Abstract
The study was performed in the mid hills of the Dharampur region in Solan district of Himachal Pradesh, India. At the study site, a total of 115 medicinal plants were documented (38 trees, 37 herbs, 34 shrubs, 5 climbers, 1 fern, and 1 grass). In the study region, extensive field surveys were performed between March 2020 and August 2021. Indigenous knowledge of wild medicinal plants was collected through questionnaires, discussions, and personal interviews during field trips. Plants with their correct nomenclature were arranged by botanical name, family, common name, habitat, parts used, routes used, and diseases treated. In the present study, the predominant family was Rosaceae, which represented the maximum number of plant species, 10, followed by Asteraceae and Lamiaceae, which represented 8 plant species. The rural inhabitants of the Dharampur region in the Solan district have been using local plants for primary health care and the treatment of various diseases for a longer time. However, information related to the traditional knowledge of medicinal plants was not documented. The rural inhabitants of the Dharampur region reported that the new generation is not so interested in traditional knowledge of medicinal plants due to modernization in society, so there is an urgent need to document ethnomedicinal plants before such knowledge becomes inaccessible and extinct.
1. Introduction
Across the world, rural people rely on traditional local knowledge of medicinal plants for primary health care [1,2]. Ethnobotany is the study of the connection that exists among precolonial cultures of individuals and plant ecosystems. Rural people have inherited traditional medicinal plant knowledge from generation to generation [3,4]. Ethnobotanical studies are essential in the quest for modern drugs derived from natural medicinal plant resources [5,6]. For rural communities in developing countries, the use of plant species as traditional medicines provides a good alternative to health care systems [7,8]. It has been reported that 80% of the population in developing countries relies on traditional medicines for primary health care. These medicinal plants are frequently reported as safe, cheap and easily available from the surroundings [9,10]. In India, approximately 7500 plant species have been reported for medicinal use in indigenous health practices and modern systems of medicines [11,12]. Since Vedic times, plants have been used for medicinal purposes and human sustenance in India. Rig Veda and Atharveda were the first to discuss the medicinal use of plants [13]. In India, approximately 75% of the population lives in rural areas. In periods of food scarcity, most rural communities depend on natural resources such as wild edible plants to meet their food requirements [14].
Approximately 800 species of food plants are eaten by rural communities [15]. Wild plants have had significant importance in human life since ancient times; they have been used for food, medicine, fiber, and other purposes, as well as fodder for livestock. Wild edible food plants are valuable to humans and have been identified as a means of maintaining a balance between population expansion and agricultural productivity, particularly in the developing world [16]. It has been reported that approximately 54 million tribal people live in different parts of India. To continue daily life routines, local inhabitants of rural regions depend on forests and forest products. Most tribal communities still rely on local traditional medicines for their survival [17,18,19].
The biodiversity of the Indian Himalayan region millions of years ago has long been considered an important foundation for traditional medicine [20]. In the northwestern Himalayas, the state of Himachal Pradesh is divided into four zones: dry temperate-alpine, subtropical, subtemperate and moist temperate. The state of Himachal Pradesh has high plant diversity, including endemic and endangered species, due to its varied altitudinal gradients and climatic conditions [21,22]. Ninety-one commercially exploited nontimber forest product species and 57 endangered wild medicinal plant species have been identified by the state forest department of Himachal Pradesh [23]. In some parts of India, there is no proper documentation of ethnomedicinal plants used by rural communities. Therefore, systematic documentation is needed for the conservation of medicinal plant prosperity from rural areas of Himachal Pradesh in India [24,25]. Himachal Pradesh is considered one of the richest areas of traditional and potential medicinal wealth. However, limited studies have been carried out in some regions of the state to document traditional knowledge of ethnomedicinal plants [26,27]
Some researchers have attempted to document useful indigenous information on the medicinal uses of plants from the mid hills of the Dharampur region in Solan district, Himachal Pradesh, India. The survey of this study region can be a good preliminary point for new phytopharmacological research in the medicinal domain. There is no proper record available for traditional medicinal knowledge of plants used by rural people of the mid hills in the Dharampur region of Solan district in Himachal Pradesh, India. With these factors in mind, the present study was carried out with the objective of determining the various uses of medicinal plants. Further studies are required to determine the chemical compounds found in medicinal plants responsible for various biological activities.
2. Results
2.1. Demography of Informants
Ethnomedicinal data were gathered through open conversations with local informants between the ages of 25 and 75 years. A total of 114 informants, including 76 males (67%) and 38 females (33%), in the study area were interviewed to document their traditional knowledge of ethnomedicinal plants. Based on interviews, it was observed that local males, compared to local females, have better knowledge about ethnomedicines; the reason behind this might be that men are usually favored in the shift of knowledge. However, it is also observed that elderly traditional medicinal practitioners, including both men and women, have equal knowledge about ethnomedicines. In this survey, informants were categorized into five groups based on age. A total of 14 informants were between the ages of 25 and 35, 25 were between the ages of 36 and 50, 30 were between the ages of 51 and 60, 35 were between the ages of 61 and 70, and 10 were between the ages of 70 and 75 years (Table 1).

Table 1.
People of different age groups were randomly selected for interviews.
2.2. Ethnomedicinal Plants
A total of 115 ethnomedicinal plants were collected from study site during survey. Table 2 demonstrate botanical name, family, common name (Hindi), habitat, voucher no., part used, administration route, use value and usage.
Table 2.
Ethnobotanical data documented from the study site.
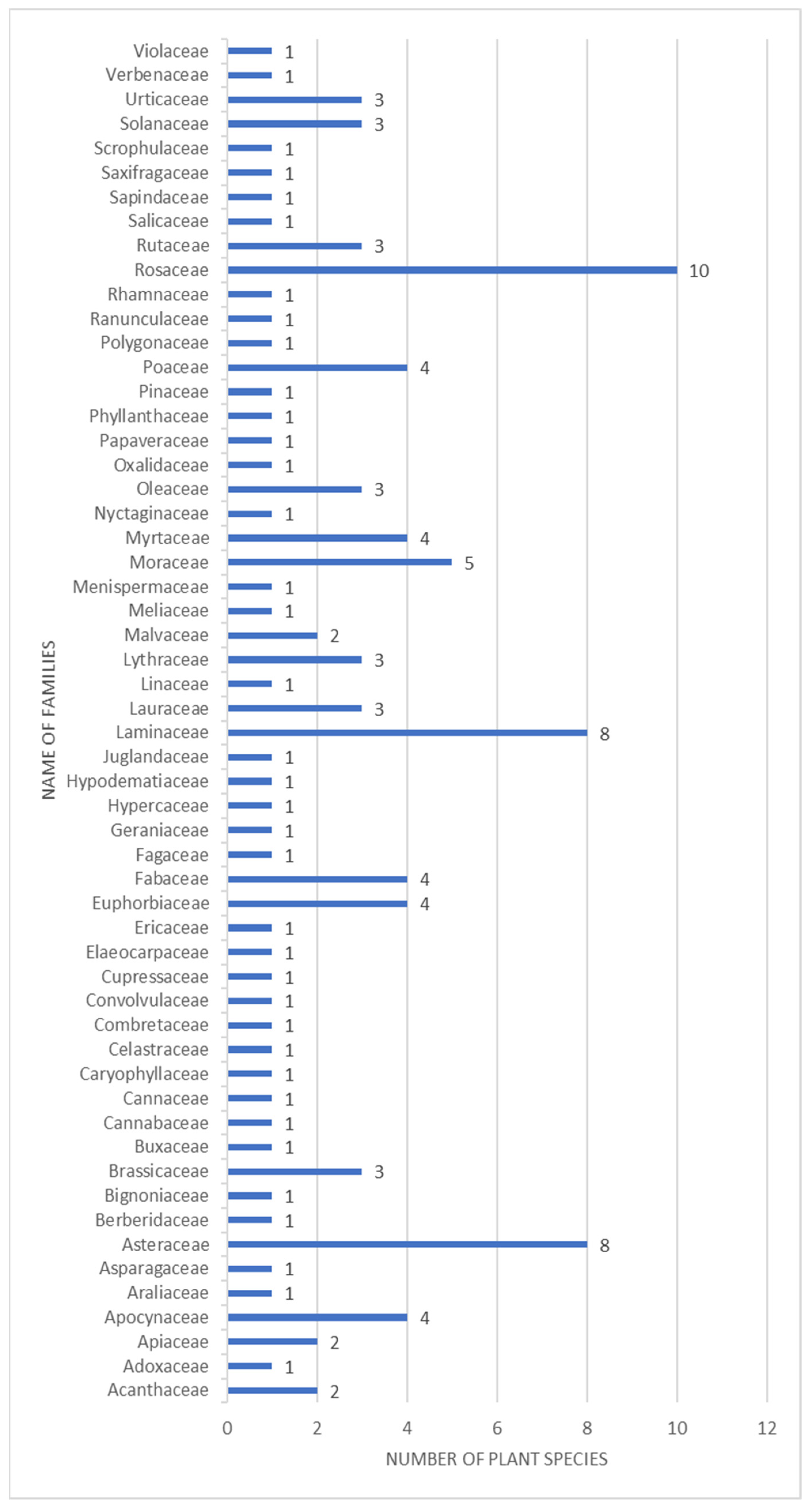
The ethnomedicinal plants collected from the study site belongs to families including Apocynaceae, Caryophyllaceae, Asteraceae, Berberidaceae, Brassicaceae, Urticaceae, Elaeocarpaceae, Salicaceae, Polygonaceae, Rhamnaceae, Rosaceae, Sapindaceae and Violaceae, etc. The highest number of ethnomedicinal plants was recorded from the family Rosaceae having 10 plant species followed by Lamiaceae and Asteraceae having 8 plant species (Figure 1).
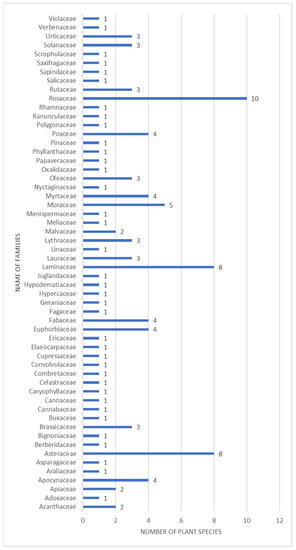
Figure 1.
Bar graph showing families and exact number of plants studied during the survey.
It was found that all the plants belonging to the Rosaceae are used to cure dysentery, fever, cough, cold and skin diseases, etc. Based on interview data it was observed that skin infection, fever cough and cold occurs more frequently as compared to other diseases. The medicinal plants reported by informers for the remedy of skin infections are Cryptolepis buchananii, Eucalyptus citriodora, Ligustrum japonicum, Pinus roxburghii, Rosa alba, Ziziphus nummularia and Sonchus oleraceus.
It was observed that some plants such as Rhododendron arboreum, Zanthoxylum armatum, Viola canescens, Quercus leucotrichophora, Rubus ellipticus, Punica granatum, Ocimum sanctum, Morus nigra, Mentha arvensis, Justicia adhatoda, Ficus benghalensis, Eriobotrya japonica, Debregeasia longifolia, Cissampelos pareira, Datura innoxia, Eucalyptus citriodora, Cynodon dactylon, Colebrookea oppositifolia, and Cannabis sativa were suggested by local informants to cure diarrhea, diabetes, dysentery, cough, cold and fever.
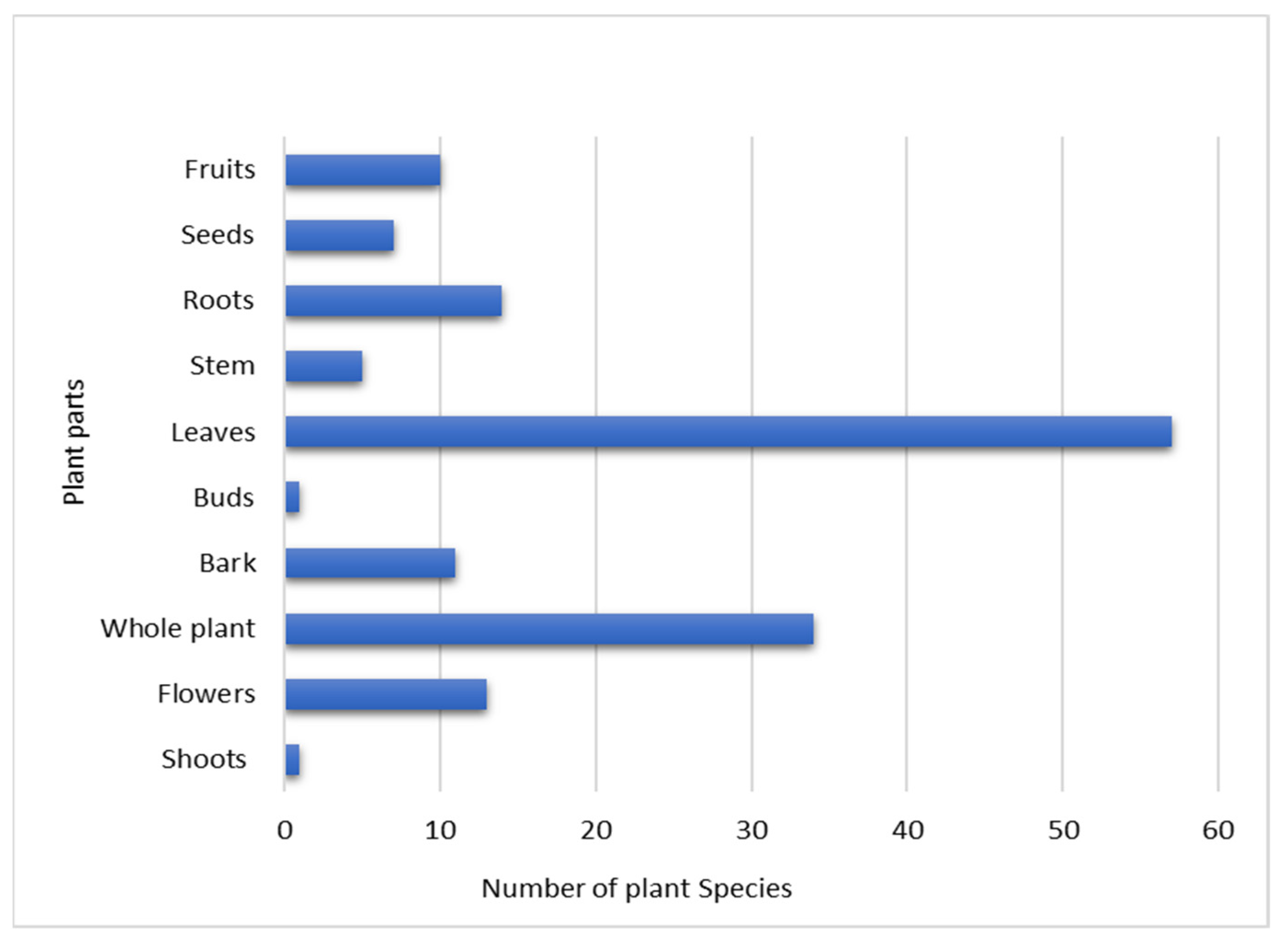
Based on the informants’ data, leaves were the most commonly used plant part, followed by whole plants, roots and flowers (Figure 2). It was also reported that in the following plant species were used: Foeniculum vulgare, Berberis asiatica, Centella asiatica, Datura innoxia, Elaeocarpus ganitrus, Euphorbia heliscopia, Euphorbia milii, Ipomoea cairica, Justicia adhatoda, Ligustrum japonicum, Nasturtium officinale, Mentha arvensis, Ocimum sanctum, Oxalis corniculata, Papaver somniferum, Prunus cerasoides, Pseudognaphalium hypoleucum, Rumex hastatus, Punica granatum, Ranunculus laetus, Salvia officinalis, Solanum virum, Spiraea cantoniensis and Stellaria media; all plant parts were utilized to cure different diseases. A few medicinal plant species reported from the study site were used in different ritual ceremonies. For example, flowers of Datura innoxia and leaves of Cannabis sativa are offered to lord Shiva in festivals such as Shivrati, and leaves of Cynodon dactylon are offered to lord Ganesh or different deities in Pooja.
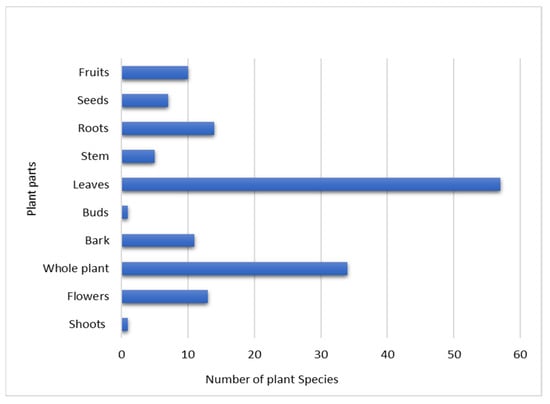
Figure 2.
Graph showing the plant parts used for medicinal purposes and the number of plant species studied in the current work.
2.3. Use Value
The results of the ethnobotanical study revealed a wealth of indigenous knowledge and the usage of traditional plants in rural people’s health care systems. The high use value of medicinal plants indicates how important they are to indigenous society in treating specific human ailments. Based on use value data, the most commonly used medicinal plant species is Catharanthus roseus (0.90), and the least commonly used medicinal plant species is Prunus persica (0.63). Catharanthus roseus is used to treat hypertension and diabetes, and Prunus persica is used to treat sores and wounds.
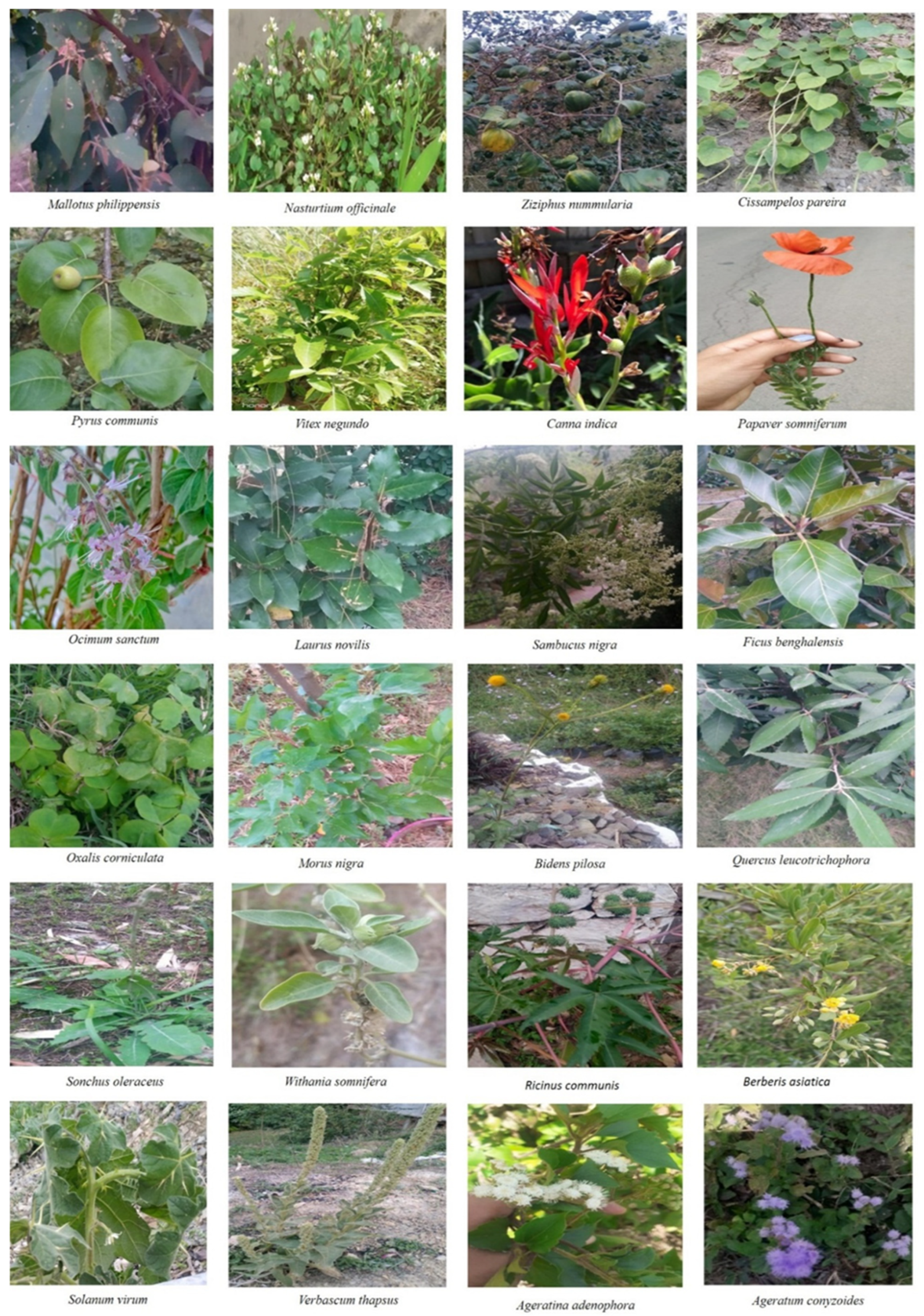
Pictures of some plants reported from the study site are shown in Figure 3.


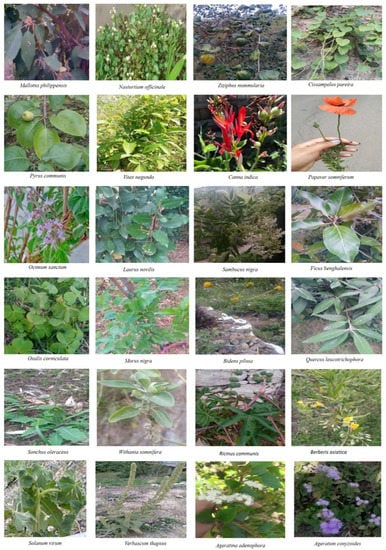
Figure 3.
Pictures of medicinal plants surveyed in the current study.
The ongoing decline of indigenous medicinal plant knowledge requires an assessment of traditional knowledge with the goal of developing the medicinal plant sector. Knowledge on indigenous uses of native plants must be studied before it becomes extinct. The findings of the current study could lead to the development of a new herbal drug for the treatment of ailments. Furthermore, ethnobotanical studies that document indigenous knowledge are important for the conservation and sustainable use of natural resources. It is essential to encourage indigenous groups and enable their participation in sustainable harvesting and conservation of natural resources to implement in situ preservation for traditional knowledge in rural areas. To enhance their position and preserve their knowledge, colleges should engage with indigenous tribes and designate them as “knowledge sites” on technical topics.
Traditional knowledge, biodiversity and cultural values are all interconnected and interdependent. These are, without a doubt, the essential factors that keep traditional knowledge intact in practice. Because of the increasing economic value of biocultural resources and threats to their existence, the government and private entities must recognize these natural resources as national wealth. Governments must establish national policy and legal frameworks to ensure that biocultural resources are effectively protected. The primary goal of this research was to document the ethnomedicinal plants utilized by rural people in the Solan district and to document indigenous knowledge about traditional plant uses through ethnobotanical research. More research into the preparation of medicinal formulations, phytochemicals, and pharmacological significance, followed by clinical trials, will add to the traditional medical and cultural systems’ knowledge base.
3. Discussion
In the present study, we documented the uses of commonly used wild medicinal plants in the mid hills of Solan district in Himachal Pradesh, India. A total of 115 plant species belonging to the same or different families were reported from the study region. Due to strong belief in the traditional system of medicine, rural people of the study region frequently prefer to use wild plants. The rural inhabitants of the study site reported that plant species Berberis aristata, Zanthoxylum armatum, Viola canescens, Rhododendron arboreum, Datura innoxia, Ocimum sanctum, Colebrookea oppositifolia, Mentha arvensis, Justicia adhatoda, Cynodon dactylon, Ficus auriculata, Cannabis sativa, Oxalis corniculata and Verbascum thapsus are highly effective in treating different types of human diseases. A few ethnomedicinal plants found in the current study have also been reported from different regions of India, such as Verbascum thapsus, Cannabis sativa, Cynodon dactylon, Ficus palmata, Urtica dioica and Juglans regia. Most of these formulations were prescribed for oral use. In recent years, it has been reported that traditional ethnobotanical knowledge of medicinal plants is gradually decreasing from society, mainly due to modernization, and some medicinal plants with ethnobotanical importance are threatened with extinction worldwide due to habitat destruction, climate change and overexploitation. Studies have reported that the documentation of ethnobotanical knowledge and ethnomedicinal plants can play a significant role in the conservation of traditional ethnobotanical knowledge and the protection of threatened ethnomedicinal plants [28,29,30,31]. The Himalayan forests provided a rich reservoir of medicinal plants that are essential to the native community [32,33]. Various studies on medicinal plants used by tribal groups in India have found that they prefer traditional medicine since it is less expensive, has fewer side effects, and is a part of their lives and culture on which our findings are set up. In India, some medicinal plants are the only source of health care in remote areas due to a lack of medical facilities [34,35,36,37]. Worldwide, traditional uses of ethnomedicinal plants vary from person to person and region to region [38,39,40,41]. Traditional knowledge of medicinal plants has deteriorated among indigenous groups in recent decades, indicating a risk of extinction. In India, recent economic advancements, exposure to the market economy, and infrastructure modernization have caused a shift in indigenous groups’ traditional lifestyles, resulting in the erosion of traditional knowledge [42]. Using indigenous knowledge of traditional medicine is an efficient method of finding novel medicines through ethnobotanical research. Some of the medicinal plants mentioned in the current study site are also documented in other studies conducted in adjoining regions of Himachal Pradesh. Freshly harvested plants or plant parts are widely utilized in human treatments. Leaves, whole plants, stems, fruits, flowers, seeds, roots, and bark are the most regularly used parts to combat human diseases. Interviewed people were enriched with traditional ethnobotanical knowledge from their parents and grandfathers. It has been found that older people have better traditional knowledge of medicinal plants than younger generations. Ethnobotanical findings could help with the development of indigenous knowledge and its application in domains including pharmacology, pharmacognosy, pharmaceuticals, toxicology, phytochemistry, ethnobotany, taxonomy, anthropology, and medicinal science. This type of alternative medical approach is now recognized as critical for community development [43,44,45]. Recent studies have reported the bioactivities of medicinal plants and phytoextracts, showing potential therapeutic use in the treatment of various ailments. The findings given in this research are preliminary and should be verified further. The link between ethnomedicinal knowledge and modern mainstream pharmacology will be highlighted by pharmacological research on ethnomedicines [46,47,48,49,50]. It has been reported that indigenous knowledge of less-known plants is gradually disappearing [51]. A recent study reported that plant-based treatments may become more popular because of the many negative effects of modern allopathic drugs [52].
Local communities lack proper knowledge of wild plant populations, marketing and selling, inadequate regulation and legal protection and have limited access to appropriate technologies for crop plantation and harvesting. Local communities also require assistance and encouragement to safeguard their knowledge and resources. The rural inhabitants of the study site reported that the new generation is not so interested in traditional knowledge of medicinal plants due to modernization, so there is an urgent need to document traditional knowledge of medicinal plants in the study site before its elimination from society. The current study may be helpful for researchers, teachers, scientists, future generations and different pharmaceutical companies to develop new drugs. A few species of wild medicinal plants (Berberis aristata, Zanthoxylum armatum and Viola canescens) were found to be overexploited by rural people and were illegally collected and sold in markets at high cost. Due to unscientific overexploitation, these plants are found in fewer numbers and need proper maintenance and conservation. Because of the current rapid shift in communities worldwide, ethnobotanical knowledge is at risk. Excessive usage of several wild plants results in destructive harvesting and a loss of plant diversity in the area. Thus, there is a need to raise awareness among the native community about the long-term use and conservation of therapeutic medicines.
4. Materials and Methods
4.1. Description of the Study Area
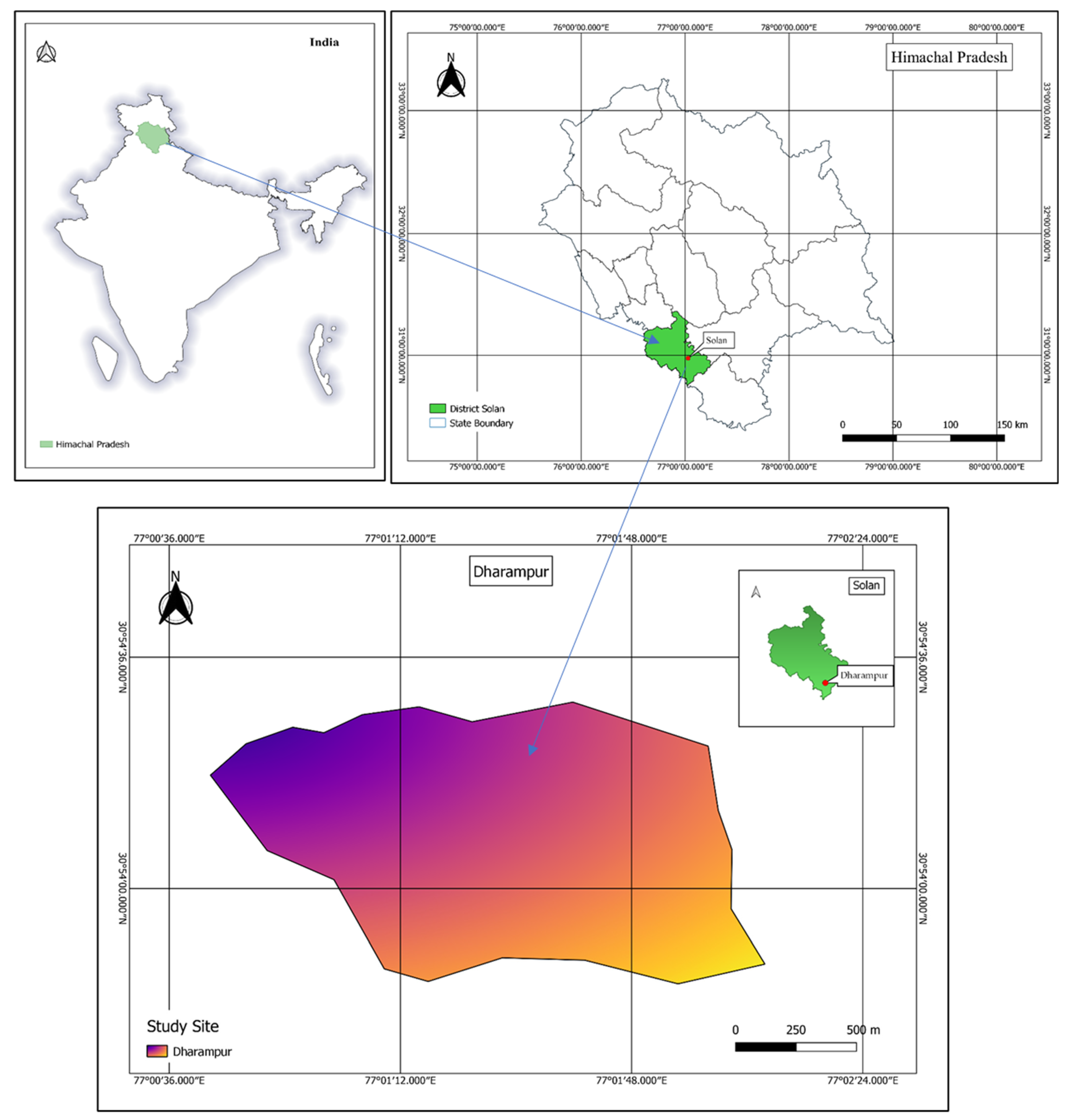
The state of Himachal Pradesh (30°22′40″–33°12′40″ N to 75°45′55″–79°04′20″ E) possesses different types of biodiversity, and it has a pleasant climate throughout the year [53]. The study was performed in the mid hills of Dharampur in Solan district of Himachal Pradesh, India. Solan district is 1350 m above sea level, with a total area of 1936 km2. The average annual rainfall is 1413 mm [25]. It snows during the winter season from Jan to Feb. Because of various climatic alterations and altitudinal gradients, Himachal Pradesh is rich in plant biodiversity, including rare and endemic plants [54]. This study documented ethnobotanical knowledge and highlighted medicinal plants that are important in the lives of rural people belonging to the Dharampur region of Solan district. A scale map of the study site is shown in Figure 4.
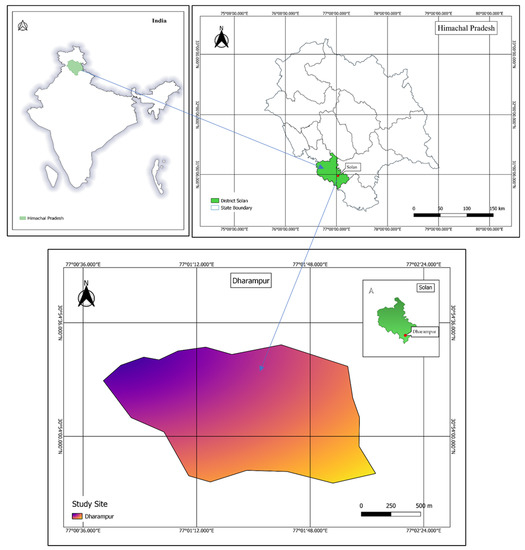
Figure 4.
Scale map showing study site Dharampur in the Solan district, Himachal Pradesh, India.
4.2. Data Collection
Extensive field surveys were carried out in the mid hills of the Dharampur region, Solan district, Himachal Pradesh from March 2020 to June 2021, as most of the plants were in the flowering stage and were easy to identify. Ethnobotanical information was gathered through a pretested questionnaire in the format given in the Supplementary information 1 (ethnobotanical survey proforma designed and pretested with local informants, later modified according to the response of informants), direct observation, discussion, and interview methods. It was found that the majority of respondents were between 61 and 75 years old. Informants with better traditional knowledge were selected by the snowball method, and the purpose of the study was explained to informants before they gave oral informed consent. Each informant agreed to participate voluntarily and was allowed to discontinue the interviews any time [55]. Local people served as guides for the field study, and samples of medicinally important plants were collected, with their local identity confirmed by informants. The collected plant specimens were dried and mounted on herbarium sheets with labelled information describing when and how plant samples were collected. All collected plant specimens were identified from the taxonomist of the Botanical Survey of India. Dehradun and voucher specimens were submitted to herbarium of Shoolini University in the Solan district, Himachal Pradesh, India.
4.3. Use Value
The importance of plant species was calculated by the use value, and a formula was used for calculation:
where Ui represents the number of usage reports mentioned by each informant for a particular plant species, and n is the total number of informants. If there are many use reports for a plant, the use values are high, which means that the plant is important, and if there are few reports, the use values are low [56,57].
UV = ΣUi/n
5. Conclusions
The current study identified 115 plant species that are utilized to treat a variety of human diseases. The findings of this study show that indigenous people living in remote tribal areas are custodians of knowledge about a wide variety of plant resource uses in the study region. The current study suggests implementing various management strategies with the involvement of indigenous communities through village administrative councils to protect medicinal plants that are threatened by extinction. Ecology is shaped by the dialectical relationship between indigenous knowledge and practice, which has an impact on the plant population. New hypotheses for sustainable resource conservation can be developed by combining indigenous knowledge and use in scientific study. Indigenous knowledge of plant resource utilization is constantly decreasing due to changing perceptions of local people and the ever-increasing influence of globalization and socioeconomic transformation. The amount of valuable plant resources is diminishing at an alarming rate due to a lack of controlled scientific and sustainable monitoring cultivation and harvesting, lack of proper management techniques, and lack of knowledge of social concerns. Additionally, indigenous knowledge of lesser-known plant uses is rapidly disappearing. Plant-based treatments may become more popular as a result of the many negative effects of modern allopathic drugs, and traditional knowledge of plants and folk remedies may be preserved. Rural inhabitants of the study area reported that the new generation is not so interested in traditional knowledge of medicinal plants due to Western influence in society, so there is an urgent need to document traditional knowledge of medicinal plants from the study region of Solan district in Himachal Pradesh. A new generation may become more aware of natural products and motivated to utilize them. However, there is less information on the active phytochemicals in these plant species; therefore, the active principles responsible for pharmacological action must be investigated further at a scientific level to validate the claim.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/plants10091842/s1, Supplementary information 1: Questionnaire for conducting the ethnomedicinal study.
Author Contributions
Conceptualization, Resources, Supervision, Writing—Original Draft Preparation, M.K., S.D., A.G.B., M.S. and S.P. (Sunil Puri); Methodology, Investigation and Writing—Original Draft Preparation, R., A.P., S.R., M.K.S., M.T., H.D., T.I. and S.P. (Suraj Prakash); Software, Writing—Review and Editing, Formal Analysis, M.M., S.P.B., M.K.B., A.S., R.A., B.B., S.N., S.C., S.S., V.K.M., A. and R.D.D.; Visualization: M.M., R. and M.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data will be available on request.
Acknowledgments
The authors are highly thankful to BSI Dehradun for identification of plant samples. The authors would like to thank the University of Kiel and Schleswig-Holstein for the support through the OA program.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO Report. WHO Global Report on Traditional and Complementary Medicine 2019; World Health Organization: Geneva, Switzerland, 2019; pp. 1–228. [Google Scholar]
- World Health Organization (WHO). WHO Traditional Medicine Strategy 2014–2023; World Health Organization: Geneva, Switzerland, 2013; pp. 1–76. [Google Scholar]
- Taek, M.M.; Banilodu, L.; Neonbasu, G.; Watu, Y.V.; EW, B.P.; Agil, M. Ethnomedicine of Tetun ethnic people in West Timor Indonesia: Philosophy and practice in the treatment of malaria. Integr. Med. Res. 2019, 8, 139–144. [Google Scholar] [CrossRef]
- Mahmood, A.; Mahmood, A.; Tabassum, A. Ethnomedicinal Survey of Plants from District Sialkot, Pakistan. J. Appl. Pharm. 2011, 3, 212–220. [Google Scholar] [CrossRef]
- Idolo, M.; Motti, R.; Mazzoleni, S. Ethnobotanical and phytomedicinal knowledge in a long history protected area, the Abruzzo, Lazio and Molise National Park (Italian Apennines). J. Ethnopharmacol. 2010, 127, 379–395. [Google Scholar] [CrossRef]
- Njoroge, G.N.; Gemmill, B.; Newton, E.L.; Ngumi, V.W.; Bussmann, R.W. Utilisation of weed species as sources of traditional medicines in central Kenya. Lyonia 2004, 7, 71–87. [Google Scholar]
- Mahmood, A.; Mahmood, A.; Malik, R.N.; Shinwari, Z.K. Indigenous knowledge of medicinal plants from Gujranwala district, Pakistan. J. Ethnopharmacol. 2013, 148, 714–723. [Google Scholar] [CrossRef] [PubMed]
- Hayta, S.; Polat, R.; Selvi, S. Traditional uses of medicinal plants in ElazIǧ (Turkey). J. Ethnopharmacol. 2014, 155, 171–184. [Google Scholar] [CrossRef]
- Fabricant, D.S.; Farnsworth, N.R. The value of plants used in traditional medicine for drug discovery. Environ. Health Perspect. 2001, 109, 69–75. [Google Scholar] [CrossRef]
- Rahman, M.A.; Mossa, J.S.; Al-Said, M.S.; Al-Yahya, M.A. Medicinal plant diversity in the flora of Saudi Arabia 1: A report on seven plant families. Fitoterapia 2004, 75, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Arti, S.; Kumar, S.V.; Pooja, S.; Sangeeta, C. Studies on Traditional Knowledge of Ethnomedicinal Plants in Jawalamukhi, Himachal Pradesh, India. Int. Res. J. Biol. Sci. 2014, 3, 6–12. [Google Scholar]
- Gowthami, R.; Sharma, N.; Pandey, R.; Agrawal, A. Status and consolidated list of threatened medicinal plants of India. Genet. Resour. Crop Evol. 2021, 68, 2235–2263. [Google Scholar] [CrossRef]
- Wani, Z.A.; Kumar, N. Akash Ethnobotanical Study of Some Threatened Plants in District Baramulla, Kashmir, Jammu and Kashmir, India. Int. J. Curr. Res. Biosci. Plant Biol. 2016, 3, 58–64. [Google Scholar] [CrossRef]
- Rashid, A.; Anand, V.K.; Serwar, J. Less known wild edible plants used by the Gujjar tribe of district Rajouri, Jammu and Kashmir State-India. Int. J. Bot. 2008, 4, 219–224. [Google Scholar] [CrossRef]
- Singh, H.B.; Arora, R.K. Wild Edible Plants of India; Daya Publishing House: New Delhi, India, 1978. [Google Scholar]
- Vishwakarma, K.L.; Dubey, V. Nutritional analysis of indigenous wild edible herbs used ineastern chhattisgarh, India. Emirates J. Food Agric. 2011, 23, 554–560. [Google Scholar]
- Vijendra, N.; Pavan Kumar, K. Traditional knowledge on ethno-medicinal uses prevailing in tribal pockets of Chhindwara and Betul Districts, Madhya Pradesh, India. Afr. J. Pharm. Pharmacol. 2010, 4, 662–670. [Google Scholar]
- Singh, K.N.; Lal, B. Ethnomedicines used against four common ailments by the tribal communities of Lahaul-Spiti in western Himalaya. J. Ethnopharmacol. 2008, 115, 147–159. [Google Scholar] [CrossRef]
- Vidyarthi, S.; Samant, S.S.; Sharma, P. Traditional and indigenous uses of medicinal plants by local residents in Himachal Pradesh, Northwestern Himalaya, India. Int. J. Biodivers. Sci. Ecosyst. Serv. Manag. 2013, 9, 185–200. [Google Scholar] [CrossRef]
- Sharma, P.; Rana, J.C.; Devi, U.; Randhawa, S.S.; Kumar, R. Floristic Diversity and Distribution Pattern of Plant Communities along Altitudinal Gradient in Sangla Valley, Northwest Himalaya. Sci. World J. 2014, 2014, 264878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chauhan, N.S. Medicinal and Aromatic Plants of Himachal Pradesh; Indus publishing: New Delhi, India, 1999. [Google Scholar]
- Sharma, P.K.; Chauhan, N.S.; Lal, B. Studies on plant associated indigenous knowledge among Malanis of Kullu district, Himachal Pradesh. Indian J. Tradit. Knowl. 2005, 4, 403–408. [Google Scholar]
- Home: Himachal Pradesh Forest Department. Available online: https://hpforest.nic.in/ (accessed on 16 July 2021).
- Muthu, C.; Ayyanar, M.; Raja, N.; Ignacimuthu, S. Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India. J. Ethnobiol. Ethnomed. 2006, 2, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, M.; Sood, S.K. Ethnobotanical survey for wild plants of district Solan, Himachal Pradesh, India. Int. J. Environ. Biol. 2013, 3, 87–95. [Google Scholar]
- Raghuvanshi, D.; Dhalaria, R.; Sharma, A.; Kumar, D.; Kumar, H.; Valis, M.; Kuča, K.; Verma, R.; Puri, S. Ethnomedicinal Plants Traditionally Used for the Treatment of Jaundice (Icterus) in Himachal Pradesh in Western Himalaya—A Review. Plants 2021, 10, 232. [Google Scholar] [CrossRef]
- Thakur, M.; Asrani, R.K.; Thakur, S.; Sharma, P.K.; Patil, R.D.; Lal, B.; Parkash, O. Observations on traditional usage of ethnomedicinal plants in humans and animals of Kangra and Chamba districts of Himachal Pradesh in North-Western Himalaya, India. J. Ethnopharmacol. 2016, 191, 280–300. [Google Scholar] [CrossRef]
- Kumar, M.; Paul, Y.; Anand, V. An Ethnobotanical Study of Medicinal Plants used by the Locals in Kishtwar, Jammu and Kashmir, India. Ethnobot. Leafl. 2009, 10, 5. [Google Scholar]
- Verma, J.; Thakur, K. Kusum Ethnobotanically important plants of Mandi and Solan districts of Himachal Pradesh, Northwest Himalaya. Plant Arch. 2012, 12, 185–190. [Google Scholar]
- Kunwar, R.M. Ethnobotanical notes on flora of Khaptad National Park (KNP), far-western Nepal. Himal. J. Sci. 2003, 1, 25–30. [Google Scholar] [CrossRef]
- Thakur, M.K.; Waske, S. Study of Medicinal Plants used by Local Herbal Healers in South Block of Seoni District (M.P.). Int. J. Theor. Appl. Sci. 2018, 10, 95–99. [Google Scholar]
- Kumar, M.; Changan, S.; Tomar, M.; Prajapati, U.; Saurabh, V.; Hasan, M.; Sasi, M.; Maheshwari, C.; Singh, S.; Dhumal, S.; et al. Custard Apple (Annona squamosa L.) Leaves: Nutritional Composition, Phytochemical Profile, and Health-Promoting Biological Activities. Biomolecules 2021, 11, 614. [Google Scholar] [CrossRef] [PubMed]
- Radha; Kumar, M.; Puri, S.; Pundir, A.; Bangar, S.P.; Changan, S.; Choudhary, P.; Parameswari, E.; Alhariri, A.; Samota, M.K.; et al. Evaluation of Nutritional, Phytochemical, and Mineral Composition of Selected Medicinal Plants for Therapeutic Uses from Cold Desert of Western Himalaya. Plants 2021, 10, 1429. [Google Scholar] [CrossRef]
- Radha; Puri, S.; Kumar, V. Phytochemical screening of medicinal plants used by tribal migratory shepherds in Western Himalaya. Ann. Biol. 2019, 35, 11–14. [Google Scholar]
- Radha; Puri, S.; Chandel, K.; Pundir, A.; Thakur, M.S.; Chauhan, B.; Simer, K.; Dhiman, N.; Shivani; Thakur, Y.S.; et al. Diversity of ethnomedicinal plants in Churdhar Wildlife Sanctuary of district Sirmour of Himachal Pradesh, India. J. Appl. Pharm. Sci. 2019, 9, 48–53. [Google Scholar] [CrossRef] [Green Version]
- Radha; Janjua, S.; Ali, M.; Thakur, M.; Jamwal, R.; Rathour, S.; Kumar Pubral, A.; Kumari, N.; Puri, S.; Pundir, A.; et al. Documenting Traditional Knowledge before they are Forgotten: A Study on the Ethnomedicinal uses of Wild Plants by Rural People of Jubbarhatti in District Shimla. Int. J. Theor. Appl. Sci. 2021, 13, 37–51. [Google Scholar]
- Nautiyal, S.; Rao, K.; Maikhuri, R.; Saxena, K.G. Traditional knowledge related to medicinal and aromatic plants in tribal societies in a part of Himalaya. J. Med. Aromat. Plant Sci. 2002, 22, 528–541. [Google Scholar]
- Negi, C. Socio-cultural dimensions and ethnobotanical value of a sacred forest-Thal ke Dhar, Central Himalaya, India. Indian J. Tradit. Knowl. 2005, 4, 190–198. [Google Scholar]
- Garbyal, S.; Aggarwal, K.; Babu, C. Traditionally used medicinal plants in Dharchula Himalayas of Pithoragarh district, Uttaranchal. Indian J. Tradit. Knowl. 2005, 4, 199–207. [Google Scholar]
- Kandari, L.S.; Phondani, P.C.; Payal, K.C.; Rao, K.S.; Maikhuri, R.K. Ethnobotanical study towards conservation of medicinal and aromatic plants in upper catchments of Dhauli Ganga in the central Himalaya. J. Mt. Sci. 2012, 9, 286–296. [Google Scholar] [CrossRef]
- Bhat, J.A.; Kumar, M.; Negi, A.K.; Todaria, N.P. Informants’ consensus on ethnomedicinal plants in Kedarnath Wildlife Sanctuary of Indian Himalayas. J. Med. Plants Res. 2013, 7, 148–154. [Google Scholar] [CrossRef]
- Agrawal, D.P. Traditional knowledge systems and western science. Curr. Sci. 1997, 73, 731–733. [Google Scholar]
- Spjut, R.W. Plant folklore: A tool for predicting sources of antitumor activity? In Proceedings of the 16th annual meeting of the Society for Economic Botany: “Plants and cancer.”, Baltimore, MA, USA, 15–18 June 1975; Springer: Berlin/Heidelberg, Germany, 1976; Volume 60, pp. 979–985. [Google Scholar]
- Bisht, S.; Adhikari, B.S. Ethnobotanical study of traditional medicinal plants used by Banraji Community in Uttarakhand, West Himalayan. J. Ethnobiol. Tradit. Med. 2018, 129, 1426–1441. [Google Scholar]
- Radha, S.P.; Pundir, A. Review on Ethnomedicinal Plant: Trillium govanianum Wall. Ex D. Don. Int. J. Theor. Appl. Sci. 2019, 11, 4–9. [Google Scholar]
- Singh, R.P.; Prakash, S.; Bhatia, R.; Negi, M.; Singh, J.; Bishnoi, M.; Kondepudi, K.K. Generation of structurally diverse pectin oligosaccharides having prebiotic attributes. Food Hydrocoll. 2020, 108, 105988. [Google Scholar] [CrossRef]
- Kumar, M.; Prakash, S.; Radha; Kumari, N.; Pundir, A.; Punia, S.; Saurabh, V.; Choudhary, P.; Changan, S.; Dhumal, S.; et al. Beneficial role of antioxidant secondary metabolites from medicinal plants in maintaining oral health. Antioxidants 2021, 10, 1061. [Google Scholar] [CrossRef]
- Kumar, M.; Tomar, M.; Saurabh, V.; Sasi, M.; Punia, S.; Potkule, J.; Maheshwari, C.; Changan, S.; Radha; Bhushan, B.; et al. Delineating the inherent functional descriptors and biofunctionalities of pectic polysaccharides. Carbohydr. Polym. 2021, 269, 118319. [Google Scholar] [CrossRef]
- Kumar, M.; Tomar, M.; Punia, S.; Grasso, S.; Arrutia, F.; Choudhary, J.; Singh, S.; Verma, P.; Mahapatra, A.; Patil, S.; et al. Cottonseed: A sustainable contributor to global protein requirements. Trends Food Sci. Technol. 2021, 111, 100–113. [Google Scholar] [CrossRef]
- Kumar, M.; Potkule, J.; Patil, S.; Mageshwaran, V.; Radha; Satankar, V.; Berwal, M.K.; Mahapatra, A.; Saxena, S.; Ashtaputre, N.; et al. Evaluation of detoxified cottonseed protein isolate for application as food supplement. Toxin Rev. 2021. [Google Scholar] [CrossRef]
- Sivasankari, B.; Anandharaj, M.; Gunasekaran, P. An ethnobotanical study of indigenous knowledge on medicinal plants used by the village peoples of Thoppampatti, Dindigul district, Tamilnadu, India. J. Ethnopharmacol. 2014, 153, 408–423. [Google Scholar] [CrossRef]
- Yuan, H.; Ma, Q.; Ye, L.; Piao, G. The traditional medicine and modern medicine from natural products. Molecules 2016, 21, 559. [Google Scholar] [CrossRef] [Green Version]
- Radha, R.; Chauhan, P.; Puri, S.; Thakur, M.; Rathour, S.; Sharma, A.K.; Pundir, A. A study of wild medicinal plants used in Nargu Wildlife Sanctuary of district Mandi in Himachal Pradesh, India. J. Appl. Pharm. Sci. 2021, 11, 135–144. [Google Scholar] [CrossRef]
- Radha; Janjua, S.; Srivastava, S.; Negi, V. Ethnobotanical study of medicinal plants used in shikari devi wildlife sanctuary of Himachal Pradesh, India. Med. Plants 2020, 12, 666–673. [Google Scholar] [CrossRef]
- Ribeiro, R.V.; Bieski, I.G.C.; Balogun, S.O.; de Oliveira Martins, D.T. Ethnobotanical study of medicinal plants used by Ribeirinhos in the North Araguaia microregion, Mato Grosso, Brazil. J. Ethnopharmacol. 2017, 205, 69–102. [Google Scholar] [CrossRef] [PubMed]
- Phillips, O.; Gentry, A.H.; Reynel, C.; Wilkin, P.; B, C.G.-D. Quantitative Ethnobotany and Amazonian Conservation. Conserv. Biol. 1994, 8, 225–248. [Google Scholar] [CrossRef]
- Musa, M.S.; Abdelrasool, F.E.; Elsheikh, E.A.; Ahmed, L.A.M.N.; Mahmoud, A.L.E.; Yagi, S.M. Ethnobotanical study of medicinal plants in the Blue Nile State, South-eastern Sudan. J. Med. Plants Res. 2011, 5, 4287–4297. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).