
Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Knee Joint Infections: A Literature Review
 , , , ,
, , , , 
Abstract
:1. Introduction
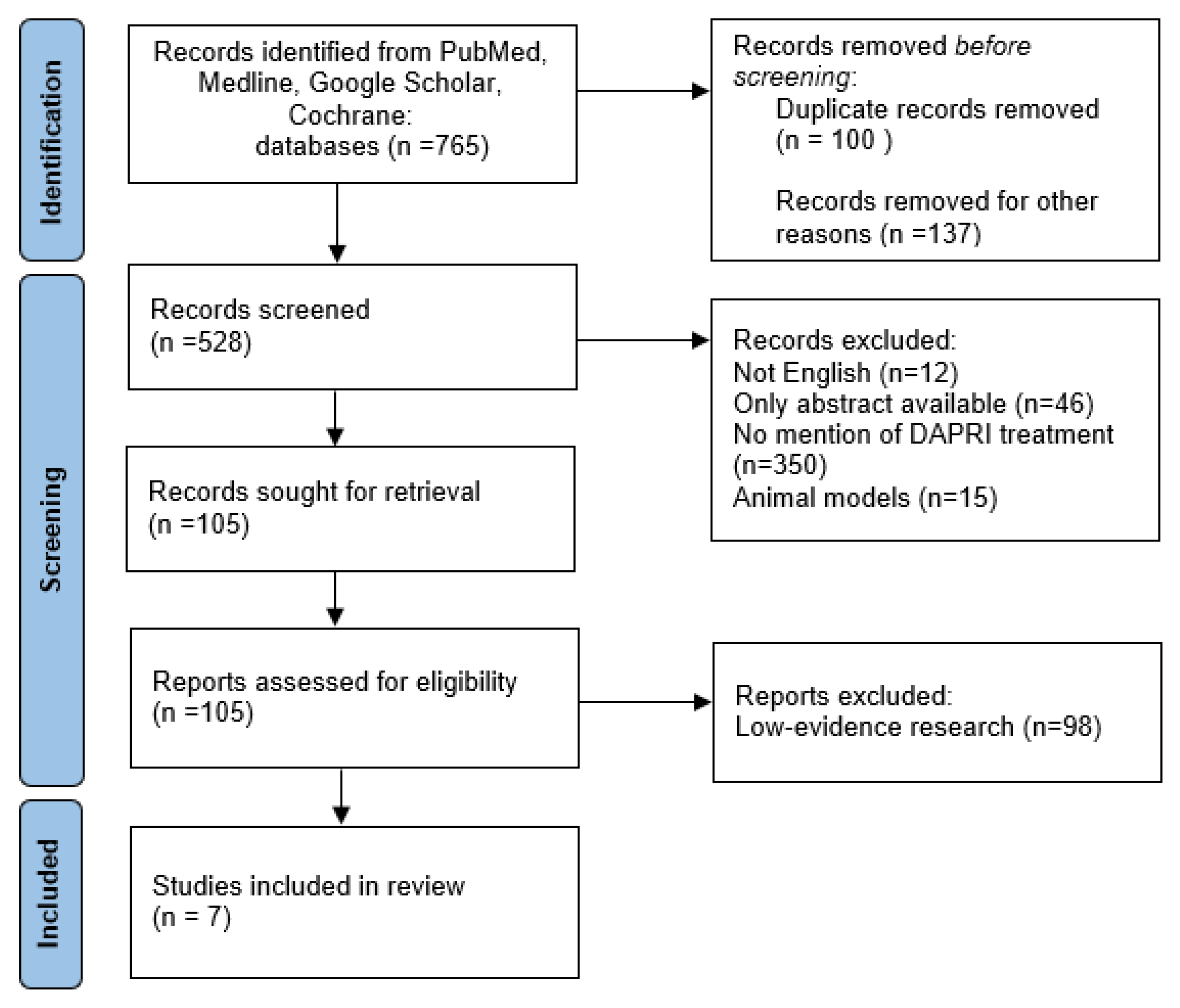
2. Materials and Methods
3. Results
3.1. Periprosthetic Joint Infections (PJIs)
3.2. PJI Definition
- Elevated serum C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) [20].
- Elevated synovial fluid white blood cell (WBC) count.
- Presence of a significant change on the leukocyte esterase test strip.
- Elevated synovial fluid polymorphonuclear neutrophil percentage (PMN%).
- Positive histological analysis of periprosthetic tissue.
- A single positive culture.
3.3. PJI Classification
- “Early Infections” are those infections that develop within the first 4 weeks postoperatively. Typically, they are associated with virulent organisms, such as Staphylococcus aureus and certain Gram-negative bacilli. These infections often cause an elevated erythrocyte sedimentation rate (ESR), joint pain, swelling, redness, warmth at the site of the implant, and fever [24]. These infections are characterized by immature biofilm formation [22].
- “Delayed Infections” are those infections occurring more than 4 weeks postoperatively. The timeframe for delayed infections extends beyond the immediate postoperative period, suggesting a more subacute or insidious onset. They are usually caused by less virulent species than early infections. Staphylococci or Cutibacterium acnes are some of the most common microorganisms responsible. People affected do not have clear symptoms, but they complain of persistent bone pain, swelling, and signs of systemic inflammation. Radiographies can show signs of implant loosening [7]. These infections are characterized by mature biofilm formation [22].
- ”Late Infections” are those infections occurring more than 24 months postoperatively [7]. They are characterized by a prolonged timeframe, indicating a delayed onset well after the initial surgical intervention. It has been shown that Staphylococci can cause late haematogenous PJIs, not only the early-onset ones [7]. Symptoms may resemble those of delayed infections, with a potential for chronicity and progressive joint deterioration. Late infections such as delayed ones may present with a more indolent course, necessitating a careful and thorough diagnostic approach to differentiate them from other potential causes of postoperative joint symptoms [7].
3.4. Indications and Contraindications: DAPRI and DAIR
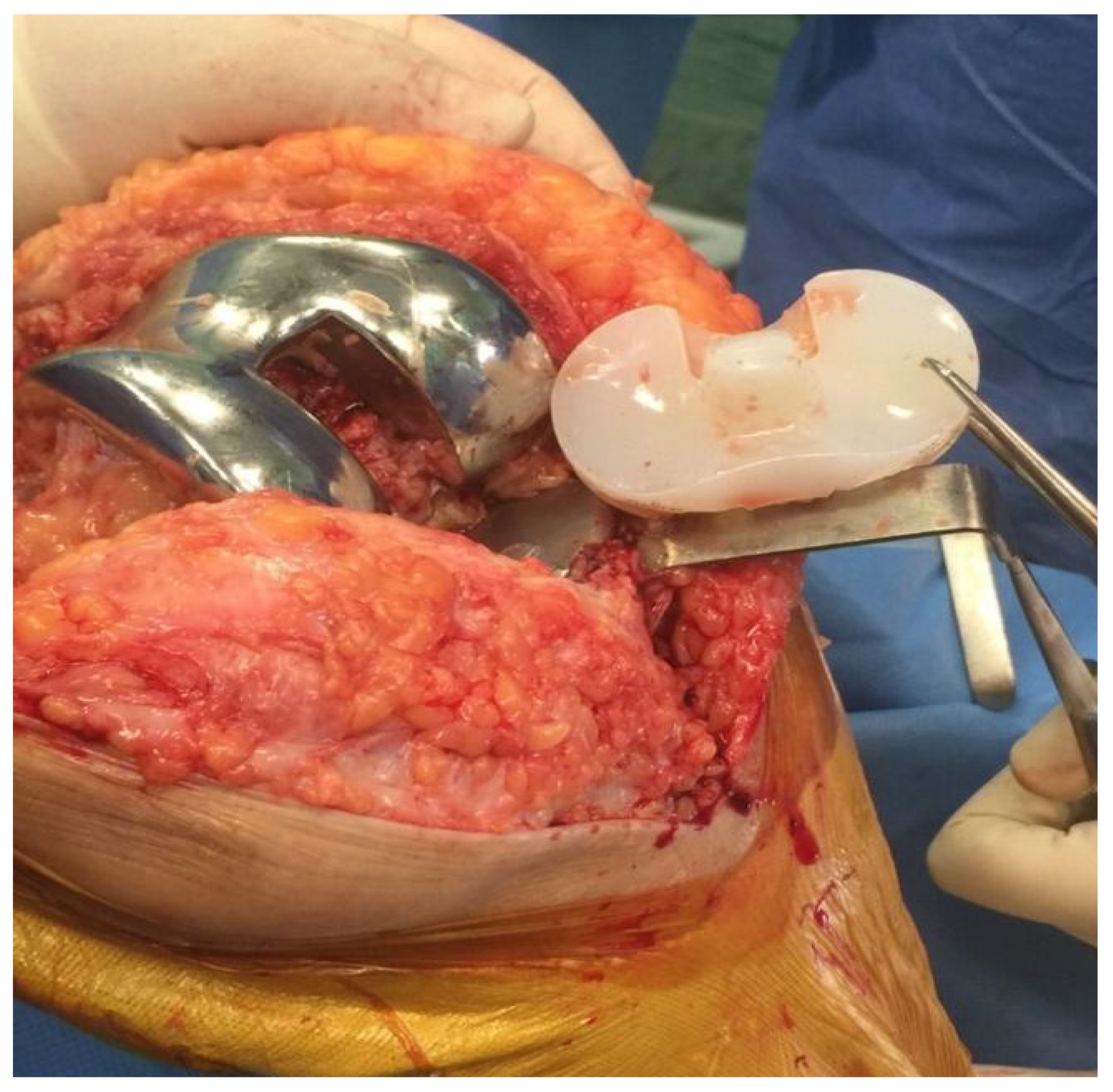
3.5. DAPRI Procedure
- Biofilm identification.
- Biofilm removal.
- Prevention of PJI recurrence.
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bizzoca, D.; Moretti, L.; Gnoni, A.; Moretti, F.L.; Scacco, S.; Banfi, G.; Piazzolla, A.; Solarino, G.; Moretti, B. The Usefulness of Synovial Fluid Proteome Analysis in Orthopaedics: Focus on Osteoarthritis and Periprosthetic Joint Infections. J. Funct. Morphol. Kinesiol. 2022, 7, 97. [Google Scholar] [CrossRef] [PubMed]
- Saracco, M.; Ciriello, V.; D’Angelo, F.; Zagra, L.; Solarino, G.; Logroscino, G. Do prior intra-articular injections impact on the risk of periprosthetic joint infection in patients undergoing total hip arthroplasty? A meta-analysis of the current evidences with a focus on the timing of injection before surgery. EFORT Open Rev. 2023, 8, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Solarino, G.; Abate, A.; Vicenti, G.; Spinarelli, A.; Piazzolla, A.; Moretti, B. Reducing periprosthetic joint infection: What really counts? Joints 2015, 3, 208–214. [Google Scholar] [CrossRef] [PubMed]
- Drago, L.; Clerici, P.; Morelli, I.; Ashok, J.; Benzakour, T.; Bozhkova, S.; Alizadeh, C.; Del Sel, H.; Sharma, H.K.; Peel, T.; et al. The world association against infection in orthopaedics and trauma (WAIOT) procedures for microbiological sampling and processing for periprosthetic joint infections (PJIs) and other implant-related infections. J. Clin. Med. 2019, 8, 933. [Google Scholar] [CrossRef] [PubMed]
- Boelch, S.P.; Jakuscheit, A.; Doerries, S.; Fraissler, L.; Hoberg, M.; Arnholdt, J.; Rudert, M. Periprosthetic infection is the major indication for TKA revision—Experiences from a university referral arthroplasty center. BMC Musculoskelet. Disord. 2018, 19, 395. [Google Scholar] [CrossRef]
- Reinisch, K.; Schläppi, M.; Meier, C.; Wahl, P. Local antibiotic treatment with calcium sulfate as carrier material improves the outcome of debridement, antibiotics, and implant retention procedures for periprosthetic joint infections after hip arthroplasty—A retrospective study. J. Bone Jt. Infect. 2022, 7, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Longo, U.G.; De Salvatore, S.; Bandini, B.; Lalli, A.; Barillà, B.; Budhiparama, N.C.; Lustig, S. Debridement, antibiotics, and implant retention (DAIR) for the early prosthetic joint infection of total knee and hip arthroplasties: A systematic review. J. ISAKOS 2024, 9, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.K.; Zeng, I.; Ravi, S.; Zhu, M.; Vince, K.G.; Young, S.W. Periprosthetic Joint Infection Is the Main Cause of Failure for Modern Knee Arthroplasty: An Analysis of 11,134 Knees. Clin. Orthop. Relat. Res. 2017, 475, 2194–2201. [Google Scholar] [CrossRef] [PubMed]
- Ghirardelli, S.; Fidanza, A.; Prati, P.; Iannotti, F.; Indelli, P.F. Debridement, antibiotic pearls, and retention of the implant in the treatment of infected total hip arthroplasty. HIP Int. 2020, 30, 34–41. [Google Scholar] [CrossRef]
- Indelli, P.F.; Ghirardelli, S.; Valpiana, P.; Bini, L.; Festini, M.; Iannotti, F. Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Joint Infections: A Consecutive Series. Pathogens 2023, 12, 605. [Google Scholar] [CrossRef]
- Patel, R. Periprosthetic Joint Infection. N. Engl. J. Med. 2023, 388, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Vasso, M.; Capasso, L.; Corona, K.; Pola, E.; Toro, G.; Panni, A.S. Periprosthetic knee infection: Treatment options. Orthop. Rev. 2022, 14, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Calanna, F.; Chen, F.; Risitano, S.; Vorhies, J.S.; Franceschini, M.; Giori, N.J.; Indelli, P.F. Debridement, antibiotic pearls, and retention of the implant (DAPRI): A modified technique for implant retention in total knee arthroplasty PJI treatment. J. Orthop. Surg. 2019, 27, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Abosala, A.; Ali, M. The Use of Calcium Sulphate beads in Periprosthetic Joint Infection, a systematic review. J. Bone Jt. Infect. 2020, 5, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Altman, D.; Antes, G.; Atkins, D.; Barbour, V.; Barrowman, N.; Berlin, J.A.; et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Tarar, M.Y.; Khalid, A.; Usman, M.; Javed, K.; Shah, N.; Abbas, M.W. Wound Leakage with the Use of Calcium Sulphate Beads in Prosthetic Joint Surgeries: A Systematic Review. Cureus 2021, 13, e19650. [Google Scholar] [CrossRef] [PubMed]
- Oussedik, S.; Gould, K.; Stockley, I.; Haddad, F.S. Defining peri-prosthetic infection. J. Bone Jt. Surg. Br. 2012, 94-B, 1455–1456. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.M.; Farley, K.X.; Guild, G.N.; Bradbury, T.L. Projections and Epidemiology of Revision Hip and Knee Arthroplasty in the United States to 2030. J. Arthroplast. 2020, 35, S79–S85. [Google Scholar] [CrossRef]
- Parvizi, J.; Gehrke, T.; Chen, A.F. Proceedings of the international consensus on periprosthetic joint infection. Bone Jt. J. 2013, 95 B, 1450–1452. [Google Scholar] [CrossRef]
- Vicenti, G.; Bizzoca, D.; Nappi, V.; Pesce, V.; Solarino, G.; Carrozzo, M.; Moretti, F.; Dicuonzo, F.; Moretti, B. Serum biomarkers in the diagnosis of periprosthetic joint infection: Consolidated evidence and recent developments. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 43–50. [Google Scholar] [CrossRef]
- Solarino, G.; Bizzoca, D.; Moretti, L.; Vicenti, G.; Piazzolla, A.; Moretti, B. What’s New in the Diagnosis of Periprosthetic Joint Infections: Focus on Synovial Fluid Biomarkers. Trop. Med. Infect. Dis. 2022, 7, 355. [Google Scholar] [CrossRef] [PubMed]
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Tsukayama, D.T.; Goldberg, V.M.; Kyle, R. Diagnosis and management of infection after total knee arthroplasty. J. Bone Jt. Surg. 2003, 85, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Lex, J.R.; Koucheki, R.; Stavropoulos, N.A.; Di Michele, J.; Toor, J.S.; Tsoi, K.; Ferguson, P.C.; Turcotte, R.E.; Papagelopoulos, P.J. Megaprosthesis anti-bacterial coatings: A comprehensive translational review. Acta Biomater. 2022, 140, 136–148. [Google Scholar] [CrossRef] [PubMed]
- Hulleman, C.W.J.; de Windt, T.S.; Veerman, K.; Goosen, J.H.M.; Wagenaar, F.C.B.M.; van Hellemondt, G.G. Debridement, Antibiotics and Implant Retention: A Systematic Review of Strategies for Treatment of Early Infections after Revision Total Knee Arthroplasty. J. Clin. Med. 2023, 12, 5026. [Google Scholar] [CrossRef] [PubMed]
- Nagra, N.S.; Hamilton, T.W.; Ganatra, S.; Murray, D.W.; Pandit, H. One-stage versus two-stage exchange arthroplasty for infected total knee arthroplasty: A systematic review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3106–3114. [Google Scholar] [CrossRef] [PubMed]
- Risitano, S.; Sabatini, L.; Atzori, F.; Massè, A.; Indelli, P.F. Static antibiotic spacers augmented by calcium sulphate impregnated beads in revision TKA: Surgical technique and review of literature. J. Orthop. 2018, 15, 313–318. [Google Scholar] [CrossRef]
- Osmon, D.R.; Berbari, E.F.; Berendt, A.R.; Lew, D.; Zimmerli, W.; Steckelberg, J.M.; Rao, N.; Hanssen, A.; Wilson, W.R. Diagnosis and management of prosthetic joint infection: Clinical practice guidelines by the infectious diseases Society of America. Clin. Infect. Dis. 2013, 56, e1–e25. [Google Scholar] [CrossRef] [PubMed]
- Fehring, T.K.; Odum, S.M.; Berend, K.R.; Jiranek, W.A.; Parvizi, J.; Bozic, K.J.; Della Valle, C.J.; Gioe, T.J. Failure of irrigation and débridement for early postoperative periprosthetic infection knee. Clin. Orthop. Relat. Res. 2013, 471, 250–257. [Google Scholar] [CrossRef]
- Urish, K.L.; Bullock, A.G.; Kreger, A.M.; Shah, N.B.; Jeong, K.; Rothenberger, S.D.; Irrgang, J.J.; Klatt, B.A.; Hamlin, B.R. A Multicenter Study of Irrigation and Debridement in Total Knee Arthroplasty Periprosthetic Joint Infection: Treatment Failure Is High. J. Arthroplast. 2018, 33, 1154–1159. [Google Scholar] [CrossRef]
- Kunutsor, S.K.; Beswick, A.D.; Whitehouse, M.R.; Wylde, V.; Blom, A.W. Debridement, antibiotics and implant retention for periprosthetic joint infections: A systematic review and meta-analysis of treatment outcomes. J. Infect. 2018, 77, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Byren, I.; Bejon, P.; Atkins, B.L.; Angus, B.; Masters, S.; McLardy-Smith, P.; Gundle, R.; Berendt, A. One hundred and twelve infected arthroplasties treated with “DAIR” (debridement, antibiotics and implant retention): Antibiotic duration and outcome. J. Antimicrob. Chemother. 2009, 63, 1264–1271. [Google Scholar] [CrossRef] [PubMed]
- Tsang, S.T.J.; Ting, J.; Simpson, A.H.R.W.; Gaston, P. Outcomes following debridement, antibiotics and implant retention in the management of periprosthetic infections of the hip: A review of cohort studies. Bone Jt. J. 2017, 99B, 1458–1466. [Google Scholar] [CrossRef]
- Tornero, E.; Martínez-Pastor, J.C.; Bori, G.; García-Ramiro, S.; Morata, L.; Bosch, J.; Mensa, J.; Soriano, A. Risk factors for failure in early prosthetic joint infection treated with debridement. Influence of etiology and antibiotic treatment. J. Appl. Biomater. Funct. Mater. 2014, 12, 129–134. [Google Scholar] [CrossRef]
- Argenson, J.N.; Arndt, M.; Babis, G.; Battenberg, A.; Budhiparama, N.; Catani, F.; Chen, F.; de Beaubien, B.; Ebied, A.; Esposito, S.; et al. Hip and Knee Section, Treatment, Debridement and Retention of Implant: Proceedings of International Consensus on Orthopedic Infections. J. Arthroplast. 2019, 34, S399–S419. [Google Scholar] [CrossRef]
- Azzam, K.A.; Seeley, M.; Ghanem, E.; Austin, M.S.; Purtill, J.J.; Parvizi, J. Irrigation and debridement in the management of prosthetic joint infection: Traditional indications revisited. J. Arthroplast. 2010, 25, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.S.; Sukeik, M.; Alazzawi, S. Is Single-stage Revision According to a Strict Protocol Effective in Treatment of Chronic Knee Arthroplasty Infections? Clin. Orthop. Relat. Res. 2015, 473, 8–14. [Google Scholar] [CrossRef]
- Achermann, Y.; Stasch, P.; Preiss, S.; Lucke, K.; Vogt, M. Characteristics and treatment outcomes of 69 cases with early prosthetic joint infections of the hip and knee. Infection 2014, 42, 511–519. [Google Scholar]
- Nucci, N.; Gazendam, A.; Gouveia, K.; Ghert, M.; Wilson, D. Management of infected extremity endoprostheses: A systematic review. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 1139–1149. [Google Scholar] [CrossRef]
- Choi, H.R.; Von Knoch, F.; Zurakowski, D.; Nelson, S.B.; Malchau, H. Can implant retention be recommended for treatment of infected TKA? Clin. Orthop. Relat. Res. 2011, 469, 961–969. [Google Scholar] [CrossRef]
- Parvin, F.; Vickery, K.; Deva, A.K.; Hu, H. Efficacy of Surgical/Wound Washes against Bacteria: Effect of Different In Vitro Models. Materials 2022, 15, 3630. [Google Scholar] [CrossRef] [PubMed]
- Siddiqi, A.; Abdo, Z.E.; Rossman, S.R.; Kelly, M.A.; Piuzzi, N.S.; Higuera, C.A.; Schwarzkopf, R.; Springer, B.D.; Chen, A.F.; Parvizi, J. What Is the Optimal Irrigation Solution in the Management of Periprosthetic Hip and Knee Joint Infections? J. Arthroplast. 2021, 36, 3570–3583. [Google Scholar] [CrossRef] [PubMed]
- Wouthuyzen-Bakker, M.; Löwik, C.A.M.; Knobben, B.A.S.; Zijlstra, W.P.; Ploegmakers, J.J.W.; Mithoe, G.; Al Moujahid, A.; Kampinga, G.A.; Jutte, P.C. Use of gentamicin-impregnated beads or sponges in the treatment of early acute periprosthetic joint infection: A propensity score analysis. J. Antimicrob. Chemother. 2018, 73, 3454–3459. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author Name | Title | Type of Article | Year |
|---|---|---|---|
| Reinisch et al. [6] | Local antibiotic treatment with calcium sulphate as carrier material improves the outcome of debridement, antibiotics, and implant retention procedures for periprosthetic joint infections after hip arthroplasty—A retrospective study | Retrospective study | 2022 |
| Ghirardelli et al. [9] | Debridement, antibiotic pearls, and retention of the implant in the treatment of infected total hip arthroplasty | Editorial | 2020 |
| Indelli et al. [10] | Debridement, Antibiotic Pearls, and Retention of the Implant | Article and Review | 2023 |
| (DAPRI) in the Treatment of Early Periprosthetic Joint | |||
| Infections: A Consecutive Series | |||
| Calanna et al. [13] | Debridement, antibiotic pearls, and retention of the implant (DAPRI): A modified technique for implant retention in total knee arthroplasty PJI treatment | Review | 2019 |
| Abosala et al. [14] | The Use of Calcium Sulphate beads in Periprosthetic | Systematic Review | 2020 |
| Joint Infection, a systematic review | |||
| Tarar et al. [16] | Wound Leakage with the Use of Calcium Sulphate Beads in Prosthetic Joint Surgeries: A Systematic Review | Systematic Review | 2021 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicenti, G.; Pesare, E.; Colasuonno, G.; Buono, C.; Albano, F.; Ladogana, T.; Passarelli, A.C.; Solarino, G. Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Knee Joint Infections: A Literature Review. Healthcare 2024, 12, 843. https://doi.org/10.3390/healthcare12080843
Vicenti G, Pesare E, Colasuonno G, Buono C, Albano F, Ladogana T, Passarelli AC, Solarino G. Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Knee Joint Infections: A Literature Review. Healthcare. 2024; 12(8):843. https://doi.org/10.3390/healthcare12080843
Chicago/Turabian StyleVicenti, Giovanni, Elisa Pesare, Giulia Colasuonno, Claudio Buono, Federica Albano, Teresa Ladogana, Anna Claudia Passarelli, and Giuseppe Solarino. 2024. "Debridement, Antibiotic Pearls, and Retention of the Implant (DAPRI) in the Treatment of Early Periprosthetic Knee Joint Infections: A Literature Review" Healthcare 12, no. 8: 843. https://doi.org/10.3390/healthcare12080843