

FTO rs9939609: T>A Variant and Physical Inactivity as Important Risk Factors for Class III Obesity: A Cross-Sectional Study

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
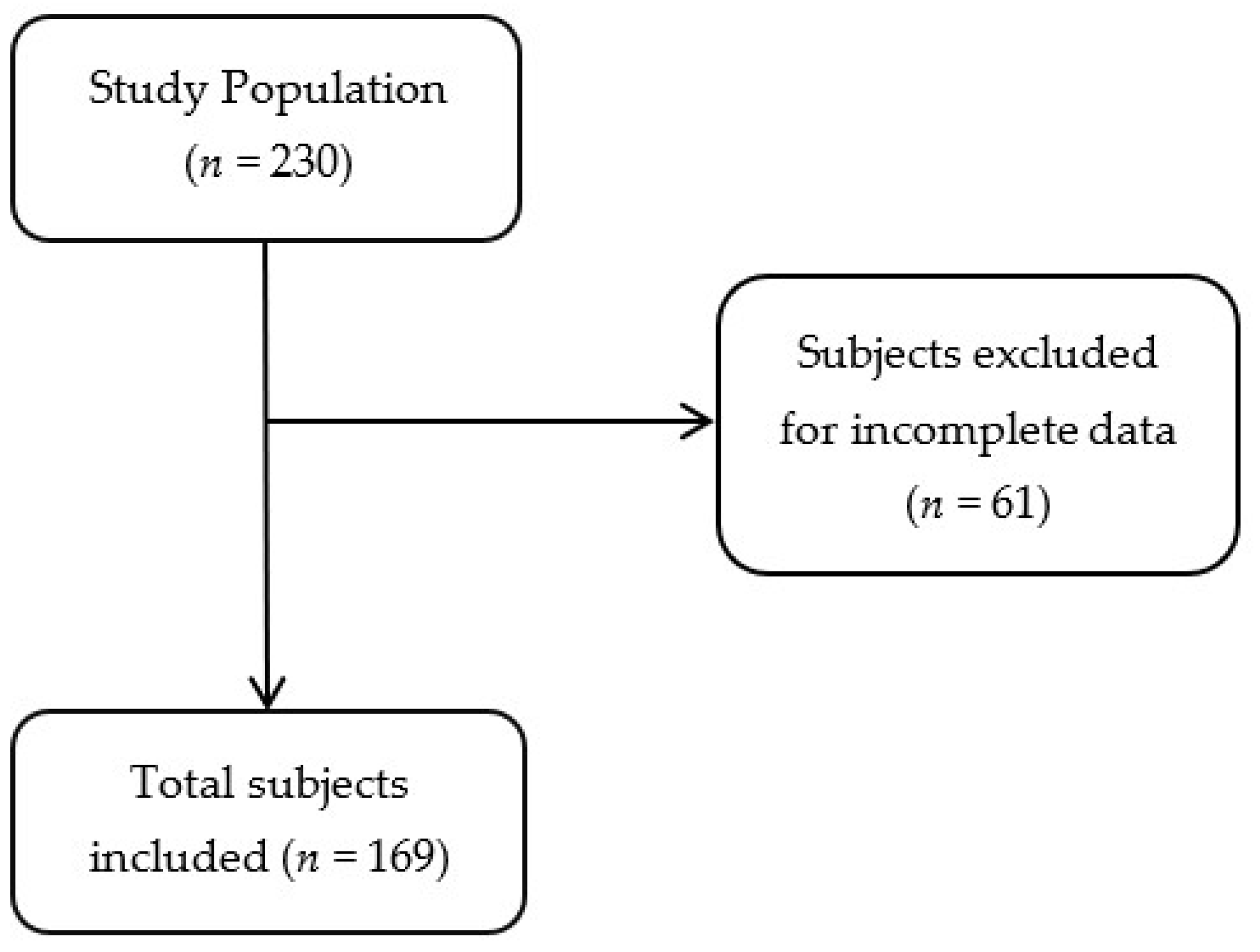
2.1. Study Population
2.2. Dietary Intake Assessment
2.3. Physical Activity
2.4. Biochemical Analysis
2.5. Anthropometric and Clinical Measurements
2.6. DNA Extraction and Genotyping
2.7. Statistical Analysis
2.8. Statement of Ethics
3. Results
3.1. Population Description
3.2. Characteristics of the Study Groups
FTO Genotype and Allelic Frequencies
3.3. Characteristics of Study Population According to FTO rs9939609 Variant
3.4. Risk Factors for Class III Obesity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Encuesta Nacional de Salud y Nutrición 2020 Sobre COVID-19 Resultados Nacionales. Available online: https://ensanut.insp.mx/encuestas/ensanutcontinua2020/doctos/informes/ensanutCovid19ResultadosNacionales.pdf (accessed on 13 March 2022).
- Disease of Obesity. Patients. ASMBS. American Society for Metabolic and Bariatric Surgery. Available online: https://asmbs.org/patients/disease-of-obesity (accessed on 21 March 2022).
- World Health Organization. Obesidad y Sobrepeso. 2021. Available online: https://www.who.int/es/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 5 July 2022).
- Centers for Disease Control and Prevention. H1N1 Flu in the News-Question & Answer: Obesity as a Risk Factor for Hospitalization and Death Due to 2009. Available online: https://www.cdc.gov/H1N1flu/in_the_news/obesity_qa.htm. (accessed on 8 March 2022).
- Secretaría de Salud. ¿Qué es la Obesidad Mórbida? 2015. Available online: http://www.gob.mx/salud/articulos/que-es-la-obesidad-a (accessed on 11 March 2022).
- Collins, J.; Meng, C.; Eng, A. Psychological Impact of Severe Obesity. Curr. Obes. Rep. 2016, 5, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Pietiläinen, K.H.; Naukkarinen, J.; Rissanen, A.; Saharinen, J.; Pekka, E.; Anu, S.; Götz, A.; Tapani, S.; Hannele, Y.J.; Matej, O. Global Transcript Profiles of Fat in Monozygotic Twins Discordant for BMI: Pathways behind Acquired Obesity. PLoS Med. 2008, 5, e51. [Google Scholar] [CrossRef] [PubMed]
- Loos, R.J. Genetic determinants of common obesity and their value in prediction. Best Pract. Res. Clin. Endocrinol. Metab. 2012, 26, 211–226. [Google Scholar] [CrossRef] [PubMed]
- Frayling, T.M.; Timpson, N.J.; Weedon, M.N.; Eleftheria, Z.; Rachel, M.; Cecilia, M.; John, R.; Katherine, S.; Hana, L.; Nigel, W. A Common Variant in the FTO Gene Is Associated with Body Mass Index and Predisposes to Childhood and Adult Obesity. Science 2007, 31, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Hofker, M.; Wijmenga, C. A supersized list of obesity genes. Nat. Genet. 2009, 41, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Kilpeläinen, T.O.; Liu, C.; Zhu, J.; Liu, Y.; Hu, C.; Yang, Z.; Zhang, W.; Bao, W.; Cha, S. Association of genetic variation in FTO with risk of obesity and type 2 diabetes with data from 96,551 East and South Asians. Diabetologia 2012, 55, 981–995. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Mou, S.; Pan, C. The FTO Gene rs9939609 Polymorphism Predicts Risk of Cardiovascular Disease: A Systematic Review and Meta-Analysis. PLoS ONE 2013, 8, e71901. [Google Scholar] [CrossRef] [PubMed]
- Jess, T.; Zimmermann, E.; Kring, S.; Berentzen, T.; Holst, C.; Toubro, S.; Astrup, A.; Hansen, T.; Pedersen, O.; Sørensen, T. Impact on weight dynamics and general growth of the common FTO rs9939609: A longitudinal Danish cohort study. Int. J. Obes. 2008, 32, 388–394. [Google Scholar] [CrossRef]
- Ri, U. The study of the rs9939609 FTO gene polymorphism in association with obesity and the management of obesity in a Romanian cohort. J. Med. Life 2015, 8, 7. [Google Scholar]
- Villalobos, C.M.; Flores, D.T.; Villarreal, M.; Rodríguez, M.C.; García, A.C.; Robles, L.; Huertas, A.V.; Saucedo, V.N.; Mardia, L.A.; Sánchez, F.M. The FTO gene is associated with adulthood obesity in the Mexican population. Obes. Silver. Spring Md. 2008, 16, 2296–2301. [Google Scholar] [CrossRef]
- USDA U.S. Department of Agriculture. Dietary Guidelines for Americans, 2020–2025. Available online: https://www.dietaryguidelines.gov/resources/2020-2025-dietary-guidelines-online-materials (accessed on 5 July 2022).
- Ministerio de Salud Pública. Manual Nacional de Abordaje del Tabaquismo en el Primer Nivel de Atención. 2009. Available online: https://www.paho.org/es/documentos/manual-nacional-abordaje-tabaquismo-primer-nivel-atencion (accessed on 18 July 2022).
- Campos, P.W.; Perez, R.M.; Torres, C.N.; Rodríguez, R.C.; De la Cerda, T.L.; Navarro, M.E.; Lopez, L.C.; Llamas, C.I.; Martinez, L.E. Physical inactivity and excessive sucrose consumption are associated with higher serum lipids in subjects with Taq1B CETP polymorphism. J. Hum. Nutr. Diet. 2020, 33, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Campos, P.W.; Perez, R.M.; Rodríguez, R.C.; Rivera, V.J.; Rodríguez, N.F.; Rivera, L.E.; Martinez, L.E. High dietary ω-6:ω-3 PUFA ratio and simple carbohydrates as a potential risk factors for gallstone disease: A cross-sectional study. Clin. Res. Hepatol. Gastroenterol. 2021, 46, 101802. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Recommendations on Physical Activity for Health. Available online: https://www.who.int/publications/i/item/9789241599979 (accessed on 18 July 2022).
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the Concentration of Low-Density Lipoprotein Cholesterol in Plasma, without Use of the Preparative Ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Powell, T.M.; Poirier, P.; Burke, L.E.; Jean, P.D.; Penny, G.L.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P. Obesity and Cardiovascular Disease: A Scientific Statement from the American Heart Association. Circulation 2021, 143, 984–1010. [Google Scholar] [CrossRef]
- Feingold, K.R. Obesity and Dyslipidemia. 2000. Available online: https://www.ncbi.nlm.nih.gov/books/NBK305895/ (accessed on 14 November 2022).
- Gonzalez, J.L.; Zabena, C.; Martinez, M.T.; Martinez, M.J.; Perez, M.B.; Serrano, R.M. Variant rs9939609 in the FTO gene is associated with obesity in an adult population from Spain. Clin. Endocrinol. 2009, 70, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Canada PHA of Obesity in Canada. Determinants and Contributing Factors. 2011. Available online: https://www.canada.ca/en/public-health/services/health-promotion/healthy-living/obesity-canada/factors.html (accessed on 13 July 2022).
- Campos, P.W.; Gonzalez, B.K.; Ramos, L.O.; Silva, G.J.; Barron, C.E.; Roman, S.; Panduro, A.; Martinez, L.E. Same Dietary but Different Physical Activity Pattern in Normal-weight and Overweight Mexican Subjects. J. Food Nutr. Res. 2016, 4, 729–735. [Google Scholar]
- World Health Organization. Physical Activity. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 12 July 2022).
- Mika, A.; Macaluso, F.; Barone, R.; Di Felice, V.; Sledzinski, T. Effect of Exercise on Fatty Acid Metabolism and Adipokine Secretion in Adipose Tissue. Front. Physiol. 2019, 10, 26. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.Y.; DeMenna, J.T.; Puppala, S.; Chittoor, G.; Schneider, J.; Duggirala, R.; Lawrence, J.; Mandarino, G.; Shaibi, D.; Coletta, K. Physical activity and FTO genotype by physical activity interactive influences on obesity. BMC Genet. 2016, 17, 47. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bell, C.G.; Walley, A.J.; Froguel, P. The genetics of human obesity. Nat. Rev. Genet. 2005, 6, 21–34. [Google Scholar] [CrossRef]
- Rankinen, T.; Zuberi, A.; Chagnon, Y.C.; Weisnagel, S.J.; Argyropoulos, G.; Walts, B.; Pérusse, L.; Bouchard, C. The human obesity gene map: The 2005 update. Obes. Silver Spring Md. 2006, 14, 529–644. [Google Scholar] [CrossRef]
- rs9939609 (SNP) Population Genetics-Homo_Sapiens—Ensembl Genome Browser. 2023. Available online: https://www.ensembl.org/Homo_sapiens/Variation/Population?db=core;r=16:53786115-53787115;v=rs9939609;vdb=variation;vf=730602335#373510_tablePanel (accessed on 15 July 2022).
- Siren, R.; Eriksson, J.G.; Vanhanen, H. Waist circumference a good indicator of future risk for type 2 diabetes and cardiovascular disease. BMC Public Health 2012, 12, 631. [Google Scholar] [CrossRef] [PubMed]
- Lappalainen, T.; Lindström, J.; Paananen, J.; Eriksson, G.J.; Karhunen, L.; Tuomilehto, J.; Uusitupa, M. Association of the fat mass and obesity-associated (FTO) gene variant (rs9939609) with dietary intake in the Finnish Diabetes Prevention Study. Br. J. Nutr. 2012, 108, 1859–1865. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Reuter, C.P.; Rosane, D.V.; Gaya, A.R.; Borges, T.S.; Klinger, E.I.; Gonçalves, L.P.; Possuelo, S.I.; Franke, R.; Kmetzsch, L.; Henning, M.V.; et al. FTO polymorphism, cardiorespiratory fitness, and obesity in Brazilian youth. Am. J. Hum. Biol. 2016, 28, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Andreasen, C.H.; Stender, K.L.; Mogensen, M.S.; Torekov, S.S.; Wegner, L.; Andersen, G.; Nielsen, A.L.; Albrechtsen, A.; Knut, B.J.; Rasmussen, S.S.; et al. Low Physical Activity Accentuates the Effect of the FTO rs9939609 Polymorphism on Body Fat Accumulation. Diabetes 2008, 57, 95–101. [Google Scholar] [CrossRef]
- Jacobsson Josefin, A.; Danielsson, P.; Svensson, V.; Klovins, J.; Gyllensten, U.; Claude, M.; Schioth Helgi, B.; Fredriksson, R. Major gender difference in association of FTO gene variant among severely obese children with obesity and obesity related phenotypes. Biochem. Biophys. Res. Commun. 2008, 368, 476–482. [Google Scholar] [CrossRef]


{kind=link}
| Variables | General Population (n = 169) | Class III Obesity (n = 55) | Normal Weight (n = 114) | p Value |
|---|---|---|---|---|
| Sociodemographic and anthropometrical | ||||
| Sex M/W (%) | 20.7/79.3 | 14.5/85.5 | 23.7/76.3 | 0.170 |
| Age (years) | 34 (27–43) | 38 (30–44) | 31.5 (24–43) | 0.014 |
| SBP (mm Hg) a | 115 (103–126) | 122.26 (117.6–126.8) | 112.18 (109.1–114.8) | <0.001 |
| DBP (mm Hg) a | 73 (65–80) | 80.10 (77–83.1) | 70.28 (68.4–72.1) | <0.001 |
| Weight (kg) a | 61 (55–68.5) | 117.78 (113.18–122.38) | 60.35 (58.81–61.89) | <0.001 |
| BMI (kg/m2) a | 23.85 (21.52–40.1) | 43.69 (42.57–44.81) | 22.32 (21.65–22.99) | <0.001 |
| Body Fat (%) a | ||||
| M (n = 35) | 21 (18–23.5) | 43.54 (36.71–50.38) | 19.27 (17.54–21) | <0.001 |
| W (n = 134) | 30 (24.25–33) | 48.96 (45.15–52.76) | 28 (26.71–29.29) | <0.001 |
| WC (cm) a | ||||
| M (n = 35) | 88 (82–101) | 140.33 (133.66–147) | 86.05 (83.21–88.88) | <0.001 |
| W (n = 134) | 79.5 (71.7–114.2) | 118.48 (115.49–121.47) | 75.12 (73.18–77.06) | <0.001 |
| Biochemical | ||||
| TC (mg/dL) a | 175 (155–205) | 177.9 (165.9–189.9) | 183.07(176–190.1) | 0.483 |
| LDL-c (mg/dL) a | 103.5 (88.2–129) | 113.11 (103.1–123) | 110.06 (104–116) | 0.618 |
| HDL-c (mg/dL) a | ||||
| M (n = 35) | 38 (34–45) | 34.18 (24.1–44.1) | 43.24 (38.9–47.5) | 0.104 |
| W (n = 134) | 44 (35–54) | 33.76 (29.8–37.6) | 50.51 (48–52.9) | <0.001 |
| TG (mg/dL) a | 116 (81.7–148.2) | 154.86 (131.2–178.5) | 121.41 (107.4–135.3) | 0.021 |
| TG/HDL-c ratio a | 2.7 (1.61–4.48) | 4.94 (4.2–5.6) | 2.77 (2.3–3.1) | <0.001 |
| TC/HDL-c ratio a | 4.15 (3.27–5.45) | 5.54 (5.1–5.9) | 3.94 (3.7–4.1) | <0.001 |
| Dietary intake | ||||
| Energy Intake (kcal) b | 2070.5 (1723.8–2576.3) | 2147.4 (1904.1–2390.6) | 2211.4 (2013.2–2409.5) | 0.688 |
| CH (%) b | 48.79 (41.39–52) | 46.38 (43.9–48.8) | 48.18 (46.1–50.1) | 0.267 |
| sCH (%) b | 11.1 (6.2–16) | 8.17 (5.4–10.8) | 11.68 (9.9–13.3) | 0.033 |
| Proteins (%) b | 15.77 (13.6–18.49) | 16.41 (15.1–17.6) | 16.45 (15.4–17.4) | 0.959 |
| TFAs (%) b | 36.79 (30–39.69) | 38.49 (36.1–40.8) | 34.89 (33–36.7) | 0.020 |
| SFAs (%) b | 10.51 (8.17–13) | 11.02 (10–11.9) | 10.65 (9.8–11.4) | 0.552 |
| MUFAs (%) b | 10.92 (8.36–13) | 11.32 (10–12.6) | 10.82 (9.78–11.8) | 0.562 |
| PUFAs (%) b | 6 (4–8) | 9.15 (7.8–10.4) | 5.21 (4.1–6.2) | <0.001 |
| n-6:n-3 ratio b | 10.69 (8.25–17.85) | 18.55 (15.9–21.1) | 11.28 (9.2–13.2) | <0.001 |
| Cholesterol (mg) b | 242.33 (153–328.3) | 290.88 (230.7–351) | 268.94 (222–315.7) | 0.572 |
| Fiber (g) b | 17.93 (13.1–26.4) | 17.25 (14.6–19.8) | 27.26 (23.9–30.5) | <0.001 |
| Genotype frequency | ||||
| TT, n (%) | 95 (56) | 26 (47) | 69 (60) | 0.025 |
| AT, n (%) | 42 (25) | 10 (18) | 32 (28) | |
| AA, n (%) | 32 (19) | 19 (35) c | 13 (12) c | |
| Allelic distribution | ||||
| A, n (%) | 52 (31) | 24 (44) | 28 (25) | <0.001 |
| T, n (%) | 117 (69) | 31 (56) | 86 (75) | |
| Qualitative variables | ||||
| Physical inactivity, n (%) | 95 (56) | 45 (82) | 50 (44) | <0.001 |
| Tobacco users, n (%) | 41 (24) | 15 (28) | 26 (23) | 0.105 |
| Alcohol drinkers, n (%) | 65 (38) | 12 (22) | 53 (47) | 0.002 |
| Variables | TT (n = 95) | AT (n = 42) | AA (n = 32) | p Value |
|---|---|---|---|---|
| Sex (M/W), % | 20/80 | 28.6/71.4 | 3.1/96.9 | 0.175 |
| Age (years) | 35.80 (33.48–38.12) | 35.11 (31.60–38.63) | 33.35 (28.48–38.22) | 0.616 |
| Clinical | ||||
| SBP (mm Hg) | 114.38 (111.5–117.2) | 114.19 (109.8–118.5) | 119.12 (112.8–125.4) | 0.376 |
| DBP (mm Hg) | 72.86 (69.7–75.9) | 72.86 (69.7–75.9) | 75.08 (70.5–79.6) | 0.487 |
| Anthropometrical | ||||
| Weight (kg) | 64.08 (59.4–68.7) | 68.3 (61.6–75) | 75.5 (64–86.9) | 0.151 |
| BMI (kg/m2) | 28.02 (25.9–30.1) | 26.91 (23.7–30) a | 35.46 (31–39.8) a | 0.005 |
| Body Fat (%) | ||||
| M (n = 35) | 19.59 (15.6–23.5) | 23.21 (18.6–27.7) | 24.12 | 0.610 |
| W (n = 134) | 29.87 (27.3–32.3) | 29.62 (25.8–33.4) | 32.98 (27.6–38.2) | 0.540 |
| WC (cm) | ||||
| M (n = 35) | 93.87 (83.4–104.2) | 94.91 (81.8–108) | 144.35 | 0.104 |
| W (n = 134) | 88.21 (82.9–93.5) | 85.45 (77–93.8) a | 101.07 (90.9–111.1) a | 0.047 |
| Biochemical | ||||
| TC (mg/dL) | 178.17 (171.1–185.1) | 184.08 (173.5–194.5) | 176.44 (161–191.3) | 0.596 |
| LDL-c(mg/dL) | 107.62 (101.7–113.4) | 112.49 (103.5–121.4) | 110.73 (98.4–123) | 0.647 |
| HDL-c(mg/dL) | ||||
| M (n = 35) | 40.03 (35.1–44.8) | 45.08 (38.9–51.1) | 30.39 | 0.246 |
| W (n = 134) | 45.51 (42.3–48.7) | 47.99 (42.9–53) | 41.97 (35.8–48) | 0.328 |
| TG (mg/dL) | 127.39 (113–141.7) | 122.09 (100.6–143.5) | 125.23 (94.6–155.7) | 0.920 |
| TG/HDL-c ratio | 3.28 (2.8–3.7) | 2.98 (2.2–3.7) | 3.63 (2.6–4.6) | 0.574 |
| TC/HDL-c ratio | 4.31 (4–4.5) | 4.12 (3.7–4.5) | 4.69 (4.09–5.3) | 0.318 |
| Variables | B | p Value | OR | 95% CI |
|---|---|---|---|---|
| FTO rs9939609:T>A variant | 1.265 | 0.002 | 3.544 | 1.347–9.322 |
| Physical inactivity | 1.853 | <0.001 | 6.377 | 2.55–5.914 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-López, E.; Perez-Robles, M.; Torres-Vanegas, J.; Godinez-Mora, S.; Llamas-Covarrubias, I.M.; Campos-Perez, W. FTO rs9939609: T>A Variant and Physical Inactivity as Important Risk Factors for Class III Obesity: A Cross-Sectional Study. Healthcare 2024, 12, 787. https://doi.org/10.3390/healthcare12070787
Martínez-López E, Perez-Robles M, Torres-Vanegas J, Godinez-Mora S, Llamas-Covarrubias IM, Campos-Perez W. FTO rs9939609: T>A Variant and Physical Inactivity as Important Risk Factors for Class III Obesity: A Cross-Sectional Study. Healthcare. 2024; 12(7):787. https://doi.org/10.3390/healthcare12070787
Chicago/Turabian StyleMartínez-López, Erika, Mariana Perez-Robles, Joel Torres-Vanegas, Sissi Godinez-Mora, Iris Monserrat Llamas-Covarrubias, and Wendy Campos-Perez. 2024. "FTO rs9939609: T>A Variant and Physical Inactivity as Important Risk Factors for Class III Obesity: A Cross-Sectional Study" Healthcare 12, no. 7: 787. https://doi.org/10.3390/healthcare12070787
APA StyleMartínez-López, E., Perez-Robles, M., Torres-Vanegas, J., Godinez-Mora, S., Llamas-Covarrubias, I. M., & Campos-Perez, W. (2024). FTO rs9939609: T>A Variant and Physical Inactivity as Important Risk Factors for Class III Obesity: A Cross-Sectional Study. Healthcare, 12(7), 787. https://doi.org/10.3390/healthcare12070787