
Strength Training vs. Aerobic Training for Managing Pain and Physical Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis

 , ,
, ,  ,
,  , ,
, ,
Abstract
:1. Introduction
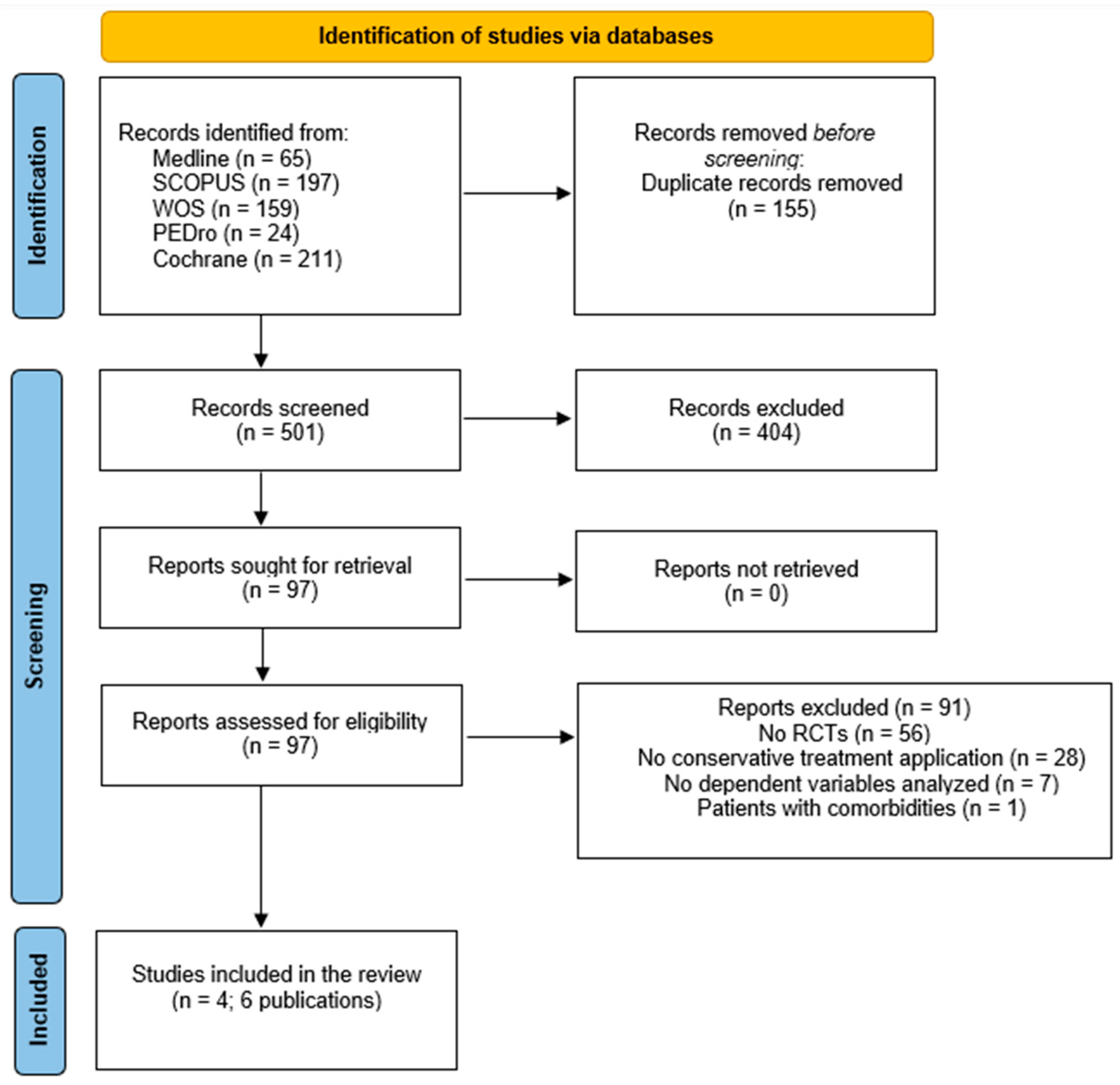
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Data Collection Process
2.3. Methodological Quality and Risk of Bias
2.4. Certainty of Evidence
2.5. Data Synthesis and Analysis
3. Results
3.1. Characteristics of the Studies: Sample, Interventions, and Outcomes
3.2. Methodological Quality and Risk of Bias


| Author | Items | Total Score | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Ettinger et al., 1997 [40] | Y | Y | Y | Y | N | N | Y | N | Y | N | Y | 6/10 | Fair |
| Messier et al., 1997 [44] | Y | Y | Y | Y | N | N | Y | N | Y | N | Y | 6/10 | Fair |
| Rejeski et al., 1998 [45] | Y | Y | Y | Y | N | N | Y | N | Y | N | N | 5/10 | Fair |
| Samut et al., 2015 [41] | Y | Y | N | Y | N | N | N | Y | N | Y | Y | 5/10 | Fair |
| Küçük et al., 2018 [42] | Y | Y | N | Y | N | N | N | Y | Y | Y | Y | 6/10 | Fair |
| Øiestad et al., 2023 [43] | Y | Y | Y | Y | N | N | Y | Y | Y | Y | Y | 8/10 | High |
3.3. Effects of Interventions
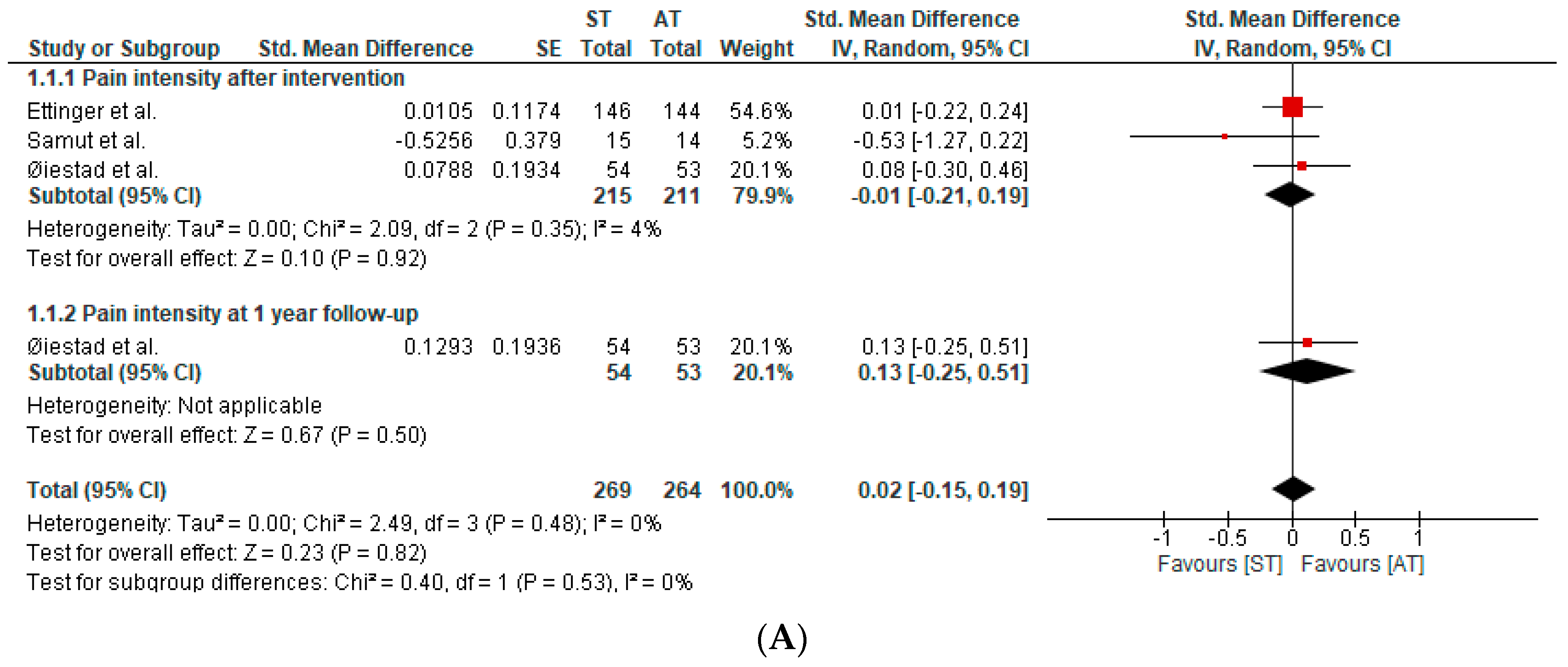
3.4. Pain
3.5. Physical Function
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
Appendix A.1. Pubmed Search Formula
- #1 (“Osteoarthritis, Knee”[Mesh] OR “Knee osteoarthritis”)
- #2 (“Resistance Training”[Mesh] OR “Resistance exercise training” OR “Resistance exercise” OR “Strength” OR “Strengthening” OR “Strengthening exercises” OR “Strength training” OR “isometric exercise” OR “quadriceps” OR “gluteus” OR “hamstring” OR “abductors” OR “eccentric” OR “concentric” OR “home-based exercise” OR “home programme” OR “isokinetic”)
- #3 (“Endurance Training”[Mesh] OR “aerobic exercise” OR “aerobic exercises” OR “aerobic program” OR “aerobic training” OR “aerobic”)
- #4 (“Pain”[Mesh] OR “pain intensity” OR “Function” OR “Physical function” OR “Functional capacity” OR “Physical capacity”)
- #5 1# AND 2# AND 3# AND 4#
- Results: 65
- Data: 29 October 2023
Appendix A.2. Cochrane Library Search Formula
- #1 (Osteoarthritis Knee OR Knee osteoarthritis)
- #2 (Resistance Training OR Resistance exercise training OR Resistance exercise OR Strength OR Strengthening OR Strengthening exercises OR Strength training OR isometric exercise OR quadriceps OR gluteus OR hamstring OR abductors OR eccentric OR concentric OR home-based exercise OR home programme OR isokinetic)
- #3 (Endurance Training OR aerobic exercise OR aerobic exercises OR aerobic program OR aerobic training OR aerobic)
- #4 (Pain OR pain intensity OR Function OR Physical function OR Functional capacity OR Physical capacity)
- #5 1# AND 2# AND 3# AND 4#
- Results: 211
- Data: 29 October 2023
Appendix A.3. PEDro Search Formula
- #1 Knee osteoarthritis AND aerobic
- #2 Strength training
- #3 lower Leg OR knee
- #4 clinical trial
- #5 1# AND 2# AND 3# AND 4#
- Results: 24
- Data: 21 December 2023
Appendix A.4. Web of Science Search Formula
- #1 (“Osteoarthritis Knee” OR “Knee osteoarthritis”)
- #2 (“Resistance Training” OR “Resistance exercise training” OR “Resistance exercise” OR “Strength” OR “Strengthening” OR “Strengthening exercises” OR “Strength training” OR “isometric exercise” OR “quadriceps” OR “gluteus” OR “hamstring” OR “adductors” OR “eccentric” OR “concentric” OR “home-based exercise” OR “home programme” OR “isokinetic”)
- #3 (“Endurance Training” OR “aerobic exercise” OR “aerobic exercises” OR “aerobic program” OR “aerobic training” OR “aerobic”)
- #4 (“Pain” OR “pain intensity” OR “Function” OR “Physical function” OR “Functional capacity” OR “Physical capacity”)
- #5 1# AND 2# AND 3# AND 4#
- Results: 159
- Data: 29 October 2023
Appendix A.5. Scopus
- #1 “Osteoarthritis, Knee” OR “Knee osteoarthritis”
- #2 “Resistance Training” OR “Resistance exercise training” OR “Resistance exercise” OR “Strength” OR “Strengthening” OR “Strengthening exercises” OR “Strength training” OR “isometric exercise” OR “quadriceps” OR “gluteus” OR “hamstring” OR “abductors” OR “eccentric” OR “concentric” OR “home-based exercise” OR “home programme” OR “isokinetic”
- #3 “Endurance Training” OR “aerobic exercise” OR “aerobic exercises” OR “aerobic program” OR “aerobic training” OR “aerobic”
- #4 “Pain” OR “pain intensity” OR “Function” OR “Physical function” OR “Functional capacity” OR “Physical capacity”
- #5 1# AND 2# AND 3# AND 4#
- Results: 197
- Data: 29 October 2023
References
- Wallace, I.J.; Worthington, S.; Felson, D.T.; Jurmain, R.D.; Wren, K.T.; Maijanen, H.; Woods, R.J.; Lieberman, D.E. Knee osteoarthritis has doubled in prevalence since the mid-20th century. Proc. Natl. Acad. Sci. USA 2017, 114, 9332–9336. [Google Scholar] [CrossRef] [PubMed]
- Cui, A.; Li, H.; Wang, D.; Zhong, J.; Chen, Y.; Lu, H. Global, regional prevalence, incidence and risk factors of knee osteoarthritis in population-based studies. EClinicalMedicine 2020, 29–30, 100587. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K. Physiotherapy management of hip osteoarthritis. J. Physiother. 2013, 59, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Slemenda, C.; Brandt, K.D.; Heilman, D.K.; Mazzuca, S.; Braunstein, E.M.; Katz, B.P.; Wolinsky, F.D. Quadriceps Weakness and Osteoarthritis of the Knee. Ann. Intern. Med. 1997, 127, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Becker, R.; Berth, A.; Nehring, M.; Awiszus, F. Neuromuscular quadriceps dysfunction prior to osteoarthritis of the knee. J. Orthop. Res. 2004, 22, 768–773. [Google Scholar] [CrossRef] [PubMed]
- E McAlindon, T.; Cooper, C.; Kirwan, J.R.; A Dieppe, P. Determinants of disability in osteoarthritis of the knee. Ann. Rheumatol. 1993, 52, 258–262. [Google Scholar] [CrossRef] [PubMed]
- Jevsevar, D.S. Treatment of Osteoarthritis of the Knee: Evidence-Based Guideline. J. Am. Acad. Orthop. Surg. 2013, 21, 571–576. [Google Scholar] [CrossRef]
- McAlindon, T.E.; Bannuru, R.R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence; National Clinical Guideline Centre. Osteoarthritis: Care and Management in Adults; National Institute for Health and Care Excellence: London, UK, 2014. [Google Scholar]
- Lambert, C.P.; Evans, W.J. Adaptations to Aerobic and Resistance Exercise in the Elderly. Rev. Endocr. Metab. Disord. 2005, 6, 137–143. [Google Scholar] [CrossRef]
- Perez-Huerta, B.D.; Díaz-Pulido, B.; Pecos-Martin, D.; Beckwee, D.; Lluch-Girbes, E.; Fernandez-Matias, R.; Rubio, M.J.B.; Gallego-Izquierdo, T. Effectiveness of a program combining strengthening, stretching, and aerobic training exercises in a standing versus a sitting position in overweight subjects with knee osteoarthritis: A randomized controlled trial. J. Clin. Med. 2020, 9, 4113. [Google Scholar] [CrossRef]
- Krauß, I. Exercise therapy for hip and knee osteoarthristis. Dtsch. Z. Sport 2016, 67, 276–281. [Google Scholar] [CrossRef]
- Marconcin, P.; Espanha, M.; Teles, J.; Bento, P.; Campos, P.; André, R.; Yázigi, F. A randomized controlled trial of a combined self-management and exercise intervention for elderly people with osteoarthritis of the knee: The PLE2NO program. Clin. Rehabil. 2017, 32, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Kabiri, S.; Halabchi, F.; Angoorani, H.; Yekaninejad, S. Comparison of three modes of aerobic exercise combined with resistance training on the pain and function of patients with knee osteoarthritis: A randomized controlled trial [with consumer summary]. Phys. Ther. Sport 2018, 32, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Esser, S.; Bailey, A. Effects of exercise and physical activity on knee osteoarthritis. Curr. Pain Headache Rep. 2011, 15, 423–430. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; McConnell, S.; Hernandez-Molina, G.; Reichenbach, S. Exercise for osteoarthritis of the hip. Cochrane Database Syst. Rev. 2014, 22, CD007912. [Google Scholar] [CrossRef] [PubMed]
- Fransen, M.; McConnell, S.; Harmer, A.R.; Van Der Esch, M.; Simic, M.; Bennell, K.L. Exercise for osteoarthritis of the knee: A Cochrane systematic review. Br. J. Sports Med. 2015, 49, 1554–1557. [Google Scholar] [CrossRef] [PubMed]
- Kadam, U.T.; Croft, P.R. Clinical comorbidity in osteoarthritis: Associations with physical function in older patients in family practice. J. Rheumatol. 2007, 34, 1899–1904. [Google Scholar]
- Tanaka, R.; Ozawa, J.; Kito, N.; Moriyama, H. Efficacy of strengthening or aerobic exercise on pain relief in people with knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2013, 27, 1059–1071. [Google Scholar] [CrossRef]
- Roddy, E.; Zhang, W.; Doherty, M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systematic review. Ann. Rheum. Dis. 2005, 64, 544–548. [Google Scholar] [CrossRef]
- Moseley, A.M.; Rahman, P.; Wells, G.A.; Zadro, J.R.; Sherrington, C.; Toupin-April, K.; Brosseau, L. Agreement between the Cochrane risk of bias tool and Physiotherapy Evidence Database (PEDro) scale: A meta-epidemiological study of randomized controlled trials of physical therapy interventions. PLoS ONE 2019, 14, e0222770. [Google Scholar] [CrossRef]
- Verhagen, A.P.; De Vet, H.C.; De Bie, R.A.; Kessels, A.G.; Boers, M.; Bouter, L.M.; Knipschild, P.G. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J. Clin. Epidemiol. 1998, 51, 1235–1241. [Google Scholar] [CrossRef] [PubMed]
- Young, J.L.; Rhon, D.I.; de Zoete, R.M.; Cleland, J.A.; Snodgrass, S.J. The influence of dosing on effect size of exercise therapy for musculoskeletal foot and ankle disorders: A systematic review. Braz. J. Phys. Ther. 2018, 22, 20–32. [Google Scholar] [CrossRef] [PubMed]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Woodcock, J.; Brozek, J.; Helfand, M.; Alonso-Coello, P.; Glasziou, P.; Jaeschke, R.; Akl, E.A.; et al. GRADE guidelines: 7. Rating the quality of evidence—Inconsistency. J. Clin. Epidemiol. 2011, 64, 1294–1302. [Google Scholar] [CrossRef]
- Dantas, L.O.; Osani, M.C.; Bannuru, R.R. Therapeutic ultrasound for knee osteoarthritis: A systematic review and meta-analysis with grade quality assessment. Braz. J. Phys. Ther. 2021, 25, 688–697. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—Imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Cciences; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Higgins, J.; Deeks, J.; Altman, D. Chapter 16. Special topics in statistics. In Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0; The Cochrane Collaboration: Oxford, UK, 2011. [Google Scholar]
- Higgins, J.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.; Welch, V. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Page, M.; Higgins, J.; Sterne, J.A.C. Chapter 13: Assessing risk of bias due to missing results in a synthesis. In Cochrane Handbook for Systematic Reviews of Interventions; Version 6.4 (Updated August 2023); John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2023. [Google Scholar]
- Ettinger, W.H.; Burns, R.; Messier, S.P.; Applegate, W.; Rejeski, W.J.; Morgan, T.; Shumaker, S.; Berry, M.J.; O’Toole, M.; Monu, J.; et al. A randomized trial comparing aerobic exercise and resistance exercise with a health education program in older adults with knee osteoarthritis: The fitness arthritis and seniors trial (FAST). J. Am. Med. Assoc. 1997, 277, 25–31. [Google Scholar] [CrossRef]
- Samut, G.; Dinçer, F.; Özdemir, O. The effect of isokinetic and aerobic exercises on serum interleukin-6 and tumor necrosis factor alpha levels, pain, and functional activity in patients with knee osteoarthritis. Mod. Rheumatol. 2015, 25, 919–924. [Google Scholar] [CrossRef]
- Küçük, E.B.; Taşkıran Ö, Ö.; Tokgöz, N.; Meray, J. Effects of isokinetic, isometric, and aerobic exercises on clinical variables and knee cartilage volume using magnetic resonance imaging in patients with osteoarthritis. Turk. J. Phys. Med. Rehabil. 2018, 64, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Øiestad, B.E.; Årøen, A.; Røtterud, J.H.; Østerås, N.; Jarstad, E.; Grotle, M.; Risberg, M.A. The efficacy of strength or aerobic exercise on quality of life and knee function in patients with knee osteoarthritis. A multi-arm randomized controlled trial with 1-year follow-up. BMC Musculoskelet. Disord. 2023, 24, 714. [Google Scholar] [CrossRef] [PubMed]
- Rejeski, W.J.; Martin, K.; Ettinger, W.H.; Morgan, T. Treating Disability in knee osteoarthritis with exercise therapy: A central role for self-efficacy and pain. Arthritis Care Res. 1998, 11, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Messier, S.P.; Thompson, C.D.; Ettinger, W.H. Effects of long-term aerobic or weight training regimens on gait in an older, osteoarthritic population. J. Appl. Biomech. 1997, 13, 205–225. [Google Scholar] [CrossRef]
- Penninx, B.W.J.H.; Rejeski, W.J.; Pandya, J.; Miller, M.E.; Di Bari, M.; Applegate, W.B.; Pahor, M. Exercise and depressive symptoms: A comparison of aerobic and resistance exercise effects on emotional and physical function in older persons with high and low depressive symptomatology. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2002, 57, 124–132. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Fuentes, J.; da Costa, B.R.; Saltaji, H.; Ha, C.; Cummings, G.G. Blinding in Physical Therapy Trials and Its Association with Treatment Effects. Am. J. Phys. Med. Rehabil. 2017, 96, 34–44. [Google Scholar] [CrossRef] [PubMed]
- Kamper, S.J. Blinding: Linking evidence to practice. J. Orthop. Sports Phys. Ther. 2018, 48, 825–826. [Google Scholar] [CrossRef] [PubMed]
- Vårbakken, K.; Lorås, H.; Nilsson, K.G.; Engdal, M.; Stensdotter, A.K. Relative difference in muscle strength between patients with knee osteoarthritis and healthy controls when tested bilaterally and joint-inclusive: An exploratory cross-sectional study. BMC Musculoskelet. Disord. 2019, 20, 593. [Google Scholar] [CrossRef]
- Messier, S.P.; Mihalko, S.L.; Beavers, D.P.; Nicklas, B.J.; DeVita, P.; Carr, J.J.; Hunter, D.J.; Lyles, M.; Guermazi, A.; Bennell, K.L.; et al. Effect of High-Intensity Strength Training on Knee Pain and Knee Joint Compressive Forces among Adults with Knee Osteoarthritis. JAMA 2021, 325, 646–657. [Google Scholar] [CrossRef]
- Yokoyama, M.; Iijima, H.; Kubota, K.; Kanemura, N. Exploring the modification factors of exercise therapy on biomechanical load in patients with knee osteoarthritis: A systematic review and meta-analysis. Clin. Rheumatol. 2023, 42, 1737–1752. [Google Scholar] [CrossRef]
- Ferenczi, M.A.; Bershitsky, S.Y.; Koubassova, N.A.; Kopylova, G.V.; Fernandez, M.; Narayanan, T.; Tsaturyan, A.K. Why muscle is an efficient shock absorber. PLoS ONE 2014, 9, e85739. [Google Scholar] [CrossRef] [PubMed]
- Segal, N.A.; Glass, N.A. Is Quadriceps Muscle Weakness a Risk Factor for Incident or Progressive Knee Osteoarthritis? Physician Sportsmed. 2011, 39, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Herzog, W.; Longino, D.; Clark, A. The role of muscles in joint adaptation and degeneration. Langenbeck’s Arch. Surg. 2003, 388, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Mikesky, A.E.; Meyer, A.; Thompson, K.L. Relationship between quadriceps strength and rate of loading during gait in women. J. Orthop. Res. 2000, 18, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Lluch, E.; Torres, R.; Nijs, J.; Van Oosterwijck, J. Evidence for central sensitization in patients with osteoarthritis pain: A systematic literature review. Eur. J. Pain 2014, 18, 1367–1375. [Google Scholar] [CrossRef] [PubMed]
- Fingleton, C.; Smart, K.; Moloney, N.; Fullen, B.; Doody, C. Pain sensitization in people with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 1043–1056. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Cicuttini, F.M.; Fairley, J.; Romero, L.; Estee, M.; Hussain, S.M.; Urquhart, D.M. Does aerobic exercise effect pain sensitisation in individuals with musculoskeletal pain? A systematic review. BMC Musculoskelet. Disord. 2022, 23, 113. [Google Scholar] [CrossRef] [PubMed]
- Barclay, T.H.; Richards, S.; Schoffstall, J.; Magnuson, C.; McPhee, C.; Price, J.; Aita, S.; Anderson, A.; Johnson, D.; Price, J. A pilot study on the effects of exercise on depression symptoms using levels of neurotransmitters and EEG as markers. Eur. J. Psychol. Educ. Stud. 2014, 1, 30. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Hood, S.D.; Drummond, P.D. A review of lifestyle factors that contribute to important pathways associated with major depression: Diet, sleep and exercise. J. Affect. Disord. 2013, 148, 12–27. [Google Scholar] [CrossRef]
- Klaperski, S.; von Dawans, B.; Heinrichs, M.; Fuchs, R. Effects of a 12-week endurance training program on the physiological response to psychosocial stress in men: A randomized controlled trial. J. Behav. Med. 2014, 37, 1118–1133. [Google Scholar] [CrossRef]
- Moylan, S.; Eyre, H.; Maes, M.; Baune, B.; Jacka, F.; Berk, M. Exercising the worry away: How inflammation, oxidative and nitrogen stress mediates the beneficial effect of physical activity on anxiety disorder symptoms and behaviours. Neurosci. Biobehav. Rev. 2013, 37, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Scheef, L.; Jankowski, J.; Daamen, M.; Weyer, G.; Klingenberg, M.; Renner, J.; Mueckter, S.; Schürmann, B.; Musshoff, F.; Wagner, M.; et al. An fMRI study on the acute effects of exercise on pain processing in trained athletes. Pain 2012, 153, 1702–1714. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | N (Sex Ratio) | Mean Age | ST | AT | Outcome (Tool) | Main Results |
|---|---|---|---|---|---|---|
| Ettinger et al., 1997 [34] | 290 (84 M/206 F) | ST: 68 (6) AT: 69 (6) | (n = 146) Protocol: 2 sets/10–12 rep, 9 exercise (upper/lower) 40 m Frequency: 3 d/w Program duration: 18 months (3 month supervised/15 month home-based) | (n = 144) Protocol: 40 min 50-walking 70% HR Frequency: 3 d/w Program duration: 18 months |
| No differences between groups |
| Messier et al., 1997 (secondary analysis of Ettinger et al.) [39] | 67 (17 M/50 F) | ST: 67.2 ± 0.9 AT: 70.3 ± 1.3 | (n = 34) Protocol: 2 sets/10–12 rep, 9 exercise (upper/lower) 40 m Frequency: 3 d/w Program duration: 18 months (3 month supervised/15 month home-based) | (n = 33) Protocol: 40 m walking 50–85% HR Frequency: 3 d/w Program duration: 18 months (3 month supervised/15 month home-based) |
| No differences between groups |
| Rejeski et al., 1998 (analysis of Ettinger et al.) [38] | 357 (104 M/253 F) | NR | Protocol: 2 sets/10–12 rep, 9 exercise (upper/lower) 40 m Frequency: 3 d/w Program duration: 18 months (3 month supervised/15 month home-based) | Protocol: 40 m walking 50–75% HR Frequency: 3 d/w Program duration: 18 months (3 month supervised/15 month home-based) |
| No differences between groups |
| Samut et al., 2015 [35] | 29 (NR) | ST: 62.46 (7.71) AT: 57.57 (5.79) | (n = 15) Protocol: 5 concentric flexion and extension at angular velocities of 60°, 90°, 120°, 180°/s Frequency: 3 d/w Program duration:1.5 months | (n = 14) Protocol: walking. 1–4 week 65–70% HR/5–6 week 70–75% HR Frequency: 3 d/w Program duration: 1.5 months |
| No differences between groups |
| Küçük et al., 2017 A [36] | 45 (45 F) | ST: 51.5 (5) AT: 52.5 (5.3) | (n = 15) Protocol: 10 isokinetic flexion-extension at 60, 90, 120, 150, 180°/s Frequency: 5 d/w Program duration: 1 month | (n = 15) Protocol: 4.5 km/h walking Frequency: 5 d/w Program duration: 1 month |
| No differences between groups |
| Küçük et al., 2017 B [36] | 45 (45 F) | ST: 52.3 (6.9) AT: 52.5 (5.3) | (n = 15) Protocol: 10 reps quadriceps isometric at 90° and 180° Frequency: 5 d/w Program duration: 1 month | (n = 15) Protocol: 4.5 km/h walking Frequency: 5 d/w Program duration: 1 month |
| No differences between groups |
| Olestad et al., 2023 [37] | 107 (49 M/57 F) | ST: 57.6 (6.6) AT: 57.3 (7.1) | (n = 54) Protocol: 1 set/8–12 rep, 6 exercise (lower) Frequency: 2–3 d/w Program duration: 3 months | (n = 53) Protocol: 30 m cycling 70–80% HR Frequency: 2–3 d/w Program duration: 3 months |
| No differences between groups |
| Certainty Assesment | No. of Patients | Effect | Certainty | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Studies | Study Design | Risk of Bias | Inconsisntency | Indirectness | Imprecission | Other Considerations | [ST] | [AT] | Relative (95% CI) | Absolute (95% CI) | ||
| Pain intensity | ||||||||||||
| 3 | RCTs | Very serious a | not serious | serious b | Not serious | none | 215 | 211 | - | SMD 0.02; 95%CI: −0.15, 0.19 | ⨁◯◯◯ Very low | |
| Physical function | ||||||||||||
| 3 | RCTs | Very serious a | not serious | serious b | Not serious | none | 215 | 211 | - | SMD: 0.07; 95%CI: −0.10, 0.24 | ⨁◯◯◯ Very low | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ceballos-Laita, L.; Lahuerta-Martín, S.; Carrasco-Uribarren, A.; Cabanillas-Barea, S.; Hernández-Lázaro, H.; Pérez-Guillén, S.; Jiménez-del-Barrio, S. Strength Training vs. Aerobic Training for Managing Pain and Physical Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 33. https://doi.org/10.3390/healthcare12010033
Ceballos-Laita L, Lahuerta-Martín S, Carrasco-Uribarren A, Cabanillas-Barea S, Hernández-Lázaro H, Pérez-Guillén S, Jiménez-del-Barrio S. Strength Training vs. Aerobic Training for Managing Pain and Physical Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Healthcare. 2024; 12(1):33. https://doi.org/10.3390/healthcare12010033
Chicago/Turabian StyleCeballos-Laita, Luis, Silvia Lahuerta-Martín, Andoni Carrasco-Uribarren, Sara Cabanillas-Barea, Héctor Hernández-Lázaro, Silvia Pérez-Guillén, and Sandra Jiménez-del-Barrio. 2024. "Strength Training vs. Aerobic Training for Managing Pain and Physical Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis" Healthcare 12, no. 1: 33. https://doi.org/10.3390/healthcare12010033
APA StyleCeballos-Laita, L., Lahuerta-Martín, S., Carrasco-Uribarren, A., Cabanillas-Barea, S., Hernández-Lázaro, H., Pérez-Guillén, S., & Jiménez-del-Barrio, S. (2024). Strength Training vs. Aerobic Training for Managing Pain and Physical Function in Patients with Knee Osteoarthritis: A Systematic Review and Meta-Analysis. Healthcare, 12(1), 33. https://doi.org/10.3390/healthcare12010033