_Rachiotis.png)
Association between Workplace Bullying, Job Stress, and Professional Quality of Life in Nurses: A Systematic Review and Meta-Analysis





Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources and Strategy
2.2. Selection and Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
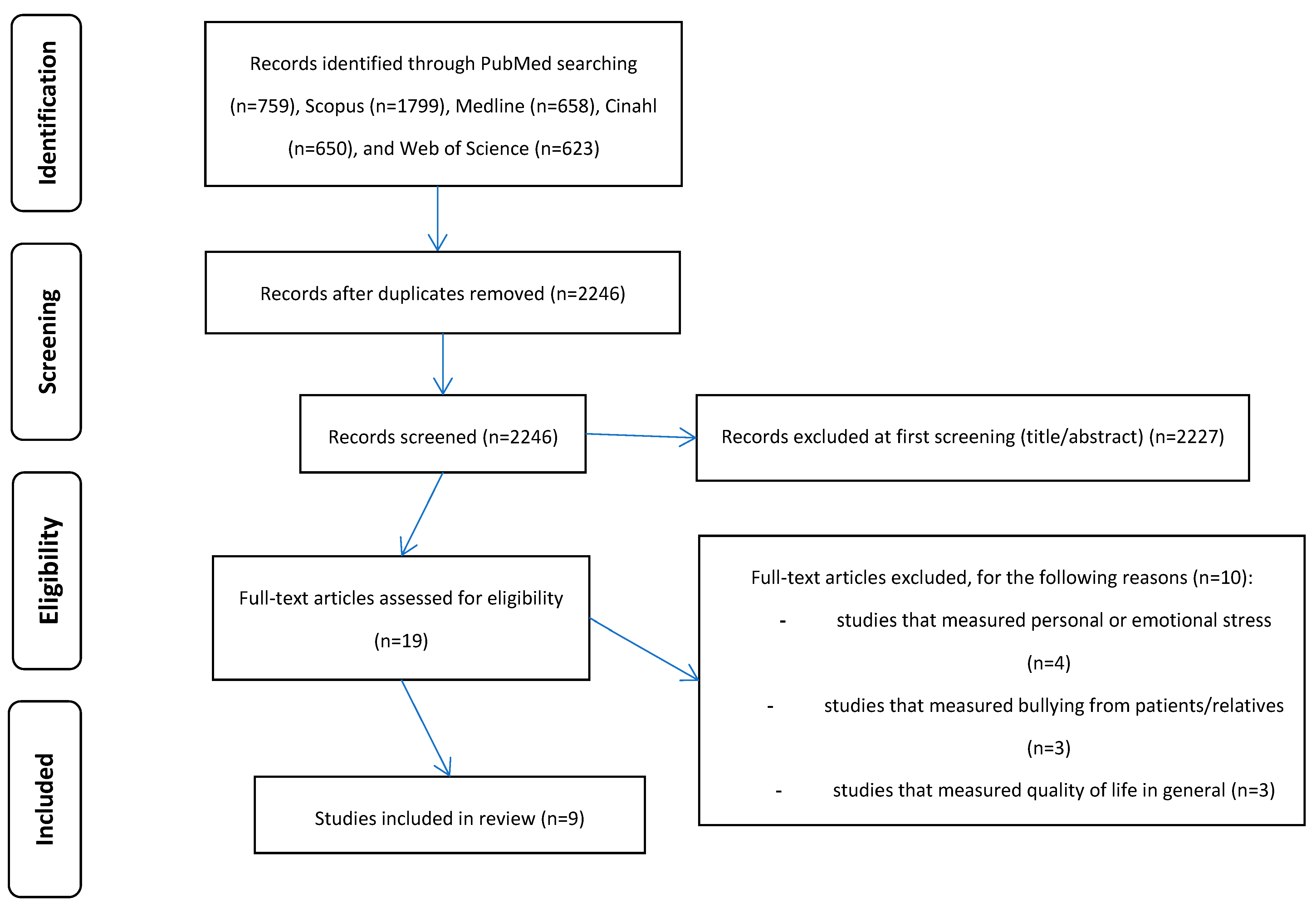
3.1. Identification and Selection of Studies
3.2. Characteristics of the Studies
3.3. Quality Assessment
3.4. Meta-Analysis
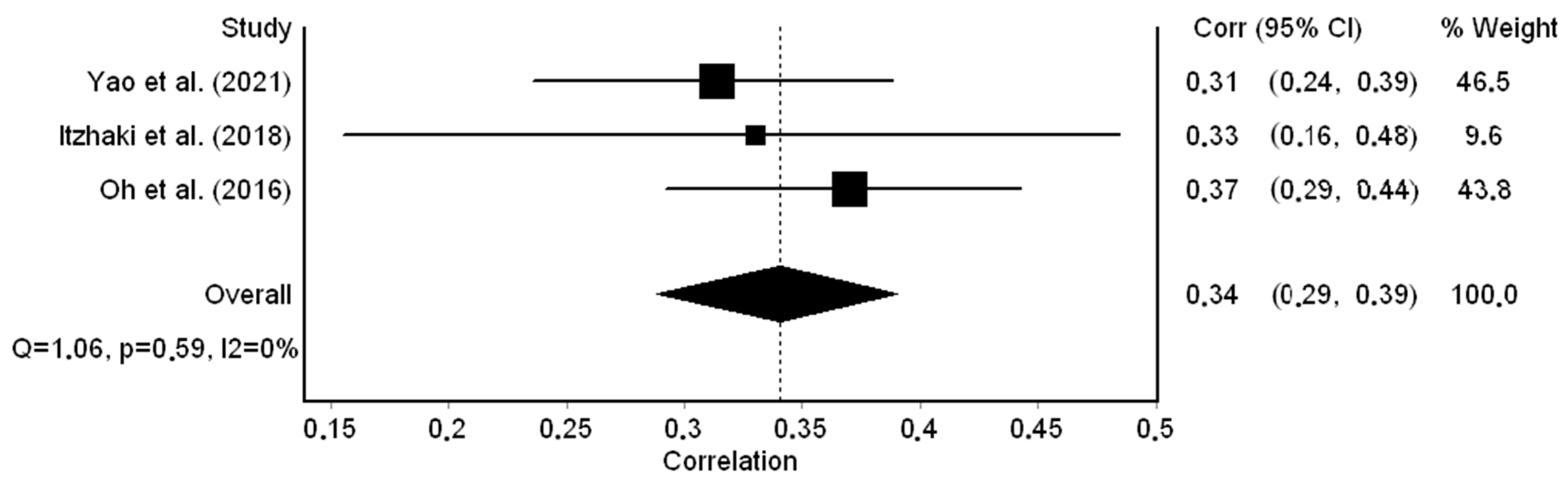
3.4.1. Workplace Bullying and Job Stress
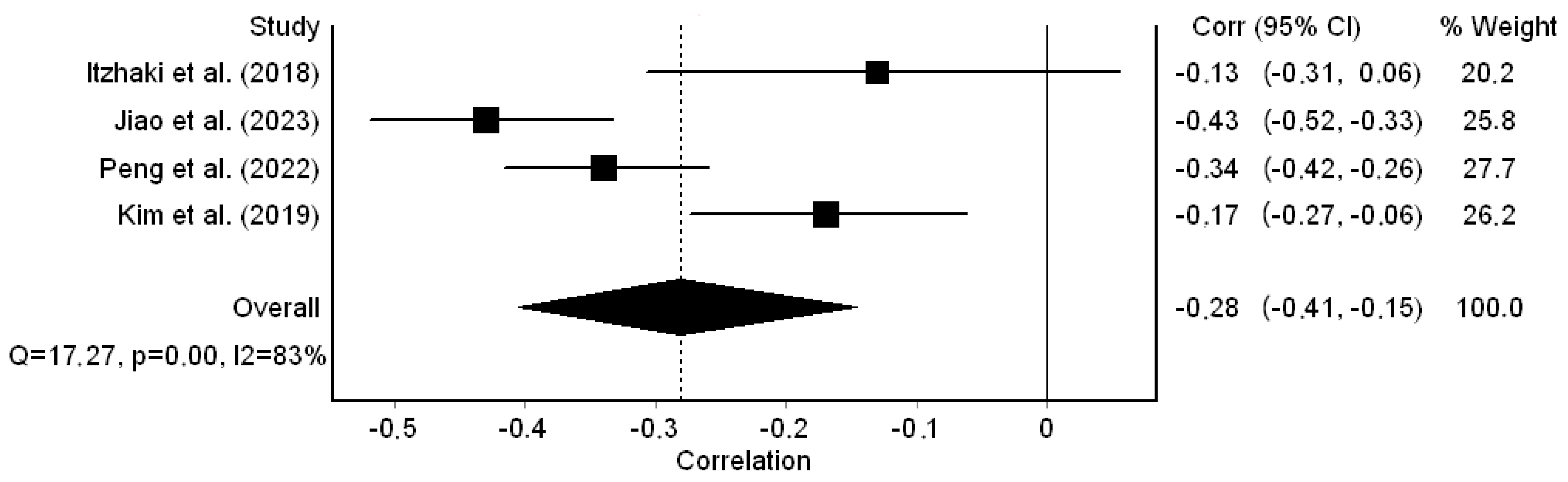
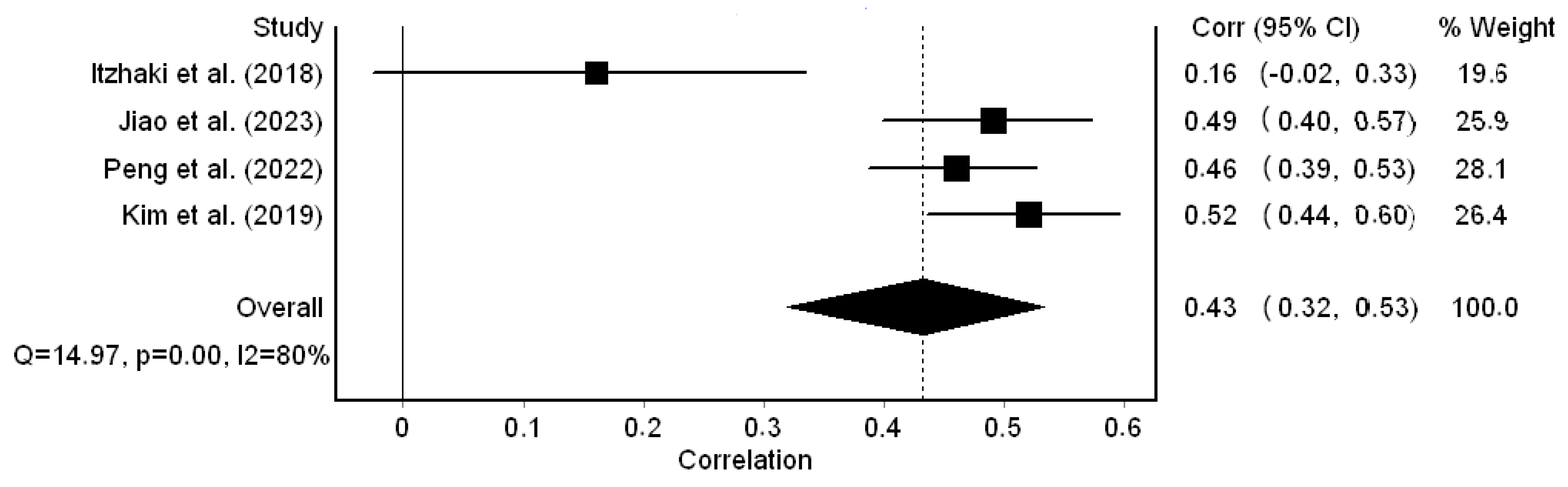
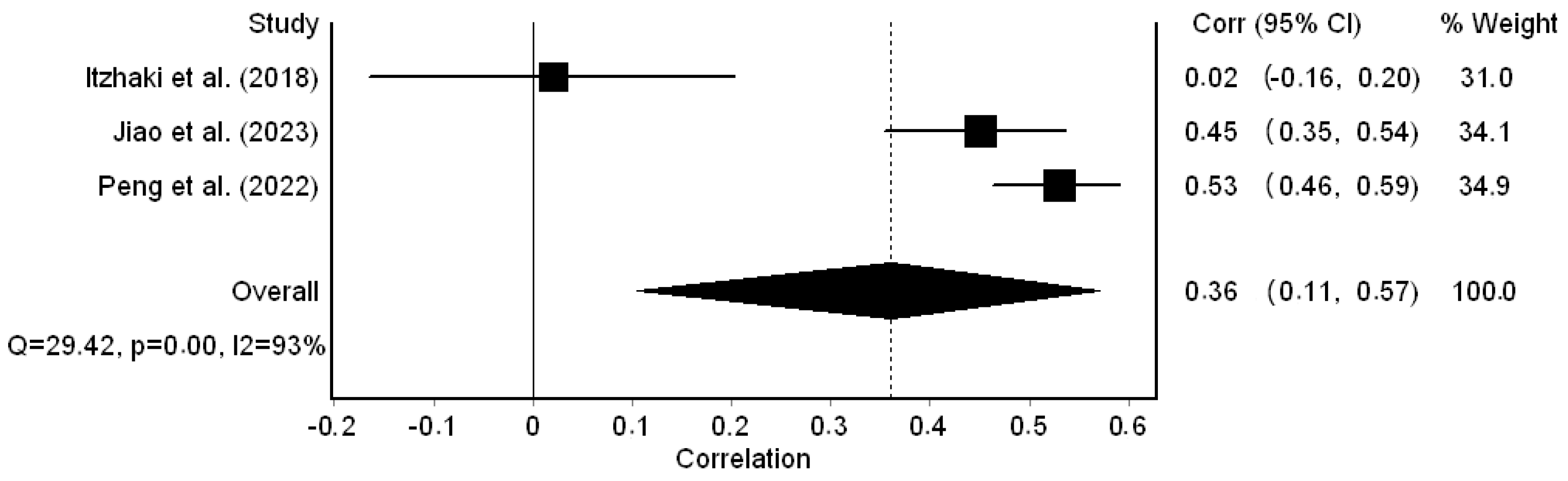
3.4.2. Workplace Bullying and Professional Quality of Life
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Einarsen, S. Harassment and Bullying at Work. Aggress. Violent Behav. 2000, 5, 379–401. [Google Scholar] [CrossRef]
- Purpora, C.; Cooper, A.; Sharifi, C.; Lieggi, M. Workplace Bullying and Risk of Burnout in Nurses: A Systematic Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 2532–2540. [Google Scholar] [CrossRef]
- Lever, I.; Dyball, D.; Greenberg, N.; Stevelink, S.A.M. Health Consequences of Bullying in the Healthcare Workplace: A Systematic Review. J. Adv. Nurs. 2019, 75, 3195–3209. [Google Scholar] [CrossRef] [PubMed]
- Trépanier, S.-G.; Fernet, C.; Austin, S. Workplace Psychological Harassment in Canadian Nurses: A Descriptive Study. J. Health Psychol. 2013, 18, 383–396. [Google Scholar] [CrossRef]
- Devonish, D. Workplace Bullying, Employee Performance and Behaviors: The Mediating Role of Psychological Well-Being. Empl. Relat. 2013, 35, 630–647. [Google Scholar] [CrossRef]
- Alshawush, K.; Hallett, N.; Bradbury-Jones, C. The Impact of Transition Programmes on Workplace Bullying, Violence, Stress and Resilience for Students and New Graduate Nurses: A Scoping Review. J. Clin. Nurs. 2022, 31, 2398–2417. [Google Scholar] [CrossRef]
- Shorey, S.; Wong, P.Z.E. A Qualitative Systematic Review on Nurses’ Experiences of Workplace Bullying and Implications for Nursing Practice. J. Adv. Nurs. 2021, 77, 4306–4320. [Google Scholar] [CrossRef] [PubMed]
- Al Omar, M.; Salam, M.; Al-Surimi, K. Workplace Bullying and Its Impact on the Quality of Healthcare and Patient Safety. Hum. Resour. Health 2019, 17, 89. [Google Scholar] [CrossRef] [PubMed]
- Serafin, L.; Sak-Dankosky, N.; Czarkowska-Pączek, B. Bullying in Nursing Evaluated by the Negative Acts Questionnaire-Revised: A Systematic Review and Meta-analysis. J. Adv. Nurs. 2020, 76, 1320–1333. [Google Scholar] [CrossRef]
- Esfahani, A.N.; Shahbazi, G. Workplace Bullying in Nursing: The Case of Azerbaijan Province, Iran. Iran. J. Nurs. Midwifery Res. 2014, 19, 409–415. [Google Scholar]
- Schlitzkus, L.L.; Vogt, K.N.; Sullivan, M.E.; Schenarts, K.D. Workplace Bullying of General Surgery Residents by Nurses. J. Surg. Educ. 2014, 71, e149–e154. [Google Scholar] [CrossRef] [PubMed]
- Shen Hsiao, S.-T.; Ma, S.-C.; Guo, S.-L.; Kao, C.-C.; Tsai, J.-C.; Chung, M.-H.; Huang, H.-C. The Role of Workplace Bullying in the Relationship between Occupational Burnout and Turnover Intentions of Clinical Nurses. Appl. Nurs. Res. 2022, 68, 151483. [Google Scholar] [CrossRef]
- Jang, S.J.; Son, Y.; Lee, H. Intervention Types and Their Effects on Workplace Bullying among Nurses: A Systematic Review. J. Nurs. Manag. 2022, 30, 1788–1800. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Lee, M. The Related Factors to Workplace Bullying in Nursing: A Systematic Review and Meta-analysis. Korean J. Adult Nurs. 2016, 28, 399. [Google Scholar] [CrossRef]
- Karatuna, I.; Jönsson, S.; Muhonen, T. Workplace Bullying in the Nursing Profession: A Cross-Cultural Scoping Review. Int. J. Nurs. Stud. 2020, 111, 103628. [Google Scholar] [CrossRef] [PubMed]
- Mohamed Ali, N.; Sayed Mohamed, H. Correlation between Workplace Violence, Work Stress, and Job Satisfaction among Psychiatric Nursing Staff. Egypt. J. Health Care 2021, 12, 1713–1730. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.D.C.; Gázquez, J.J.; Molero, M.D.M.; Oropesa, N.F.; Martos, Á. Violence and Job Satisfaction of Nurses: Importance of a Support Network in Healthcare. Eur. J. Psychol. Appl. Leg. Context 2020, 13, 21–28. [Google Scholar] [CrossRef]
- Tuna, R.; Kahraman, B. Workplace Bullying: A Qualitative Study on Experiences of Turkish Nurse Managers. J. Nurs. Manag. 2019, 27, 1159–1166. [Google Scholar] [CrossRef]
- Souza, R.C.; Silva, S.M.; Alves de Sousa Costa, M.L. Occupational Stress in Hospital Settings: Review of Coping Strategies of Nursing Professionals. Rev. Bras. Med. Trab. 2018, 16, 493–502. [Google Scholar] [CrossRef]
- Lim, J.-Y.; Kim, G.-M.; Kim, E.-J. Factors Associated with Job Stress among Hospital Nurses: A Meta-Correlation Analysis. Int. J. Environ. Res. Public. Health 2022, 19, 5792. [Google Scholar] [CrossRef]
- Labrague, L.J.; McEnroe-Petitte, D.M. Job Stress in New Nurses during the Transition Period: An Integrative Review. Int. Nurs. Rev. 2018, 65, 491–504. [Google Scholar] [CrossRef]
- Mele, F.; Buongiorno, L.; Montalbò, D.; Ferorelli, D.; Solarino, B.; Zotti, F.; Carabellese, F.F.; Catanesi, R.; Bertolino, A.; Dell’Erba, A.; et al. Reporting Incidents in the Psychiatric Intensive Care Unit: A Retrospective Study in an Italian University Hospital. J. Nerv. Ment. Dis. 2022, 210, 622–628. [Google Scholar] [CrossRef]
- Tsukamoto, S.A.S.; Galdino, M.J.Q.; Barreto, M.F.C.; Martins, J.T. Burnout Syndrome and Workplace Violence among Nursing Staff: A Cross-Sectional Study. Sao Paulo Med. J. 2022, 140, 101–107. [Google Scholar] [CrossRef]
- Hassard, J.; Teoh, K.R.H.; Visockaite, G.; Dewe, P.; Cox, T. The Cost of Work-Related Stress to Society: A Systematic Review. J. Occup. Health Psychol. 2018, 23, 1–17. [Google Scholar] [CrossRef]
- Siu, O.L.; Cooper, C.L.; Roll, L.C.; Lo, C. Occupational Stress and Its Economic Cost in Hong Kong: The Role of Positive Emotions. Int. J. Environ. Res. Public Health 2020, 17, 8601. [Google Scholar] [CrossRef] [PubMed]
- Robert, F. Impact of Workplace Bullying on Job Performance and Job Stress. J. Manag. Info 2018, 5, 12–15. [Google Scholar] [CrossRef]
- Babapour, A.-R.; Gahassab-Mozaffari, N.; Fathnezhad-Kazemi, A. Nurses’ Job Stress and Its Impact on Quality of Life and Caring Behaviors: A Cross-Sectional Study. BMC Nurs. 2022, 21, 75. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.-H.; Lee, H. Workplace Violence against Nurses in Korea and Its Impact on Professional Quality of Life and Turnover Intention. J. Nurs. Manag. 2017, 25, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Stamn, B. The Concise ProQOL Manual: The Concise Manual for the Professional Quality of Life Scale, 2nd ed.; Beth Hudnall Stamm: Pocatello, ID, USA, 2010. [Google Scholar]
- Xie, W.; Chen, L.; Feng, F.; Okoli, C.T.C.; Tang, P.; Zeng, L.; Jin, M.; Zhang, Y.; Wang, J. The Prevalence of Compassion Satisfaction and Compassion Fatigue among Nurses: A Systematic Review and Meta-Analysis. Int. J. Nurs. Stud. 2021, 120, 103973. [Google Scholar] [CrossRef] [PubMed]
- Guseva Canu, I.; Marca, S.C.; Dell’Oro, F.; Balázs, Á.; Bergamaschi, E.; Besse, C.; Bianchi, R.; Bislimovska, J.; Koscec Bjelajac, A.; Bugge, M.; et al. Harmonized Definition of Occupational Burnout: A Systematic Review, Semantic Analysis, and Delphi Consensus in 29 Countries. Scand. J. Work. Environ. Health 2021, 47, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Peng, J.; Luo, H.; Ma, Q.; Zhong, Y.; Yang, X.; Huang, Y.; Sun, X.; Wang, X.; He, J.; Song, Y. Association between Workplace Bullying and Nurses’ Professional Quality of Life: The Mediating Role of Resilience. J. Nurs. Manag. 2022, 30, 1549–1558. [Google Scholar] [CrossRef]
- Giorgi, F.; Mattei, A.; Notarnicola, I.; Petrucci, C.; Lancia, L. Can Sleep Quality and Burnout Affect the Job Performance of Shift-work Nurses? A Hospital Cross-sectional Study. J. Adv. Nurs. 2018, 74, 698–708. [Google Scholar] [CrossRef]
- Johnson, A.H.; Benham-Hutchins, M. The Influence of Bullying on Nursing Practice Errors: A Systematic Review. AORN J. 2020, 111, 199–210. [Google Scholar] [CrossRef]
- Wang, Q.; Lv, W.; Qian, R.; Zhang, Y. Job Burnout and Quality of Working Life among Chinese Nurses: A Cross-sectional Study. J. Nurs. Manag. 2019, 27, 1835–1844. [Google Scholar] [CrossRef]
- Goh, H.S.; Hosier, S.; Zhang, H. Prevalence, Antecedents, and Consequences of Workplace Bullying among Nurses—A Summary of Reviews. Int. J. Environ. Res. Public. Health 2022, 19, 8256. [Google Scholar] [CrossRef]
- Zhang, Y.; Yin, R.; Lu, J.; Cai, J.; Wang, H.; Shi, X.; Mao, L. Association between Horizontal Violence and Turnover Intention in Nurses: A Systematic Review and Meta-Analysis. Front. Public Health 2022, 10, 964629. [Google Scholar] [CrossRef]
- Jang, S.J.; Son, Y.; Lee, H. Prevalence, Associated Factors and Adverse Outcomes of Workplace Violence towards Nurses in Psychiatric Settings: A Systematic Review. Int. J. Ment. Health Nurs. 2022, 31, 450–468. [Google Scholar] [CrossRef]
- Chakraborty, S.; Mashreky, S.R.; Dalal, K. Violence against Physicians and Nurses: A Systematic Literature Review. J. Public Health 2022, 30, 1837–1855. [Google Scholar] [CrossRef]
- Wang, J.; Zeng, Q.; Wang, Y.; Liao, X.; Xie, C.; Wang, G.; Zeng, Y. Workplace Violence and the Risk of Post-traumatic Stress Disorder and Burnout among Nurses: A Systematic Review and Meta-analysis. J. Nurs. Manag. 2022, 30, 2854–2868. [Google Scholar] [CrossRef]
- Stafford, S.; Avsar, P.; Nugent, L.; O’Connor, T.; Moore, Z.; Patton, D.; Watson, C. What Is the Impact of Patient Violence in the Emergency Department on Emergency Nurses’ Intention to Leave? J. Nurs. Manag. 2022, 30, 1852–1860. [Google Scholar] [CrossRef]
- Kafle, S.; Paudel, S.; Thapaliya, A.; Acharya, R. Workplace Violence against Nurses: A Narrative Review. J. Clin. Transl. Res. 2022, 8, 421–424. [Google Scholar] [CrossRef]
- Fricke, J.; Siddique, S.M.; Douma, C.; Ladak, A.; Burchill, C.N.; Greysen, R.; Mull, N.K. Workplace Violence in Healthcare Settings: A Scoping Review of Guidelines and Systematic Reviews. Trauma Violence Abus. 2023, 24, 3363–3383. [Google Scholar] [CrossRef]
- Rossi, M.F.; Beccia, F.; Cittadini, F.; Amantea, C.; Aulino, G.; Santoro, P.E.; Borrelli, I.; Oliva, A.; Ricciardi, W.; Moscato, U.; et al. Workplace Violence against Healthcare Workers: An Umbrella Review of Systematic Reviews and Meta-Analyses. Public Health 2023, 221, 50–59. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015 Statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Porritt, K.; Gomersall, J.; Lockwood, C. JBI’s Systematic Reviews: Study Selection and Critical Appraisal. Am. J. Nurs. 2014, 114, 47–52. [Google Scholar] [CrossRef]
- Cohen, B. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; ImprintRoutledge: New York, NY, USA, 2013. [Google Scholar]
- Higgins, J. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Shi, L.; Lin, L. The Trim-and-Fill Method for Publication Bias: Practical Guidelines and Recommendations Based on a Large Database of Meta-Analyses. Medicine 2019, 98, e15987. [Google Scholar] [CrossRef]
- Wallace, B.C.; Schmid, C.H.; Lau, J.; Trikalinos, T.A. Meta-Analyst: Software for Meta-Analysis of Binary, Continuous and Diagnostic Data. BMC Med. Res. Methodol. 2009, 9, 80. [Google Scholar] [CrossRef]
- Yao, X.; Shao, J.; Wang, L.; Zhang, J.; Zhang, C.; Lin, Y. Does Workplace Violence, Empathy, and Communication Influence Occupational Stress among Mental Health Nurses? Int. J. Ment. Health Nurs. 2021, 30, 177–188. [Google Scholar] [CrossRef]
- Kwak, Y.; Han, Y.; Song, J.; Kim, J. Impact of Emotional Labour and Workplace Violence on Professional Quality of Life among Clinical Nurses. Int. J. Nurs. Pract. 2020, 26, e12792. [Google Scholar] [CrossRef]
- Itzhaki, M.; Bluvstein, I.; Peles Bortz, A.; Kostistky, H.; Bar Noy, D.; Filshtinsky, V.; Theilla, M. Mental Health Nurse’s Exposure to Workplace Violence Leads to Job Stress, Which Leads to Reduced Professional Quality of Life. Front. Psychiatry 2018, 9, 59. [Google Scholar] [CrossRef]
- Magnavita, N. Workplace Violence and Occupational Stress in Healthcare Workers: A Chicken-and-Egg Situation—Results of a 6-Year Follow-up Study. J. Nurs. Scholarsh. 2014, 46, 366–376. [Google Scholar] [CrossRef]
- Jiao, R.; Li, J.; Cheng, N.; Liu, X.; Tan, Y. The Mediating Role of Coping Styles between Nurses’ Workplace Bullying and Professional Quality of Life. BMC Nurs. 2023, 22, 459. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, E.; Lee, H. Association between Workplace Bullying and Burnout, Professional Quality of Life, and Turnover Intention among Clinical Nurses. PLoS ONE 2019, 14, e0226506. [Google Scholar] [CrossRef]
- Oh, H.; Uhm, D.; Yoon, Y.J. Workplace Bullying, Job Stress, Intent to Leave, and Nurses’ Perceptions of Patient Safety in South Korean Hospitals. Nurs. Res. 2016, 65, 380–388. [Google Scholar] [CrossRef]
- Einarsen, S.; Hoel, H.; Notelaers, G. Measuring Exposure to Bullying and Harassment at Work: Validity, Factor Structure and Psychometric Properties of the Negative Acts Questionnaire-Revised. Work Stress 2009, 23, 24–44. [Google Scholar] [CrossRef]
- Adriaenssens, J.; Hamelink, A.; Bogaert, P.V. Predictors of Occupational Stress and Well-Being in First-Line Nurse Managers: A Cross-Sectional Survey Study. Int. J. Nurs. Stud. 2017, 73, 85–92. [Google Scholar] [CrossRef]
- Kakemam, E.; Raeissi, P.; Raoofi, S.; Soltani, A.; Sokhanvar, M.; Visentin, D.C.; Cleary, M. Occupational Stress and Associated Risk Factors among Nurses: A Cross-Sectional Study. Contemp. Nurse 2019, 55, 237–249. [Google Scholar] [CrossRef]
- Simpson, K.R.; Lyndon, A.; Ruhl, C. Consequences of Inadequate Staffing Include Missed Care, Potential Failure to Rescue, and Job Stress and Dissatisfaction. J. Obstet. Gynecol. Neonatal Nurs. 2016, 45, 481–490. [Google Scholar] [CrossRef]
- Pishgooie, A.H.; Atashzadeh-Shoorideh, F.; Falcó-Pegueroles, A.; Lotfi, Z. Correlation between Nursing Managers’ Leadership Styles and Nurses’ Job Stress and Anticipated Turnover. J. Nurs. Manag. 2019, 27, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Fontes, K.B.; Alarcão, A.C.J.; Santana, R.G.; Pelloso, S.M.; Barros Carvalho, M.D. Relationship between Leadership, Bullying in the Workplace and Turnover Intention among Nurses. J. Nurs. Manag. 2019, 27, 535–542. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Lee, J.; You, S.J.; Song, K.J.; Hong, K.J. Nurse Staffing, Nurses Prioritization, Missed Care, Quality of Nursing Care, and Nurse Outcomes. Int. J. Nurs. Pract. 2020, 26, e12803. [Google Scholar] [CrossRef] [PubMed]
- Karaca, A.; Durna, Z. Patient Satisfaction with the Quality of Nursing Care. Nurs. Open 2019, 6, 535–545. [Google Scholar] [CrossRef]
- Schwendimann, R.; Blatter, C.; Dhaini, S.; Simon, M.; Ausserhofer, D. The Occurrence, Types, Consequences and Preventability of in-Hospital Adverse Events—A Scoping Review. BMC Health Serv. Res. 2018, 18, 521. [Google Scholar] [CrossRef]
- Deng, J.; Guo, Y.; Ma, T.; Yang, T.; Tian, X. How Job Stress Influences Job Performance among Chinese Healthcare Workers: A Cross-Sectional Study. Environ. Health Prev. Med. 2019, 24, 2. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.; Ojemeni, M.M.; Kalamani, R.; Tong, J.; Crecelius, M.L. Relationship between Nurse Burnout, Patient and Organizational Outcomes: Systematic Review. Int. J. Nurs. Stud. 2021, 119, 103933. [Google Scholar] [CrossRef]
- Jobe, J.A.; Gillespie, G.L.; Schwytzer, D. A National Survey of Secondary Traumatic Stress and Work Productivity of Emergency Nurses Following Trauma Patient Care. J. Trauma Nurs. 2021, 28, 243–249. [Google Scholar] [CrossRef]
- Bock, C.; Heitland, I.; Zimmermann, T.; Winter, L.; Kahl, K.G. Secondary Traumatic Stress, Mental State, and Work Ability in Nurses—Results of a Psychological Risk Assessment at a University Hospital. Front. Psychiatry 2020, 11, 298. [Google Scholar] [CrossRef]
- Hämmig, O. Work- and Stress-Related Musculoskeletal and Sleep Disorders among Health Professionals: A Cross-Sectional Study in a Hospital Setting in Switzerland. BMC Musculoskelet. Disord. 2020, 21, 319. [Google Scholar] [CrossRef]
- Galanis, P.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsoulas, T.; Moisoglou, I.; Gallos, P.; Kaitelidou, D. The Influence of Job Burnout on Quiet Quitting among Nurses: The Mediating Effect of Job Satisfaction. Res. Square 2023. [Google Scholar] [CrossRef]
- Fateminia, A.; Hasanvand, S.; Goudarzi, F.; Mohammadi, R. Post-Traumatic Stress Disorder among Frontline Nurses during the COVID-19 Pandemic and Its Relationship with Occupational Burnout. Iran. J. Psychiatry 2022, 17, 436. [Google Scholar] [CrossRef] [PubMed]
- Miguel-Puga, J.A.; Cooper-Bribiesca, D.; Avelar-Garnica, F.J.; Sanchez-Hurtado, L.A.; Colin-Martínez, T.; Espinosa-Poblano, E.; Anda-Garay, J.C.; González-Díaz, J.I.; Segura-Santos, O.B.; Vital-Arriaga, L.C.; et al. Burnout, Depersonalization, and Anxiety Contribute to Post-traumatic Stress in Frontline Health Workers at COVID-19 Patient Care, a Follow-up Study. Brain Behav. 2021, 11, e02007. [Google Scholar] [CrossRef]
- Zaghini, F.; Biagioli, V.; Proietti, M.; Badolamenti, S.; Fiorini, J.; Sili, A. The Role of Occupational Stress in the Association between Emotional Labor and Burnout in Nurses: A Cross-Sectional Study. Appl. Nurs. Res. 2020, 54, 151277. [Google Scholar] [CrossRef] [PubMed]
- Barbagianni, S.; Moisoglou, I.; Meimeti, E.; Dimitriadi, I.; Gialama, M.; Galanis, P. Quality of Working Life in Relation to Occupational Stress, Anxiety and Depression of Workers in Primary and Secondary Healthcare Workplaces. Int. J. Caring Sci. 2023, 16, 1684–1693. [Google Scholar]
- Sauer, P.A.; McCoy, T.P. Nurse Bullying: Impact on Nurses’ Health. West. J. Nurs. Res. 2017, 39, 1533–1546. [Google Scholar] [CrossRef] [PubMed]
- Edmonson, C.; Zelonka, C. Our Own Worst Enemies: The Nurse Bullying Epidemic. Nurs. Adm. Q. 2019, 43, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, N.; Jeong, S.; Smith, T. New Graduate Registered Nurses’ Exposure to Negative Workplace Behaviour in the Acute Care Setting: An Integrative Review. Int. J. Nurs. Stud. 2019, 93, 41–54. [Google Scholar] [CrossRef]
- Jarrad, R.A.; Hammad, S. Oncology Nurses’ Compassion Fatigue, Burn out and Compassion Satisfaction. Ann. Gen. Psychiatry 2020, 19, 22. [Google Scholar] [CrossRef]
- Hegney, D.G.; Craigie, M.; Hemsworth, D.; Osseiran-Moisson, R.; Aoun, S.; Francis, K.; Drury, V. Compassion Satisfaction, Compassion Fatigue, Anxiety, Depression and Stress in Registered Nurses in Australia: Study 1 Results. J. Nurs. Manag. 2014, 22, 506–518. [Google Scholar] [CrossRef]
- Sacco, T.L.; Copel, L.C. Compassion Satisfaction: A Concept Analysis in Nursing. Nurs. Forum 2018, 53, 76–83. [Google Scholar] [CrossRef]
- Balinbin, C.B.V.; Balatbat, K.T.R.; Balayan, A.N.B.; Balcueva, M.I.C.; Balicat, M.G.B.; Balidoy, T.A.S.; Macindo, J.R.B.; Torres, G.C.S. Occupational Determinants of Compassion Satisfaction and Compassion Fatigue among Filipino Registered Nurses. J. Clin. Nurs. 2020, 29, 955–963. [Google Scholar] [CrossRef]
- Hinderer, K.A.; VonRueden, K.T.; Friedmann, E.; McQuillan, K.A.; Gilmore, R.; Kramer, B.; Murray, M. Burnout, Compassion Fatigue, Compassion Satisfaction, and Secondary Traumatic Stress in Trauma Nurses. J. Trauma Nurs. 2014, 21, 160–169. [Google Scholar] [CrossRef]
- Baek, H.; Trinkoff, A.M. Bullying Experience and the Work Environment in Nurses: A Cross-sectional Data Analysis. J. Nurs. Manag. 2022, 30, 1861–1868. [Google Scholar] [CrossRef] [PubMed]
- Trépanier, S.; Peterson, C.; Fernet, C.; Austin, S.; Desrumaux, P. When Workload Predicts Exposure to Bullying Behaviours in Nurses: The Protective Role of Social Support and Job Recognition. J. Adv. Nurs. 2021, 77, 3093–3103. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ Burnout and Associated Risk Factors during the COVID-19 Pandemic: A Systematic Review and Meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, J.; Li, Y.; Bentley, S.K.; Lall, M.D.; Messman, A.M.; Liu, Y.T.; Diercks, D.B.; Merritt-Recchia, R.; Sorge, R.; Warchol, J.M.; et al. The Perceived Work Environment and Well-being: A Survey of Emergency Health Care Workers during the COVID-19 Pandemic. Acad. Emerg. Med. 2022, 29, 851–861. [Google Scholar] [CrossRef] [PubMed]
- Baek, J.; Cho, H.; Han, K.; Lee, H. Association between Nursing Work Environment and Compassion Satisfaction among Clinical Nurses. J. Nurs. Manag. 2020, 28, 368–376. [Google Scholar] [CrossRef]
- Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Meimeti, E.; Kaitelidou, D. Increased Job Burnout and Reduced Job Satisfaction for Nurses Compared to Other Healthcare Workers after the COVID-19 Pandemic. Nurs. Rep. 2023, 13, 1090–1100. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Johnson, K.L.; Bay, R.C.; Todd, M. Key Elements of the Critical Care Work Environment Associated With Burnout and Compassion Satisfaction. Am. J. Crit. Care 2021, 30, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hampton, D.; Tharp-Barrie, K.; Kay Rayens, M. Experience of Nursing Leaders with Workplace Bullying and How to Best Cope. J. Nurs. Manag. 2019, 27, 517–526. [Google Scholar] [CrossRef]
- Smith, C.R.; Palazzo, S.J.; Grubb, P.L.; Gillespie, G.L. Standing up against Workplace Bullying Behavior: Recommendations from Newly Licensed Nurses. J. Nurs. Educ. Pract. 2020, 10, 35. [Google Scholar] [CrossRef] [PubMed]
- Yosep, I.; Hikmat, R.; Mardhiyah, A. Types of Nursing Intervention to Reduce Impact of Bullying and Aggression on Nurses in the Workplace. Healthcare 2022, 10, 1463. [Google Scholar] [CrossRef] [PubMed]
- João, A.L.; Portelada, A. Coping with Workplace Bullying: Strategies Employed by Nurses in the Healthcare Setting. Nurs. Forum 2023, 2023, 8447804. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Country | Data Collection Time | Females (%) | Age, Mean (SD) | Sample Size (n) | Study Design | Sampling Method | Clinical Settings | Assessment Tool for Workplace Bullying | Assessment Tool for Job Stress | Assessment Tool for Professional QoL | Response Rate (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Yao et al. [52] | China | 2019 | 73.5 | 35.9 (8.0) | 539 | Cross-sectional | Convenience | Mental health services | Workplace violence scale | Chinese nursing stress scale | None | 97.8 |
| Kwak et al. [53] | Republic of Korea | 2016 | NR | <30 years, 66.4% | 399 | Cross-sectional | Convenience | University hospitals | Workplace violence scale | None | ProQOL | NR |
| Itzhaki et al. [54] | Israel | 2018 | 56.3 | 47.3 (9) | 114 | Cross-sectional | Convenience | Mental health services | 5-point Likert scale | 5-point Likert scale | ProQOL | NR |
| Magnavita [55] | Italy | 2003–2009 | 64.0 | 38.9 (8.7) | 698 | Follow-up | Convenience | Public health care unit | Violent incidents | Continuous scale | None | 96.5 |
| Jiao et al. [56] | China | 2022 | 92.6 | ≤35 years, 88.6% | 297 | Cross-sectional | Convenience | Tertiary hospitals | NAQR | None | ProQOL | 97.1 |
| Peng et al. [32] | China | 2021 | 93.5 | ≤35 years, 44.4% | 493 | Cross-sectional | Convenience | Tertiary hospitals | NAQR | None | ProQOL | NR |
| Kim et al. [57] | Republic of Korea | 2018 | 96.3 | NR | 324 | Cross-sectional | Convenience | Tertiary hospitals | NAQR | None | ProQOL | NR |
| Choi & Lee [28] | Republic of Korea | 2015 | 96.9 | NR | 358 | Cross-sectional | Convenience | Tertiary hospitals | Verbal and physical violence, and physical threats | None | ProQOL | NR |
| Oh et al. [58] | Republic of Korea | 2013 | 97.2 | 25.6 (3.8) | 508 | Cross-sectional | Convenience | Tertiary hospitals | NAQR | Occupational stress scale-short form | None | 95.8 |
| Reference | Association between Workplace Bullying and Job Stress | Association between Workplace Bullying and Professional QoL | |||
|---|---|---|---|---|---|
| Correlation Coefficient (p-Value) | Regression Coefficient Beta (p-Value) | Odds Ratio (p-Value) | Correlation Coefficient (p-Value) | Regression Coefficient Beta (p-Value) | |
| Yao et al. [52] | 0.31 (<0.001) | 0.06 (<0.001) | |||
| Kwak et al. [53] | CS: 0.03 (0.07); B: 0.03 (0.037); STS: 0.09 < 0.001 | ||||
| Itzhaki et al. [54] | 0.33 (<0.001) | CS: −0.13 (>0.05); B: 0.16 (>0.05); STS: 0.02 (>0.05) | CS: NR (>0.05); B: NR (>0.05); STS: NR (>0.05) | ||
| Magnavita [55] | Physical aggression: 1.18 (>0.05); Non-physical aggression: 1.81 (<0.01) | ||||
| Jiao et al. [56] | CS: −0.43 (<0.001); B: 0.49 (<0.001); STS: 0.45 (<0.001) | ||||
| Peng et al. [32] | CS: −0.34 (<0.01); B: 0.46 (<0.01); STS: 0.53 (<0.01) | ||||
| Kim et al. [57] | CS: −0.17 (<0.01); B: 0.52 (<0.01) | CS: 0.02 (0.65); B: 0.15 (<0.01) | |||
| Choi & Lee [28] | CS: 0.05 (>0.05); B: 0.03 (>0.05); STS: 0.06 (>0.05) | ||||
| Oh et al. [58] | 0.37 (<0.001) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; Mastrogianni, M. Association between Workplace Bullying, Job Stress, and Professional Quality of Life in Nurses: A Systematic Review and Meta-Analysis. Healthcare 2024, 12, 623. https://doi.org/10.3390/healthcare12060623
Galanis P, Moisoglou I, Katsiroumpa A, Mastrogianni M. Association between Workplace Bullying, Job Stress, and Professional Quality of Life in Nurses: A Systematic Review and Meta-Analysis. Healthcare. 2024; 12(6):623. https://doi.org/10.3390/healthcare12060623
Chicago/Turabian StyleGalanis, Petros, Ioannis Moisoglou, Aglaia Katsiroumpa, and Maria Mastrogianni. 2024. "Association between Workplace Bullying, Job Stress, and Professional Quality of Life in Nurses: A Systematic Review and Meta-Analysis" Healthcare 12, no. 6: 623. https://doi.org/10.3390/healthcare12060623
APA StyleGalanis, P., Moisoglou, I., Katsiroumpa, A., & Mastrogianni, M. (2024). Association between Workplace Bullying, Job Stress, and Professional Quality of Life in Nurses: A Systematic Review and Meta-Analysis. Healthcare, 12(6), 623. https://doi.org/10.3390/healthcare12060623