Abstract
Antenatal care (ANC) is essential in maternal and child health since it provides care to pregnant women from conception through to labour in order to ensure a safe pregnancy and childbirth. In recent years, mobile health (mHealth) interventions have emerged as a promising solution to improve maternal and child health outcomes in low- and middle-income countries (LMICs). The present study aimed to conduct a systematic review and meta-analysis of trials to evaluate the effectiveness of mHealth interventions to monitor prenatal care among pregnant women in LMICs. A systematic literature review was conducted using the databases CINHAL, Embase, MEDLINE, and PsycINFO on the effectiveness of mHealth interventions in monitoring the antenatal care of pregnant women. The study selection, data extraction of the included articles, and quality appraisal were assessed. Our study included six studies considering 7886 participants. All articles were from low- and middle-income countries (LMICs). Antenatal mothers who used a mobile health intervention were more likely (RR = 1.66, 95%CI = 1.07–2.58, I2 = 98%) to attend ANC check-ups when compared with the women who did not use any mobile health applications or did not receive any short message services. mHealth technologies are being utilised more and more to increase care accessibility and improve maternal and fetal health. Policymakers should prioritise the integration of mHealth interventions into maternal healthcare services in LMICs, ensuring that they are cost-effective, accessible, and sustainable and that healthcare workers are trained to deliver these interventions effectively.
1. Introduction
Despite progress in reducing global maternal mortality, it remains unacceptably high, particularly in low- and middle-income countries (LMICs) [1]. LMICs are defined as those with a GNI per capita between USD 1036 and USD 4045 according to the World Bank. Efforts towards achieving Sustainable Development Goal (SDG) 3.1, aimed at reducing maternal mortality, have fallen short of expectations due to many factors. These include inadequate quality of care, insufficient access to family planning, disparities in socioeconomic status and race/ethnicity, inadequate allocation of national resources, and inadequate health system infrastructure [2]. Antenatal care (ANC) is critical in maternal and child health by providing care to pregnant women from conception until labour to ensure a healthy pregnancy and childbirth. The World Health Organization (WHO) recommends that pregnant women receive at least eight antenatal care contacts, which include a range of services such as physical examinations, laboratory tests, health education, and counselling [3,4]. Antenatal care (ANC) is beneficial in promoting full-term births with average birth weight [5].
Consequently, there is an immediate requirement for innovative and efficient measures to enhance the well-being and survival of both mothers and infants [6]. According to the WHO, 94% of maternal deaths occur in LMICs, with sub-Saharan Africa and South Asia accounting for most of these deaths [7]. In LMICs, only 66% of pregnant women receive the recommended four or more antenatal care visits [8]. In India, which has one of the highest maternal mortality rates in the world, only 51% of pregnant women receive the recommended number of antenatal care visits. The lack of access to adequate antenatal care contributes to maternal and infant mortality and morbidity in LMICs [9], with complications such as pre-eclampsia, postpartum haemorrhage (PPH), and sepsis leading to maternal deaths [10].
Skilled care before and after childbirth can lower complications and prevent maternal deaths [11,12]. The government has implemented various programs like Janani Suraksha Yojana (JSY), Janani Shishu Suraksha Karyakram (JSSK), Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA), and LaQshya to improve maternal and child health care. Various IEC materials, such as training packages, manuals, booklets, and videos, have been created to enhance the effectiveness of these programs, and capacity-building programs like Skilled Attendance at Birth and DAKSHATA have also been implemented [13]. In recent years mobile health (mHealth) interventions have emerged as a promising solution to improve maternal and child health outcomes in LMICs [14]. mHealth solutions offer a convenient and affordable way to overcome the challenges of accessing healthcare in LMICs. They can benefit pregnant women in remote and rural areas by enabling online/telephonic consultations, referrals, and appointment scheduling with community health workers. Furthermore, mHealth tools can aid in data collection and maintaining accurate health records [15,16].
Several mHealth interventions have been developed for antenatal care in LMICs, which use mobile devices to send reminders, educate pregnant women, and monitor their health status [17,18]. Studies show that text messaging and mobile phone-based interventions have successfully enhanced access to antenatal care and improved maternal and neonatal health outcomes in LMICs, reducing the incidence of stillbirths and neonatal mortality [19,20].
Mobile health (mHealth) interventions have been proposed to improve antenatal care access and quality in LMICs. The mHealth interventions used are short message service (SMS), voice messaging, notification alerts through a mobile application, and IVRS (interactive voice response system). Some trials have been conducted in countries among pregnant women regarding their development of knowledge through mobile health technologies to improve their prenatal healthcare. Therefore, to make noticeable policy changes with a compilation of individual studies, the present study aimed to conduct a systematic review and meta-analysis of trials to evaluate the effectiveness of mHealth interventions to monitor prenatal care among pregnant women in LMICs.
2. Materials and Methods
2.1. Criteria for Considering Studies for the Review
- Types of studies—All published randomised, quasi-experimental, and cluster randomised trials were included in this analysis. After making an unsuccessful effort to contact the study author for more information, studies reported in abstract form, without adequate information on study methods, or where the findings were ambiguous were excluded. This systematic analysis excluded studies involving case reports, case studies, editorials, perspectives, literature reviews, conference abstracts, observational studies, commentaries, and studies published in languages other than English.
The inclusion criteria were peer-reviewed articles, published in the English language, published studies conducted in LMICs, published randomised, quasi-experimental, and cluster randomised trials.
The exclusion criteria were observational studies, literature reviews, case reports, meta-analyses, and systematic reviews.
- b.
- Types of participants—Pregnant women (from the first trimester to the third trimester) (up to delivery) in LMICs.
- -
- The pregnant women were followed by routine care with mHealth intervention and utilized a mobile application.
- c.
- Types of interventions—mHealth application for monitoring antenatal health intervention activities—short message service (SMS), voice calling, voice messaging, notification alerts through a mobile application, and IVRS (interactive voice response system).
- d.
- Types of outcome measures
- Primary outcomes for the mother: ANC attendance
2.2. Search Methods for the Identification of Studies
- Data sources and search strategy—This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines [21]. We comprehensively searched the MEDLINE, Embase, and CINAHL databases from inception from January to May 2022. Additional citations were sought from the references in articles retrieved through searches.
2.3. Data Collection and Analysis
- Selection of studies—The studies were selected independently by two reviewers (MM and DP) by reading their titles and abstracts through the use of Rayyan software, and disagreements were resolved through discussion with a third reviewer (JM). Full articles were retrieved for studies that did not provide a summary or had a scant abstract to determine their eligibility for inclusion. Two review authors (MM and DP) independently evaluated the full texts of the remaining papers for inclusion. Disagreements between them were solved through discussion and concord. A third review author was involved in deciding if no conclusion was reached. Details of the screening are provided below in the PRISMA flow chart.
- Data extraction and management—Using a predesigned data extraction form, two review authors individually retrieved the following information: (1) study information (study ID, date of extraction, title, authors, and source of study if not published); (2) study characteristics (study design, sample size, and inclusion/exclusion criteria used in the study, geographical location, and setting); (3) characteristics of the participants, including population type and mean age; (4) details of interventions; and (5) outcomes as described in the outcome measures above.
- Assessment of risk of bias in the included studies—We used the ‘Revman risk of bias’ assessment tool to assess the risk of bias for the included studies. Two review authors (JM and DS) independently evaluated the risk of bias in the included studies—the details are presented in Table 1 (risk of bias table). Disagreements were resolved through discussion or a conversation with a third review author.
 Table 1. The basic characteristics of all the individual studies have been outlined.
Table 1. The basic characteristics of all the individual studies have been outlined. - Measurement of treatment effect—The statistical analysis was executed according to [22]. We expressed effect measures as risk ratios and risk differences with 95% confidence intervals in the case of dichotomous outcomes. Based on the numerator and denominator of the studies where the risk ratio was not reported, we calculated the risk ratio between mothers who used a mobile phone and those who did not in both the intervention and control arms.
- Assessment of reporting bias—By determining whether the study was registered in a trial registry, a protocol was accessible, and an outcome was provided in the methods section, reporting bias was evaluated. The list of results from those sources was contrasted with the results mentioned in the paper that was published. An inverted funnel plot was used to assess potential publication bias.
- Data synthesis—We used Review Manager 5 software (version 5.4) to carry out the meta-analysis for this study. The meta-analysis was carried out by statistically combining the pregnancy outcomes of increased attendance at antenatal check-ups in various studies. The statistical analyses were carried out according to [22]. We conducted a random-effect meta-analysis where appropriate. We used funnel plots to assess publication bias in the meta-analysis with I2 value and heterogeneity.
- Quality of evidence—A quality check of the evidence was carried out by Review Manager 5 software (version 5.4) using the risk of bias tool depicting the included studies at high, low, or moderate risk. In all analyses, a p-value of less than 0.05 was considered statistically significant.
3. Results
3.1. Identification and Characteristics of Included Studies for SR and MA
A comprehensive electronic search of various databases revealed a total of 541 articles. After removing 73 duplicate articles, we scrutinised the titles and abstracts of 468 articles, out of which 46 were full-text articles. However, as illustrated in the PRISMA flow diagram (Figure 1), we excluded 40 articles for various reasons like different primary outcomes for some studies, different methods of study, and those studies which did not fulfill our eligibility criteria. A total of six studies, those that ideally addressed the PICO question for systematic review and meta-analysis, were included with a total of 7886 women.
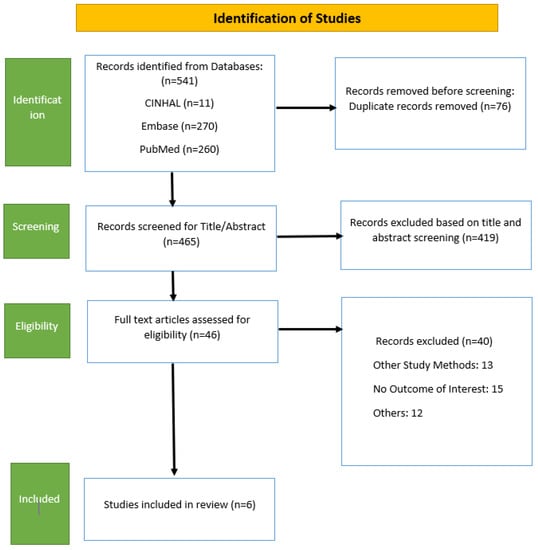
Figure 1.
PRISMA flow diagram.
P—pregnant women (from the first trimester to the third trimester) (up-to delivery) in India. I—mHealth application for monitoring antenatal health. C—pregnant women not using mobile health apps. O—decreased maternal mortality.
An overview of the characteristics of each study, which targeted antenatal women in the first to the third trimester in rural and remote areas of low- or lower-middle-income countries, and all of the RCTs performed in healthcare facilities including in India (one study conducted at the Rural Medical College, Loni, Ahmednagar), Zanzibar (two studies), Nigeria (one study), Brazil (one study) and another study conducted in Ethiopia are provided in Table 1.
All of the studies compared antenatal mothers with a mobile health intervention to a control group of antenatal mothers. Out of the six studies, the “M SAKSHI” application was used as an intervention for one study [25], whereas in another five studies, short message services, text messages, and mobile phone calls were the mode of intervention for monitoring the outcome effect (antenatal health) (Table 2).
Table 2.
Risk of bias of the included studies. Overall, five studies were assessed as low risk of bias, and one [28] as an unclear bias which is illustrated as below.
3.2. Results for ANC Attendance
Antenatal mothers who used a mobile health intervention were more likely (RR = 1.66, 95% CI = 1.07–2.58, I2 = 98%) to attend ANC check-ups when compared with the women who did not use any mobile health applications or did not receive any short message services (Figure 2).
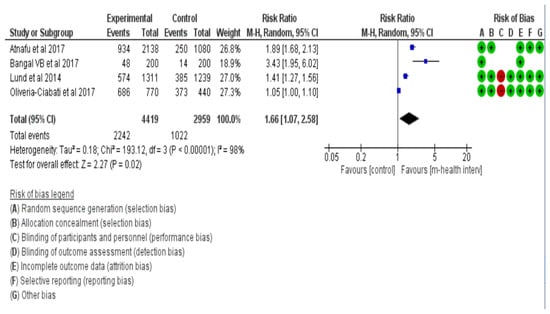
Figure 2.
Forest plot for ANC attendance [25,26,27,28].
A funnel plot (Figure 3) using data from the six reported studies representing asymmetrical distribution, which signifies a chance of publication bias.
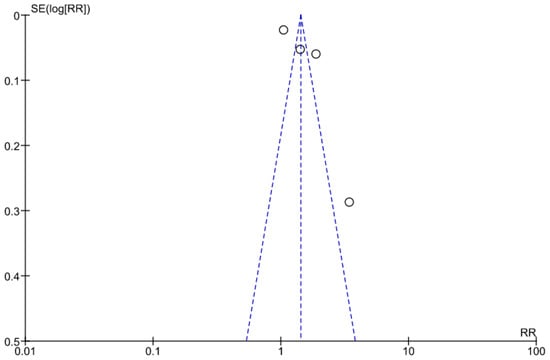
Figure 3.
Funnel plot for ANC attendance.
4. Discussion
The primary goal of conducting a systematic review and meta-analysis on the effectiveness of mHealth interventions for monitoring antenatal health is to develop or strengthen the evidence for the effectiveness of mHealth in antenatal care. Moreover, this study will aid in determining the potential to significantly improve ANC attendance among antenatal mothers, thereby contributing to improved maternal and fetal health outcomes in low-income countries. Several studies have addressed the use of mHealth to promote MNCH in LMICs, but only a small number have thoroughly assessed how these interventions have affected health outcomes in these populations. mHealth technologies are being utilised more and more to increase care accessibility and improve maternal and fetal health. Unfortunately, compared to women in higher-income countries, women in low-income countries have a 120-fold higher risk of dying from causes related to pregnancy and childbirth [29]. Therefore, in the present meta-analysis, we pooled data from selected studies conducted in low- and middle-income countries.
In the present study, we found that antenatal mothers who used mobile health interventions had an approximately two times higher chance of receiving ANC check-ups than women who did not use any mobile health applications or did not receive any short message services, which is higher than in another systematic review conducted in a population of LMICs in the time frame from 2008–2020 (OR = 1.89, 95% CI: 1.49–2.19) [30]. Despite the fact that most people exhibit techno-skepticism (i.e., a skeptical attitude toward technology), this meta-analysis revealed that mHealth has the potential to increase antenatal attendance when compared to conventional approaches. A further randomised controlled trial was carried out in Zanzibar between March 2009 and March 2010 in low- and middle-income nations, which confirmed these results. It showed that women who received a mobile phone intervention were more than twice as likely to receive four or more antenatal care visits compared to those who did not receive the intervention [23]. Irrespective of the typically low antenatal coverage in Sub-Saharan African countries, our findings were supported by a prospective randomised controlled trial conducted in Kenya in 2012 [31]. However, another systematic review and meta-analysis carried out in Ethiopia discovered that women who were sent text messages were around three times more likely to attend ANC appointments compared to those who did not receive such messages (OR = 2.74 95% CI: 1.41, 5.32) [15], which shows a greater result compared to our study.
Technology does not discriminate, and a well-functioning system has the potential to improve service coverage equality for both disadvantaged and non-marginalised populations [32]. Similarly, a USAID-supported study in Afghanistan resulted in not only mass participation but also enhanced the health-seeking behavior of the respective community [33]. Thus, it is important to comprehend the trend and pattern of mobile ownership across different geographic scales. Pregnant women who received text messages reported higher levels of satisfaction than women who received standard prenatal care, according to Jareethum et al.’s optimistic data from Thailand. Similarly, Kaewkungwal et al. [34] demonstrated that using mHealth in Thailand increased the coverage of ANC and immunization among expectant mothers and kids. This implies that other resource-poor nations like India may use mobile text messages as a promising behavior-change communication approach [35]. Clinical mHealth cannot be successful on its alone without the use of such cost-effective technologies in public health. Healthcare systems may develop a comprehensive and sustainable ecosystem that utilises the benefits of both areas by emphasizing collaboration and integration of clinical mHealth with cost-effective technologies in public health. This integration maximises clinical mHealth’s potential to improve healthcare delivery, improve public health outcomes, and contribute to individuals’ and communities’ overall well-being.
4.1. Policy Implications
- Integration of mHealth interventions: Policymakers should prioritise the integration of mHealth interventions into the existing maternal health care services in LMICs. This will ensure that antenatal mothers have access to mHealth interventions and traditional healthcare services [36,37].
- Cost-effective interventions: When compared to traditional healthcare services, mHealth interventions have the potential to improve maternal health outcomes at a lower cost. When making decisions about maternal health care, policymakers should consider the cost-effectiveness of these interventions.
- Accessibility of technology: Policymakers should prioritise increasing access to mobile phones and Internet services, as these are essential for mHealth interventions to be effective. This may involve increasing investment in telecommunication infrastructure and making Internet and mobile phone services more affordable [38].
- Capacity building: India has launched various initiatives to improve public healthcare infrastructure, including the National Rural Health Mission (NRHM) and the Indian Public Health Standards (IPHS). Structural changes have been proposed to provide quality care to rural populations, and training and capacity building of healthcare personnel is critical. Policymakers must prioritise building the capacity of healthcare workers to deliver effective mHealth interventions, including training on the use of mHealth tools and ensuring access to necessary resources [39].
- Monitoring and evaluation: To ensure the effectiveness and sustainability of mHealth interventions for maternal health outcomes, policymakers should prioritise monitoring and evaluating their impact. In resource-limited settings, mHealth interventions should be considered by public health practitioners, policymakers, and researchers. This study’s findings and evidence-based recommendations could be useful in addressing maternal healthcare challenges in low- and middle-income countries (LMICs) through the use of various mHealth interventions, thereby contributing to the achievement of the Sustainable Development Goal of Maternal and Child Health [40,41].
Overall, policymakers should prioritise the integration of mHealth interventions into maternal healthcare services in LMICs, ensuring that they are cost-effective, accessible, and sustainable and that healthcare workers are trained to deliver these interventions effectively.
4.2. Strengths and Limitations of This Study
Even with limited support such as SMS, there has been an improvement in the utilization of antenatal services amidst the changing landscape of technology.
The inclusion of studies from low- and middle-income countries (LMICs) enables results to be generalised to their respective populations.
As an intervention, the broad term “mHealth” has resulted in heterogeneity.
The limitation of this study is that only articles published in English were included, which may have resulted in the exclusion of relevant studies published in other languages. However, this decision was made to ensure consistency in the intervention, study design, participants, and outcome measures.
5. Conclusions
The emergence of mobile health technology (mHealth) has made it possible to improve prenatal care and empower pregnant women. It enhances emergency obstetric referrals, promotes collaboration among health workers, and improves overall care delivery. Moreover, mHealth can also strengthen preventative services through the widespread dissemination of antenatal care promotion. Finally, mHealth has revolutionised prenatal care by making it more accessible and providing pregnant women with the knowledge and resources they need to actively participate in their own prenatal care. This not only improves individual results but also benefits community health and well-being because healthier pregnancies result in healthier populations.
Author Contributions
Concept and design, S.P., J.S.K. and T.R.; monitored analysis and critical revision of the manuscript for important intellectual content, S.P., J.S.K. and T.R.; conceptualization, formal analysis, methodology, writing—original draft preparation, M.M., D.P., J.M. and D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
For developing this review, formal ethics approval was not required as the analysis was mainly based on a review of existing data, and documentation was based on published articles using a published tool.
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors declare that the data collected was gathered from publicly available databases and is available with this publication.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Masoi, T.J.; Kibusi, S.M. Improving pregnant women’s knowledge on danger signs and birth preparedness practices using an interactive mobile messaging alert system in Dodoma region, Tanzania: A controlled quasi experimental study. Reprod. Health 2019, 16, 177. [Google Scholar] [CrossRef] [PubMed]
- Islam, M.A.; Sathi, N.J.; Abdullah, H.M.; Naime, J.; Butt, Z.A. Factors affecting the utilisation of antenatal care services during pregnancy in Bangladesh and 28 other low-and middle-income countries: A meta-analysis of demographic and health survey data. Dr. Sulaiman Al Habib Med. J. 2022, 4, 19–31. [Google Scholar] [CrossRef]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. 2016. Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 4 February 2023).
- National Health Mission. Guidelines for—Antenatal Care and Skilled Attendance at Birth. Available online: https://nhm.gov.in/images/pdf/programmes/maternal-health/guidelines/sba_guidelines_for_skilled_attendance_at_birth.pdf (accessed on 4 February 2023).
- Jinga, N.; Mongwenyana, C.; Moolla, A.; Malete, G.; Onoya, D. Reasons for late presentation for antenatal care, healthcare providers’ perspective. BMC Health Serv. Res. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/news/item/05-10-2021-new-global-targets-to-prevent-maternal-deaths (accessed on 4 February 2023).
- Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality (accessed on 4 February 2023).
- Available online: https://data.unicef.org/topic/maternal-health/antenatal-care/ (accessed on 4 February 2023).
- Kumar, G.; Choudhary, T.S.; Srivastava, A.; Upadhyay, R.P.; Taneja, S.; Bahl, R.; Martines, J.; Bhan, M.K.; Bhandari, N.; Mazumder, S. Utilisation, equity and determinants of full antenatal care in India: Analysis from the National Family Health Survey 4. BMC Pregnancy Childbirth 2019, 19, 1–9. [Google Scholar] [CrossRef]
- Vallely, L.M.; Calvert, B.; De Silva, M.; Panisi, L.; Babona, D.; Bolnga, J.; Duro-Aina, T.; Noovao-Hill, A.; Naidu, S.; Leisher, S.; et al. Improving maternal and newborn health and reducing stillbirths in the Western Pacific Region–Current situation and the way forward. Lancet Reg. Health-West. Pac. 2022, 13, 100653. [Google Scholar] [CrossRef]
- van den Broek, N. Content and quality–integrated, holistic, one-stop antenatal care is needed for all. BJOG Int. J. Obstet. Gynaecol. 2016, 123, 558. [Google Scholar] [CrossRef][Green Version]
- Available online: https://www.unicef.org/india/what-we-do/maternal-health (accessed on 6 February 2023).
- Maternal Health—National Health Mission. Available online: https://nhm.gov.in/index1.php?lang=1&level=2&sublinkid=822&lid=218 (accessed on 6 February 2023).
- Free, C.; Phillips, G.; Galli, L.; Watson, L.; Felix, L.; Edwards, P.; Patel, V.; Haines, A. The effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: A systematic review. PLoS Med. 2013, 10, e1001362. [Google Scholar] [CrossRef]
- Wagnew, F.; Dessie, G.; Alebel, A.; Mulugeta, H.; Belay, Y.A.; Abajobir, A.A. Does short message service improve focused antenatal care visit and skilled birth attendance? A systematic review and meta-analysis of randomised clinical trials. Reprod. Health 2018, 15, 191. [Google Scholar] [CrossRef]
- Modi, D.; Dholakia, N.; Gopalan, R.; Venkatraman, S.; Dave, K.; Shah, S.; Desai, G.; Qazi, S.A.; Sinha, A.; Pandey, R.M.; et al. mHealth intervention “ImTeCHO” to improve delivery of maternal, neonatal, and child care services—A cluster-randomised trial in tribal areas of Gujarat, India. PLoS Med. 2019, 16, e1002939. [Google Scholar] [CrossRef]
- Yadav, P.; Kant, R.; Kishore, S.; Barnwal, S.; Khapre, M. The Impact of Mobile Health Interventions on Antenatal and Postnatal Care Utilization in Low-and Middle-Income Countries: A Meta-Analysis. Cureus 2022, 14, e21256. [Google Scholar] [CrossRef]
- Rahman, M.O.; Yamaji, N.; Nagamatsu, Y.; Ota, E. Effects of mHealth Interventions on Improving Antenatal Care Visits and Skilled Delivery Care in Low-and Middle-Income Countries: Systematic Review and Meta-analysis. J. Med. Internet Res. 2022, 24, e34061. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.; Eriksen, J.; Black, V.; Thorson, A.; Hatcher, A. The mobile alliance for maternal action text message–Based mHealth intervention for maternal care in South Africa: Qualitative user study. JMIR Hum. Factors 2020, 7, e14078. [Google Scholar] [CrossRef] [PubMed]
- Murthy, N.; Chandrasekharan, S.; Prakash, M.P.; Ganju, A.; Peter, J.; Kaonga, N.; Mechael, P. Effects of an mHealth voice message service (mMitra) on maternal health knowledge and practices of low-income women in India: Findings from a pseudo-randomised controlled trial. BMC Public Health 2020, 20, 820. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://www.prisma-statement.org/PRISMAStatement/FlowDiagram (accessed on 7 February 2023).
- Cochrane Handbook for Systematic Reviews of Interventions. Available online: https://training.cochrane.org/handbook (accessed on 18 February 2023).
- Lund, S.; Nielsen, B.B.; Hemed, M.; Boas, I.M.; Said, A.; Said, K.; Makungu, M.H.; Rasch, V. Mobile phones improve antenatal care attendance in Zanzibar: A cluster randomised controlled trial. BMC Pregnancy Childbirth 2014, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Omole, O.; Ijadunola, M.Y.; Olotu, E.; Omotoso, O.; Bello, B.; Awoniran, O.; Phillips, A.; Fatusi, A. The effect of mobile phone short message service on maternal health in south—west Nigeria. Int. J. Health Plan. Manag. 2018, 33, 155–170. [Google Scholar] [CrossRef]
- Lund, S.; Rasch, V.; Hemed, M.; Boas, I.M.; Said, A.; Said, K.; Makundu, M.H.; Nielsen, B.B. Mobile phone intervention reduces perinatal mortality in zanzibar: Secondary outcomes of a cluster randomised controlled trial. JMIR mHealth uHealth 2014, 2, e2941. [Google Scholar] [CrossRef]
- Oliveira-Ciabati, L.; Vieira, C.S.; Franzon, A.C.; Alves, D.; Zaratini, F.S.; Braga, G.C.; Sanchez, J.A.; Bonifácio, L.P.; Andrade, M.S.; Fernandes, M.; et al. PRENACEL—A mHealth messaging system to complement antenatal care: A cluster randomized trial. Reprod. Health 2017, 14, 1–2. [Google Scholar] [CrossRef]
- Atnafu, A.; Otto, K.; Herbst, C.H. The role of mHealth intervention on maternal and child health service delivery: Findings from a randomized controlled field trial in rural Ethiopia. Mhealth 2017, 3, 39. [Google Scholar] [CrossRef]
- Bangal, V.B.; Borawake, S.K.; Gavhane, S.P.; Aher, K.H. Use of mobile phone for improvement in maternal health: A randomized control trial. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 5458–5464. [Google Scholar] [CrossRef]
- World Health Organization. Maternal and Reproductive Health. 2020. Available online: https://www.who.int/gho/maternal_health/mortality/maternal_mortality_text/en/#: (accessed on 15 February 2023).
- Kant, R.; Yadav, P.; Kishore, S.; Barnwal, S.; Kumar, R.; Khapre, M. Impact of mHealth interventions on antenatal and postnatal care utilisation in low and middle-income countries: A Systematic Review and Meta-Analysis. medRxiv 2020. [Google Scholar] [CrossRef]
- Fedha, T. Impact of mobile telephone on maternal health service care: A case of Njoro division. Open J. Prev. Med. 2014, 4, 365–376. [Google Scholar] [CrossRef]
- Balakrishnan, R.; Gopichandran, V.; Chaturvedi, S.; Chatterjee, R.; Mahapatra, T.; Chaudhuri, I. Continuum of Care Services for Maternal and Child Health using mobile technology—A health system strengthening strategy in low and middle income countries. BMC Med. Inform. Decis. Mak. 2016, 16, 84. [Google Scholar] [CrossRef] [PubMed]
- USAID. Mobile Technology Strengthens Behavior Change Communication and Referrals by Community Health Workers for Maternal, Newborn, and Child Health in Rural Afghanistan. World Vision. 2014. Available online: http://www.usaid.gov/sites/default/files/documents/1864/WorldVisionORBrief.pdf (accessed on 1 February 2015).
- Kaewkungwal, J.; Apidechkul, T.; Jandee, K.; Khamsiriwatchara, A.; Lawpoolsri, S.; Sawang, S.; Sangvichean, A.; Wansatid, P.; Krongrungroj, S. Application of mobile technology for improving expanded program on immunization among highland minority and stateless populations in northern Thailand border. JMIR mHealth uHealth 2015, 3, e3704. [Google Scholar] [CrossRef]
- Jareethum, R.; Titapant, V.; Tienthai, C.; Viboonchart, S.; Chuenwattana, P.; Chatchainoppakhun, J. Satisfaction of healthy pregnant women receiving short message service via mobile phone for prenatal support: A randomised controlled trial. Med. J. Med. Assoc. Thail. 2008, 91, 458. [Google Scholar]
- Ahmed, T.; Lucas, H.; Khan, A.S.; Islam, R.; Bhuiya, A.; Iqbal, M. eHealth and mHealth initiatives in Bangladesh: A scoping study. BMC Health Serv. Res. 2014, 14, 260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. mHealth: New Horizons for Health through Mobile Technologies; Global Observatory for eHealth Series; World Health Organization: Geneva, Switzerland, 2011; Volume 3, pp. 1–101. [Google Scholar]
- Tamrat, T.; Ratanaprayul, N.; Barreix, M.; Tunçalp, Ö.; Lowrance, D.; Thompson, J.; Rosenblum, L.; Kidula, N.; Chahar, R.; Gaffield, M.E.; et al. Transitioning to Digital Systems: The Role of World Health Organization’s Digital Adaptation Kits in Operationalizing Recommendations and Interoperability Standards. Glob. Health Sci. Pract. 2022, 10, e2100320. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Pallikadavath, S.; Ram, F.; Ogollah, R. Inequalities in advice provided by public health workers to women during antenatal sessions in rural India. PLoS ONE 2012, 7, e44931. [Google Scholar] [CrossRef] [PubMed]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E (accessed on 18 February 2023).
- World Health Organization. Maternal and Newborn Health. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/maternal-newborn-child-and-adolescent-health (accessed on 18 February 2023).



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).