
Influence of Health Insurance Coverage on the Survival Rate for Primary Total Knee Arthroplasty: Minimum 5-Year Follow-Up Analysis


Abstract
1. Introduction
2. Materials and Methods
2.1. Health Insurance Coverage
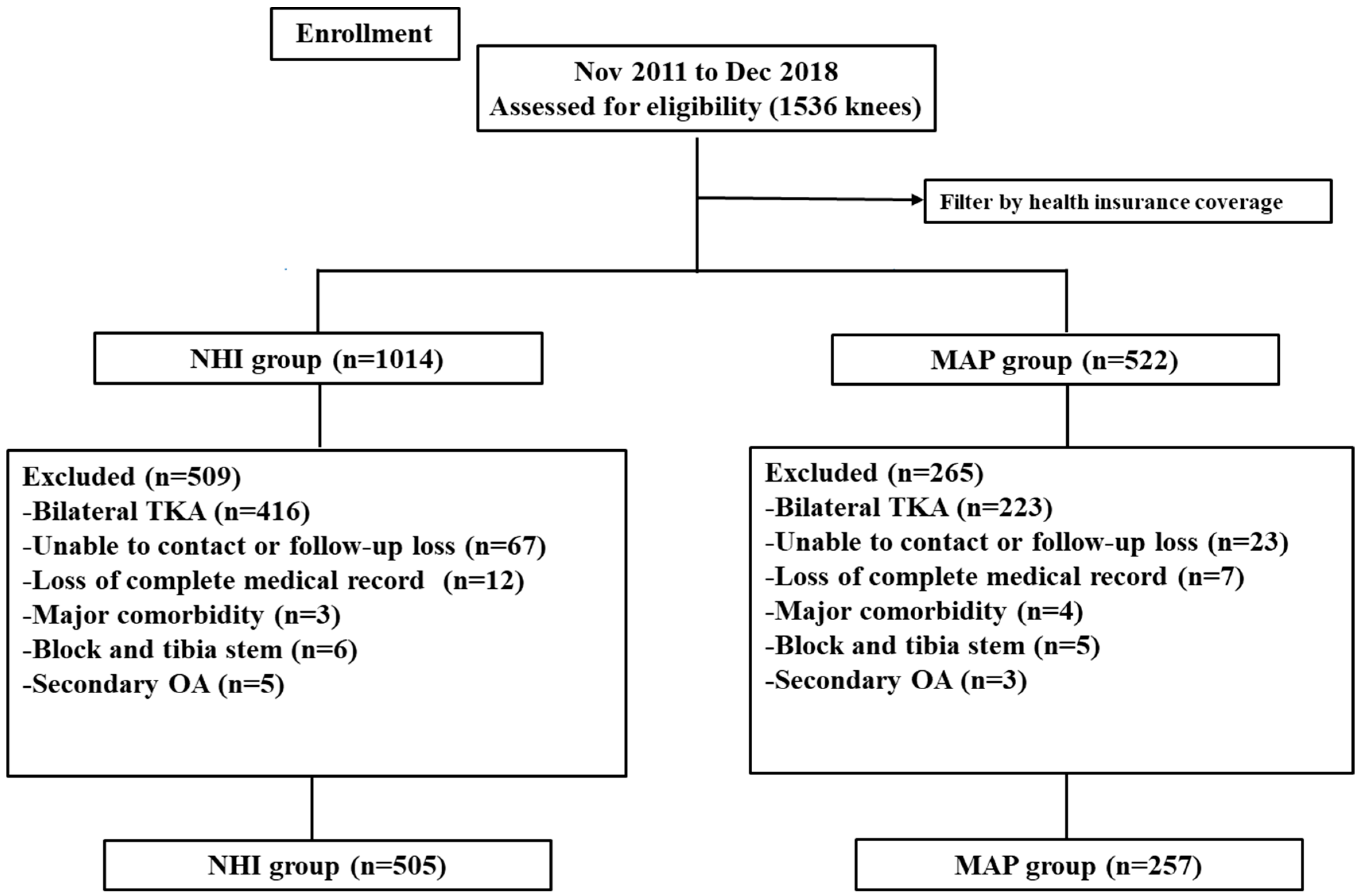
2.2. Study Design and Patients
2.3. Surgical Methods and Postoperative Management
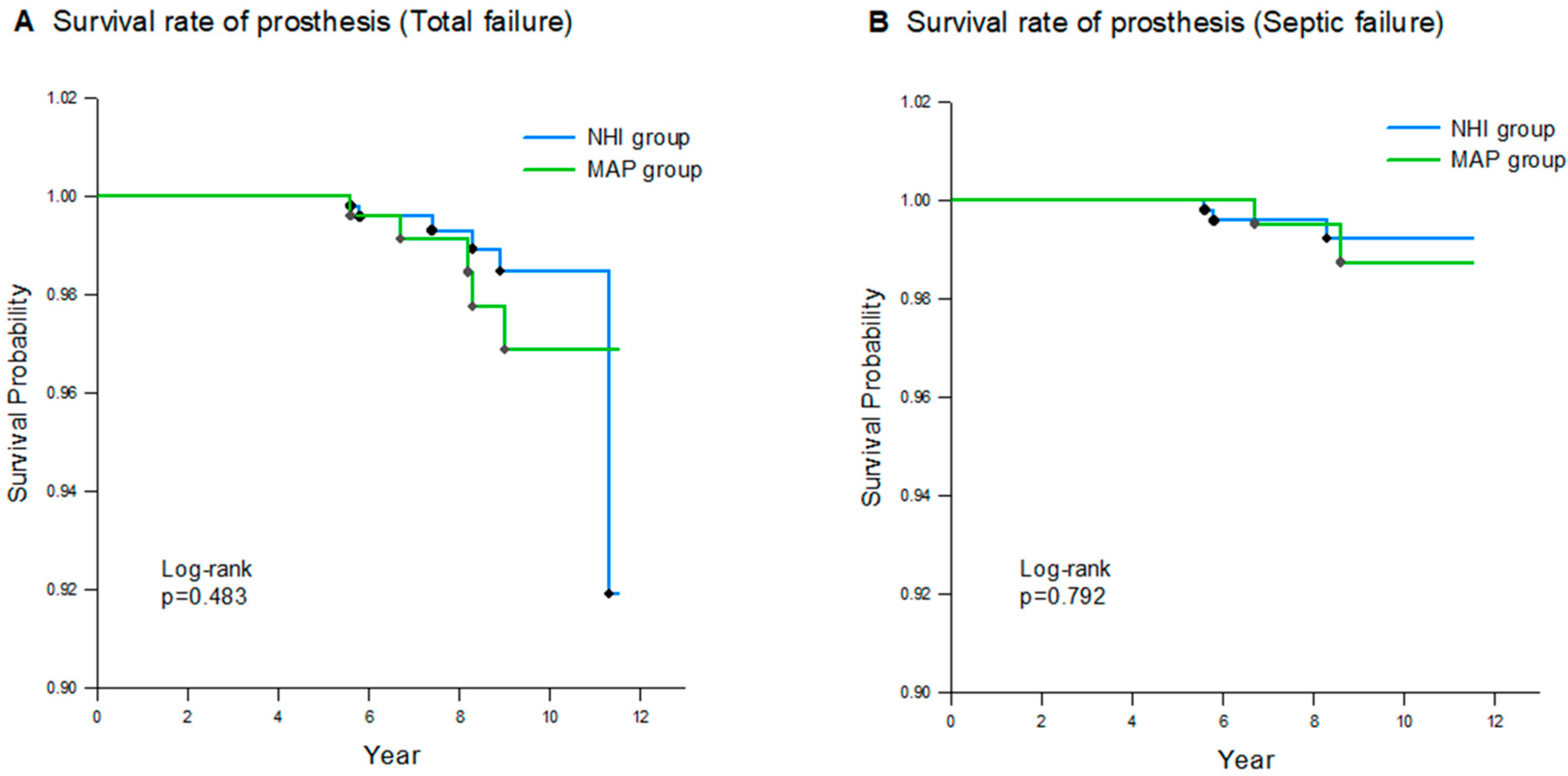
2.4. Clinical Evaluations and Survival Rate
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gill, G.S.; Joshi, A.B.; Mills, D.M. Total Condylar Knee Arthroplasty: 16- to 21-Year Results. Clin. Orthop. Relat. Res. 1999, 367, 210–215. [Google Scholar] [CrossRef]
- Suleiman, L.I.; Manista, G.C.; Sherman, A.E.; Adhia, A.H.; Karas, V.; Sporer, S.M.; Levine, B.R. The impact of race and socioeconomic status on total joint arthroplasty care. J. Arthroplast. 2021, 36, 2729–2733. [Google Scholar] [CrossRef] [PubMed]
- Martsolf, G.R.; Barrett, M.L.; Weiss, A.J.; Kandrack, R.; Washington, R.; Steiner, C.A.; Mehrotra, A.; SooHoo, N.F.; Coffey, R. Impact of race/ethnicity and socioeconomic status on risk-adjusted hospital readmission rates following hip and knee arthroplasty. JBJS 2016, 98, 1385–1391. [Google Scholar] [CrossRef] [PubMed]
- Barrack, R.L.; Ruh, E.L.; Chen, J.; Lombardi, A.V.; Berend, K.R.; Parvizi, J.; Della Valle, C.J.; Hamilton, W.G.; Nunley, R.M. Impact of socioeconomic factors on outcome of total knee arthroplasty. Clin. Orthop. Relat. Res. 2014, 472, 86–97. [Google Scholar] [CrossRef] [PubMed]
- Davis, E.T.; Lingard, E.A.; Schemitsch, E.H.; Waddell, J.P. Effects of socioeconomic status on patients’ outcome after total knee arthroplasty. Int. J. Qual. Health Care 2008, 20, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Penson, D.F.; Stoddard, M.L.; Pasta, D.J.; Lubeck, D.P.; Flanders, S.C.; Litwin, M.S. The association between socioeconomic status, health insurance coverage, and quality of life in men with prostate cancer. J. Clin. Epidemiol. 2001, 54, 350–358. [Google Scholar] [CrossRef] [PubMed]
- Veltre, D.R.; Yi, P.H.; Sing, D.C.; Curry, E.J.; Endo, A.; Smith, E.L.; Li, X. Insurance status affects in-hospital complication rates after total knee arthroplasty. Orthopedics 2018, 41, e340–e347. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, B.D.; Hulst, J.B.; Moric, M.; Levine, B.R.; Sporer, S.M. The effect of payer type on clinical outcomes in total knee arthroplasty. J. Arthroplast. 2014, 29, 295–298. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.L.; LaPar, D.J.; Mulloy, D.P.; Rasmussen, S.K.; Kane, B.J.; McGahren, E.D.; Rodgers, B.M. Primary payer status is significantly associated with postoperative mortality, morbidity, and hospital resource utilization in pediatric surgical patients within the United States. J. Pediatr. Surg. 2013, 48, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Inneh, I.A. The combined influence of sociodemographic, preoperative comorbid and intraoperative factors on longer length of stay after elective primary total knee arthroplasty. J. Arthroplast. 2015, 30, 1883–1886. [Google Scholar] [CrossRef] [PubMed]
- Browne, J.A.; Novicoff, W.M.; D’Apuzzo, M.R. Medicaid payer status is associated with in-hospital morbidity and resource utilization following primary total joint arthroplasty. JBJS 2014, 96, e180. [Google Scholar] [CrossRef] [PubMed]
- Courtney, P.M.; Huddleston, J.I.; Iorio, R.; Markel, D.C. Socioeconomic risk adjustment models for reimbursement are necessary in primary total joint arthroplasty. J. Arthroplast. 2017, 32, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.-H.; Lee, K.-S.; Yoo, K.-B.; Park, E.-C. The differences in health care utilization between Medical Aid and health insurance: A longitudinal study using propensity score matching. PLoS ONE 2015, 10, e0119939. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Jang, J.; Choi, D.-W.; Jang, S.-I.; Park, E.-C. The effect of shifting medical coverage from National Health Insurance to Medical Aid type I and type II on health care utilization and out-of-pocket spending in South Korea. BMC Health Serv. Res. 2020, 20, 979. [Google Scholar] [CrossRef]
- Sohn, M.; Jung, M. Effects of public and private health insurance on medical service utilization in the National Health Insurance System: National panel study in the Republic of Korea. BMC Health Serv. Res. 2016, 16, 503. [Google Scholar] [CrossRef] [PubMed]
- Braun, H.J.; Gold, G.E. Diagnosis of osteoarthritis: Imaging. Bone 2012, 51, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Daines, B.K.; Dennis, D.A. Gap balancing vs. measured resection technique in total knee arthroplasty. Clin. Orthop. Surg. 2014, 6, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Liow, R.Y.; Walker, K.; Wajid, M.A.; Bedi, G.; Lennox, C.M. The reliability of the American Knee Society score. Acta Orthop. Scand. 2000, 71, 603–608. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.T.; Callaghan, J.J.; Liu, S.S.; Gao, Y.; Warth, L.C.; Johnston, R.C. Disparity in total joint arthroplasty patient comorbidities, demographics, and postoperative outcomes based on insurance payer type. J. Arthroplast. 2012, 27, 1761–1765.e1. [Google Scholar] [CrossRef] [PubMed]
- D’Apuzzo, M.R.; Villa, J.M.; Alcerro, J.C.; Rossi, M.D.; Lavernia, C.J. Total joint arthroplasty: A granular analysis of outcomes in the economically disadvantaged patient. J. Arthroplast. 2016, 31, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Hinman, A.; Bozic, K.J. Impact of payer type on resource utilization, outcomes and access to care in total hip arthroplasty. J. Arthroplast. 2008, 23, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Halawi, M.J.; Cote, M.P.; Savoy, L.; Williams, V.J.; Lieberman, J.R. The effect of payer type on patient-reported outcomes in total joint arthroplasty is modulated by baseline patient characteristics. J. Arthroplast. 2019, 34, 1072–1075. [Google Scholar] [CrossRef]
- Argenson, J.-N.; Boisgard, S.; Parratte, S.; Descamps, S.; Bercovy, M.; Bonnevialle, P.; Briard, J.-L.; Brilhault, J.; Chouteau, J.; Nizard, R. Survival analysis of total knee arthroplasty at a minimum 10 years’ follow-up: A multicenter French nationwide study including 846 cases. Orthop. Traumatol. Surg. Res. 2013, 99, 385–390. [Google Scholar] [CrossRef]
- Nakamura, S.; Kobayashi, M.; Ito, H.; Nakamura, K.; Ueo, T.; Nakamura, T. The Bi-Surface total knee arthroplasty: Minimum 10-year follow-up study. Knee 2010, 17, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Vogt, J.-C.; Saarbach, C. LCS mobile-bearing total knee replacement. A 10-year’s follow-up study. Orthop. Traumatol. Surg. Res. 2009, 95, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Dall’Oca, C.; Ricci, M.; Vecchini, E.; Giannini, N.; Lamberti, D.; Tromponi, C.; Magnan, B. Evolution of TKA design. Acta Bio Medica Atenei Parm. 2017, 88, 17–31. [Google Scholar]
- Begum, F.A.; Kayani, B.; Magan, A.A.; Chang, J.S.; Haddad, F.S. Current concepts in total knee arthroplasty: Mechanical, kinematic, anatomical, and functional alignment. Bone Jt. Open 2021, 2, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Tornese, D.; Robustelli, A.; Ricci, G.; Rancoita, P.M.V.; Maffulli, N.; Peretti, G.M. Predictors of postoperative hospital length of stay after total knee arthroplasty. Singap. Med. J. 2024, 65, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Mathijssen, N.M.; Verburg, H.; van Leeuwen, C.C.; Molenaar, T.L.; Hannink, G. Factors influencing length of hospital stay after primary total knee arthroplasty in a fast-track setting. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2692–2696. [Google Scholar] [CrossRef]
- Skura, B.W.; Goubeaux, C.; Passias, B.J.; Schuette, H.B.; Melaragno, A.J.; Glazier, M.T.; Faherty, M.; Burgette, W. Increased length of stay following total joint arthroplasty based on insurance type. Arch. Orthop. Trauma Surg. 2023, 143, 2273–2281. [Google Scholar] [CrossRef] [PubMed]
- Bahk, J.; Kang, H.-Y.; Khang, Y.-H. Age-and cause-specific contributions to the life expectancy gap between Medical Aid recipients and National Health Insurance beneficiaries in Korea, 2008–2017. PLoS ONE 2020, 15, e0241755. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variables | NHI Group (n = 505) | MAP Group (n = 257) | p-Value |
|---|---|---|---|
| Sex (male/female) | 93/412 | 54/203 | 0.391 |
| Mean age (years) | 73.0 ± 6.7 | 72.5 ± 6.4 | 0.386 |
| Mean BMI (kg/m2) | 27.1 ± 5.3 | 27.4 ± 5.3 | 0.375 |
| Mean ASA score | 0.214 | ||
| 1 | 40 (7.9) | 17 (6.6) | |
| 2 | 377 (74.7) | 182 (70.8) | |
| 3 | 88 (17.4) | 58 (22.6) | |
| Comorbidity | 0.527 | ||
| Hypertension | 377 (74.7) | 207 (80.5) | |
| Diabetes mellitus | 243 (48.1) | 143 (55.6) | |
| Angina | 74 (14.7) | 51 (19.8) | |
| Stroke/CVA | 47 (9.3) | 28 (10.9) | |
| CKD | 24 (4.8) | 21 (8.2) | |
| Preoperative HKA angle (°) | −8.2 ± 6.4 | −8.9 ± 6.6 | 0.661 |
| Preoperative K-L grade (3/4) | 78/427 | 42/215 | 0.748 |
| Length of hospital stay (days) | 13.1 ± 0.9 | 13.4 ± 1.6 | 0.031 |
| Follow-up period (years) | 8.3 ± 1.8 | 8.5 ± 1.8 | 0.176 |
| Implant | NHI Group | MAP Group | p-Value a |
|---|---|---|---|
| (n = 505 Knees) | (n = 257 Knees) | ||
| 0.002 | |||
| Vanguard, Biomet | 105 (20.8) | 76 (29.6) | |
| Scorpio NRG, Stryker | 112 (22.2) | 67 (26.1) | |
| Genesis, Smith-nephew | 142 (28.1) | 57 (22.2) | |
| Optetrak, Exactech | 84 (16.6) | 22 (8.7) | |
| Lospa, Corentec | 62 (12.3) | 35 (13.6) |
| NHI Group (n = 505) | MAP Group (n = 257) | p-Value a | |
|---|---|---|---|
| Preoperative | |||
| AKS knee score | 31.9 ± 12.5 | 25.1 ± 12.1 | <0.001 |
| AKS function score | 29.8 ± 11.6 | 23.5 ± 11.9 | <0.001 |
| FC (°) | 8.6 ± 8.3 | 8.9 ± 8.7 | 0.623 |
| FF (°) | 124.8 ± 10.5 | 125.1 ± 9.3 | 0.620 |
| Postoperative | |||
| AKS knee score | 92.3 ± 4.8 | 85.0 ± 4.8 | <0.001 |
| AKS function score | 92.4 ± 4.7 | 85.5 ± 4.6 | <0.001 |
| FC (°) | 1.2 ± 2.5 | 1.4 ± 2.5 | 0.649 |
| FF (°) | 129.0 ± 2.7 | 128.9 ± 3.1 | 0.176 |
| Improvement from preoperative | |||
| AKS knee score | 60.4 ± 13.4 | 60.0 ± 12.8 | 0.659 |
| AKS function score | 62.5 ± 12.9 | 62.0 ± 12.3 | 0.575 |
| FC (°) | 7.4 ± 7.9 | 7.5 ± 8.6 | 0.879 |
| FF (°) | 4.2 ± 9.9 | 3.8 ± 8.8 | 0.509 |
| Variables | NHI Group (n = 505 Knees) | MAP Group (n = 257 Knees) |
|---|---|---|
| Stiffness | 5 (1) | 2 (0.8) |
| Hemarthrosis | 3 (0.6) | 1 (0.4) |
| Proximal DVT | 4 (0.8) | 2 (0.8) |
| Patella tendon rupture | 2 (0.4) | 1 (0.4) |
| Cellulitis (away from surgical site) | 7 (1.4) | 4 (1.6) |
| Wound dehiscence | 10 (2.0) | 5 (1.9) |
| Superficial SSI | 7 (1.4) | 4 (1.6) |
| PJI | 3 (0.6) | 2 (0.8) |
| Aseptic loosening | 2 (0.4) | 2 (0.8) |
| Dislocation/instability | 1 (0.2) | 1 (0.4) |
| Periprosthetic fracture | 5 (1) | 3 (1.2) |
| 90-day readmission | 15 (3.0) | 9 (3.5) |
| Variables | NHI Group (n = 505 Knees) | MAP Group (n = 257 Knees) | p-Value a |
|---|---|---|---|
| Pneumonia | 3 (0.6) | 5 (1.9) | 0.127 |
| Pulmonary embolism | 1 (0.2) | 1 (0.4) | 1 |
| Stroke/CVA | 2 (0.4) | 3 (1.2) | 0.342 |
| Myocardial infarction | 2 (0.4) | 3 (1.2) | 0.342 |
| Sepsis | 1 (0.2) | 1 (0.4) | 1 |
| Death | 1 (0.2) | 2 (0.8) | 0.264 |
| Transferred to other departments | 7 (1.4) | 10 (3.9) | 0.037 |
| 90-day readmission | 7 (1.4) | 7 (2.7) | 0.253 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seo, J.-S.; Bae, J.-K.; Shin, S.-K.; Ryu, H.-G.; Kim, K.J.; Cho, S.Y. Influence of Health Insurance Coverage on the Survival Rate for Primary Total Knee Arthroplasty: Minimum 5-Year Follow-Up Analysis. Healthcare 2024, 12, 1601. https://doi.org/10.3390/healthcare12161601
Seo J-S, Bae J-K, Shin S-K, Ryu H-G, Kim KJ, Cho SY. Influence of Health Insurance Coverage on the Survival Rate for Primary Total Knee Arthroplasty: Minimum 5-Year Follow-Up Analysis. Healthcare. 2024; 12(16):1601. https://doi.org/10.3390/healthcare12161601
Chicago/Turabian StyleSeo, Jae-Sung, Jung-Kwon Bae, Seong-Kee Shin, Hyung-Gon Ryu, Kyu Jin Kim, and Seung Yeon Cho. 2024. "Influence of Health Insurance Coverage on the Survival Rate for Primary Total Knee Arthroplasty: Minimum 5-Year Follow-Up Analysis" Healthcare 12, no. 16: 1601. https://doi.org/10.3390/healthcare12161601
APA StyleSeo, J.-S., Bae, J.-K., Shin, S.-K., Ryu, H.-G., Kim, K. J., & Cho, S. Y. (2024). Influence of Health Insurance Coverage on the Survival Rate for Primary Total Knee Arthroplasty: Minimum 5-Year Follow-Up Analysis. Healthcare, 12(16), 1601. https://doi.org/10.3390/healthcare12161601