Abstract
As the proportion of the population comprising the elderly cohort increases, so too does the demand for medical care for long-term conditions among this demographic. The advent of information technology and artificial intelligence has prompted a crucial examination of the potential of smart medical technology and equipment to enhance the quality of long-term care and the operational efficiency of long-term care facilities. The introduction of smart healthcare into long-term care is influenced by a few factors, and expert opinions often exhibit ambiguity and subjectivity in the evaluation process. As Z-numbers are capable of adequately expressing the ambiguity of expert assessments and the degree of certainty associated with them, they are employed in this study to convey the opinions of the experts. Furthermore, the Decision-Making Trial and Evaluation Laboratory (DEMATEL) method is an effective approach to analyzing the relationships between factors. Consequently, this study integrates the Z-numbers and DEMATEL methods for empirical analysis. The present study focuses on two long-term care institutions with different natures as empirical subjects. The findings of the study indicate that Institution A identifies the “Internet of Things” as the most pivotal key factor, whereas Institution B deems “Smart clinics and urgent care centers” to be the most crucial key factor. The analysis demonstrates that three factors—global positioning systems, telemedicine, and electronic medical records—are all regarded as significant influencing factors for different long-term care institutions. Consequently, the analytical model of this study is not only theoretically sound but also effective in identifying the key factors and importance of introducing smart healthcare into long-term care institutions.
Keywords:
long-term care; smart healthcare; Z-numbers; decision-making trial and evaluation laboratory (DEMATEL) method MSC:
65H04; 65H05; 65H10; 65H17
1. Introduction
In recent years, the proportion of the elderly population has continued to increase, resulting in a rapid increase in the demand for medical care for the elderly. In response to this, a new medical care model, designated as “long-term care”, has emerged. The term ‘long-term care’ encompasses a broad range of services provided to individuals with disabilities in various settings, including their own homes, nursing homes, and assisted living facilities [1]. Furthermore, shifts in family structure, changes in work patterns, and increased demand for labor have also contributed to an increase in the number of families requiring long-term care services. To meet the demand for long-term care services, long-term care institutions have emerged with the objective of assisting families who require these services and thereby alleviating the burden and pressure of care.
The enhancement of living conditions and the progression of medical technology have resulted in a sustained improvement in the standard of living and an accompanying increase in the average life expectancy of the global population. Furthermore, the decline in the birth rate of newborns has resulted in the gradual transition of many countries towards an aging population structure. Long-term care services can facilitate the elderly population’s engagement in daily activities, encourage social participation, and monitor their physical and mental well-being. Consequently, long-term care for the elderly has emerged as a significant concern [2].
In recent years, the advent of smart medicine has led to a reduction in the number of medical burdens through the utilization of smart medicine-related technologies and equipment. Additionally, Taiwan’s medical system is facilitating collaboration between the medical and electronic industries, thereby ushering in a new era of medical technology and healthcare. It is therefore imperative to introduce smart medical technology into the long-term care system with a view to improving the quality of care. The majority of long-term care units in Taiwan are deficient in both robust information systems and the operational capabilities required to effectively utilize them. This presents a significant challenge in the integration of smart medicine into long-term care settings. It is therefore imperative to identify the key factors of smart medical care for long-term care services and ascertain the psychological needs of long-term caregivers. Doing so will not only mitigate the impact of the shortage of medical professionals but also enhance the efficacy of integrating smart medical care into long-term care [3,4].
Indeed, numerous factors influence the integration of smart medical care into long-term care, with these factors often exhibiting a correlation [5]. Furthermore, the subjective assessment of experts when evaluating factors is typically vague and uncertain. Accordingly, the linguistic Z-number permits experts to articulate their subjective opinions in a comprehensive manner, thereby reducing the ambiguity and uncertainty inherent to the evaluation process [6]. The fuzzy Delphi method is an effective approach for incorporating and integrating the opinions of all experts [7,8]. Concurrently, the Decision-Making Trial and Evaluation Laboratory (DEMATEL) method is capable of effectively analyzing the degree of influence between factors, calculating the importance of key factors, and confirming the causal relationship of key factors [9,10,11]. Accordingly, this study employs a two-stage systematic analysis model that integrates the linguistic Z-number, the fuzzy Delphi method, and the DEMATEL method to effectively analyze the key factors and their importance in the introduction of smart medical care into long-term care. The initial phase of the study entailed the collation and examination of the pertinent literature, as well as the identification of pivotal factors through the linguistic Z-number and fuzzy Delphi methods. The second phase of the study entailed measuring the degree of relevance of the key factors and calculating the importance of the key influencing factors through the DEMATEL method. Moreover, a case study was conducted on two long-term care institutions with disparate characteristics and sizes.
2. Literature Review
2.1. Long-Term Care
In recent years, several factors have contributed to a significant growth in the social structure of the elderly population. These include the formation of an aging society, the expansion of medical technology, the increase in average life expectancy, and the decline in the birth rate. This has led to a rapid rise in the demand for medical care for the elderly. The term ‘long-term care’ encompasses a broad range of services provided to individuals with disabilities in various settings, including their own homes, nursing homes, and assisted living facilities [1]. Furthermore, shifts in family structure, alterations in work patterns, and an elevated demand for labor have contributed to an escalating number of families requiring long-term care services. It follows that long-term care institutions and care services are inextricably linked, rendering long-term care services a pivotal concern in the welfare policy for the elderly. Tchouaket et al. [12] posit that long-term care services encompass assistance with activities of daily living (ADL), including transfer and mobility, bathing, dressing, personal hygiene, toileting, meal preparation, and medication administration. The content of long-term care services varies from country to country due to differences in healthcare systems and funding mechanisms. However, there are common characteristics that are present in most long-term care services. These include the need for 24 h service, the provision of accommodation facilities, including professional medical services, and personal care services such as meals, laundry, and housekeeping services [13].
As the phenomenon of declining birthrate becomes increasingly serious, it has resulted in a shortage of care human resources and has also had an impact on the development of the long-term care industry. The interconnected reliability, preventive collaboration, and innovative features of the industry can serve to mitigate the impact of the shrinking human resource population. To illustrate, a robot with an appealing appearance and an anthropomorphic dialogue function could be employed to provide exercise classes and spiritual healing functions, thereby assisting caregivers in their daily care and rehabilitation guidance. The integration of intelligent medical care with care behavior not only preserves the user’s sense of self-worth but also curtails the expenditure incurred by long-term care institutions and long-term medical care on personnel.
2.2. Smart Medicine
The shift in population structure and the proliferation of information technology have precipitated the ascendance of smart healthcare as a pivotal aspect of global medical policy formulation in recent years. The concept of smart healthcare is not merely an advancement of medical technology; it also has a significant impact on the medical level [14]. This impact can be observed in several areas, including changes in the medical model (from disease-centered to patient-centered), changes in information construction (from clinical information to regional medical information), changes in medical management (from comprehensive management to personalized management), and changes in prevention and treatment concepts (from focusing on disease treatment to focusing on preventive healthcare). As defined by the World Health Organization [15], “smart health (e-health) is the utilization of information and communication technology in a cost-effective and secure manner to facilitate health and health-related domains, encompassing healthcare services, health monitoring, health literature, and health education, knowledge and research”. For hospitals, the implementation of smart health enables medical teams to dedicate a greater proportion of their time to direct patient care, while simultaneously reducing the expenditure associated with the acquisition and maintenance of information technology. From the perspective of medical staff, the utilization of smart health technologies can facilitate the selection of appropriate pharmaceuticals, provide information on potential adverse effects or interactions, and reduce instances of incorrect medication and medical errors, thus enhancing the overall safety of medical care [14]. The utilization of wearable devices facilitates the implementation of continuous monitoring and online medical consultations, thereby addressing patients’ specific medical care requirements and enhancing the efficiency of both medical professionals and patients [14].
In recent years, the development of technologies such as artificial intelligence, cloud computing, ICT, and the Internet of Things has facilitated the accelerated development of smart medical technologies and equipment, such as the application of telemedicine, AI surgical robots, and other related medical technologies [9,16]. At present, a considerable number of hospitals have commenced the implementation of the concept of smart wards. The proliferation of wireless networks, network-enabled medical instruments, wearable device sensors, and smartphone app applications has led to a significant expansion of the original medical environment beyond hospitals, encompassing individuals, families, institutions, communities, and even entire cities. The integration of information technology and communications allows for the development of smart medicine, which in turn facilitates the development of smart life and smart health.
In conclusion, the concept of smart healthcare can be defined as the integration of information technology, the Internet of Things, and multiple medical fields. The introduction of this concept into the long-term care industry has the potential to achieve several key objectives. Firstly, it has the capacity to save human resources, reduce the cost of chronic disease care, and obtain information needed for care without time and space restrictions. Secondly, it can facilitate the effective acceleration of long-term care development through the integration of smart healthcare and long-term care services. The term “smart healthcare” is used to describe the utilization of a range of information and communication technologies (ICTs) to deliver medical care and support services. This study presents a summary of the pertinent influencing factors associated with the introduction of smart healthcare into long-term care, as illustrated in Table 1.

Table 1.
Factors influencing smart healthcare in long-term care.
2.3. Fuzzy Set Theory
2.3.1. Triangular Fuzzy Numbers
A triangular fuzzy number is a frequently utilized representation of a fuzzy number in decision analysis models, with applications spanning numerous fields, including fuzzy control and fuzzy decision-making [30]. Since the operation of triangular fuzzy numbers is relatively simple and describes the ambiguity of experts’ opinions, this study uses triangular fuzzy numbers to express experts’ opinions and conduct operational analyses.
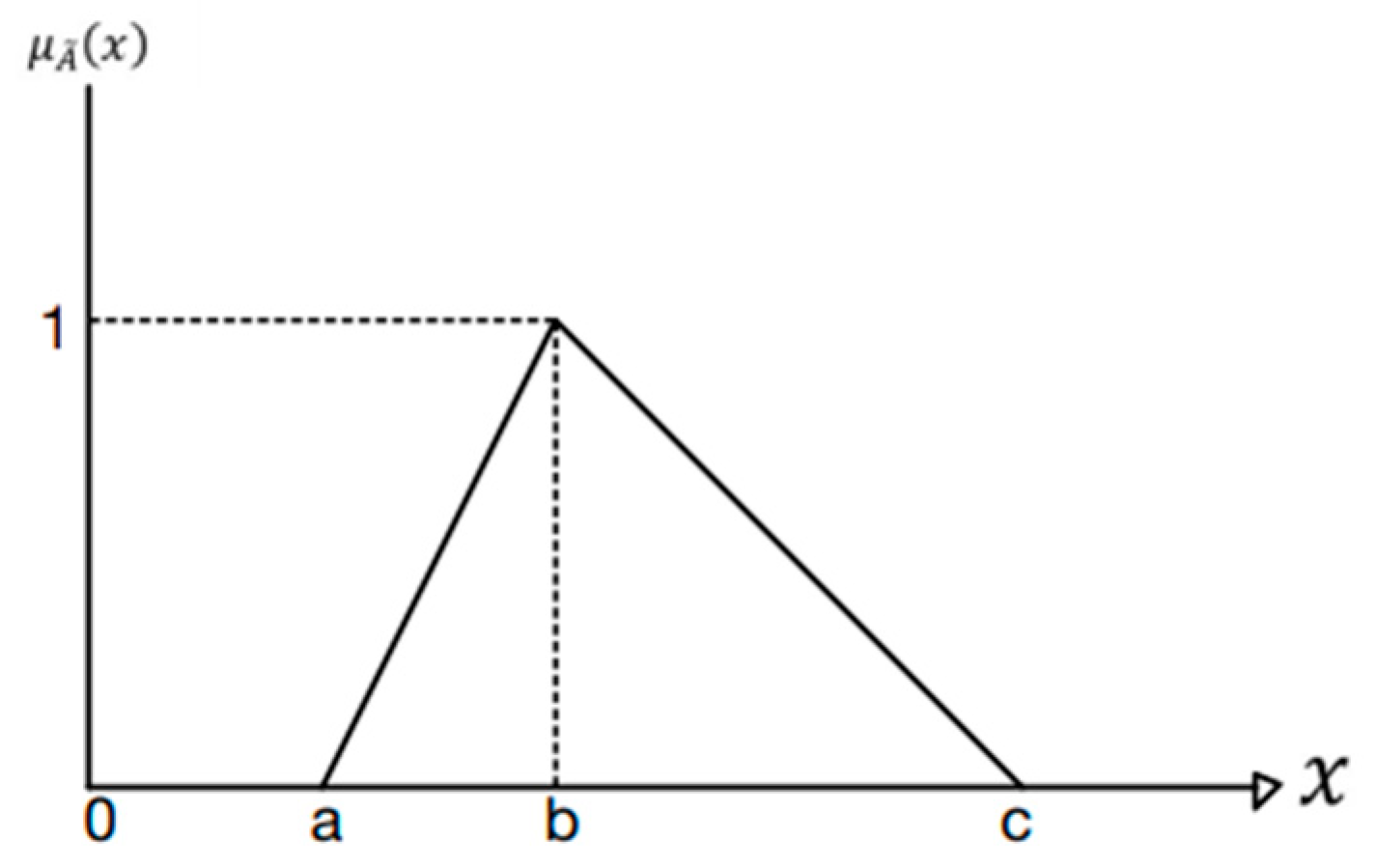
A triangular fuzzy number, represented by , is a fuzzy set. Its membership function, , is as follows (see Figure 1) [31,32]:
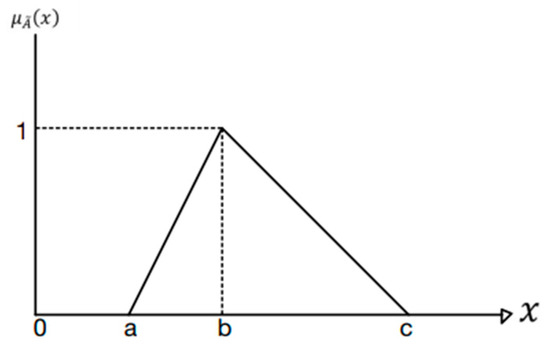
Figure 1.
Triangular fuzzy numbers.
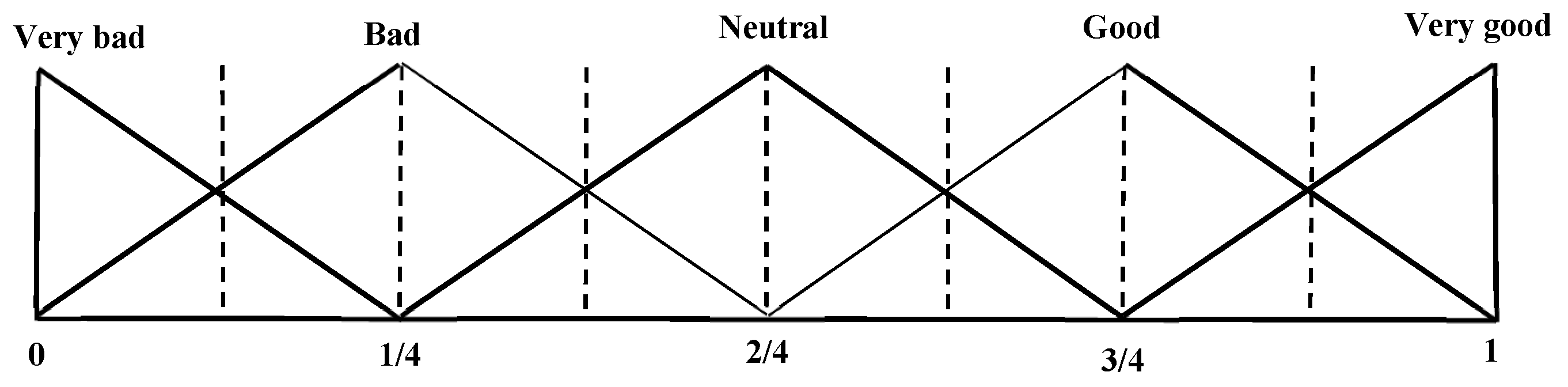
2.3.2. Linguistic Variables
Linguistic variables are words or sentences in natural or human language that describe complex or ambiguous situations that cannot be expressed with crisp values [31]. In the context of decision-making, experts can readily employ linguistic variables to articulate their subjective perspectives in a comprehensive manner. To illustrate, the membership functions of five linguistic variables are presented in Figure 2. The triangular fuzzy number representing the linguistic variable “good” is expressed as (0.5, 0.75, 1.0).
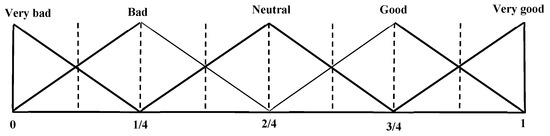
Figure 2.
Linguistic variable scale.
2.3.3. Fuzzy Operations
Let us assume that two positive triangular fuzzy numbers are given by and . The fuzzy operation rules are as follows [33,34]:
2.3.4. Defuzzification Methods
Defuzzification may be defined as the process of converting a fuzzy number into a crisp value. The centroid method is a frequently employed defuzzification technique. The calculation method is as follows [9,35]:
where is the membership function of the fuzzy set , and is the defuzzified value of .
2.3.5. Z Number
Zadeh [36] expanded the concept of fuzzy numbers and proposed Z-numbers as a means of providing a basis for the calculation of incompletely reliable fuzzy sets. Z-numbers are represented by the formula Z = (A, R), where A is the fuzzy evaluation value and R is the reliability value of A [37]. Z-numbers provide a means of describing the situation of imperfect information pertaining to a random variable, through the use of an evaluation value and a credibility value [38,39]. Let us assume that a Z-number is represented by the equation Z = (,), where is a triangular fuzzy number, expressed as . The reliability of the description, expressed as , is represented by .
The following is a description of the calculation process for converting a Z-number into a triangular fuzzy number () and for defuzzification:
Step 1: Convert the fuzzy credibility () into a crisp value () using the centroid method as follows [40]:
where is the membership function of .
Step 2: The Z number should be converted into a triangular fuzzy number, designated as . The crisp value () is multiplied by the fuzzy evaluation value to obtain the triangular fuzzy number . The calculation formula is as follows:
Step 3: Use the centroid method to convert into , calculated as follows:
where is the membership function of triangular fuzzy number .
3. The Proposed Model
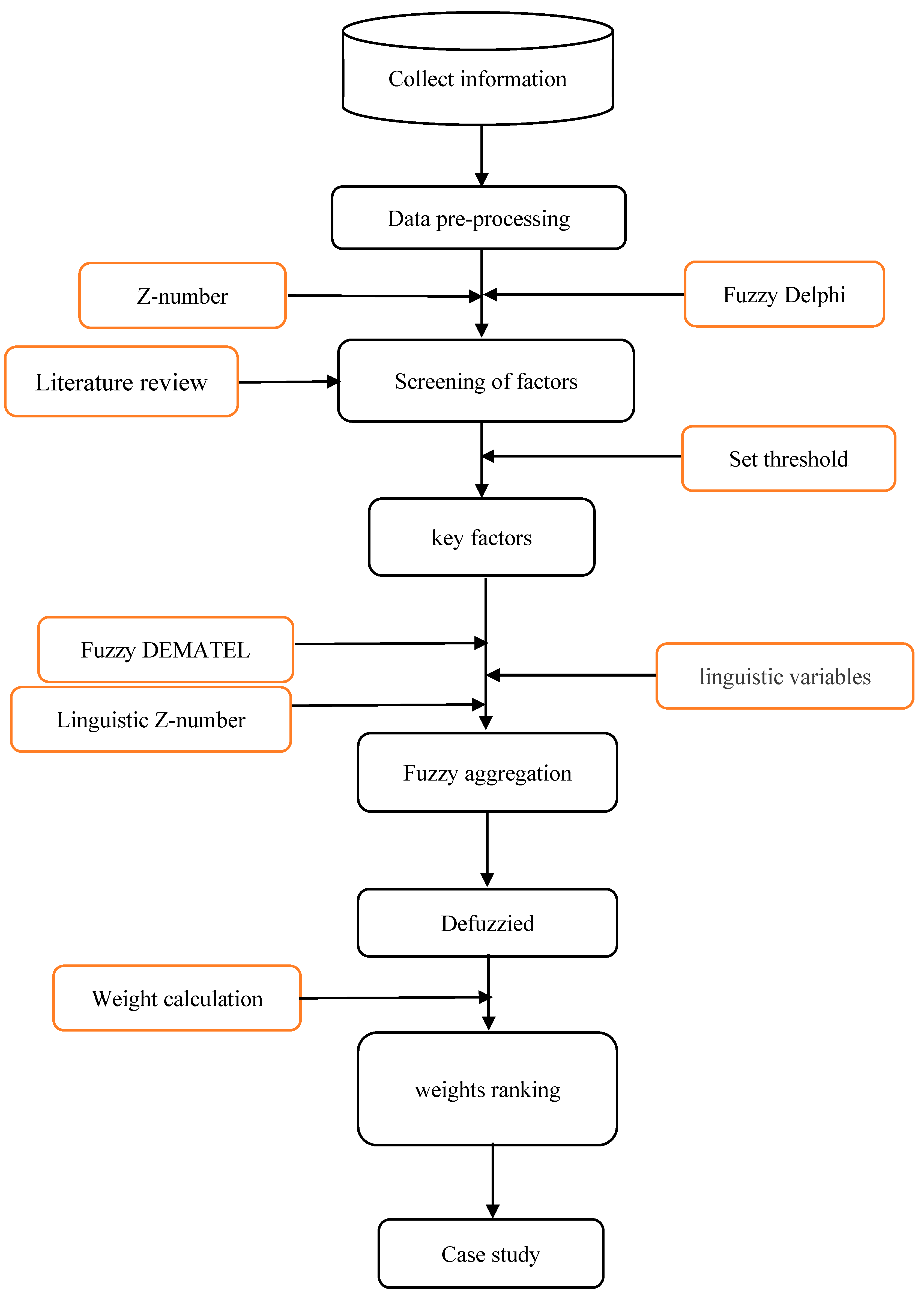
This study employs a combined approach, integrating the linguistic Z-number and the Decision-Making Trial and Evaluation Laboratory (DEMATEL) method, to examine the pivotal influencing factors associated with the integration of smart medical care into long-term care. The proposed model comprises two stages. The initial stage employs the fuzzy Delphi method [7,8] in conjunction with the linguistic Z-number to identify the pivotal influencing factors associated with the integration of smart medical care into long-term care. This is achieved through a consensus among experts and the establishment of threshold values. The second stage employs the linguistic Z-number and the DEMATEL method [9,10,11] to analyze the mutual influence degree between key influencing factors and the importance of key factors. The research process of this study is shown in Figure 3.
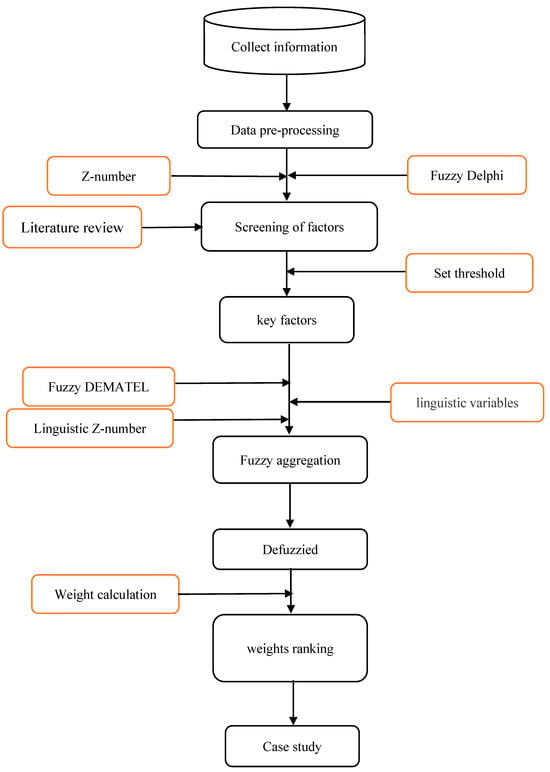
Figure 3.
The research process of this study.
3.1. Integrate Expert Opinions
This study employs the Fuzzy Delphi method and Linguistic Z-number to synthesize the opinions of experts and identify the pivotal factors for the integration of smart healthcare into long-term care. The following section outlines the steps in detail.
Step 1: Collect relevant literature and summarize the influencing factors .
Step 2: The linguistic Z-number is employed by each expert to evaluate the importance of the influencing factors. The k-th expert (k = 1, 2, …, K) assesses the importance of the i-th factor as follows:
where is the linguistic Z-number evaluation value of the importance evaluation of the i-th factor by the k-th expert. is the linguistic evaluation value of the importance of the factor i by the expert . is the degree of certainty of the importance of the factor i by the expert .
Step 3: The objective is to transform the expert’s linguistic Z-number evaluation value into a triangular fuzzy number. The centroid method should be employed in order to defuzzify into . Let us assume that is represented by the triplet . The is then converted into a triangular fuzzy number, .
Step 4: A consensus is deemed to have been reached when the opinions of each expert align with those of at least one other expert. Once all experts have reached a consensus, the triangular fuzzy numbers , which represent the importance of the i-th factor according to all experts, are integrated as follows:
where is the triangular fuzzy number of the importance of the i-th influencing factor and , , .
Step 5: The integrated expert opinions should be defuzzied. The defuzzification of the triangular fuzzy number associated with the i-th influencing factor is as follows:
where is the defuzzified value of the triangular fuzzy number .
Step 6: It is essential to identify and assess the key factors that contribute to the outcome of interest. If the threshold value of factor importance is assumed to be , then the influencing factor i is considered to be the key factor if the defuzzified value of is greater than or equal to the threshold value (). In the event that is less than the threshold value , the influencing factor i is removed.
3.2. Calculation of Key Factors Importance
The second stage is to analyze the causal relationship, influence intensity, and weight ranking between key factors through the use of linguistic Z-numbers and the Decision-Making Trial and Evaluation Laboratory (DEMATEL) method. The following section outlines the relevant steps in detail.
Step 1: It is assumed that the initial stage finds the primary factors, indexed by n (with i = 1, 2, …, n).
Step 2: The role of the expert is to evaluate the degree of influence between any two factors. The linguistic Z-number is employed by each expert to assess the extent of influence exerted by the principal factors. The degree of influence exerted by the key factor i on the factor j, as evaluated by expert , is as follows:
where represents the linguistic Z-number of the influence of the key factor i on the factor j by expert . represents the semantic evaluation value of the influence of factor i on factor j by expert . represents the degree of certainty of the degree of influence of factor i on factor j by expert .
Step 3: Defuzzify into using the centroid method. Assume that The will be converted into triangular fuzzy numbers .
Step 4: Once a consensus has been reached by the experts, the triangular fuzzy numbers provided by each expert are integrated in accordance with the following procedure:
where is the triangular fuzzy number of factor i influencing factor j, , , .
Step 5: The should be defuzzified using the centroid method. The calculation is as follows:
Step 6: A direct relationship matrix (A) is established on the basis of the degree of influence exerted by key factors, as follows:
where is the degree value of the key factor i influencing factor j.
Step 7: In accordance with the direct relationship matrix A, a normalized direct relationship matrix D is to be established as follows:
Step 8: In accordance with the principles set forth in the normalized direct relationship matrix D, the total influence relationship matrix T is to be constructed as follows:
where . The represents that the total influence value of factor i influences factor j. The is the unit matrix.
Step 9: In accordance with the total influence relationship matrix, the centrality () and causality () of factor i are to be calculated as follows:
where represents the sum of the degree to which the i-th factor affects other factors, while denotes the sum of the degree to which the i-th factor is affected by other factors. The centrality of the i-th factor, represented by (), indicates the total degree to which the i-th factor affects and is affected. It can therefore be used to demonstrate the core degree of the factor among all factors. () represents the causal degree of the i-th factor. A positive value for () indicates that the i-th factor exerts an influence on other factors. Should () be negative, this indicates that the i-th factor is affected by other factors.
The value of ( + ) represents the total degree to which factor i affects and is affected by other factors. Consequently, the larger this value is, the more important factor i is considered to be. In this study, the normalization of this value is used to express the influential weight of factor i.
Step 10: Calculate the influential weight of each factor as follows:
where represents the importance of the i-th key factor.
Step 11: Construct factors causation
In accordance with the total influence relationship matrix (T), the threshold values (, ) for calculating the degree of influence are as follows:
In order to construct the causal relationship matrix of the factors (C), it is first necessary to derive the total influence relationship matrix (T) and the threshold value () of the influenced degree. The causal relationship matrix of the factors (C) is as follows:
where
A value of indicates that factor i exerts an influence on factor j. Conversely, a value of signifies that factor i does not exert any influence on factor j. The causal relationship matrix (C) can be employed to construct a causal relationship diagram encompassing all factors.
4. Empirical Analysis
4.1. Screening Key Influencing Factors
4.1.1. Summary of Influencing Factors
Based on the analysis of the existing literature and the subsequent discussion, this study presents a summary of the 18 key factors that have been identified as influencing the introduction of smart medical technology into long-term care, as illustrated in Table 2. The significance of each influencing factor is illustrated in Table 3.
Table 2.
Influencing factors.
Table 3.
The significance of each influencing factor.
4.1.2. Assessment of Factor Importance
In this study, the evaluation was conducted by a panel of 12 experts. As the evaluation data from three experts did not align with the responses of the other experts, the data from nine experts was ultimately adopted for analysis following the deletion of the data from the three experts. The nine experts were drawn from a range of industry categories, with a particular focus on the education and healthcare sectors. The experts held positions as either head of unit or professionals, and the majority of the companies they represented had more than 1000 employees. The relevant information pertaining to the experts is presented in Table 4.
Table 4.
Background information of experts.
Each expert employed the linguistic Z-number to assign an evaluation value for the importance of the 18 factors in question. The triangular fuzzy number that corresponds to the linguistic Z-number is presented in Table 5. The linguistic Z-number evaluation values assigned by all experts are presented in Table 6, Table 7 and Table 8.
Table 5.
Linguistic variables of importance and certainty.
Table 6.
The linguistic Z-number evaluations of experts 1 to 3.
Table 7.
The linguistic Z-number evaluations of experts 4 to 6.
Table 8.
The linguistic Z-number evaluations of experts 7 to 9.
4.1.3. Converting Linguistic Variables of Certainty to Crisp Values
The degree of certainty is calculated using the centroid method, which provides a crisp value. To illustrate, the linguistic variable “certainty” () of the degree of certainty is represented by the following membership function:
The calculation result using the centroid method is:
4.1.4. Integration of All Expert Evaluations
The linguistic Z-number values of each factor, as determined by nine experts, were converted into triangular fuzzy numbers after consensus was reached among the experts. The fuzzy Delphi method was employed for the integration of the evaluation values provided by the nine experts. The integrated triangular fuzzy numbers for each influencing factor, along with their defuzzification results, are presented in Table 9.
Table 9.
Integrated triangular fuzzy numbers and defuzzied values.
4.1.5. Screening Evaluation Factors
When filtering factors, it is essential to set an appropriate threshold range. If the threshold is set too high, the number of factors to be filtered will be insufficiently representative. Conversely, if the threshold is set too low, the number of factors to be filtered will be excessive, thereby preventing the identification of the most important factors. In this study, we propose that at least half of the number of factors should be retained, and therefore the importance threshold is set at 0.68, and subsequently identified nine factors as detailed in Table 10.
Table 10.
Key influencing factors.
4.2. Case Analysis
In order to gain insight into the key influencing factors, this study conducted a case analysis of two long-term care institutions, with a view to comparing the differences between the two.
4.2.1. Institution A
Institution A is situated in a northern city in Taiwan. The institution was established in 1998 and currently employs approximately 500 individuals. The service is designed to meet the needs of children, individuals with physical and mental disabilities, and the elderly. It offers direct and professional social services to a range of target groups. The institution’s principal services encompass home-based care for the elderly and community integration initiatives. Long-term care services encompass both home services and community-integrated services. The following analysis of Institution A identifies the key factors:
- (1)
- Assessment of the degree of mutual influence between factorsIn order to evaluate Institution A, this study invited three experts to utilize the linguistic Z-number, as demonstrated in Table 11. The results of the evaluation conducted by the three experts on the degree of influence between factors are presented in Table 12, Table 13 and Table 14.
Table 11. Linguistic variables of influence and certainty.
Table 12. Evaluations of linguistic Z-number by expert 1 for Institution A.
Table 13. Evaluations of linguistic Z-number by expert 2 for Institution A.
Table 14. Evaluations of linguistic Z-number by expert 3 for Institution A.
- (2)
- The outcomes of the integration of the triangular fuzzy number assessments provided by the three experts are presented in Table 15.
Table 15. The integrated evaluations by three experts of Institution A.
- (3)
- The direct relationship matrix of Institution A is presented in Table 16.
Table 16. Direct relationship matrix of Institution A.
- (4)
- The normalized direct relationship matrix of Institution A is presented in Table 17.
Table 17. Normalized direct relationship matrix of Institution A.
- (5)
- The total influence relationship matrix (T) of Institution A is presented in Table 18.
Table 18. Total influence relationship matrix of Institution A.
- (6)
- The factor weights and rankings of Institution A, as derived from the total influence relationship matrix, are presented in Table 19.
Table 19. The influential weights and ranking of key factors of Institution A.
- (7)
- Causation of key factors for Institution A
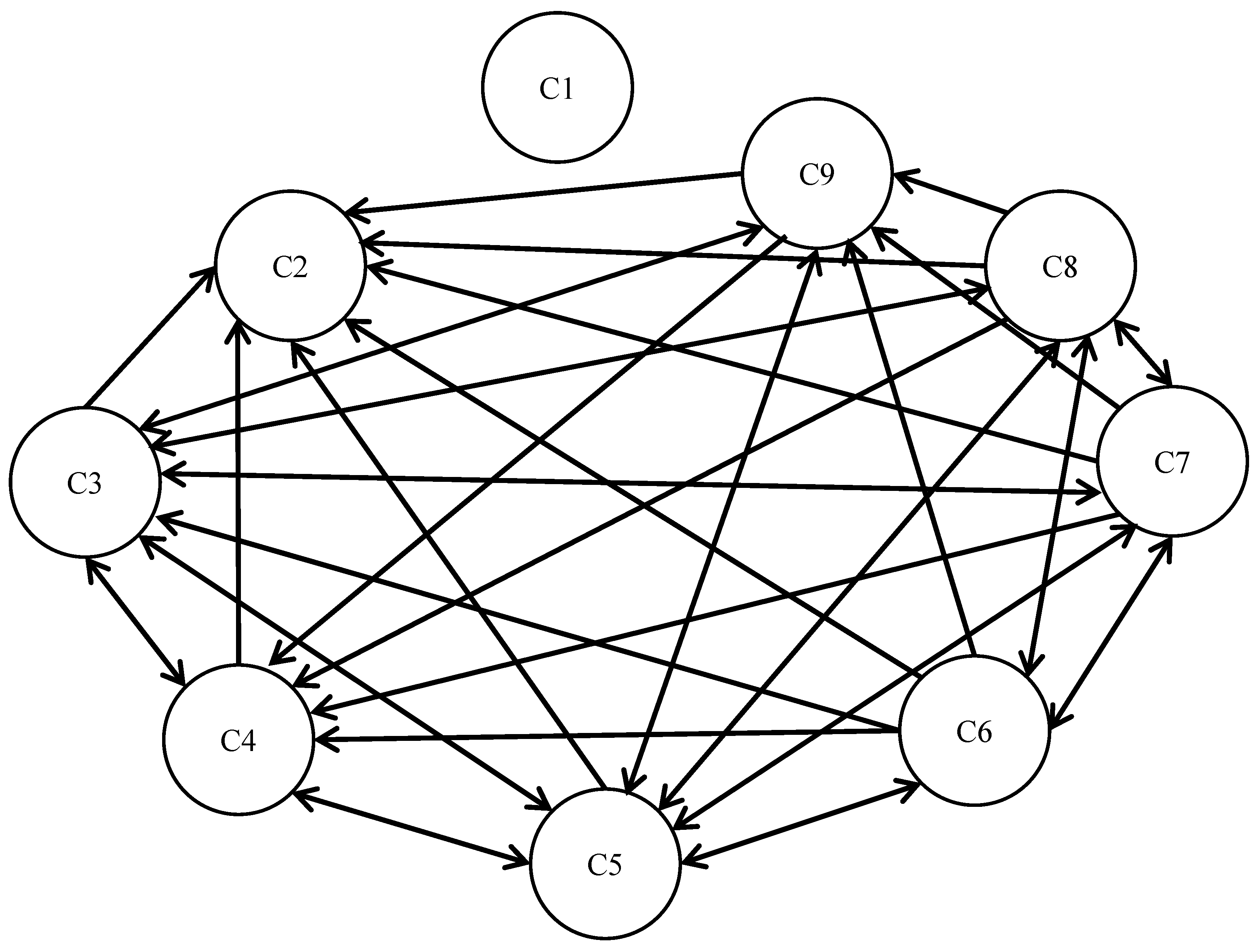
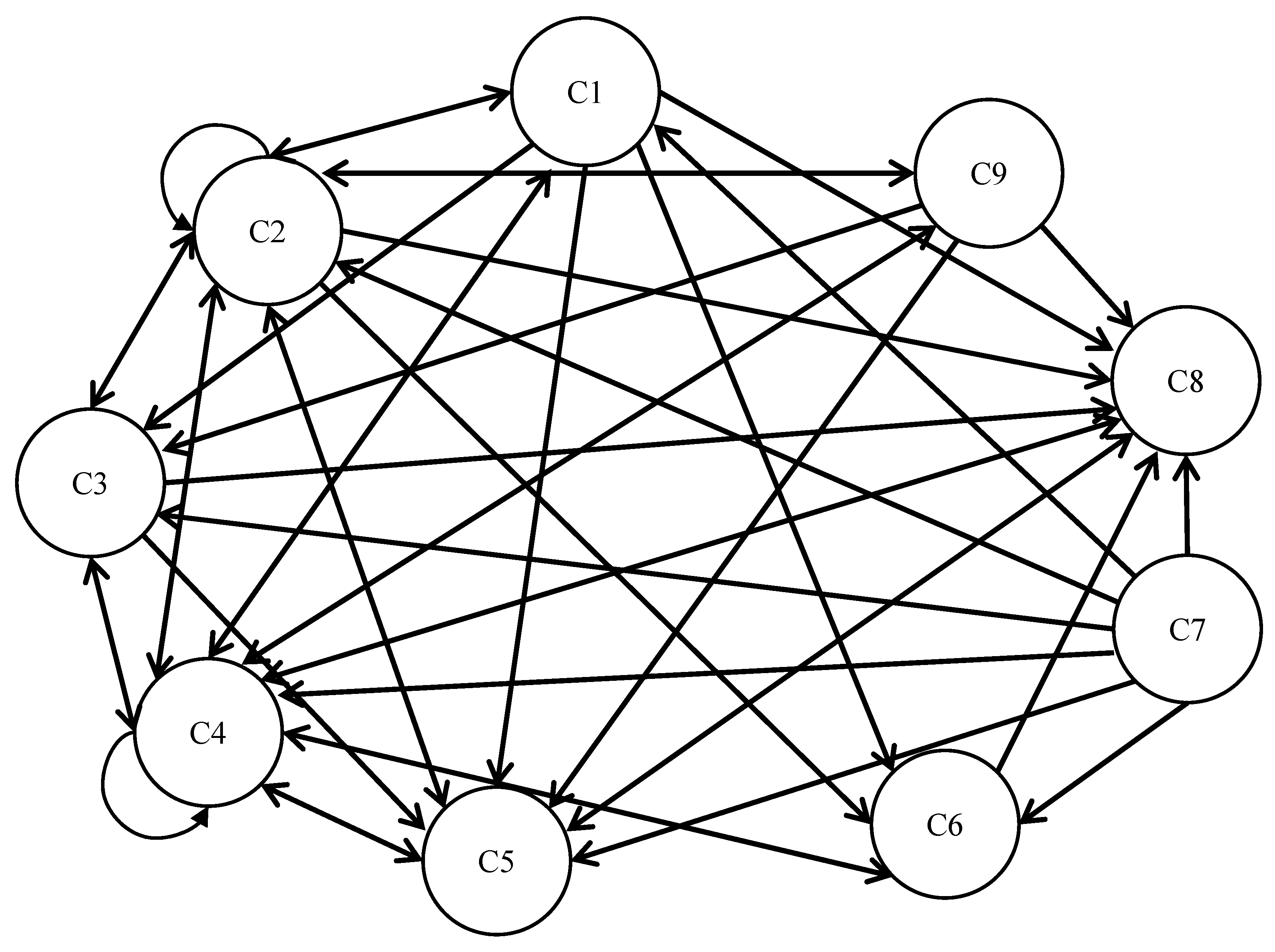
In accordance with the total impact relationship matrix and the threshold value , the causal relationship matrix can be derived as illustrated in Table 20. The causal relationship matrix in Table 20 allows the identification of the causal relationships between key factors, as illustrated in Figure 4. As illustrated in Figure 4, the global positioning system (C3), smart clinics and urgent care centers (C4), telemedicine (C5), the Internet of Things (C6), smart medical talent acquisition (C7), and electronic medical records (C8) are of particular significance. The Internet of Things (C6), smart medical talent acquisition (C7), and electronic medical records (C8) are identified as “influencing factors”. Three-dimensional printing technology (C1), sensors (C2), global positioning systems (C3), smart clinics and urgent care centers (C4), telemedicine (C5), and assistive smart wheelchairs (C9) are classified as “influenced factors”.
Table 20.
Causal matrix of Institution A with .
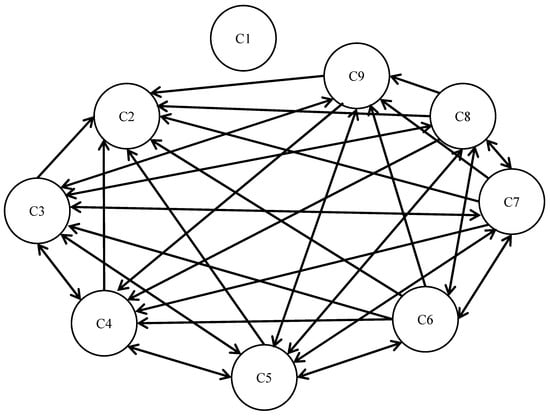
Figure 4.
Causal relationship of key factors of Institution A with .
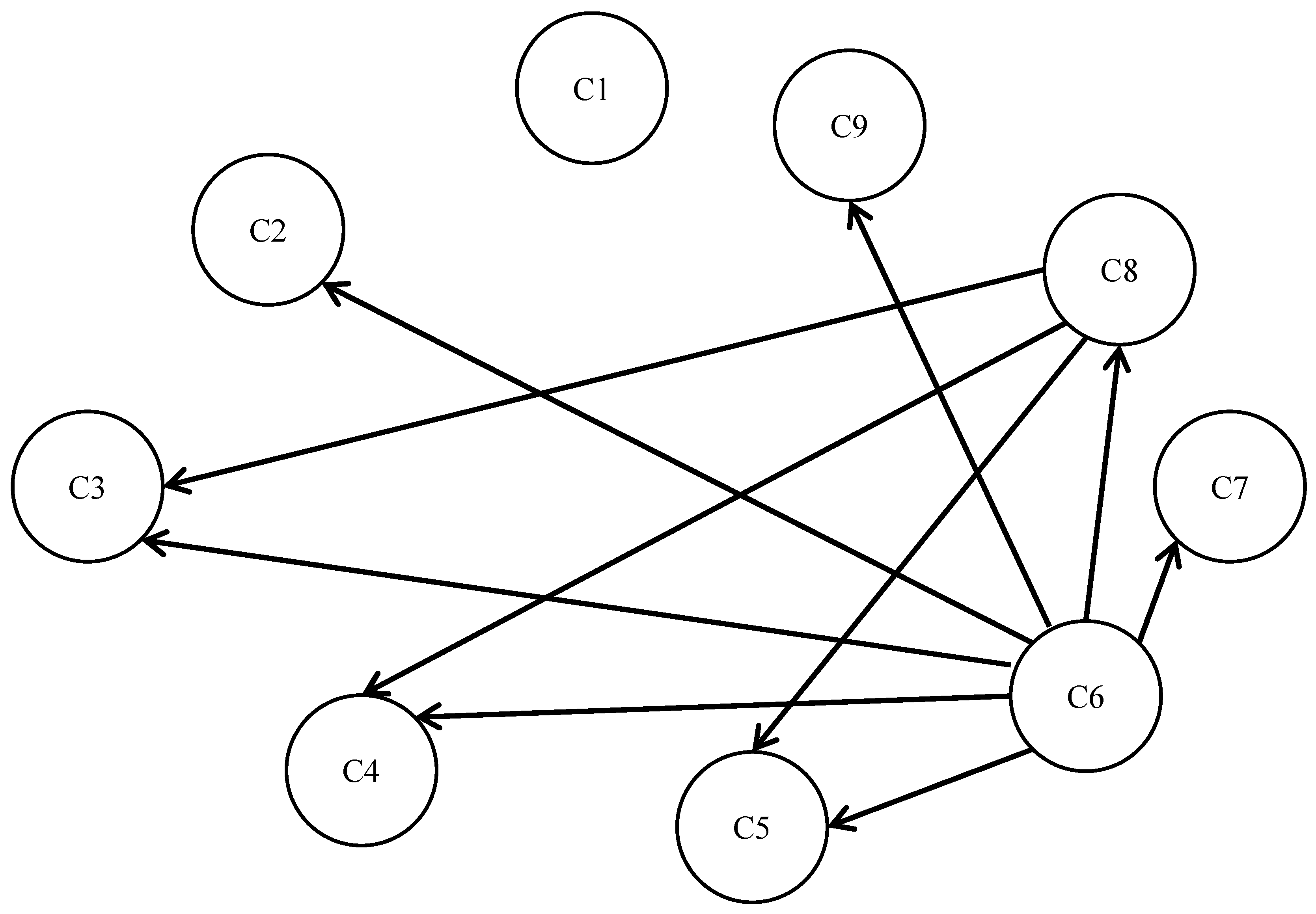
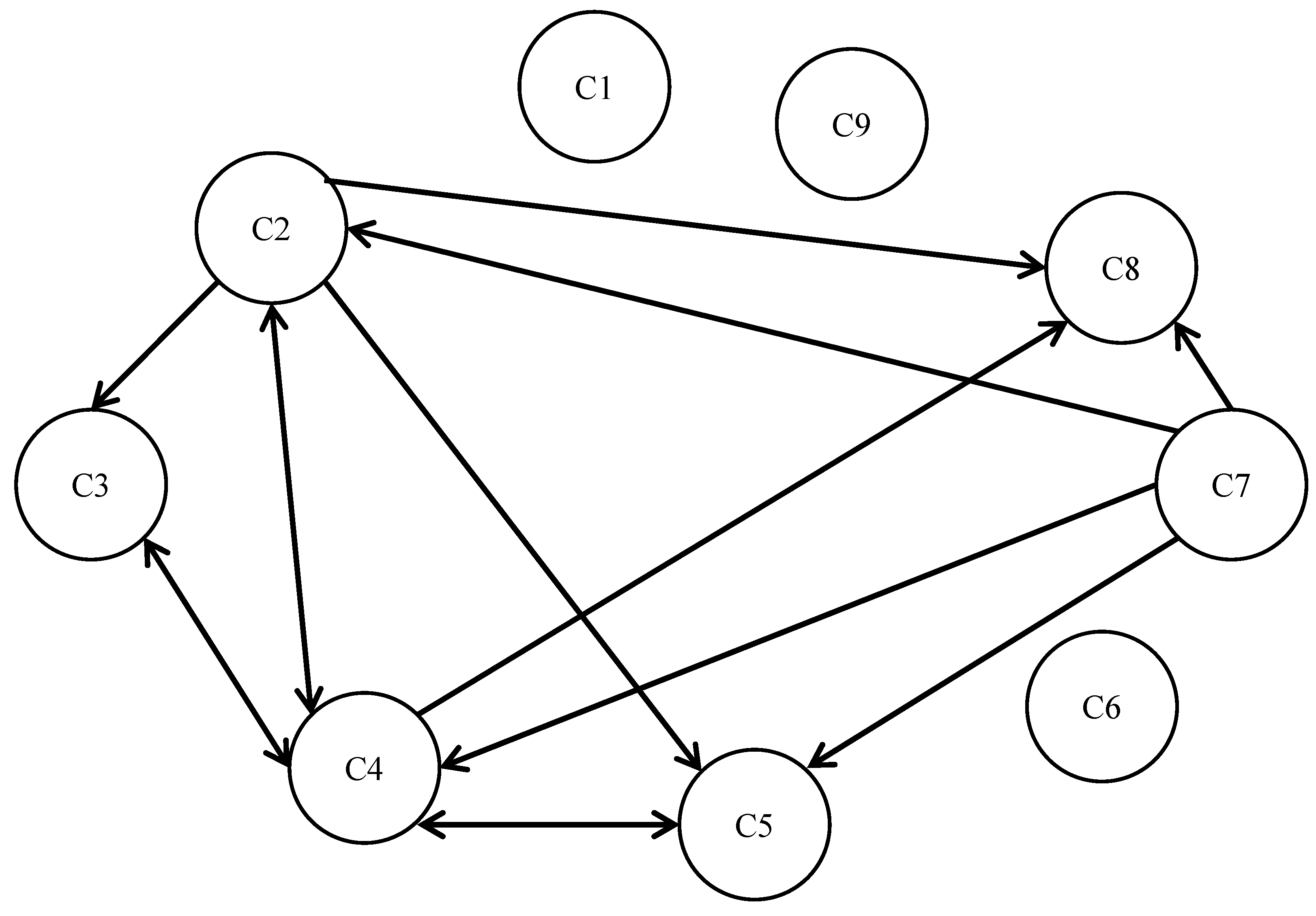
In accordance with the total impact relationship matrix and the threshold value , the causal relationship matrix can be derived as illustrated in Table 21. The causal relationship matrix in Table 21 allows the identification of the causal relationships between key factors, as illustrated in Figure 5. As illustrated in Figure 5, the Internet of Things (C6), smart medical talent acquisition (C7), and electronic medical records (C8) are identified as “influencing factors”. The sensors (C2), global positioning systems (C3), smart clinics and urgent care centers (C4), telemedicine (C5), smart medical talent acquisition (C7), and assistive smart wheelchairs (C9) are classified as “influenced factors”.
Table 21.
Causal matrix of Institution A with .
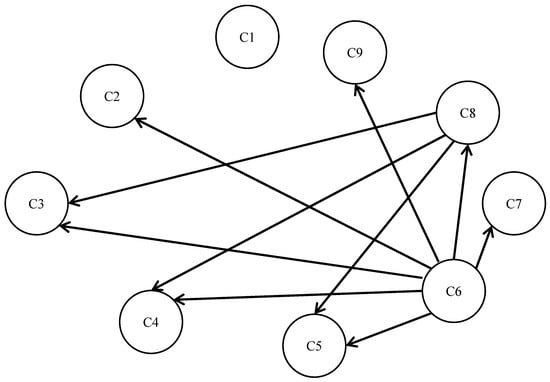
Figure 5.
Causal relationship of key factors of Institution A with .
4.2.2. Institution B
Institution B is situated in the central region of Taiwan. The institution was established in 2010 and has a workforce of fewer than 200 employees. The organization is closely aligned with the needs of the community, offering a diverse range of services. By providing comprehensive services within the community, the organization implements the community care concept of “local aging”. The service business encompasses respite care, dementia centers, daycare, case management, community support, welfare services, and long-term care, with the objective of alleviating family care pressure and promoting social welfare development. A similar calculation process was employed in the case analysis, which is presented below:
- (1)
- The total influence relationship matrix (T) of Institution B is presented in Table 22.
Table 22. Total influence relationship matrix of Institution B.
- (2)
- The relative importance of the key factors of Institution B is determined through the calculation of the total influence relationship matrix, as illustrated in Table 23.
Table 23. The influential weights and ranking of key factors of Institution B.
As indicated in Table 23, the “smart clinics and urgent care centers (C4)” represent the most significant key factor, whereas the “Internet of Things (C6)” is identified as the least crucial for Institution B.
The causal relationship matrix can be obtained based on the total influence relationship matrix and threshold value , as illustrated in Table 24. Figure 6 illustrates the causal relationships between the key factors of Institution B. As illustrated in Figure 6, the six factors, namely sensors (C2), global positioning systems (C3), smart clinics and urgent care centers (C4), telemedicine (C5), the Internet of Things (C6), and electronic medical records (C8), are of particular significance. The four factors, namely 3D printing technology (C1), sensors (C2), smart medical talent acquisition (C7), and assistive smart wheelchairs (C9), can be classified as “influencing factors”. The five factors, namely global positioning systems (C3), smart clinics and urgent care centers (C4), telemedicine (C5), the Internet of Things (C6), and electronic medical records (C8), are classified as “affected factors”.
Table 24.
Causal matrix of Institution B with .
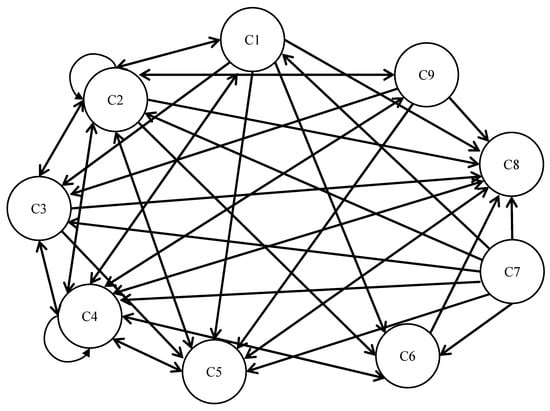
Figure 6.
Causal relationship of key factors of Institution B with .
The causal relationship matrix can be obtained based on the total influence relationship matrix and threshold value , as illustrated in Table 25. Figure 7 illustrates the causal relationships between the key factors of Institution B. As illustrated in Figure 7, smart medical talent acquisition (C7) can be classified as “influencing factors”. The five factors, namely sensors (C2), global positioning systems (C3), smart clinics and urgent care centers (C4), telemedicine (C5), and electronic medical records (C8), are classified as “affected factors”.
Table 25.
Causal matrix of Institution B with .
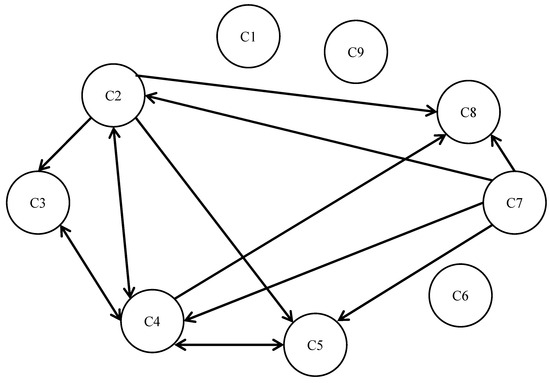
Figure 7.
Causal relationship of key factors of Institution B with .
Table 19 and Table 23 illustrate that there is a discrepancy in the weighting of the influential factors for Institution A and Institution B. The weighting of the critical factors for Institution A and Institution B is presented in Table 26. Table 26 also depicts the rankings and contrasts in the weights of the principal factors for Institution A and Institution B.
Table 26.
Ranking and difference in critical factor weights for two institutions.
4.3. Management Implications
The results of the analysis indicate that Institution A considers the “Internet of Things (C6)” to be the most significant factor influencing the integration of smart medical care into long-term care, whereas Institution B deems the “smart clinics and urgent care centers (C4)” to be the most crucial element.
- (1)
- Institution AThe data indicates that when implementing smart healthcare in Institution A, it is essential to consider factors such as the integration of hardware with long-term care and the attitudes of the staff. The following recommendations are proposed for Institution A with regard to the implementation of smart healthcare in long-term care:
- (i)
- By facilitating collaborative endeavors and fostering inter-institutional partnerships with entities specializing in 3D printing technology, long-term caregivers and employees can gain a deeper comprehension of the underlying principles of 3D printing, thereby reducing their sense of rejection.
- (ii)
- It would be beneficial to arrange training courses for employees to gain hands-on experience with smart assistive devices, such as smart wheelchairs and smart medicine boxes. This would help them to understand the advantages and challenges of the hardware.
- (iii)
- It would be beneficial to collaborate with hospitals or universities to acquire the requisite smart medical talents and thereby improve the feasibility of introducing smart medical care.
- (2)
- Institution BThe data indicates that when implementing smart healthcare in Institution B, it is essential to consider factors such as the acceptance of information technology and the integration of hardware with long-term care. The following recommendations are proposed for Institution B about the implementation of smart healthcare in long-term care:
- (1)
- It would be beneficial to establish an information department and to recruit additional personnel with information capabilities, with the objective of enhancing the information capabilities of the institution.
- (2)
- It would be beneficial to pilot short-term smart care services, such as obtaining the vital signs and status of the caregiver through the use of wearable devices, in order to gain a deeper understanding of the level of acceptance among both staff and care recipients.
- (3)
- It is recommended that hospitals collaborate with one another in order to mitigate the adverse effects of inadequate resources through the utilization of AI-based diagnostic techniques and robotic assistance.
Given that Institution A is an institution with a superior organizational structure and a higher level of information, the technical factors are accorded greater importance. Institution B is situated in a less favorable geographical location and has access to fewer resources, which makes the importance of medical factors more significant. In light of the aforementioned analysis, it can be concluded that the key factors for both institutions are the “global positioning system (C3)”, “telemedicine (C5)”, and “electronic medical records (C8)”. It can thus be concluded that the organizational structure and scale of long-term care institutions are disparate, and that the medical treatment and protection measures for caregivers remain the pivotal factors recognized by both institutions.
5. Conclusions
In light of the accelerated advancement of information technology, the integration of “smart medicine” into the domain of “long-term care” to enhance the quality of care has emerged as a pivotal concern. A number of factors influence the successful implementation of smart medicine in long-term care, and the assessment of these factors by experts is inherently subjective and ambiguous. Accordingly, this study employs fuzzy set theory and the linguistic Z-number as a foundation for the analysis of the pivotal factors influencing the integration of smart healthcare into long-term care.
This study is based on fuzzy set theory and employs the fuzzy Delphi method in conjunction with the linguistic Z-number to identify nine pivotal factors. The DEMATEL method and the linguistic Z-number method are employed to calculate the weights of the key influencing factors, after which a systematic analysis model is proposed for exploring the importance of different institutions for the key influencing factors of the introduction of smart medical care in long-term care. This study makes the following main contributions: (1) The key influencing factors of the introduction of smart medicine into long-term care can be effectively identified through the fuzzy Delphi method, which can then be used to develop technical measurement items for the introduction of smart medicine into long-term care institutions. (2) The DEMATEL method allows the relevance and importance of the key factors affecting the introduction of smart medicine into long-term care to be effectively grasped. (3) In consideration of the inherent fuzziness of expert opinions, a two-stage systematic analysis model is proposed using linguistic variables, which can effectively assist long-term care institutions in analyzing the introduction of smart medical technologies and equipment.
The principal constraints of this study are the lack of straightforward access to expert assessment data, the considerable number of variables influencing the integration of smart healthcare into long-term care (LTC) institutions, and the high degree of diversity within LTC institutions. These limitations can be investigated in greater depth in future empirical studies, thus enhancing the practical value of the findings.
Author Contributions
Conceptualization, C.-T.C. and C.-C.C.; methodology, C.-T.C.; validation, C.-T.C. and C.-C.C.; formal analysis, C.-T.C.; investigation, C.-C.C.; data curation, C.-C.C.; writing—original draft preparation, C.-T.C.; writing—review and editing, C.-T.C.; visualization, C.-C.C.; funding acquisition, C.-T.C. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported partially by the Taiwan Ministry of Science and Technology under project No. “MOST 111-2410-H-239-011-MY2”.
Data Availability Statement
No new data were created.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stallard, E. International Encyclopedia of Public Health Long Term Care for Aging Populations; Springer: Berlin/Heidelberg, Germany, 2017; pp. 447–458. [Google Scholar]
- Loveys, K.; Prina, M.; Axford, C.; Domènec, Ò.R.; Weng, W.; Broadbent, E.; Pujari, S.; Jang, H.; Han, Z.A.; Thiyagarajan, J.A. Artificial intelligence for older people receiving long-term care: A systematic review of acceptability and effectiveness studies. Lancet Healthy Longev. 2022, 3, 286–297. [Google Scholar] [CrossRef] [PubMed]
- Oderanti, F.O.; Li, F.; Cubric, M.; Shi, X. Business models for sustainable commercialization of digital healthcare (eHealth) innovations for an increasingly aging population. Technol. Forecast. Soc. Change 2021, 171, 120969. [Google Scholar] [CrossRef]
- Chen, W.H.; Chang, K.C.; Liou, H.H.; Chen, H.S.; Hwang, J.J.; Huang, W.L. The psychopathology and happiness of the older adults in Yunlin, Taiwan: What do we need for long-term care service? J. Formos. Med. Assoc. 2022, 121, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zhu, H.; Wu, C.K.; Koo, C.H.; Tsang, Y.T.; Liu, Y.; Chi, H.R.; Tsang, K.F. Smart healthcare in the era of internet-of-things. IEEE Consum. Electron. Mag. 2019, 8, 26–30. [Google Scholar] [CrossRef]
- Ding, X.F.; Zhu, L.X.; Lu, M.S.; Wang, Q.; Feng, Y.Q. A novel linguistic Z-number QUALIFLEX method and its application to large group emergency decision making. Sci. Program. 2020, 2020, 1–13. [Google Scholar] [CrossRef]
- Dawood, K.A.; Sharif, K.Y.; Ghani, A.A.; Zulzalil, H.; Zaidan, A.A.; Zaidan, B.B. Towards a unified criteria model for usability evaluation in the context of open source software based on a fuzzy Delphi method. Inf. Softw. Technol. 2021, 130, 1–30. [Google Scholar] [CrossRef]
- Marlina, E.; Hidayanto, A.N.; Purwandari, B. Towards a model of research data management readiness in Indonesian context: An investigation of factors and indicators through the fuzzy Delphi method. Libr. Inf. Sci. Res. 2022, 101141, 1–12. [Google Scholar] [CrossRef]
- Hsu, W.C.J.; Liou, J.J.; Lo, H.W. A group decision-making approach for exploring trends in the development of the healthcare industry in Taiwan. Decis. Support Syst. 2021, 141, 113447. [Google Scholar] [CrossRef]
- Jiang, S.; Shi, H.; Lin, W.; Liu, H.C. A large group linguistic Z-DEMATEL approach for identifying key performance indicators in hospital performance management. Appl. Soft Comput. 2020, 86, 105900. [Google Scholar] [CrossRef]
- Liu, Y.; Wood, L.C.; Venkatesh, V.; Zhang, A.; Farooque, M. Barriers to sustainable food consumption and production in China: A fuzzy DEMATEL analysis from a circular economy perspective. Sustain. Prod. Consum. 2021, 28, 1114–1129. [Google Scholar] [CrossRef]
- Tchouaket, E.; Kilpatrick, K.; Jabbour, M. Effectiveness for introducing nurse practitioners in six long-term care facilities in Québec, Canada: A cost-savings analysis. Nurs. Outlook 2020, 68, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Giesbrecht, M.; Stajduhar, K.I.; Cloutier, D.; Dujela, C. We are to be like machines…fill the bed before it gets cold. Exploring the emotional geographies of healthcare providers caring for dying residents in long-term care facilities. Soc. Sci. Med. 2021, 272, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shuo, T.; Wenbo, Y.; Jehane ML, G.; Peng, W.; Wei, H.; Zhewei, Y. Smart healthcare: Making medical care more intelligent. Glob. Health J. 2019, 3, 62–65. [Google Scholar]
- World Health Organization. Long-Term Care. Available online: https://reurl.cc/3Y1gKV (accessed on 18 January 2022).
- Lukkien, D.R.; Nap, H.H.; Buimer, H.P.; Peine, A.; Boon, W.P.; Ket, J.C.; Minkman, M.; Moors, E.H. Toward responsible artificial intelligence in long-term care: A scoping review on practical approaches. Gerontologist 2021, 63, 1–14. [Google Scholar] [CrossRef]
- Legato, P.; Mazza, R.M.; Fortino, G. A multi-level simulation-based optimization framework for IoT-enabled elderly care systems. Simul. Model. Pract. Theory 2022, 114, 102420. [Google Scholar] [CrossRef]
- Rubeis, G. The disruptive power of artificial intelligence. Ethical aspects of gerontechnology in elderly care. Arch. Gerontol. Geriatr. 2020, 91, 104186. [Google Scholar] [CrossRef]
- Leu, F.Y.; Chiang, P.J.; Susanto, H.; Hung, R.T.; Huang, H.L. Mobile physiological sensor cloud system for long-term care. Internet Things 2020, 11, 100209. [Google Scholar] [CrossRef]
- Wu, B.; Pi, Y.; Chen, J. Privacy Protection of Medical Service Data Based on Blockchain and Artificial Intelligence in the Era of Smart Medical Care. Wirel. Commun. Mob. Comput. 2022, 2022, 1–10. [Google Scholar] [CrossRef]
- Nguyen, H.H.; Mirza, F.; Naeem, M.A.; Nguyen, M. A Review on IoT Healthcare Monitoring Applications and a Vision for Transforming Sensor Data into Real-Time Clinical Feedback. In Proceedings of the IEEE 21st International Conference on Computer Supported Cooperative Work in Design, Wellington, New Zealand, 26–28 April 2017; pp. 257–262. [Google Scholar]
- Wang, L.; Gu, D.; Wu, B. Technology-Enabled Long-Term Care Services and Supports (T-eLTCSS) in Home Settings. In Encyclopedia of Gerontology and Population Aging; Springer International Publishing: Cham, Switzerland, 2019; pp. 1–8. [Google Scholar]
- Hussain, A.; Wenbi, R.; Da Silva, A.L.; Nadher, M.; Mudhish, M. Health and emergency-care platform for the elderly and disabled people in the smart city. J. Syst. Softw. 2015, 110, 253–263. [Google Scholar] [CrossRef]
- Kruse, C.S.; Mileski, M.; Vijaykumar, A.G.; Viswanathan, S.V.; Suskandla, U.; Chidambaram, Y. Impact of electronic health records on long-term care facilities: Systematic review. JMIR Med. Inform. 2017, 5, 1–9. [Google Scholar] [CrossRef]
- Chou, H.M. A collaborative framework with artificial intelligence for long-term care. IEEE Access 2020, 8, 1–10. [Google Scholar] [CrossRef]
- Haddara, M.; Staaby, A. RFID applications and adoptions in healthcare: A review on patient safety. Procedia Comput. Sci. 2018, 138, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Ganesh, D.; Seshadri, G.; Sokkanarayanan, S.; Rajan, S.; Sathiyanarayanan, M. Iot-Based Google Duplex Artificial Intelligence Solution for Elderly Care. In Proceedings of the 2019 International Conference on Contemporary Computing and Informatics, Singapore, 12–14 December 2019; pp. 1–7. [Google Scholar]
- Heo, S.P.; Jeong, S. Internet of Things in the Bathroom: Smart Health-Monitoring Bidet System. Math. Probl. Eng. 2021, 2021, 1–9. [Google Scholar] [CrossRef]
- Ekanayaka, D.; Cooray, O.; Madhusanka, N.; Ranasinghe, H.; Priyanayana, S.; Buddhika, A.G.; Jayasekara, P. Elderly Supportive Intelligent Wheelchair. In Proceedings of the 2019 Moratuwa Engineering Research Conference, Moratuwa, Sri Lanka, 3–5 July 2019; pp. 627–632. [Google Scholar]
- Wang, J.; Ding, D.; Liu, O.; Li, M. A synthetic method for knowledge management performance evaluation based on triangular fuzzy number and group support systems. Appl. Soft Comput. 2016, 39, 11–20. [Google Scholar] [CrossRef]
- Zadeh, L.A. The concept of a linguistic variable and its application to approximate reasoning—I. Inf. Sci. 1975, 8, 199–249. [Google Scholar] [CrossRef]
- Nirmala, G.; Uthra, G. AHP based on triangular intuitionistic fuzzy number and its application to supplier selection problem. Mater. Today Proc. 2019, 16, 987–993. [Google Scholar] [CrossRef]
- Gao, S.; Zhang, Z.; Cao, C. Multiplication operation on fuzzy numbers. J. Softw. 2009, 4, 331–338. [Google Scholar] [CrossRef]
- Gani, A.N.; Assarudeen, S.M. A new operation on triangular fuzzy number for solving fuzzy linear programming problem. Appl. Math. Sci. 2012, 6, 525–532. [Google Scholar]
- Van Leekwijck, W.; Kerre, E.E. Defuzzification: Criteria and classification. Fuzzy Sets Syst. 1999, 108, 159–178. [Google Scholar] [CrossRef]
- Zadeh, L.A. A Note on a Z-Number. J. Inf. Sci. 2011, 181, 2923–2932. [Google Scholar] [CrossRef]
- Aliev, R.A.; Pedrycz, W.; Huseynov, O.H. Functions defined on a set of Z-numbers. Inf. Sci. 2018, 423, 353–375. [Google Scholar] [CrossRef]
- Azadeh, A.; Saberi, M.; Atashbar, N.Z.; Chang, E.; Pazhoheshfar, P. Z-AHP: A Z-Number Extension of Fuzzy Analytical Hierarchy Process. In Proceedings of the 2013 7th IEEE International Conference on Digital Ecosystems and Technologies (DEST), Menlo Park, CA, USA, 24–26 July 2013; pp. 141–147. [Google Scholar]
- Aboutorab, H.; Saberi, M.; Asadabadi, M.R.; Hussain, O.; Chang, E. ZBWM: The Z-number extension of best worst method and its application for supplier development. Expert Syst. Appl. 2018, 107, 115–125. [Google Scholar] [CrossRef]
- Lawnik, M.; Krakowczyk, J.; Banasik, A. Fuzzy Delphi method with Z-numbers. Commun. Comput. Inf. Sci. 2019, 1078, 24–32. [Google Scholar]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).