M.P.; James, P.; Besser, L.M.; et al. Longitudinal Neighbourhood Determinants with Cognitive Health and Dementia Disparities: Protocol of the Multi-Ethnic Study of Atherosclerosis Neighborhoods and Aging Prospective Cohort Study. BMJ Open 2022, 12, e066971. [Google Scholar] [CrossRef] [PubMed]
- Glaser, S.; Jung, R.C.; Schweikert, K. Spatial Panel Count Data: Modeling and Forecasting of Urban Crimes. J. Spat. Econom. 2022, 3, 2. [Google Scholar] [CrossRef]
- Eom, T.H.; Lee, S.H.; Xu, H. Introduction to Panel Data Analysis. In Handbook of Research Methods in Public Administration, 2nd ed.; Miller, G.J., Brandler, S., Roman, C.P., Yang, K., Eds.; CRC Press: Boca Raton, FL, USA, 2007; pp. 571–590. ISBN 978-042-924-549-7. [Google Scholar]
- Greene, W.H. Econometric Analysis, 4th ed.; Prentice Hall: New York, NY, USA, 2000. [Google Scholar]
- Salima, B.A.; Julie, L.G.; Lionel, V. Spatial Econometrics on Panel Data. In Handbook of Spatial Analysis: Theory and Practical Application with R; Institut National de la Statistique et des Études Économiques: Paris, France, 2018; pp. 179–203. [Google Scholar]
- Paul, L.A.; Hystad, P.; Burnett, R.T.; Kwong, J.C.; Crouse, D.L.; van Donkelaar, A.; Tu, K.; Lavigne, E.; Copes, R.; Martin, R.V.; et al. Urban Green Space and the Risks of Dementia and Stroke. Environ. Res. 2020, 186, 109520. [Google Scholar] [CrossRef]
- Bagheri, N.; Wangdi, K.; Cherbuin, N.; Anstey, K.J. Combining Geospatial Analysis With Dementia Risk Utilising General Practice Data: A Systematic Review. J. Prev. Alzheimer’s Dis. 2017, 5, 71–77. [Google Scholar] [CrossRef]
- Slawsky, E.D.; Hajat, A.; Rhew, I.C.; Russette, H.; Semmens, E.O.; Kaufman, J.D.; Leary, C.S.; Fitzpatrick, A.L. Neighborhood Greenspace Exposure as a Protective Factor in Dementia Risk among US Adults 75 Years or Older: A Cohort Study. Environ. Health 2022, 21, 14. [Google Scholar] [CrossRef] [PubMed]
- de la Iglesia Martinez, A.; Labib, S.M. Demystifying Normalized Difference Vegetation Index (NDVI) for Greenness Exposure Assessments and Policy Interventions in Urban Greening. Environ. Res. 2023, 220, 115155. [Google Scholar] [CrossRef]
- Elhorst, J.P. The Dynamic General Nesting Spatial Econometric Model for Spatial Panels with Common Factors: Further Raising the Bar. Rev. Reg. Res. 2022, 42, 249–267. [Google Scholar] [CrossRef]
- Jung, I. Explaining the Development and Adoption of Social Policy in Korea: The Case of the National Basic Livelihood Security Act. Heal. Soc. Welf. Rev. 2009, 29, 44–68. [Google Scholar] [CrossRef]
- Lu, M.; Chen, J.; Tang, H.; Rao, Y.; Yang, P.; Wu, W. Land Cover Change Detection by Integrating Object-Based Data Blending Model of Landsat and MODIS. Remote Sens. Environ. 2016, 184, 374–386. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Z.; Liao, H.; Li, C. Improving the Performance of GIS Polygon Overlay Computation with MapReduce for Spatial Big Data Processing. Clust. Comput. 2015, 18, 507–516. [Google Scholar] [CrossRef]
- Copeland, K.A.F. Applied Linear Statistical Models. J. Qual. Technol. 1997, 29, 233. [Google Scholar] [CrossRef]
- Croissant, Y.; Millo, G. Panel Data Econometrics in R: The Plm Package. J. Stat. Softw. 2008, 27, 1–43. [Google Scholar] [CrossRef]
- Feng, Y.; Wang, X.; Du, W.; Wu, H.; Wang, J. Effects of Environmental Regulation and FDI on Urban Innovation in China: A Spatial Durbin Econometric Analysis. J. Clean. Prod. 2019, 235, 210–224. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, S.; Zhang, W.; Zhan, D.; Li, J. Does Foreign Direct Investment Affect Environmental Pollution in China’s Cities? A Spatial Econometric Perspective. Sci. Total Environ. 2018, 613, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Tamamadin, M.; Lee, C.; Kee, S.H.; Yee, J.J. Regional Typhoon Track Prediction Using Ensemble K-Nearest Neighbor Machine Learning in the GIS Environment. Remote Sens. 2022, 14, 5292. [Google Scholar] [CrossRef]
- Xu, P.; Zhao, X.; Li, H.; Guo, S. Spatial Effect Analysis of Health Expenditure and Health Output in China From 2011 to 2018. Front. Public Health 2022, 10, 794177. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Shao, S.; Tian, Z.; Xie, Z.; Yin, P. Impacts of Air Pollution and Its Spatial Spillover Effect on Public Health Based on China’s Big Data Sample. J. Clean. Prod. 2017, 142, 915–925. [Google Scholar] [CrossRef]
- Elhorst, J.P. Specification and Estimation of Spatial Panel Data Models. Int. Reg. Sci. Rev. 2003, 26, 244–268. [Google Scholar] [CrossRef]
- Millo, G.; Piras, G. Splm: Spatial Panel Data Models in R. J. Stat. Softw. 2012, 47, 1–38. [Google Scholar] [CrossRef]
- Lee, K. Association between depression and green space before and after the COVID-19: Panel data evidence in South Korea. J. Korean Soc. Surv. Geod. Photogramm. Cartogr. 2022, 40, 459–467. [Google Scholar] [CrossRef]
- Wakefield, J.; Lyons, H. Spatial Aggregation and the Ecological Fallacy. In Handbook of Spatial Statistics, 1st ed.; Gelfand, A.E., Diggle, P., Guttorp, P., Fuentes, M., Eds.; CRC Press: Boca Raton, FL, USA, 2010; pp. 541–558. ISBN 978-042-913-650-4. [Google Scholar]
- Byeon, G.; Kwon, S.O.; Jhoo, J.; Jang, J.-W.; Kim, Y. Dementia Incidence Rate Before and After Implementing the National Responsibility Policy for Dementia Care in Patients With Vascular Risk Factors in Korea. Dement. Neurocognitive Disord. 2023, 22, 49. [Google Scholar] [CrossRef] [PubMed]
- Gascon, M.; Cirach, M.; Martínez, D.; Dadvand, P.; Valentín, A.; Plasència, A.; Nieuwenhuijsen, M.J. Normalized Difference Vegetation Index (NDVI) as a Marker of Surrounding Greenness in Epidemiological Studies: The Case of Barcelona City. Urban For. Urban Green. 2016, 19, 88–94. [Google Scholar] [CrossRef]
- Barboza, E.P.; Cirach, M.; Khomenko, S.; Iungman, T.; Mueller, N.; Barrera-Gómez, J.; Rojas-Rueda, D.; Kondo, M.; Nieuwenhuijsen, M. Green Space and Mortality in European Cities: A Health Impact Assessment Study. Lancet Planet. Health 2021, 5, e718–e730. [Google Scholar] [CrossRef]
- Jimenez, R.B.; Lane, K.J.; Hutyra, L.R.; Fabian, M.P. Spatial Resolution of Normalized Difference Vegetation Index and Greenness Exposure Misclassification in an Urban Cohort. J. Expo. Sci. Environ. Epidemiol. 2022, 32, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Vilcins, D.; Sly, P.D.; Scarth, P.; Mavoa, S. Green Space in Health Research: An Overview of Common Indicators of Greenness. Rev. Environ. Health 2022. [Google Scholar] [CrossRef] [PubMed]
- Kyoung, D.-S.; Lee, J.; Nam, H.; Park, M.H. Dementia and COVID-19 Mortality in South Korea. Dement. Neurocognitive Disord. 2021, 20, 38. [Google Scholar] [CrossRef]
- Chen, Z.C.; Liu, S.; Gan, J.; Ma, L.; Du, X.; Zhu, H.; Han, J.; Xu, J.; Wu, H.; Fei, M.; et al. The Impact of the COVID-19 Pandemic and Lockdown on Mild Cognitive Impairment, Alzheimer’s Disease and Dementia With Lewy Bodies in China: A 1-Year Follow-Up Study. Front. Psychiatry 2021, 12, 711658. [Google Scholar] [CrossRef]
- Axenhus, M.; Schedin-Weiss, S.; Tjernberg, L.; Wimo, A.; Eriksdotter, M.; Bucht, G.; Winblad, B. Changes in Dementia Diagnoses in Sweden during the COVID-19 Pandemic. BMC Geriatr. 2022, 22, 365. [Google Scholar] [CrossRef]
- Gaigher, J.M.; Lacerda, I.B.; Dourado, M.C.N. Dementia and Mental Health During the COVID-19 Pandemic: A Systematic Review. Front. Psychiatry 2022, 13, 879598. [Google Scholar] [CrossRef]
- Choi, Y.J.; Kim, S.; Hwang, Y.J.; Kim, C. Prevalence of Dementia in Korea Based on Hospital Utilization Data from 2008 to 2016. Yonsei Med. J. 2021, 62, 948–953. [Google Scholar] [CrossRef] [PubMed]
- Seong, S.J.; Kim, B.N.; Kim, K.W. Comparative Analysis on the Policy Approaches in the National Dementia Plans of G7 Countries and Korea and Their Implementation. J. Korean Med. Sci. 2023, 38, e227. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean | SD | Min | Max |
|---|---|---|---|---|
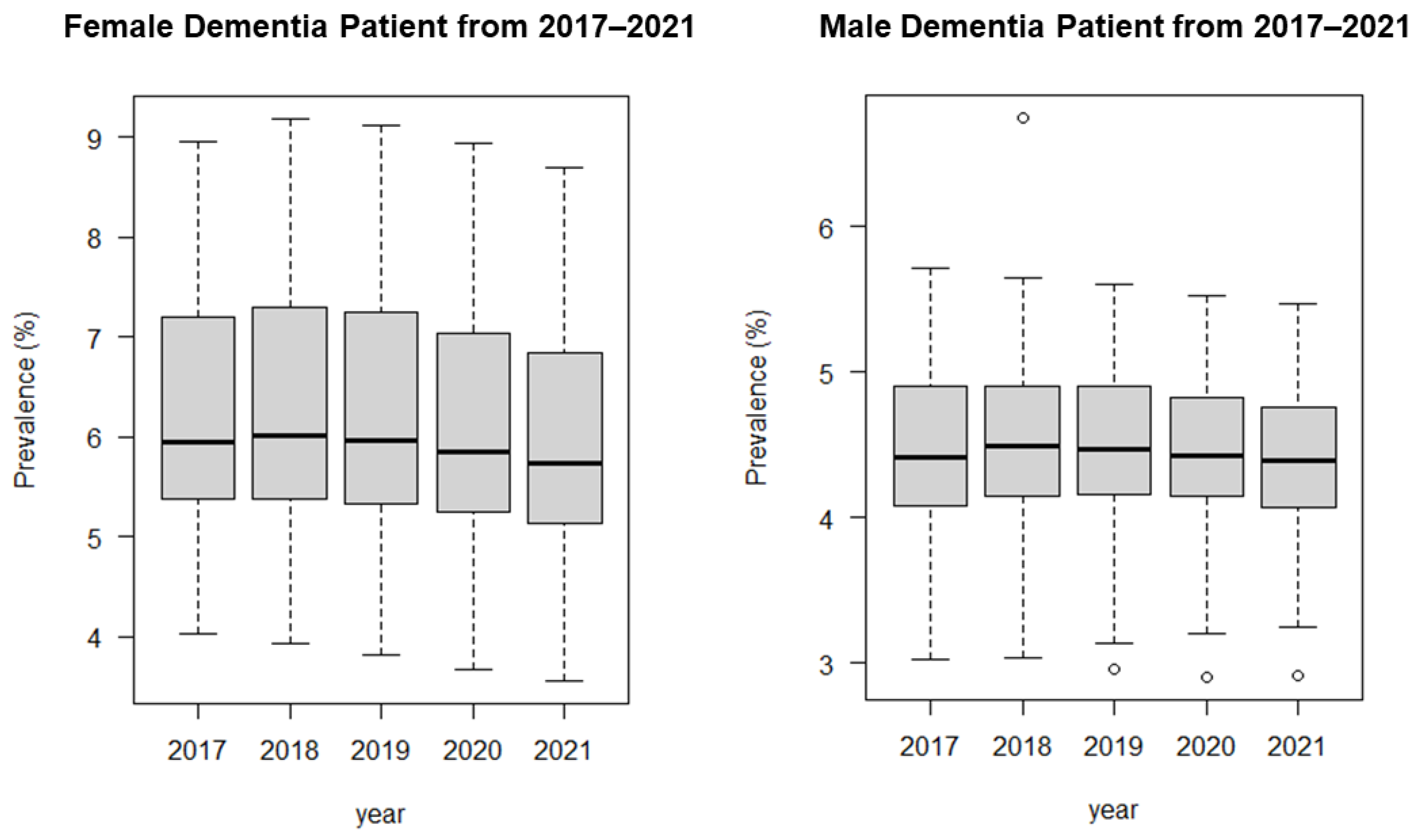
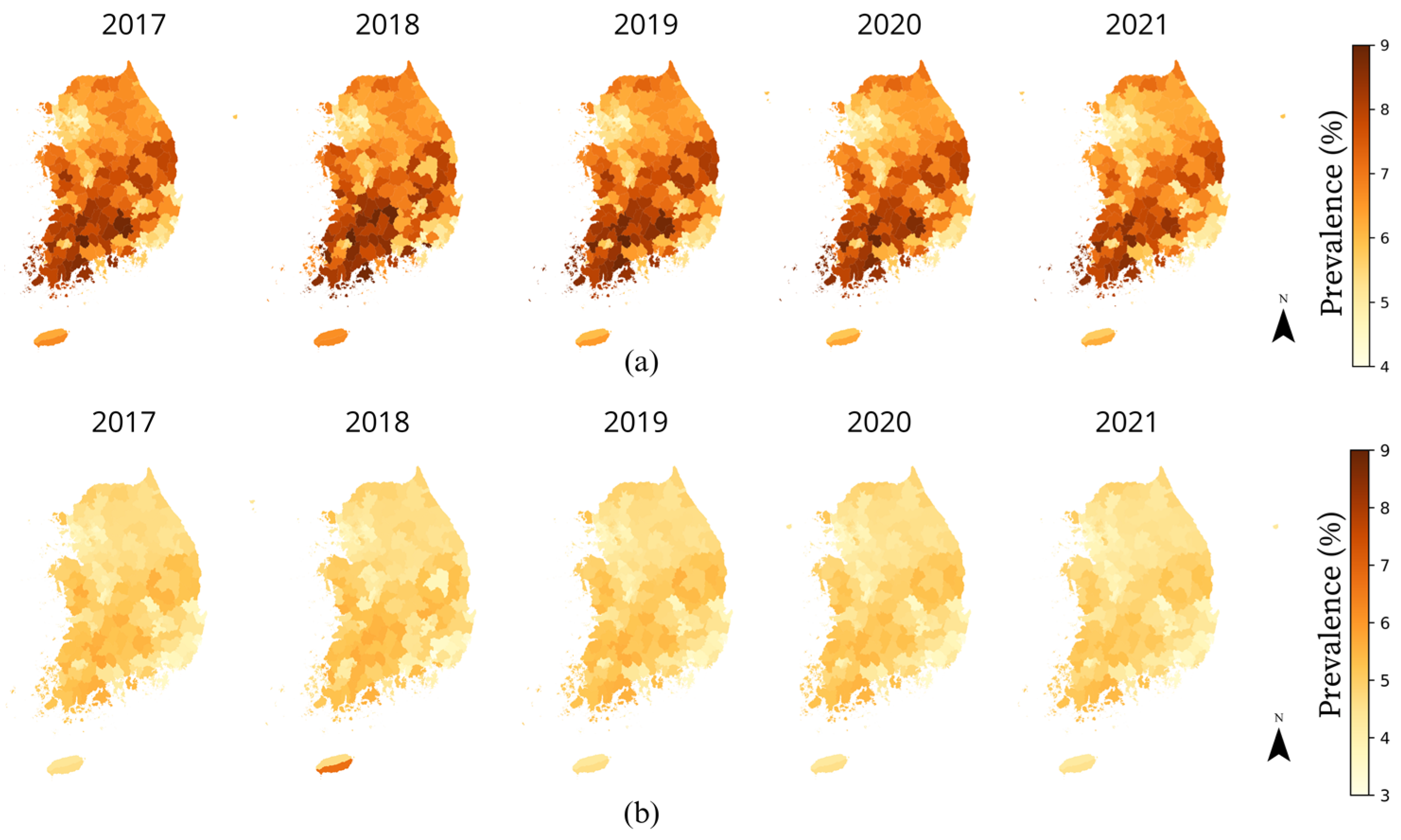
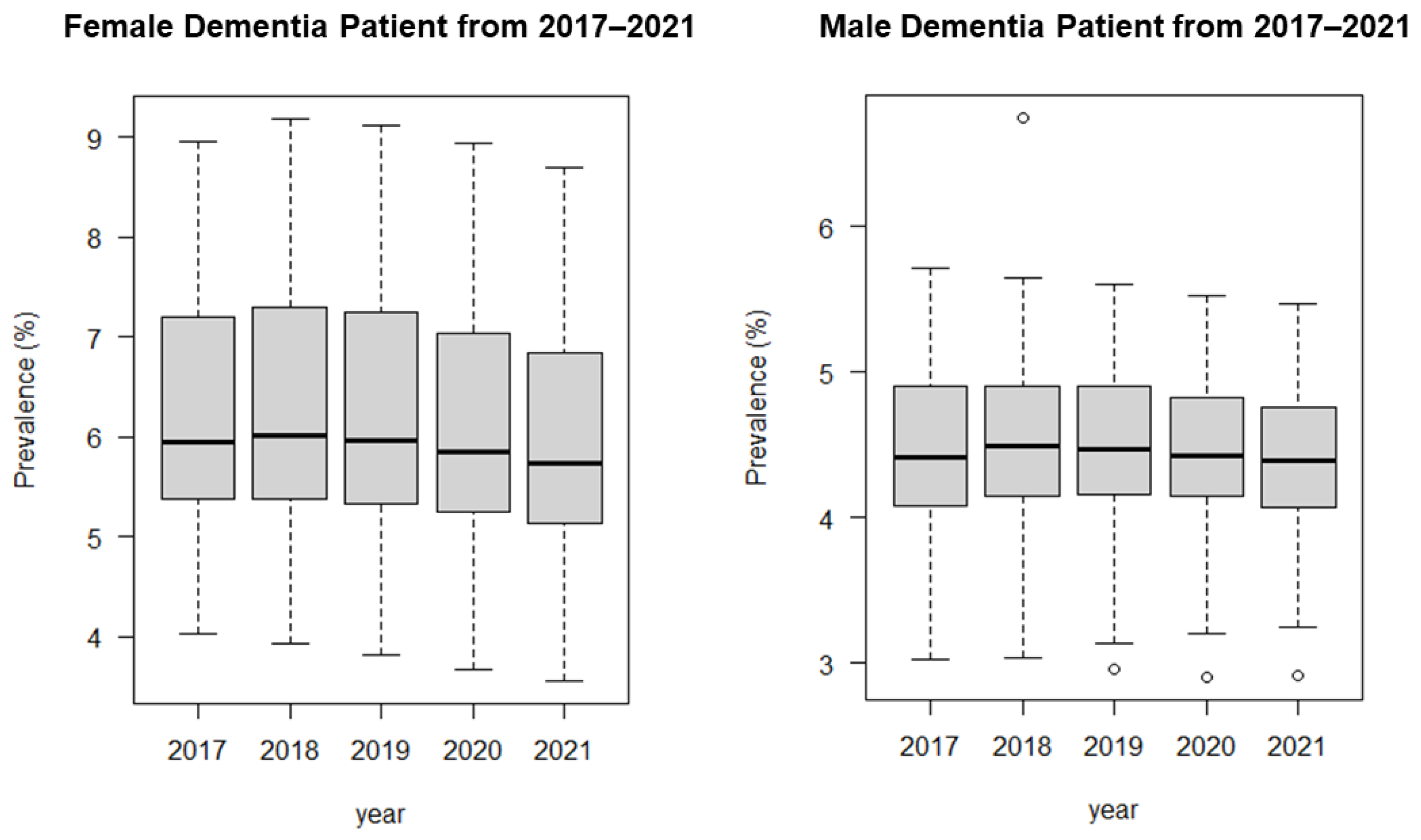
| Prevalence of female patients with dementia over 65 years (%) | 6.27 | 1.12 | 3.55 | 9.18 |
| Prevalence of male patients with dementia over 65 years (%) | 4.51 | 0.53 | 3.03 | 6.74 |
| Female patient population (%) | 50.35 | 1.39 | 43.62 | 53.49 |
| Male patient population (%) | 49.65 | 1.39 | 46.51 | 56.38 |
| Age (mean age of population) | 45.21 | 4.95 | 34.93 | 57.35 |
| Population density (individuals/km2) | 3666.08 | 5513.50 | 17.00 | 24,588.00 |
| Green-area (NDVI value) | 0.47 | 0.15 | 0.09 | 0.75 |
| Open space (%) | 4.86 | 7.71 | 0.00 | 58.64 |
| Welfare recipients (%) | 3.16 | 1.55 | 0.13 | 10.59 |
| Health status | 3.30 | 0.16 | 2.85 | 3.81 |
| Variables | NDVI | Open Space | ||||||
|---|---|---|---|---|---|---|---|---|
| Pooled OLS | Fixed-Effect | Pooled OLS | Fixed-Effect | |||||
| Female | Male | Female | Male | Female | Male | Female | Male | |
| Female patient pop. | 0.107 *** | 0.072 | 0.109 *** | 0.045 | ||||
| Male patient pop. | −0.084 *** | −0.098 *** | −0.084 *** | −0.094 *** | ||||
| Age | 0.129 *** | 0.062 *** | −0.069 *** | −0.026 *** | 0.134 *** | 0.065 *** | 0.048 | −0.012 |
| Population density | −0.0001 *** | −0.00002 *** | −0.0003 *** | −0.0002 *** | −0.0001 *** | −0.00002 *** | −0.0003 *** | −0.0002 *** |
| NDVI | 0.805 *** | 0.300 *** | 1.381 *** | 0.421 *** | ||||
| Open space | −0.003 | 0.001 | −8666.450 *** | −1466.621 * | ||||
| Welfare recipients | −0.002 | 0.006 | −0.007 | 0.002 | −0.011 | 0.002 | −0.009 | 0.0003 |
| Health status | −1.035 *** | −0.303 *** | −0.167 * | −0.067 | −1.066 *** | −0.322 *** | −0.159 * | −0.065 |
| Con. | −1.650 * | 6.766 *** | −1.468 | 6.886 *** | ||||
| N | 1175 | 1175 | 1175 | 1175 | 1175 | 1175 | 1175 | 1175 |
| R2 | 0.724 | 0.635 | 0.156 | 0.094 | 0.721 | 0.633 | 0.144 | 0.084 |
| Adjusted R2 | 0.723 | 0.634 | −0.061 | −0.139 | 0.719 | 0.631 | −0.076 | −0.151 |
| F statistic | 511.829 *** | 339.336 *** | 28.724 *** | 16.131 *** | 501.847 *** | 335.230 *** | 26.180 *** | 14.328 *** |
| AIC | 2261.532 | 667.128 | 167.806 | −1134.243 | 2278.252 | 676.196 | 184.132 | −1121.845 |
| Test | F | chisq | Df | p-Value | Result |
|---|---|---|---|---|---|
| Chow test (NDVI-female) | 19.682 | 235 | <0.001 | rejected | |
| Chow test (NDVI-male) | 14.467 | 235 | <0.001 | rejected | |
| Chow test (Open space-female) | 19.69 | 235 | <0.001 | rejected | |
| Chow test (Open space -male) | 14.415 | 235 | <0.001 | rejected | |
| Hausman test (NDVI-female) | 188.04 | 6 | <0.001 | rejected | |
| Hausman test (NDVI-male) | 94.25 | 6 | <0.001 | rejected | |
| Hausman test (Open space-female) | 265.33 | 6 | <0.001 | rejected | |
| Hausman test (Open space-male) | 97.681 | 6 | <0.001 | rejected |
| Variables | NDVI | Open Space | ||||||
|---|---|---|---|---|---|---|---|---|
| SAR-FE | SEM-FE | SAR-FE | SEM-FE | |||||
| Female | Male | Female | Male | Female | Male | Female | Male | |
| Female patient pop. | 0.0451 | 0.05494 | 0.0242 | 0.0251 | ||||
| Male patient pop. | −0.0730 ** | −0.0787 ** | −0.0692 ** | −0.0744 ** | ||||
| Age | −0.0485 ** | −0.0220 * | −0.0674 *** | −0.0314 ** | 0.0348 | −0.0127 | 0.0221 | −0.0236 *** |
| Population density | −0.0002 *** | −0.0002 *** | −0.0002 *** | −0.0001 *** | −0.0002 ** | −0.0002 *** | −0.0002 *** | −0.0002 *** |
| NDVI | 0.9793 *** | 0.3136 ** | 1.3181 *** | 0.3844 ** | ||||
| Open space | −6142.9 ** | −1022.9 | −7943.2 *** | −1161.7 | ||||
| Welfare recipients | −0.0054 | 0.0017 | −0.0037 | 0.0032 | −0.0065 | 0.0009 | −0.0045 | 0.0027 |
| Health status | −0.1392 | −0.0569 | −0.2037 * | −0.074 | −0.1309 | −0.0553 | −0.1563 | −0.0692 |
| σ2 | 0.6427 | 0.3208 | ||||||
| Rho | 0.0561 *** | 0.0511 *** | 0.1188 *** | 0.1172 *** | 0.057 | 0.051 | 0.061 *** | 0. |
| AIC | 100.305 | −1186.981 | 170.653 | −1129.437 | 106.101 | −1180.336 | 188.781 | −1115.99 |
| Years | NDVI | Open Space | ||
|---|---|---|---|---|
| Female | Male | Female | Male | |
| 2017 | 0.1420 | 0.0591 | 0.1601 | 0.0637 |
| 2018 | 0.0764 | 0.0496 | 0.1425 | 0.0675 |
| 2019 | −0.0352 | 0.0025 | −0.0083 | 0.0086 |
| 2020 | −0.0126 | −0.0314 | −0.0248 | −0.0328 |
| 2021 | −0.1706 | −0.0798 | −0.2694 | −0.1071 |
| p-value | *** | *** | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karurung, W.S.; Lee, K.; Lee, W. Comparison of Different Green Space Measures and Their Impact on Dementia Cases in South Korea: A Spatial Panel Analysis. ISPRS Int. J. Geo-Inf. 2024, 13, 126. https://doi.org/10.3390/ijgi13040126
Karurung WS, Lee K, Lee W. Comparison of Different Green Space Measures and Their Impact on Dementia Cases in South Korea: A Spatial Panel Analysis. ISPRS International Journal of Geo-Information. 2024; 13(4):126. https://doi.org/10.3390/ijgi13040126
Chicago/Turabian StyleKarurung, Wulan Salle, Kangjae Lee, and Wonhee Lee. 2024. "Comparison of Different Green Space Measures and Their Impact on Dementia Cases in South Korea: A Spatial Panel Analysis" ISPRS International Journal of Geo-Information 13, no. 4: 126. https://doi.org/10.3390/ijgi13040126
APA StyleKarurung, W. S., Lee, K., & Lee, W. (2024). Comparison of Different Green Space Measures and Their Impact on Dementia Cases in South Korea: A Spatial Panel Analysis. ISPRS International Journal of Geo-Information, 13(4), 126. https://doi.org/10.3390/ijgi13040126