
Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review



Abstract
1. Introduction
2. Materials and Methods
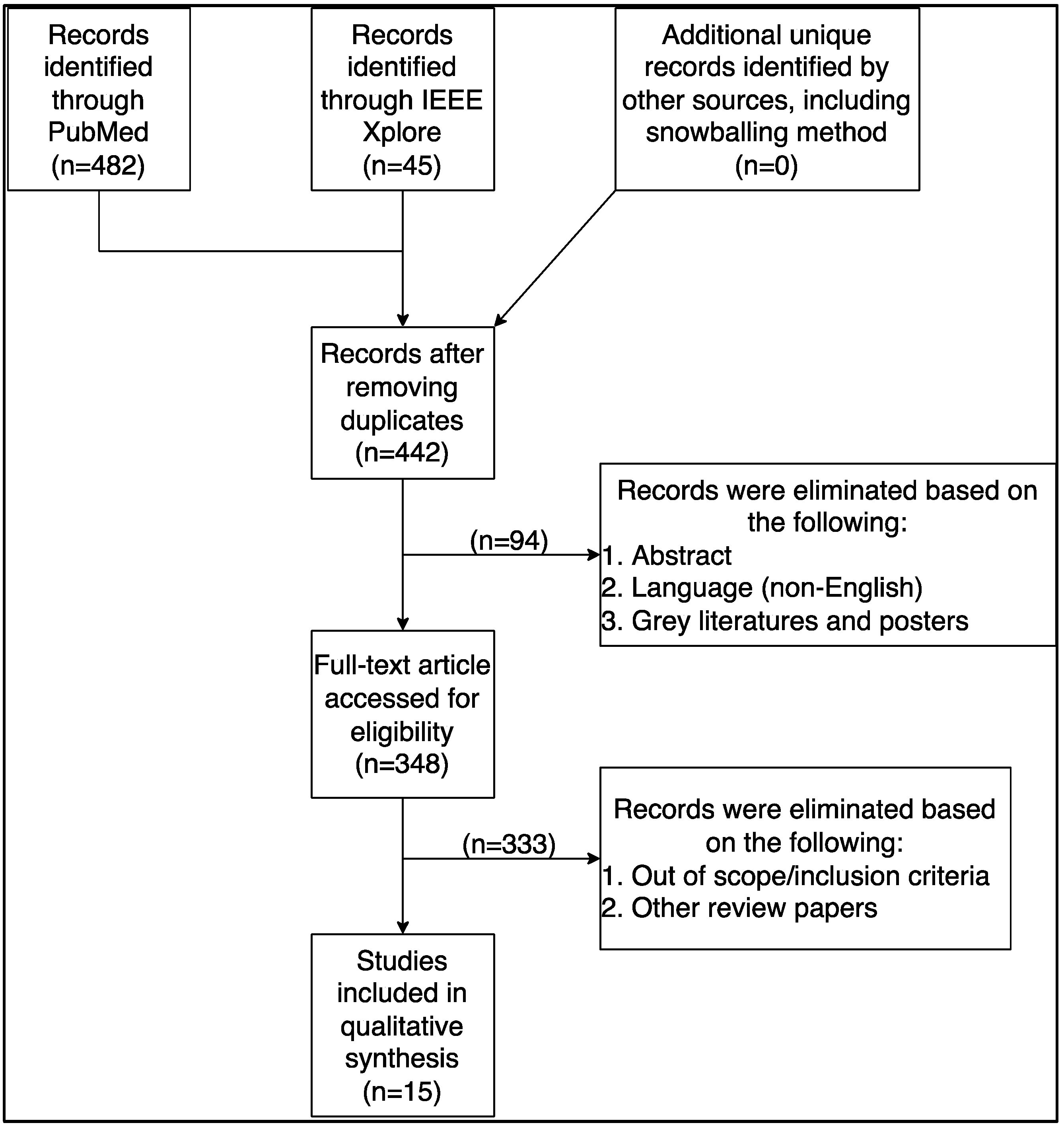
2.1. Search Query
2.2. Selection Criteria
2.3. Coding and Data Extraction
3. Results
3.1. Mobile App for Mental Health
3.2. Mental Health Attributes and Assessment
4. Discussion
4.1. Main Findings
4.2. Digital Divide
4.3. Gender Disparity and Sample Size
4.4. Recommendations
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galderisi, S.; Heinz, A.; Kastrup, M.; Beezhold, J.; Sartorius, N. Toward a New Definition of Mental Health. World Psychiatry 2015, 14, 231–233. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Mental Health Report: Transforming Mental Health for All; WHO: Geneva, Switzerland, 2022; p. 296. [Google Scholar]
- Villarroel, M.A.; Terlizzi, E.P. Symptoms of Depression among Adults: United States, 2019. NCHS Data Brief 2020, 1–8. [Google Scholar]
- Pedrelli, P.; Nyer, M.; Yeung, A.; Zulauf, C.; Wilens, T. College Students: Mental Health Problems and Treatment Considerations. Acad. Psychiatry 2015, 39, 503–511. [Google Scholar] [CrossRef]
- Bruffaerts, R.; Mortier, P.; Kiekens, G.; Auerbach, R.P.; Cuijpers, P.; Demyttenaere, K.; Green, J.G.; Nock, M.K.; Kessler, R.C. Mental health problems in college freshmen: Prevalence and academic functioning. J. Affect. Disord. 2018, 225, 97–103. [Google Scholar] [CrossRef]
- Eisenberg, D.; Hunt, J.; Speer, N. Mental health in American colleges and universities: Variation across student subgroups and across campuses. J. Nerv. Ment. Dis. 2013, 201, 60–67. [Google Scholar] [CrossRef]
- Coombs, N.C.; Meriwether, W.E.; Caringi, J.; Newcomer, S.R. Barriers to healthcare access among U.S. adults with mental health challenges: A population-based study. SSM Popul. Health 2021, 15, 100847. [Google Scholar] [CrossRef] [PubMed]
- Ebert, D.D.; Mortier, P.; Kaehlke, F.; Bruffaerts, R.; Baumeister, H.; Auerbach, R.P.; Alonso, J.; Vilagut, G.; Martínez, K.I.; Lochner, C.; et al. Barriers of mental health treatment utilization among first-year college students: First cross-national results from the WHO World Mental Health International College Student Initiative. Int. J. Methods Psychiatr. Res. 2019, 28, e1782. [Google Scholar] [CrossRef]
- Chandrashekar, P. Do mental health mobile apps work: Evidence and recommendations for designing high-efficacy mental health mobile apps. Mhealth 2018, 4, 6. [Google Scholar] [CrossRef]
- Watt, A.; Cameron, A.; Sturm, L.; Lathlean, T.; Babidge, W.; Blamey, S.; Facey, K.; Hailey, D.; Norderhaug, I.; Maddern, G. Rapid versus full systematic reviews: Validity in clinical practice? ANZ J. Surg. 2008, 78, 1037–1040. [Google Scholar] [CrossRef]
- Harrer, M.; Apolinário-Hagen, J.; Fritsche, L.; Salewski, C.; Zarski, A.-C.; Lehr, D.; Baumeister, H.; Cuijpers, P.; Ebert, D.D. Effect of an internet- and app-based stress intervention compared to online psychoeducation in university students with depressive symptoms: Results of a randomized controlled trial. Internet Interv. 2021, 24, 100374. [Google Scholar] [CrossRef]
- Kleiman, E.M.; Bentley, K.H.; Wacha-Montes, A.; Taylor, M.E.; Lozy, O.; Conti, K.; Reese Mayer, W. A Pilot Implementation-Effectiveness Trial of a Single-Session Telehealth Workshop and Smartphone-Based Cognitive Behavioral Intervention for Managing Emotions Among College Students. Behav. Ther. 2022, 53, 1024–1036. [Google Scholar] [CrossRef] [PubMed]
- Bruehlman-Senecal, E.; Hook, C.J.; Pfeifer, J.H.; FitzGerald, C.; Davis, B.; Delucchi, K.L.; Haritatos, J.; Ramo, D.E. Smartphone App to Address Loneliness Among College Students: Pilot Randomized Controlled Trial. JMIR Ment. Health 2020, 7, e21496. [Google Scholar] [CrossRef] [PubMed]
- Haeger, J.A.; Davis, C.H.; Levin, M.E. Utilizing ACT daily as a self-guided app for clients waiting for services at a college counseling center: A pilot study. J. Am. Coll. Health 2022, 70, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Huberty, J.; Green, J.; Glissmann, C.; Larkey, L.; Puzia, M.; Lee, C. Efficacy of the Mindfulness Meditation Mobile App “Calm” to Reduce Stress Among College Students: Randomized Controlled Trial. JMIR Mhealth Uhealth 2019, 7, e14273. [Google Scholar] [CrossRef]
- Lattie, E.; Cohen, K.A.; Winquist, N.; Mohr, D.C. Examining an App-Based Mental Health Self-Care Program, IntelliCare for College Students: Single-Arm Pilot Study. JMIR Ment. Health 2020, 7, e21075. [Google Scholar] [CrossRef]
- Levin, M.E.; Hicks, E.T.; Krafft, J. Pilot evaluation of the stop, breathe & think mindfulness app for student clients on a college counseling center waitlist. J. Am. Coll. Health 2022, 70, 165–173. [Google Scholar] [CrossRef]
- Bruhns, A.; Lüdtke, T.; Moritz, S.; Bücker, L. A Mobile-Based Intervention to Increase Self-esteem in Students with Depressive Symptoms: Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e26498. [Google Scholar] [CrossRef]
- Schulte-Frankenfeld, P.M.; Trautwein, F.M. App-based mindfulness meditation reduces perceived stress and improves self-regulation in working university students: A randomised controlled trial. Appl. Psychol. Health Well Being 2022, 14, 1151–1171. [Google Scholar] [CrossRef]
- Harrer, M.; Adam, S.H.; Fleischmann, R.J.; Baumeister, H.; Auerbach, R.; Bruffaerts, R.; Cuijpers, P.; Kessler, R.C.; Berking, M.; Lehr, D.; et al. Effectiveness of an Internet- and App-Based Intervention for College Students with Elevated Stress: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e136. [Google Scholar] [CrossRef]
- Lee, R.A.; Jung, M.E. Evaluation of an mHealth App (DeStressify) on University Students’ Mental Health: Pilot Trial. JMIR Ment. Health 2018, 5, e2. [Google Scholar] [CrossRef]
- Kajitani, K.; Higashijima, I.; Kaneko, K.; Matsushita, T.; Fukumori, H.; Kim, D. Short-term effect of a smartphone application on the mental health of university students: A pilot study using a user-centered design self-monitoring application for mental health. PLoS ONE 2020, 15, e0239592. [Google Scholar] [CrossRef] [PubMed]
- Clarke, J.; Draper, S. Intermittent mindfulness practice can be beneficial, and daily practice can be harmful. An in depth, mixed methods study of the “Calm” app’s (mostly positive) effects. Internet Interv. 2020, 19, 100293. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.; Park, J.Y.; Joung, D.; Jhung, K. Response Time as an Implicit Self-Schema Indicator for Depression among Undergraduate Students: Preliminary Findings From a Mobile App-Based Depression Assessment. JMIR Mhealth Uhealth 2019, 7, e14657. [Google Scholar] [CrossRef]
- Bendtsen, M.; Müssener, U.; Linderoth, C.; Thomas, K. A Mobile Health Intervention for Mental Health Promotion among University Students: Randomized Controlled Trial. JMIR Mhealth Uhealth 2020, 8, e17208. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, A.; Choudhury, M. Mobile for Mothers mHealth Intervention to Augment Maternal Health Awareness and Behavior of Pregnant Women in Tribal Societies: Randomized Quasi-Controlled Study. JMIR Mhealth Uhealth 2022, 10, e38368. [Google Scholar] [CrossRef]
- Wallis, L.; Blessing, P.; Dalwai, M.; Shin, S.D. Integrating mHealth at point of care in low- and middle-income settings: The system perspective. Glob. Health Action 2017, 10, 1327686. [Google Scholar] [CrossRef]
- Cao, L.; Chongsuvivatwong, V.; McNeil, E.B. The Sociodemographic Digital Divide in Mobile Health App Use Among Clients at Outpatient Departments in Inner Mongolia, China: Cross-sectional Survey Study. JMIR Hum. Factors 2022, 9, e36962. [Google Scholar] [CrossRef]
- Källander, K.; Tibenderana, J.K.; Akpogheneta, O.J.; Strachan, D.L.; Hill, Z.; ten Asbroek, A.H.A.; Conteh, L.; Kirkwood, B.R.; Meek, S.R. Mobile Health (mHealth) Approaches and Lessons for Increased Performance and Retention of Community Health Workers in Low- and Middle-Income Countries: A Review. J. Med. Internet Res. 2013, 15, e17. [Google Scholar] [CrossRef]
- Bell, M.L.; Kenward, M.G.; Fairclough, D.L.; Horton, N.J. Differential dropout and bias in randomised controlled trials: When it matters and when it may not. BMJ 2013, 346, e8668. [Google Scholar] [CrossRef]
- Nideffer, R.M. Test of attentional and interpersonal style. J. Personal. Soc. Psychol. 1976, 34, 394. [Google Scholar] [CrossRef]
- Koh, J.; Tng, G.Y.Q.; Hartanto, A. Potential and Pitfalls of Mobile Mental Health Apps in Traditional Treatment: An Umbrella Review. J. Pers. Med. 2022, 12, 1376. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Location | Intervention | Follow-Up | Participants at Baseline | Dropout Rate | Female | Minority Race |
|---|---|---|---|---|---|---|
| Weeks | Weeks | n | % | n (%) | % | |
| [15] USA | 8 | 4 | 88 | 0 | 79 (88) | 39 |
| [20] Multinational | 7 | 5 | 150 | 30 | 112 (75) | Na |
| [25] Sweden | 10 | 2 | 654 | 48 | 510 (78) | Na |
| [16] USA | 8 | None | 21 | 1 | 17 (81) | 28 |
| [21] Canada | 4 | 4 | 206 | 21 | 103 (63) | 21 |
| [18] Germany | 4 | None | 400 | 34 | 357 (89) | Na |
| [19] Germany | 8 | None | 99 | 35 | 67 (68) | Na |
| [22] Japan | 2 | None | 68 | 16 | 17 (30) | Na |
| [13] USA | 4 | 4 | 221 | 5 | 131 (59) | 47 |
| [11] Germany | 7 | 5 | 200 | 24 | 170 (85) | Na |
| [24] South Korea | 2 | None | 70 | 7 | 33 (51) | Na |
| [23] Scotland | 1 | 2 | 269 | 50 | 218 (81) | 16 |
| [17] USA | 4 | None | 23 | 30 | 16 (100) | 0 |
| [12] Unidentified | 8 | None | 222 | 20 | 138 (78) | 67 |
| [14] USA | 2 | 2 | 11 | 0 | 9 (82) | 9 |
| Name of the App | Access to the App | Methodology of the App | Intervention Delivery Approach | Frequency of App Use |
|---|---|---|---|---|
| [15] Calm | Public | Meditation, CBT | TGE | 10 min Daily |
| [20] StudiCare Stress | Participants | CBT and Mindfulness, Emotions, Acceptance | TGE, e-Coach (chatbot) | Two weekly modules |
| [25] mHealth PPMP | Participants | Positive Psychology | Text Messages, TGE | 10 min Daily |
| [16] IntelliCare for College Students | Participants | Cognitive Restructuring, Behavioral Activation | Mood Rating and Journal, Symptom Check, Lessons, and Resources | 1 Text daily |
| [21] DeStressify | Public | Mindfulness | TGE | 5 days/week) |
| [18] MCT & More | Public | CBT, Mindfulness, ACT, Metacognitive Training | TGE | 3–10 min daily |
| [19] Balloon | Public | MCT, Mindfulness, and Meditation | TGE | 10 min daily |
| [22] Mental App | Participants | Focus on Diagnosis Rather Than Treatment | Self-Monitoring, Self-Screening, and Referrals | Not defined |
| [13] Nod | Public | Positive Psychology, Mindfulness, CBT | Social Challenges, Reflections, and Written Testimonials | Not defined |
| [11] StudiCare | Participants | ERS | TGE | 1 weekly module |
| [24] K-CESD-R Mobile App | Participants | K-CESD-R Surveys | K-CESD-R Surveys | 1 session daily |
| [23] Calm | Public | Meditation, CBT | TGE | 10 min daily |
| [17] Stop, Breathe, and Think | Public | Meditation | TGE, Meditation and Emotional Check-Ins | 1 prompt daily |
| [12] MetricWire | Study | Mindfulness, Cognitive Flexibility, ERS | Therapeutic Workshop Skills | 4 prompts daily |
| [14] ACT Daily | Public | ACT | Coaching Sessions | 3 questionnaires daily |
| Mental Health Factors (Primary) | Other Factors Related to Mental Health (Secondary) | |||||||
|---|---|---|---|---|---|---|---|---|
| Study | Depression | Anxiety | Stress | Sleep Quality | Self-Image | Burnout | Quality of Life | General Health |
| [15] | Y * | Y * | Y * | |||||
| [20] | Y * | Y * | Y * | Y | Y * | Y * | ||
| [25] | Y * | Y * | Y * | |||||
| [16] | Y | Y | Y * | |||||
| [21] | Y | Y * | Y | Y | Y * | |||
| [18] | Y * | Y * | Y | |||||
| [19] | Y * | Y | ||||||
| [22] | Y | Y * | ||||||
| [13] | Y | Y | Y | |||||
| [11] | Y * | Y * | Y * | Y * | Y * | |||
| [24] | Y | Y | ||||||
| [23] | Y | |||||||
| [17] | Y | Y * | Y * | |||||
| [12] | Y * | Y * | ||||||
| [14] | Y * | Y * | Y * | |||||
| Study | Validated Scales Used by Different Studies to Measure Different Mental Health Factor |
|---|---|
| Mental Health and Related Factor (Scales Used) | |
| [15] | Stress (PSS), Mindfulness (FFMQ), Self-Compassion (SCS-SF), Sleep Quality (PROMIS), Binge Drinking (YRBS), Physical Activity Participation (YRBS), Healthy Eating (YRBS) |
| [20] | Stress (PSS), Depression (CES-D), Anxiety (STAI), General Well-Being (WHO-5), Emotional Exhaustion (MBI-S), Dysfunctional Perfectionism (RAPS), Resilience (CD-RISC), Self-Compassion (SCS), Self-Esteem (RSES), Work Impairment (WIS), Academic Self-Efficacy (ASES), Academic Worrying (AWQ) |
| [25] | Mental Health and Well Being (MHC-SF), Depression (HADS), Anxiety (HADS) |
| [16] | Depression (PHQ), Anxiety (GAD), Anxiety Literacy (ALQ), Depression Literacy (DLQ), Knowledge and Beliefs About Services (KBSS), Cognitive and Behavioral Response to Stress (CB-RSS) |
| [21] | Stress (PSS), Anxiety (STAI), Depression (QIDS-SR), Sleep Quality (PSQI), Quality of Life (RAND-HS), Work Productivity (WPAI) |
| [18] | Depression (PHQ), Self-Esteem (RSES), Quality of Life (WHOQOL-BREF), Attitude Towards Psychological Online Interventions (APOI), Patient Therapy Expectation and Evaluation (PATHEV), Negative Effects of Psychotherapy (INEP) |
| [19] | Stress (PSS), Self-Regulation (SRS), Life Satisfaction and Happiness (QAH), Mindfulness (FMI), Emotional Regulation (ERQ), Social Desirability (SEA) |
| [22] | Public Stigma (LSS), Depression (CES-D), General Health (GHQ) |
| [13] | Loneliness (UCLA), Anxiety (GAD), Depression (PHQ), Social Anxiety (MSPI), Sleep Quality (PSQI), Perceived Social Support (CIT), Campus Belonging (SERUQ), Social Adjustment to College (SACQ), Intention to Return to College (NSSE) |
| [11] | Depression (CES-D), Behavioral Activation for Depression (BADS), Stress (PSS), Anxiety (STAD), Worrying (AWQ), Emotional Exhaustion (MBI-S), Work Impairment (WIS), Work Output (WOS), Work Cutback (PS-S), College Self-Efficacy (CSED), Resilience (CD-RISC), Emotion Regulation Competencies (SEK), Self-Compassion (SCS-D), Self-Esteem (RSES), Negative Beliefs About Stress (BASS), Positive Beliefs About Stress (BASS), Controllability Beliefs About Stress (BASS) |
| [24] | Depression (PHQ, CES-D, QIDS-SR, MADRS, HAM-D), Anxiety (HAM-A), Severity of Illness (CGI-S), Neuropsychiatric Interview (MINI) |
| [23] | Mindfulness (FFMQ), Generalized Self-Efficacy (GSE), Mental Well-Being (SWEMWBS) |
| [17] | Positive Mental Health (CCAPS, MHC-SF), Mindfulness (FFMQ), Values Progress (V.Q.) |
| [12] | Depression (EMA), Anxiety (EMA) |
| [14] | Depression (DASS), Anxiety (DASS), Stress (DASS), Psychological Inflexibility (AAQ), Cognitive Fusion (CFQ), Mindfulness (PHLMS), Valued Living (V.Q.), Emotional Self-Awareness (ESAS) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choudhury, A.; Kuehn, A.; Shamszare, H.; Shahsavar, Y. Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review. Healthcare 2023, 11, 272. https://doi.org/10.3390/healthcare11020272
Choudhury A, Kuehn A, Shamszare H, Shahsavar Y. Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review. Healthcare. 2023; 11(2):272. https://doi.org/10.3390/healthcare11020272
Chicago/Turabian StyleChoudhury, Avishek, Annabella Kuehn, Hamid Shamszare, and Yeganeh Shahsavar. 2023. "Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review" Healthcare 11, no. 2: 272. https://doi.org/10.3390/healthcare11020272
APA StyleChoudhury, A., Kuehn, A., Shamszare, H., & Shahsavar, Y. (2023). Analysis of Mobile App-Based Mental Health Solutions for College Students: A Rapid Review. Healthcare, 11(2), 272. https://doi.org/10.3390/healthcare11020272