
Hibiscus sabdariffa, a Treatment for Uncontrolled Hypertension. Pilot Comparative Intervention

 , , ,
, , ,  , ,
, ,
Abstract
:1. Introduction
2. Results
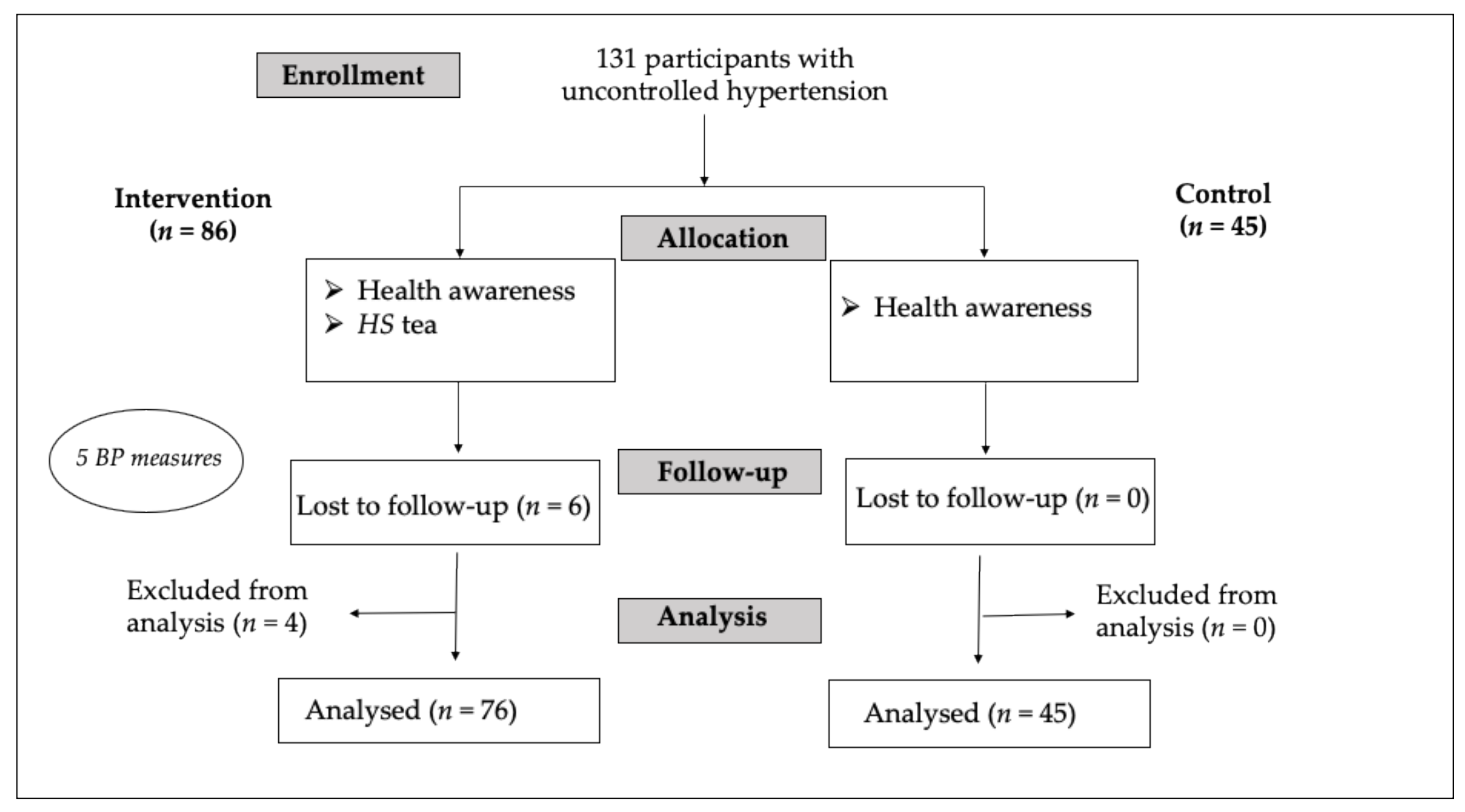
2.1. Recruitment and Baseline Characteristics
2.2. Chemical Composition of HS Decoction
3. Discussion
Limitations of the Study
4. Materials and Methods
4.1. Study Design
4.2. Participants
- Inclusion criteria:
- Age > 18 years.
- Systolic BP (SBP) ≥ 140 mmHg and/or diastolic BP (DBP) ≥ 90 mmHg, with or without ongoing antihypertensive medication.
- No evidence of cardiovascular, renal, or retinal complication.
- 2.
- Exclusion criteria:
- Hypertensive crisis requiring urgent medication.
- Overt kidney failure (serum creatinine > 1.4 mg/dL).
- Pregnant or lactating women (excluded on principle, although there is no evidence of any problems encountered with the tested food product).
- Previous adverse reaction to HS.
4.3. Intervention
4.4. Measurement Procedures
4.5. Ethical Issues
4.6. Outcome Measurements
- 1.
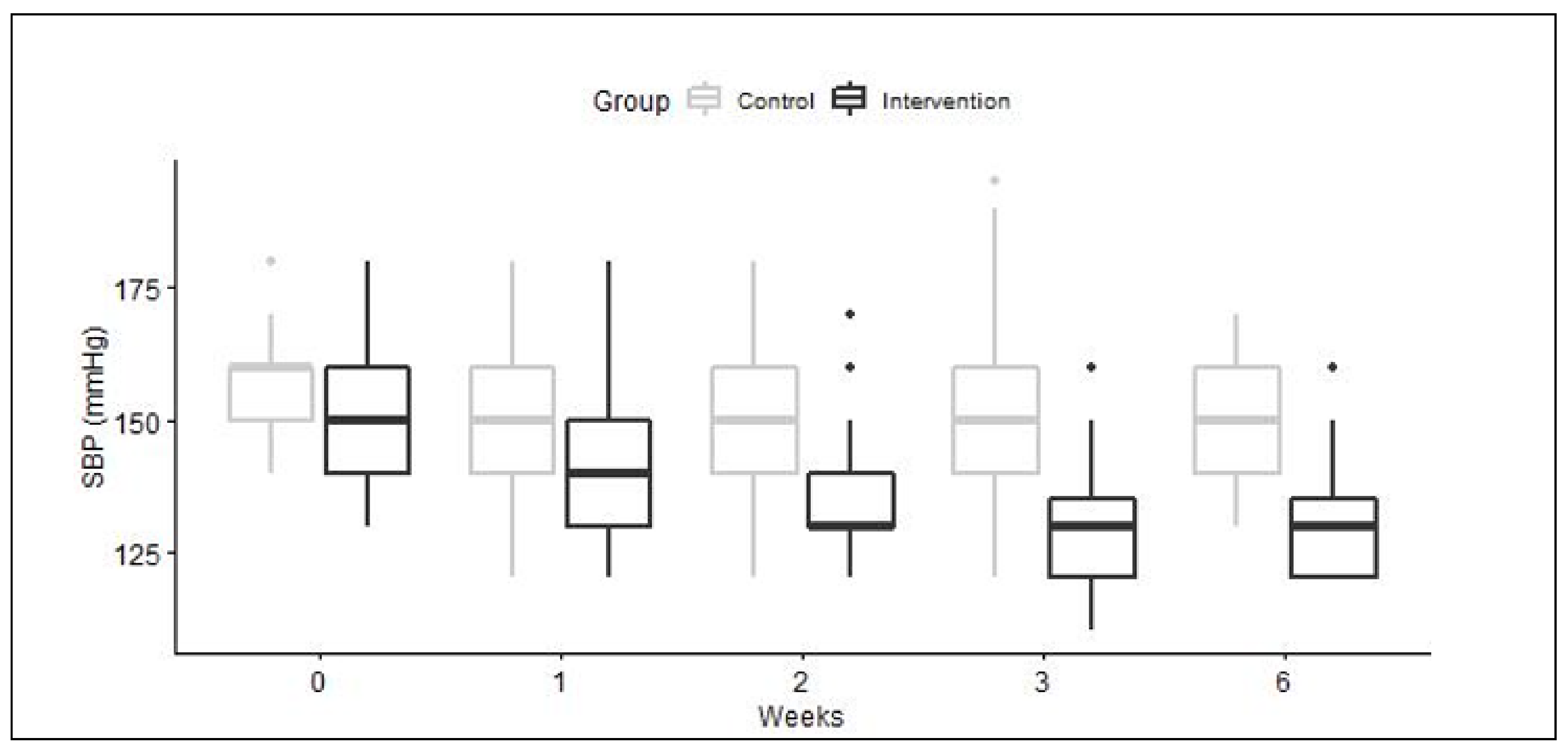
- SBP and DBP change after 6 weeks.
- 2.
- Proportion of participants reaching target BP (< 140/90 mmHg) after 6 weeks.
- 3.
- Percentage of participants for whom the SBP change was clinically significant (defined as a decrease of at least 10 mmHg).
- 4.
- Adverse events (any new symptoms, plausibility of a causal link).
- 5.
- Interaction with other medication, plausibility of a causal link.
- 6.
- Need to increase HS dosage during follow-up.
4.7. Statistical Analysis
4.8. General Experimental Procedures for the Chemical Analysis
4.9. Plant Material
4.10. HS Decoction Chemical Content Analysis
4.10.1. HPLC-PDA-ELSD Analysis of the HS Decoction
4.10.2. Quantitation of Anthocyanins
4.10.3. Identification and Quantitation of Hibiscus Acid by 1H-NMR
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Riaz, G.; Chopra, R. A review on phytochemistry and therapeutic uses of Hibiscus sabdariffa L. Biomed. Pharmacother. 2018, 102, 575–586. [Google Scholar] [CrossRef] [PubMed]
- Haji Faraji, M.; Haji Tarkhani, A. The effect of sour tea (Hibiscus sabdariffa) on essential hypertension. J. Ethnopharmacol. 1999, 65, 231–236. [Google Scholar] [CrossRef]
- Herrera-Arellano, A.; Flores-Romero, S.; Chavez-Soto, M.A.; Tortoriello, J. Effectiveness and tolerabil-ity of a standardized extract from Hibiscus sabdariffa in patients with mild to moderate hypertension: A controlled and randomized clinical trial. Phytomedicine 2004, 11, 375–382. [Google Scholar] [CrossRef]
- Herrera-Arellano, A.; Miranda-Sánchez, J.; Ávila-Castro, P.; Herrera-Alvarez, S.; Jiménez-Ferrer, J.; Zamilpa, A.; Román-Ramos, R.; Ponce-Monter, H.; Tortoriello, J. Clinical Effects Produced by a Standardized Herbal Medicinal Product of Hibiscus sabdariffa on Patients with Hypertension. A Randomized, Double-blind, Lisinopril-Controlled Clinical Trial. Planta Med. 2006, 73, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Carvajal-Zarrabal, O.; Barradas-Dermitz, D.M.; Orta-Flores, Z.; Hayward-Jones, P.M.; Nolasco-Hipólito, C.; Aguilar-Uscanga, M.G.; Miranda-Medina, A.; Bin Bujang, K. Hibiscus sabdariffa L., roselle calyx, from ethnobotany to pharmacology. J. Exp. Pharmacol. 2012, 4, 25–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boushehri, S.N.; Karimbeiki, R.; Ghasempour, S.; Ghalishourani, S.; Pourmasoumi, M.; Hadi, A.; Mbabazi, M.; Pour, Z.K.; Assarroudi, M.; Mahmoodi, M.; et al. The efficacy of sour tea (Hibiscus sabdariffa L.) on selected cardiovascular disease risk factors: A systematic review and meta-analysis of randomized clinical trials. Phytotherapy Res. 2020, 34, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Ojeda, D.; Jiménez-Ferrer, E.; Zamilpa, A.; Herrera-Arellano, A.; Tortoriello, J.; Alvarez, L. Inhibition of angiotensin convertin enzyme (ACE) activity by the anthocyanins delphinidin- and cyanidin-3-O-sambubiosides from Hibiscus sabdariffa. J. Ethnopharmacol. 2010, 127, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Zheoat, A.M.; Gray, A.I.; Igoli, J.O.; Ferro, V.A.; Drummond, R.M. Hibiscus acid from Hibiscus sabdariffa (Malvaceae) has a vasorelaxant effect on the rat aorta. Fitoterapia 2019, 134, 5–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourqui, A.; Niang, E.A.B.; Graz, B.; Diop, E.A.; Dahaba, M.; Thiaw, I.; Soumare, K.; Valmaggia, P.; Nogueira, R.C.; Cavin, A.L.; et al. Hypertension treatment with Combretum micranthum or Hibiscus sabdariffa, as decoction or tablet: A randomized clinical trial. J. Hum. Hypertens 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- AL-Anbaki, M.; Nogueira, R.C.; Cavin, A.L.; AL-Hadid, M.; AL-Ajlouni, I.; Shuhaiber, L.; Graz, B. Treat-ing Uncontrolled Hypertension with Hibiscus sabdariffa When Standard Treatment Is Insufficient: Pilot Intervention. J. Altern. Complementary Med. 2019, 25, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- UNHCR. Global Focus Iraq [Online]. UNHCR. 2020. Available online: https://reporting.unhcr.org/iraq (accessed on 28 July 2020).
- Pharmacopee Francaise. Dosage des Anthocyanides Dans la Vigne Rouge (Vitis vinifera), 11th ed.; ANSN: Saint-Denis, France, 1996. [Google Scholar]
- Wang, J.; Cao, X.; Ferchaud, V.; Qi, Y.; Jiang, H.; Tang, F.; Yue, Y.; Chin, K.L. Variations in chemical finger-prints and major flavonoid contents from the leaves of thirty-one accessions of Hibiscus sabdariffa L. Biomed. Chromatogr. 2016, 30, 8807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, A.; Kagawa, D.; Ochiai, R.; Tokimitsu, I.; Saito, I. Green Coffee Bean Extract and Its Metabolites Have a Hypotensive Effect in Spontaneously Hypertensive Rats. Hypertens. Res. 2002, 25, 99–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keasley, J.; Oyebode, O.; Shantikumar, S.; Proto, W.; McGranahan, M.; Sabouni, A.; Kidy, F. A systematic review of the burden of hypertension, access to services and patient views of hypertension in humanitarian crisis settings. BMJ Glob. Health 2020, 5, e002440. [Google Scholar] [CrossRef] [PubMed]
- Law, M.R.; Morris, J.K.; Wald, N.J. Use of blood pressure lowering drugs in the prevention of cardiovascular disease: Meta-analysis of 147 randomised trials in the context of expectations from prospective epidemiological studies. BMJ 2009, 338, b1665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peter, E.; Mashoto, K.O.; Rumisha, S.F.; Malebo, H.M.; Shija, A.; Oriyo, N. Iron and Ascorbic Acid Content in Hibiscus sabdariffa Calyces in Tanzania: Modeling and Optimization of Extraction Conditions. Int. J. Food Sci. Nutr. Eng. 2014, 4, 27–35. [Google Scholar]
- Ghiasi, S.S.; Jalalyazdi, M.; Ramezani, J.; Izadi-Moud, A.; Madani-Sani, F.; Shahlaei, S. Effect of Hibiscus sabdariffa on blood pressure in patients with stage 1 hypertension. J. Adv. Pharm. Technol. Res. 2019, 10, 107–111. [Google Scholar] [CrossRef] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Zheoat, A.M.; Gray, A.I.; Igoli, J.O.; Kennedy, A.R.; Ferro, V.A. Crystal structures of hibiscus acid and hi-biscus acid dimethyl ester isolated from Hibiscus sabdariffa (Malvaceae). Acta Crystallogr. Sect. E: Crystallogr. Commun. 2017, 73, 1368–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holzgrabe, U. Quantitative NMR spectroscopy in pharmaceutical applications. Prog. Nucl. Magn. Reson. Spectrosc. 2010, 57, 229–240. [Google Scholar] [CrossRef] [PubMed]
- Pauli, G.F.; Chen, S.-N.; Simmler, C.; Lankin, D.C.; Gödecke, T.; Jaki, B.U.; Friesen, J.B.; McAlpine, J.B.; Napolitano, J.G. Importance of Purity Evaluation and the Potential of Quantitative1H NMR as a Purity Assay. J. Med. Chem. 2014, 57, 9220–9231. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention n = 76 | Control n = 45 | |
|---|---|---|
| Age (mean ± SD) | 51.0 ± 10.3 | 53.5 ± 12.8 |
| Gender (%Female) | 60.5 | 48.9 |
| % on anti-hypertensive medication | 61.8 | 88.9 |
| Baseline SBP | 151.6 ± 11.7 | 155.9 ± 10.6 |
| Baseline DBP | 93.9 ± 8.8 | 88.7 ± 12.2 |
| SBP after 6 weeks | 128.6 ± 9.2 | 151.4 ± 10.7 |
| DBP after 6 weeks | 81.9 ± 7.7 | 85.1 ± 7.9 |
| Mean reduction SBP * | 23.1 ± 11.8 | 4.4 ± 10.2 |
| Mean reduction DBP ** | 12.0 ± 11.2 | 3.6 ± 8.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Anbaki, M.; Cavin, A.-L.; Nogueira, R.C.; Taslimi, J.; Ali, H.; Najem, M.; Shukur Mahmood, M.; Abdullah Khaleel, I.; Saad Mohammed, A.; Ramadhan Hasan, H.; et al. Hibiscus sabdariffa, a Treatment for Uncontrolled Hypertension. Pilot Comparative Intervention. Plants 2021, 10, 1018. https://doi.org/10.3390/plants10051018
Al-Anbaki M, Cavin A-L, Nogueira RC, Taslimi J, Ali H, Najem M, Shukur Mahmood M, Abdullah Khaleel I, Saad Mohammed A, Ramadhan Hasan H, et al. Hibiscus sabdariffa, a Treatment for Uncontrolled Hypertension. Pilot Comparative Intervention. Plants. 2021; 10(5):1018. https://doi.org/10.3390/plants10051018
Chicago/Turabian StyleAl-Anbaki, Marwah, Anne-Laure Cavin, Renata Campos Nogueira, Jaafar Taslimi, Hayder Ali, Mohammed Najem, Mustafa Shukur Mahmood, Ibrahim Abdullah Khaleel, Abdulqader Saad Mohammed, Hasan Ramadhan Hasan, and et al. 2021. "Hibiscus sabdariffa, a Treatment for Uncontrolled Hypertension. Pilot Comparative Intervention" Plants 10, no. 5: 1018. https://doi.org/10.3390/plants10051018