
Stable Gastric Pentadecapeptide BPC 157 as Useful Cytoprotective Peptide Therapy in the Heart Disturbances, Myocardial Infarction, Heart Failure, Pulmonary Hypertension, Arrhythmias, and Thrombosis Presentation
 , , ,
, , ,  ,
,  , ,
, ,
Abstract
:1. Introduction
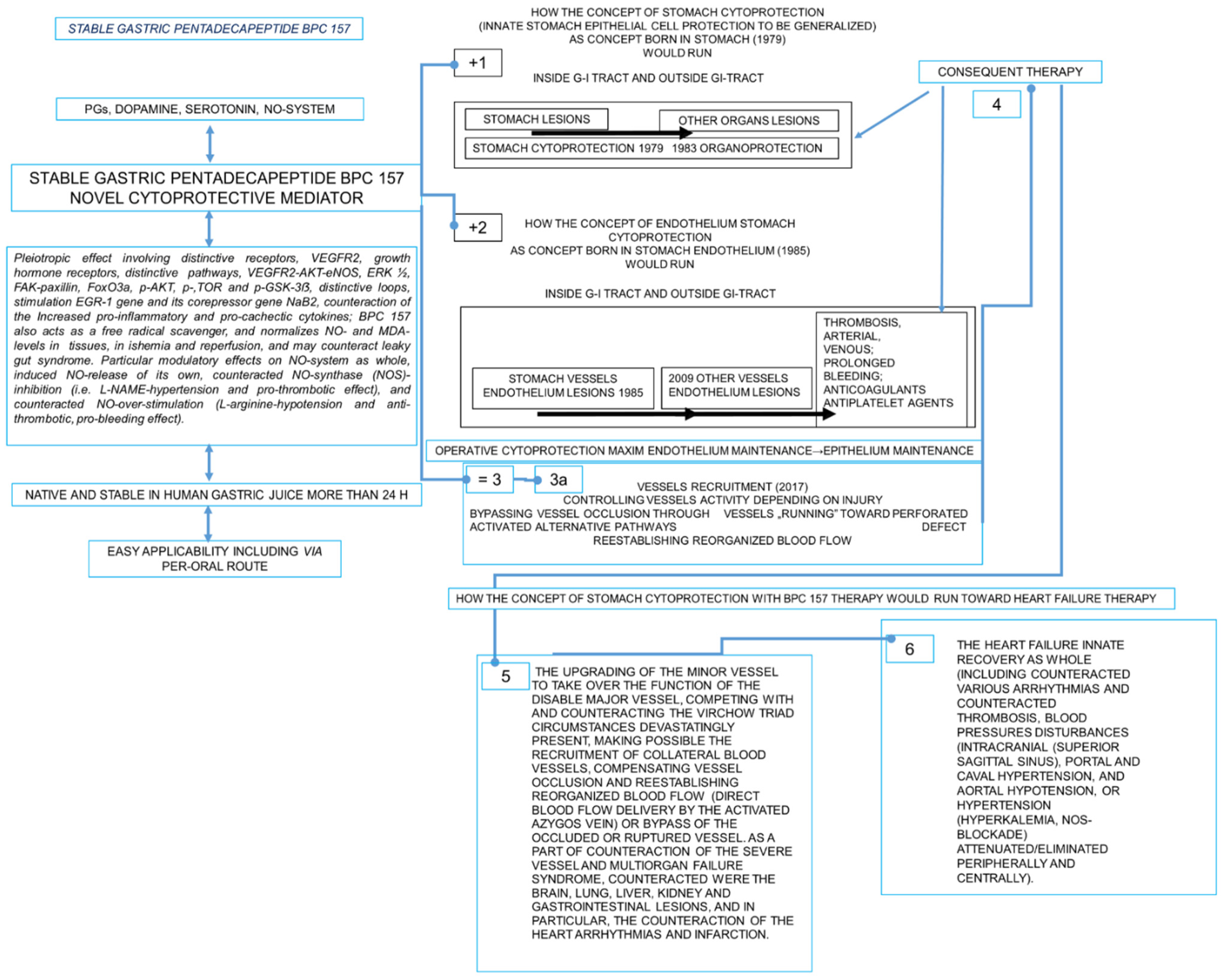
1.1. Cytoprotection Background (Direct Epithelial Cell Protection) for BPC 157 Beneficial Activity
1.2. Cytoprotection Background (Direct Endothelial Cell Protection) for BPC 157 Beneficial Activity
2. Myocardial Infarction
2.1. Isoprenaline Myocardial Infarction
2.2. Heart Failure
2.3. Heart Failure Concomitant Pathology
3. Thrombosis
4. Blood Pressure
Smooth Muscle
5. Arrhythmias
5.1. Digitalis
5.2. Hyperkalemia
5.3. Succinylcholine
5.4. Hypokalemia
5.5. Local Anesthetics, Bupivacaine
5.6. Local Anesthetics, Lidocaine
5.7. Neuroleptics and Prokinetics Induced Prolonged QTc Interval
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Savage, P.; Cox, B.; Linden, K.; Coburn, J.; Shahmohammadi, M.; Menown, I. Advances in clinical cardiology 2021: A summary of key clinical trials. Adv. Ther. 2022, 39, 2398–2437. [Google Scholar] [CrossRef] [PubMed]
- Vukojevic, J.; Milavic, M.; Perovic, D.; Ilic, S.; Zemba Cilic, A.; Duran, N.; Strbe, S.; Zoricic, Z.; Filipcic, I.; Brecic, P.; et al. Pentadecapeptide BPC 157 and the central nervous system. Neural. Regen. Res. 2022, 17, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Seiwerth, S.; Milavic, M.; Vukojevic, J.; Gojkovic, S.; Krezic, I.; Vuletic, L.B.; Pavlov, K.H.; Petrovic, A.; Sikiric, S.; Vranes, H.; et al. Stable gastric pentadecapeptide BPC 157 and wound healing. Front. Pharmacol. 2021, 12, 627533. [Google Scholar] [CrossRef]
- Sikiric, P.; Hahm, K.B.; Blagaic, A.B.; Tvrdeic, A.; Pavlov, K.H.; Petrovic, A.; Kokot, A.; Gojkovic, S.; Krezic, I.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157, Robert’s stomach cytoprotection/adaptive cytoprotection/organoprotection, and Selye’s stress coping response: Progress, achievements, and the future. Gut Liver 2020, 14, 153–167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.M.; Lee, H.J.; Sikiric, P.; Hahm, K.B. BPC 157 rescued NSAID-cytotoxicity via stabilizing intestinal permeability and enhancing cytoprotection. Curr. Pharm. Des. 2020, 26, 2971–2981. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.A.; Han, Y.M.; An, J.M.; Park, Y.J.; Sikiric, P.; Kim, D.H.; Kwon, K.A.; Kim, Y.J.; Yang, D.; Tchah, H.; et al. BPC157 as potential agent rescuing from cancer cachexia. Curr. Pharm. Des. 2018, 24, 1947–1956. [Google Scholar] [CrossRef]
- Sikiric, P.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. Novel cytoprotective mediator, stable gastric pentadecapeptide BPC 157. Vascular recruitment and gastrointestinal tract healing. Curr. Pharm. Des. 2018, 24, 1990–2001. [Google Scholar] [CrossRef]
- Sikiric, P.; Skrtic, A.; Gojkovic, S.; Krezic, I.; Zizek, H.; Lovric, E.; Sikiric, S.; Knezevic, M.; Strbe, S.; Milavic, M.; et al. Cytoprotective gastric pentadecapeptide BPC 157 resolves major vessel occlusion disturbances, ischemia-reperfusion injury following Pringle maneuver, and Budd-Chiari syndrome. World J. Gastroenterol. 2022, 28, 23–46. [Google Scholar] [CrossRef]
- Deek, S.A. BPC 157 as potential treatment for COVID-19. Med. Hypotheses 2021, 158, 110736. [Google Scholar] [CrossRef]
- Robert, A. Cytoprotection by prostaglandins. Gastroenterology 1979, 77, 761–767. [Google Scholar] [CrossRef]
- Szabo, S. Mechanism of mucosal protection. In Gastric Cytoprotection: A Clinician’s Guide; Hollander, D., Tarnawski, A., Eds.; Plenum Medical Book Co.: New York, NY, USA, 1989; pp. 49–90. [Google Scholar]
- Szabo, S.; Trier, J.S.; Brown, A.; Schnoor, J. Early vascular injury and increased vascular permeability in gastric mucosal injury caused by ethanol in the rat. Gastroenterology 1985, 88, 228–236. [Google Scholar] [CrossRef]
- Elliott, G.; Whited, B.A.; Purmalis, A.; Davis, J.P.; Field, S.O.; Lancaster, C.; Robert, A. Effect of 16,16-dimethyl PGE2 on renal papillary necrosis and gastrointestinal ulcerations (gastric, duodenal, intestinal) produced in rats by mefenamic acid. Life Sci. 1986, 39, 423–432. [Google Scholar] [CrossRef]
- Robert, A.; Lum, J.T.; Lancaster, C.; Olafsson, A.S.; Kolbasa, K.P.; Nezamis, J.E. Prevention by prostaglandins of caerulein-induced pancreatitis in rats. Lab. Investig. 1989, 60, 677–691. [Google Scholar]
- Szabo, S. Experimental basis for a role for sulfhydryls and dopamine in ulcerogenesis: A primer for cytoprotection--organoprotection. Klin Wochenschr. 1986, 64 (Suppl. S7), 116–122. [Google Scholar]
- Szabó, S. Role of sulfhydryls and early vascular lesions in gastric mucosal injury. Acta Physiol. Hung. 1984, 64, 203–214. [Google Scholar]
- Szabo, S.; Usadel, K.H. Cytoprotection—Organoprotection by somatostatin: Gastric and hepatic lesions. Experientia 1982, 38, 254–256. [Google Scholar] [CrossRef]
- Hrelec, M.; Klicek, R.; Brcic, L.; Brcic, I.; Cvjetko, I.; Seiwerth, S.; Sikiric, P. Abdominal aorta anastomosis in rats and stable gastric pentadecapeptide BPC 157, prophylaxis and therapy. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 161–165. [Google Scholar]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Vranes, H.; Knezevic, T.; Barisic, I.; Horvat Pavlov, K.; et al. Occlusion of the superior mesenteric artery in rats reversed by collateral pathways activation: Gastric pentadecapeptide BPC 157 therapy counteracts multiple organ dysfunction syndrome; intracranial, portal and caval hypertension; and aortal hypotension. Biomedicines 2021, 9, 609. [Google Scholar] [CrossRef]
- Vukojevic, J.; Vrdoljak, B.; Malekinusic, D.; Siroglavic, M.; Milavic, M.; Kolenc, D.; Boban Blagaic, A.; Bateljam, L.; Drmic, D.; Seiwerth, S.; et al. The effect of pentadecapeptide BPC 157 on hippocampal ischemia/reperfusion injuries in rats. Brain Behav. 2020, 10, e01726. [Google Scholar] [CrossRef]
- Zlatar, M.; Kokot, A.; Vuletic, L.B.; Masnec, S.; Kralj, T.; Perisa, M.M.; Barisic, I.; Radic, B.; Milanovic, K.; Drmic, D.; et al. BPC 157 as a therapy for retinal ischemia induced by retrobulbar application of L-NAME in rats. Front. Pharmacol. 2021, 12, 632295. [Google Scholar] [CrossRef]
- Vukojevic, J.; Siroglavic, M.; Kasnik, K.; Kralj, T.; Stancic, D.; Kokot, A.; Kolaric, D.; Drmic, D.; Sever, A.Z.; Barisic, I.; et al. Rat inferior caval vein (ICV) ligature and particular new insights with the stable gastric pentadecapeptide BPC 157. Vascul. Pharmacol. 2018, 106, 54–66. [Google Scholar] [CrossRef] [PubMed]
- Gojkovic, S.; Krezic, I.; Vrdoljak, B.; Malekinusic, D.; Barisic, I.; Petrovic, A.; Horvat Pavlov, K.; Kolovrat, M.; Duzel, A.; Knezevic, M.; et al. Pentadecapeptide BPC 157 resolves suprahepatic occlusion of the inferior caval vein, Budd-Chiari syndrome model in rats. World J. Gastrointest. Pathophysiol. 2020, 11, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Pavlov, K.H.; Drmic, D.; et al. Complex syndrome of the complete occlusion of the end of the superior mesenteric vein, opposed with the stable gastric pentadecapeptide BPC 157 in rats. Biomedicines 2021, 9, 1029. [Google Scholar] [CrossRef] [PubMed]
- Amic, F.; Drmic, D.; Bilic, Z.; Krezic, I.; Zizek, H.; Peklic, M.; Klicek, R.; Pajtak, A.; Amic, E.; Vidovic, T.; et al. Bypassing major venous occlusion and duodenal lesions in rats, and therapy with the stable gastric pentadecapeptide BPC 157, L-NAME and L-arginine. World J. Gastroenterol. 2018, 24, 5366–5378. [Google Scholar] [CrossRef] [PubMed]
- Kralj, T.; Kokot, A.; Zlatar, M.; Masnec, S.; Kasnik Kovac, K.; Milkovic Perisa, M.; Batelja Vuletic, L.; Giljanovic, A.; Strbe, S.; Sikiric, S.; et al. Stable gastric pentadecapeptide BPC 157 therapy of rat glaucoma. Biomedicines 2021, 10, 89. [Google Scholar] [CrossRef]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Pavlov, K.H.; Petrovic, A.; Batelja, L.; Milavic, M.; Sikiric, S.; et al. BPC 157 therapy and the permanent occlusion of the superior sagittal sinus in rat. Vascular recruitment. Biomedicines 2021, 9, 744. [Google Scholar] [CrossRef]
- Kolovrat, M.; Gojkovic, S.; Krezic, I.; Malekinusic, D.; Vrdoljak, B.; Kasnik Kovac, K.; Kralj, T.; Drmic, D.; Barisic, I.; Horvat Pavlov, K.; et al. Pentadecapeptide BPC 157 resolves Pringle maneuver in rats, both ischemia and reperfusion. World J. Hepatol. 2020, 12, 184–206. [Google Scholar] [CrossRef]
- Knezevic, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Malekinusic, D.; Vrdoljak, B.; Knezevic, T.; Vranes, H.; Drmic, D.; Staroveski, M.; et al. Occluded superior mesenteric artery and vein. Therapy with the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 792. [Google Scholar] [CrossRef]
- Duzel, A.; Vlainic, J.; Antunovic, M.; Malekinusic, D.; Vrdoljak, B.; Samara, M.; Gojkovic, S.; Krezic, I.; Vidovic, T.; Bilic, Z.; et al. Stable gastric pentadecapeptide BPC 157 in the treatment of colitis and ischemia and reperfusion in rats: New insights. World J. Gastroenterol. 2017, 23, 8465–8488. [Google Scholar] [CrossRef]
- Tepes, M.; Gojkovic, S.; Krezic, I.; Zizek, H.; Madzar, Z.; Santak, G.; Batelja, L.; Milavic, M.; Sikiric, S.; Kocman, I.; et al. Stable gastric pentadecapeptide BPC 157 therapy for primary abdominal compartment syndrome in rats. Front. Pharmacol. 2021, 12, 718147. [Google Scholar] [CrossRef]
- Drmic, D.; Samara, M.; Vidovic, T.; Malekinusic, D.; Antunovic, M.; Vrdoljak, B.; Ruzman, J.; Milkovic, P.M.; Horvat, K.P.; Jeyakumar, J.; et al. Counteraction of perforated cecum lesions in rats: Effects of pentadecapeptide BPC 157, L-NAME and L-arginine. World J. Gastroenterol. 2018, 24, 5462–5476. [Google Scholar] [CrossRef] [PubMed]
- Bilic, Z.; Gojkovic, S.; Kalogjera, L.; Krezic, I.; Malekinusic, D.; Knezevic, M.; Sever, M.; Lojo, N.; Kokot, A.; Kasnik, K.; et al. Novel insight into Robert’s cytoprotection: Complex therapeutic effect of cytoprotective pentadecapeptide pentadecapeptide BPC 157 in rats with perforated stomach throughout modulation of nitric oxide-system. Comparison with L-arginine, ranitidine and pantoprazole therapy and L-NG-nitro-L-arginine methyl ester worsening. J. Physiol. Pharmacol. 2021, 72. [Google Scholar] [CrossRef]
- Cesar, L.B.; Gojkovic, S.; Krezic, I.; Malekinusic, D.; Zizek, H.; Vuletic, L.B.; Petrovic, A.; Pavlov, K.H.; Drmic, D.; Kokot, A.; et al. Bowel adhesion and therapy with the stable gastric pentadecapeptide BPC 157, L-NAME and L-arginine in rats. World J. Gastrointest. Pharmacol. Ther. 2020, 11, 93–109. [Google Scholar] [CrossRef] [PubMed]
- Perovic, D.; Kolenc, D.; Bilic, V.; Somun, N.; Drmic, D.; Elabjer, E.; Buljat, G.; Seiwerth, S.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 can improve the healing course of spinal cord injury and lead to functional recovery in rats. J. Orthop. Surg. Res. 2019, 14, 199. [Google Scholar] [CrossRef] [PubMed]
- Perovic, D.; Milavic, M.; Dokuzovic, S.; Krezic, I.; Gojkovic, S.; Vranes, H.; Bebek, I.; Bilic, V.; Somun, N.; Brizic, I.; et al. Novel therapeutic effects in rat spinal cord injuries: Recovery of the definitive and early spinal cord injury by the administration of pentadecapeptide BPC 157 therapy. Curr. Issues Mol. Biol. 2022, 44, 1901–1927. [Google Scholar] [CrossRef]
- Smoday, I.M.; Petrovic, I.; Kalogjera, L.; Vranes, H.; Zizek, H.; Krezic, I.; Gojkovic, S.; Skorak, I.; Hriberski, K.; Brizic, I.; et al. Therapy effect of the stable gastric pentadecapeptide BPC 157 on acute pancreatitis as vascular failure-induced severe peripheral and central syndrome in rats. Biomedicines 2022, 10, 1299. [Google Scholar] [CrossRef]
- Barisic, I.; Balenovic, D.; Udovicic, M.; Bardak, D.; Strinic, D.; Vlainic, J.; Vranes, H.; Smoday, I.M.; Krezic, I.; Milavic, M.; et al. Stable gastric pentadecapeptide BPC 157 may counteract myocardial infarction induced by isoprenaline in rats. Biomedicines 2022, 10, 265. [Google Scholar] [CrossRef]
- Strbe, S.; Gojkovic, S.; Krezic, I.; Zizek, H.; Vranes, H.; Barisic, I.; Strinic, D.; Orct, T.; Vukojevic, J.; Ilic, S.; et al. Over-dose lithium toxicity as an occlusive-like syndrome in rats and gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1506. [Google Scholar] [CrossRef]
- Gojkovic, S.; Krezic, I.; Vranes, H.; Zizek, H.; Drmic, D.; Batelja Vuletic, L.; Milavic, M.; Sikiric, S.; Stilinovic, I.; Simeon, P.; et al. Robert’s intragastric alcohol-induced gastric lesion model as an escalated general peripheral and central syndrome, counteracted by the stable gastric pentadecapeptide BPC 157. Biomedicines 2021, 9, 1300. [Google Scholar] [CrossRef]
- Udovicic, M.; Sever, M.; Kavur, L.; Loncaric, K.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Batelja Vuletic, L.; et al. Stable gastric pentadecapeptide BPC 157 therapy for monocrotaline-induced pulmonary hypertension in rats leads to prevention and reversal. Biomedicines 2021, 9, 822. [Google Scholar] [CrossRef]
- Faillie, J.L. Pharmacological aspects of the safety of gliflozins. Pharmacol. Res. 2017, 118, 71–81. [Google Scholar] [CrossRef]
- Choi, C.I. Sodium-glucose cotransporter 2 (SGLT2) inhibitors from natural products: Discovery of next-generation antihyperglycemic agents. Molecules 2016, 21, 1136. [Google Scholar] [CrossRef] [Green Version]
- Merovci, A.; Solis-Herrera, C.; Daniele, G.; Eldor, R.; Fiorentino, T.V.; Tripathy, D.; Xiong, J.; Perez, Z.; Norton, L.; Abdul-Ghani, M.A.; et al. Dapagliflozin improves muscle insulin sensitivity but enhances endogenous glucose production. J. Clin. Investig. 2014, 124, 509–514. [Google Scholar] [CrossRef]
- Jandeleit-Dahm, K.; Cooper, M.E. Hypertension and diabetes: Role of the renin–angiotensin system. Endocrinol. Metab. Clin. North Am. 2006, 35, 469–490. [Google Scholar] [CrossRef]
- Wang, W.; McKinnie, S.M.; Farhan, M.; Paul, M.; McDonald, T.; McLean, B.; Llorens-Cortes, C.; Hazra, S.; Murray, A.G.; Vederas, J.C.; et al. Angiotensin converting enzyme 2 metabolizes and partially inactivates pyrapelin-13 and apelin-17: Physiological effects in the cardiovascular system. Hypertension 2016, 68, 365–377. [Google Scholar] [CrossRef] [Green Version]
- Fogari, R.; Zoppi, A.; Corradi, L.; Lazzari, P.; Mugellini, A.; Lusardi, P. Comparative effect of lisonopril and losartan on insulin sensitivity in the treatment of non diabetic hypertensive patients. Br. J. Clin. Pharmacol. 1998, 46, 467–471. [Google Scholar] [CrossRef] [Green Version]
- Freemantle, N.; Cleland, J.; Young, P.; Mason, J.; Harrison, J. Beta blockade after myocardial infarction: Systematic review and meta regression analysis. BMJ 1999, 318, 1730–1737. [Google Scholar] [CrossRef] [Green Version]
- Ivanova, A.D.; Kuzmin, V.S. Electrophysiological characteristics of the rat azygos vein under electrical pacing and adrenergic stimulation. J. Physiol. Sci. 2018, 68, 617–628. [Google Scholar] [CrossRef]
- Chang, C.H.; Tsai, W.C.; Lin, M.S.; Hsu, Y.H.; Pang, J.H.S. The promoting effect of pentadecapeptide BPC 157 on tendon healing involves tendon outgrowth, cell survival, and cell migration. J. Appl. Physiol. 2011, 110, 774–780. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.H.; Tsai, W.C.; Hsu, Y.H.; Pang, J.H.S. Pentadecapeptide BPC 157 enhances the growth hormone receptor expression in tendon fibroblasts. Molecules 2014, 19, 19066–19077. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.; Zhang, K.; Sun, L.; Xue, X.; Zhang, C.; Shu, Z.; Mu, N.; Gu, J.; Zhang, W.; Wang, Y.; et al. Body protective compound-157 enhances alkali-burn wound healing in vivo and promotes proliferation, migration, and angiogenesis in vitro. Drug Des. Devel. Ther. 2015, 9, 2485–2499. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, M.J.; Lee, C.H.; Chueh, H.Y.; Chang, G.J.; Huang, H.Y.; Lin, Y.; Pang, J.S. Modulatory effects of BPC 157 on vasomotor tone and the activation of Src-Caveolin-1-endothelial nitric oxide synthase pathway. Sci. Rep. 2020, 10, 17078. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, M.J.; Liu, H.T.; Wang, C.N.; Huang, H.Y.; Lin, Y.; Ko, Y.S.; Wang, J.S.; Chang, V.H.; Pang, J.S. Therapeutic potential of pro-angiogenic BPC157 is associated with VEGFR2 activation and up-regulation. J. Mol. Med. 2017, 95, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Tkalcevic, V.I.; Cuzic, S.; Brajsa, K.; Mildner, B.; Bokulic, A.; Situm, K.; Perovic, D.; Glojnaric, I.; Parnham, M.J. Enhancement by PL 14736 of granulation and collagen organization in healing wounds and the potential role of egr-1 expression. Eur. J. Pharmacol. 2007, 570, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Qu, M.; Duan, R.; Shi, D.; Jin, L.; Gao, J.; Wood, J.D.; Li, J.; Wang, G.D. Cytoprotective mechanism of the novel gastric peptide BPC157 in gastrointestinal tract and cultured enteric neurons and glial cells. Neurosci. Bull. 2019, 35, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Wei, M.; Li, N.; Lu, Q.; Shrestha, S.M.; Tan, J.; Zhang, Z.; Wu, G.; Shi, R. Clopidogrel-induced gastric injury in rats is attenuated by stable gastric pentadecapeptide BPC 157. Drug Des. Devel. Ther. 2020, 14, 5599–5610. [Google Scholar] [CrossRef]
- Stupnisek, M.; Kokot, A.; Drmic, D.; Hrelec Patrlj, M.; Zenko Sever, A.; Kolenc, D.; Radic, B.; Suran, J.; Bojic, D.; Vcev, A.; et al. Pentadecapeptide BPC 157 reduces bleeding and thrombocytopenia after amputation in rats treated with heparin, warfarin, L-NAME and L-arginine. PLoS ONE 2015, 10, e0123454. [Google Scholar] [CrossRef]
- Stupnisek, M.; Franjic, S.; Drmic, D.; Hrelec, M.; Kolenc, D.; Radic, B.; Bojic, D.; Vcev, A.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 reduces bleeding time and thrombocytopenia after amputation in rats treated with heparin, warfarin or aspirin. Thromb. Res. 2012, 129, 652–659. [Google Scholar] [CrossRef]
- Konosic, S.; Petricevic, M.; Ivancan, V.; Konosic, L.; Goluza, E.; Krtalic, B.; Drmic, D.; Stupnisek, M.; Seiwerth, S.; Sikiric, P. Intragastric application of aspirin, clopidogrel, cilostazol, and BPC 157 in rats: Platelet aggregation and blood clot. Oxid. Med. Cell. Longev. 2019, 2019, 9084643. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Stable gastric pentadecapeptide BPC 157-NO-system relation. Curr. Pharm. Des. 2014, 20, 1126–1135. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Grabarevic, Z.; Rucman, R.; Petek, M.; Jagic, V.; Turkovic, B.; Rotkvic, I.; Mise, S.; Zoricic, I.; et al. The influence of a novel pentadecapeptide, BPC 157, on N(G)-nitro-L-arginine methylester and L-arginine effects on stomach mucosa integrity and blood pressure. Eur. J. Pharmacol. 1997, 332, 23–33. [Google Scholar] [CrossRef]
- Turkovic, B.; Sikiric, P.; Seiwerth, S.; Mise, S.; Anic, T.; Petek, M. Stable gastric pentadecapeptide BPC 157 studied for inflammatory bowel disease (PLD-116, PL14736, Pliva) induces nitric oxide synthesis. Gastroenterology 2004, 126, 287. [Google Scholar]
- Demiryűrek, A.T.; Demiryűrek, S. Cardiotoxicity of digitalis glycosides: Roles of autonomic pathways, autacoids and ion channels. Auton. Autacoid. Pharmacol. 2005, 25, 35–52. [Google Scholar] [CrossRef]
- Pabla, R.; Curtis, M.J. Effects of NO modulation on cardiac arrhythmias in the rat isolated heart. Circ. Res. 1995, 77, 984–992. [Google Scholar] [CrossRef]
- Balenovic, D.; Bencic, M.L.; Udovicic, M.; Simonji, K.; Hanzevacki, J.S.; Barisic, I.; Kranjcevic, S.; Prkacin, I.; Coric, V.; Brcic, L.; et al. Inhibition of methyldigoxin-induced arrhythmias by pentadecapeptide BPC 157: A relation with NO-system. Regul. Pept. 2009, 156, 83–89. [Google Scholar] [CrossRef]
- Barisic, I.; Balenovic, D.; Klicek, R.; Radic, B.; Nikitovic, B.; Drmic, D.; Udovicic, M.; Strinic, D.; Bardak, D.; Berkopic, L.; et al. Mortal hyperkalemia disturbances in rats are NO-system related. The life saving effect of pentadecapeptide BPC 157. Regul Pept. 2013, 181, 50–66. [Google Scholar] [CrossRef]
- Stambolija, V.; Stambolija, T.P.; Holjevac, J.K.; Murselovic, T.; Radonic, J.; Duzel, V.; Duplancic, B.; Uzun, S.; Zivanovic-Posilovic, G.; Kolenc, D.; et al. BPC 157: The counteraction of succinylcholine, hyperkalemia, and arrhythmias. Eur. J. Pharmacol. 2016, 781, 83–91. [Google Scholar] [CrossRef]
- Balenovic, D.; Barisic, I.; Prkacin, I.; Horvat, I.; Udovicic, M.; Uzun, S.; Strinic, D.; Pevec, D.; Drmic, D.; Radic, B.; et al. Mortal furosemide-hypokalemia-disturbances in rats NO-system related shorten survival by L-NAME. Therapy benefit with BPC 157 peptide more than with L-arginine. J. Clin. Exp. Cardiolog. 2012, 3, 7. [Google Scholar] [CrossRef] [Green Version]
- Zivanovic-Posilovic, G.; Balenovic, D.; Barisic, I.; Strinic, D.; Stambolija, V.; Udovicic, M.; Uzun, S.; Drmic, D.; Vlainic, J.; Bencic, M.L.; et al. Stable gastric pentadecapeptide BPC 157 and bupivacaine. Eur. J. Pharmacol. 2016, 793, 56–65. [Google Scholar] [CrossRef]
- Lozic, M.; Stambolija, V.; Krezic, I.; Dugandzic, A.; Zivanovic-Posilovic, G.; Gojkovic, S.; Kovacevic, J.; Vrdoljak, L.; Mirkovic, I.; Kokot, A.; et al. In relation to NO-system, stable pentadecapeptide BPC 157 counteracts lidocaine-Induced adverse effects in rats and depolarisation in vitro. Emerg. Med. Int. 2020, 2020, 6805354. [Google Scholar] [CrossRef]
- Strinic, D.; Belosic Halle, Z.; Luetic, K.; Nedic, A.; Petrovic, I.; Sucic, M.; Zivanovic Posilovic, G.; Balenovic, D.; Strbe, S.; Udovicic, M.; et al. BPC 157 counteracts QTc prolongation induced by haloperidol, fluphenazine, clozapine, olanzapine, quetiapine, sulpiride, and metoclopramide in rats. Life Sci. 2017, 186, 66–79. [Google Scholar] [CrossRef] [PubMed]
- Bosnjak, Z.J.; Graf, B.M.; Sikiric, P.; Stowe, D.F. Protective effects of newly isolated gastric peptide following hypoxic and reoxygenation injury in the isolated guinea pig heart. FASEB J. 1994, 8, A12. [Google Scholar]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Turkovic, B.; Rokotov, D.S.; Brcic, L.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; et al. Toxicity by NSAIDs: Counteraction by stable gastric pentadecapeptide BPC 157. Curr. Pharm. Des. 2013, 19, 76–83. [Google Scholar] [PubMed]
- Bleumink, G.S.; Feenstra, J.; Sturkenboom, M.C.J.M.; Stricker, B.H.C. Nonsteroidal anti-inflammatory drugs and heart failure. Drugs 2003, 63, 525–534. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Sabzwari, S.R.A.; Vargova, V. Cardiovascular risk of nonsteroidal anti-inflammatory drugs: An under-recognized public health issue. Cureus 2017, 9, e1144. [Google Scholar] [CrossRef] [Green Version]
- Loosen, S.H.; Roderburg, C.; Curth, O.; Gaensbacher, J.; Joerdens, M.; Luedde, T.; Konrad, M.; Kostev, K.; Luedde, M. The spectrum of comorbidities at the initial diagnosis of heart failure a case control study. Sci. Rep. 2022, 12, 2670. [Google Scholar] [CrossRef]
- Lawson, C.A.; Testani, J.M.; Mamas, M.; Damman, K.; Jones, P.W.; Teece, L.; Kadam, U.T. Chronic kidney disease, worsening renal function and outcomes in a heart failure community setting: A UK national study. Int. J. Cardiol. 2018, 267, 120–127. [Google Scholar] [CrossRef] [Green Version]
- Lawson, C.A.; Solis-Trapala, I.; Dahlstrom, U.; Mamas, M.; Jaarsma, T.; Kadam, U.T.; Stromberg, A. Comorbidity health pathways in heart failure patients: A sequences-of-regressions analysis using cross-sectional data from 10,575 patients in the Swedish Heart Failure Registry. PLoS Med. 2018, 15, e1002540. [Google Scholar] [CrossRef]
- Hubich, A.I.; Bondar, A.Y.; Kastsiuk, T.U.; Kastsiuk, U.A.; Lakhvich, F.A.; Sholukh, M.V. Hepatoprotective action of prostaglandin A(2) analogs under CCl(4)-induced liver injury in vitro. Hepatol. Res. 2007, 37, 416–424. [Google Scholar] [CrossRef]
- Vincenti, F.; Goldberg, L.I. Combined use of dopamine and prostaglandin A1 in patients with acute renal failure and hepatorenal syndrome. Prostaglandins. 1978, 15, 463–472. [Google Scholar] [CrossRef]
- Takakuma, A.; Nishii, M.; Valaperti, A.; Hiraga, H.; Saji, R.; Sakai, K.; Matsumura, R.; Miyata, Y.; Oba, N.; Nunose, F.; et al. Prostaglandin-E2 receptor-4 stimulant rescues cardiac malfunction during myocarditis and protects the heart from adverse ventricular remodeling after myocarditis. Sci. Rep. 2021, 11, 20961. [Google Scholar] [CrossRef]
- Tudor, M.; Jandric, I.; Marovic, A.; Gjurasin, M.; Perovic, D.; Radic, B.; Blagaic, A.B.; Kolenc, D.; Brcic, L.; Zarkovic, K.; et al. Traumatic brain injury in mice and pentadecapeptide BPC 157 effect. Regul Pept. 2010, 160, 26–32. [Google Scholar] [CrossRef]
- Lovric-Bencic, M.; Sikiric, P.; Hanzevacki, J.S.; Seiwerth, S.; Rogic, D.; Kusec, V.; Aralica, G.; Konjevoda, P.; Batelja, L.; Blagaic, A.B. Doxorubicine-congestive heart failure-increased big endothelin-1 plasma concentration: Reversal by amlodipine, losartan, and gastric pentadecapeptide BPC157 in rat and mouse. J. Pharmacol. Sci. 2004, 95, 19–26. [Google Scholar] [CrossRef] [Green Version]
- Stancic-Rokotov, D.; Slobodnjak, Z.; Aralica, J.; Aralica, G.; Perovic, D.; Staresinic, M.; Gjurasin, M.; Anic, T.; Zoricic, I.; Buljat, G.; et al. Lung lesions and anti-ulcer agents beneficial effect: Anti-ulcer agents pentadecapeptide BPC 157, ranitidine, omeprazole and atropine ameliorate lung lesion in rats. J. Physiol. Paris 2001, 95, 303–308. [Google Scholar] [CrossRef]
- Grabarevic, Z.; Tisljar, M.; Artukovic, B.; Bratulic, M.; Dzaja, P.; Seiwerth, S.; Sikiric, P.; Peric, J.; Geres, D.; Kos, J. The influence of BPC 157 on nitric oxide agonist and antagonist induced lesions in broiler chicken. J. Physiol. Paris 1997, 91, 139–149. [Google Scholar] [CrossRef]
- Stancic-Rokotov, D.; Sikiric, P.; Seiwerth, S.; Slobodnjak, Z.; Aralica, J.; Aralica, G.; Perovic, D.; Anic, T.; Zoricic, I.; Buljat, G.; et al. Ethanol gastric lesion aggravated by lung injury in rat. Therapy effect of antiulcer agents. J. Physiol. Paris 2001, 95, 289–293. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Grabarevic, Z.; Rucman, R.; Petek, M.; Rotkvic, I.; Turkovic, B.; Jagic, V.; Mildner, B.; Duvnjak, M.; et al. Hepatoprotective effect of BPC 157, a 15-amino acid peptide, on liver lesions induced by either restraint stress or bile duct and hepatic artery ligation or CCl4 administration. A comparative study with dopamine agonists and somatostatin. Life Sci. 1993, 53, PL291–PL296. [Google Scholar] [CrossRef]
- Prkacin, I.; Separovic, J.; Aralica, G.; Perovic, D.; Gjurasin, M.; Lovric-Bencic, M.; Stancic-Rokotov, D.; Staresinic, M.; Anic, T.; Mikus, D.; et al. Portal hypertension and liver lesions in chronically alcohol drinking rats prevented and reversed by stable gastric pentadecapeptide BPC 157 (PL-10, PLD-116), and propranolol, but not ranitidine. J. Physiol. Paris 2001, 95, 315–324. [Google Scholar] [CrossRef]
- Sever, A.Z.; Sever, M.; Vidovic, T.; Lojo, N.; Kolenc, D.; Vuletic, L.B.; Drmic, D.; Kokot, A.; Zoricic, I.; Coric, M.; et al. Stable gastric pentadecapeptide BPC 157 in the therapy of the rats with bile duct ligation. Eur. J. Pharmacol. 2019, 847, 130–142. [Google Scholar] [CrossRef]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. High hepatotoxic dose of paracetamol produces generalized convulsions and brain damage in rats. A counteraction with the stable gastric pentadecapeptide BPC 157 (PL 14736). J. Physiol. Pharmacol. 2010, 61, 241–250. [Google Scholar]
- Drmic, D.; Kolenc, D.; Ilic, S.; Bauk, L.; Sever, M.; Zenko Sever, A.; Luetic, K.; Suran, J.; Seiwerth, S.; Sikiric, P. Celecoxib-induced gastrointestinal, liver and brain lesions in rats, counteraction by BPC 157 or L-arginine, aggravation by L-NAME. World J. Gastroenterol. 2017, 23, 5304–5312. [Google Scholar] [CrossRef] [PubMed]
- Lojo, N.; Rasic, Z.; Sever, A.Z.; Kolenc, D.; Vukusic, D.; Drmic, D.; Zoricic, I.; Sever, M.; Seiwerth, S.; Sikiric, P. Effects of diclofenac, L-NAME, L-arginine, and pentadecapeptide BPC157 on gastrointestinal, liver, and brain lesions, failed anastomosis, and intestinal adaptation deterioration in 24 h-short-bowel rats. PLoS ONE 2016, 11, e0162590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilic, S.; Drmic, D.; Zarkovic, K.; Kolenc, D.; Brcic, L.; Radic, B.; Djuzel, V.; Blagaic, A.B.; Romic, Z.; Dzidic, S.; et al. Ibuprofen hepatic encephalopathy, hepatomegaly, gastric lesion and gastric pentadecapeptide BPC 157 in rats. Eur. J. Pharmacol. 2011, 667, 322–329. [Google Scholar] [CrossRef] [PubMed]
- Ilic, S.; Drmic, D.; Franjic, S.; Kolenc, D.; Coric, M.; Brcic, L.; Klicek, R.; Radic, B.; Sever, M.; Djuzel, V.; et al. Pentadecapeptide BPC 157 and its effects on a NSAID toxicity model: Diclofenac-induced gastrointestinal, liver, and encephalopathy lesions. Life Sci. 2011, 88, 535–542. [Google Scholar] [CrossRef]
- Ilic, S.; Brcic, I.; Mester, M.; Filipovicm, M.; Sever, M.; Klicek, R.; Barisic, I.; Radic, B.; Zoricic, Z.; Bilic, V.; et al. Over-dose insulin and stable gastric pentadecapeptide BPC 157: Attenuated gastric ulcers, seizures, brain lesions, hepatomegaly, fatty liver, breakdown of liver glycogen, profound hypoglycemia and calcification in rats. J. Physiol. Pharmacol. 2009, 60, 107–114. [Google Scholar] [PubMed]
- Vranes, H.; Krezic, I.; Gojkovic, S.; Zizek, H.; Durasin, T.; Petrovic, A.; Horvat Pavlov, K.; Batelja, L.; Blagaic Boban, A.; Seiwerth, S.; et al. In hydornephrosis-rats, BPC 157 exerts a strong anti-ulcer effect in both stomach and duodenum along with marked kidney recovery. FASEB J. 2020, 34 (Suppl. S1), 1. [Google Scholar] [CrossRef]
- Drmic, D.; Sucic, M.; Zenko Sever, A.; Kolenc, D.; Suran, J.; Seiwerth, S.; Sikiric, P. BPC 157 counteracts gastric lesions after bilateral nephrectomy and attenuates deleterious course in rats. FASEB J. 2015, 29 (Suppl. S1), 628.10. [Google Scholar] [CrossRef]
- Drmic, D.; Sucic, M.; Zenko Sever, A.; Kolenc, D.; Andrijasevic, V.; Suran, J.; Seiwerth, S.; Sikiric, P. Attenuation of the deleterious couse and gastric lesions after bilateral nephrectomy in rats, NO-system relation. BPC 157, L-arginine, L-NAME. FASEB J. 2016, 30 (Suppl. S1), 720.2. [Google Scholar]
- Sikirić, P.; Seiwerth, S.; Grabarević, Z.; Rucman, R.; Petek, M.; Jagić, V.; Turković, B.; Rotkvić, I.; Mise, S.; Zoricić, I.; et al. Salutary and prophylactic effect of pentadecapeptide BPC 157 on acute pancreatitis and concomitant gastroduodenal lesions in rats. Dig. Dis. Sci. 1996, 41, 1518–1526. [Google Scholar] [CrossRef]
- Petrovic, I.; Dobric, I.; Drmic, D.; Sever, M.; Klicek, R.; Radic, B.; Brcic, L.; Kolenc, D.; Zlatar, M.; Kunjko, K.; et al. BPC 157 therapy to detriment sphincters failure-esophagitis-pancreatitis in rat and acute pancreatitis patients low sphincters pressure. J. Physiol. Pharmacol. 2011, 62, 527–534. [Google Scholar]
- Seiwerth, S.; Rucman, R.; Turkovic, B.; Sever, M.; Klicek, R.; Radic, B.; Drmic, D.; Stupnisek, M.; Misic, M.; Vuletic, L.B.; et al. BPC 157 and standard angiogenic growth factors. Gastrointestinal tract healing, lessons from tendon, ligament, muscle and bone healing. Curr. Pharm. Des. 2018, 24, 1972–1989. [Google Scholar] [CrossRef]
- Bilic, M.; Bumber, Z.; Blagaic, A.B.; Batelja, L.; Seiwerth, S.; Sikiric, P. The stable gastric pentadecapeptide BPC 157, given locally, improves CO2 laser healing in mice. Burns 2005, 31, 310–315. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Mise, S.; Staresinic, M.; Bedekovic, V.; Zarkovic, N.; Borovic, S.; Gjurasin, M.; Boban-Blagaic, A.; Batelja, L.; et al. Corticosteroid-impairment of healing and gastric pentadecapeptide BPC-157 creams in burned mice. Burns 2003, 29, 323–334. [Google Scholar] [CrossRef]
- Mikus, D.; Sikiric, P.; Seiwerth, S.; Petricevic, A.; Aralica, G.; Druzijancic, N.; Rucman, R.; Petek, M.; Pigac, B.; Perovic, D.; et al. Pentadecapeptide BPC 157 cream improves burn-wound healing and attenuates burn-gastric lesions in mice. Burns 2001, 27, 817–827. [Google Scholar] [CrossRef]
- Gjurasin, M.; Miklic, P.; Zupancic, B.; Perovic, D.; Zarkovic, K.; Brcic, L.; Kolenc, D.; Radic, B.; Seiwerth, S.; Sikiric, P. Peptide therapy with pentadecapeptide BPC 157 in traumatic nerve injury. Regul. Pept. 2010, 160, 33–41. [Google Scholar] [CrossRef]
- Staresinic, M.; Sebecic, B.; Patrlj, L.; Jadrijevic, S.; Suknaic, S.; Perovic, D.; Aralica, G.; Zarkovic, N.; Borovic, S.; Srdjak, M.; et al. Gastric pentadecapeptide BPC 157 accelerates healing of transected rat Achilles tendon and in vitro stimulates tendocytes growth. J. Orthop. Res. 2003, 21, 976–983. [Google Scholar] [CrossRef]
- Krivic, A.; Anic, T.; Seiwerth, S.; Huljev, D.; Sikiric, P. Achilles detachment in rat and stable gastric pentadecapeptide BPC 157: Promoted tendon-to-bone healing and opposed corticosteroid aggravation. J. Orthop. Res. 2006, 24, 982–989. [Google Scholar] [CrossRef]
- Krivic, A.; Majerovic, M.; Jelic, I.; Seiwerth, S.; Sikiric, P. Modulation of early functional recovery of Achilles tendon to bone unit after transection by BPC 157 and methylprednisolone. Inflamm. Res. 2008, 57, 205–210. [Google Scholar] [CrossRef]
- Brcic, L.; Brcic, I.; Staresinic, M.; Novinscak, T.; Sikiric, P.; Seiwerth, S. Modulatory effect of gastric pentadecapeptide BPC 157 on angiogenesis in muscle and tendon healing. J. Physiol. Pharmacol. 2009, 60, 191–196. [Google Scholar]
- Japjec, M.; Horvat Pavlov, K.; Petrovic, A.; Staresinic, M.; Sebecic, B.; Buljan, M.; Vranes, H.; Giljanovic, A.; Drmic, D.; Japjec, M.; et al. Stable Gastric Pentadecapeptide BPC 157 as a therapy for the disable myotendinous junctions in rats. Biomedicines 2021, 9, 1547. [Google Scholar] [CrossRef]
- Staresinic, M.; Petrovic, I.; Novinscak, T.; Jukic, I.; Pevec, D.; Suknaic, S.; Kokic, N.; Batelja, L.; Brcic, L.; Boban-Blagaic, A.; et al. Effective therapy of transected quadriceps muscle in rat: Gastric pentadecapeptide BPC 157. J. Orthop. Res. 2006, 24, 1109–1117. [Google Scholar] [CrossRef]
- Novinscak, T.; Brcic, L.; Staresinic, M.; Jukic, I.; Radic, B.; Pevec, D.; Mise, S.; Tomasovic, S.; Brcic, I.; Banic, T.; et al. Gastric pentadecapeptide BPC 157 as an effective therapy for muscle crush injury in the rat. Surg. Today 2008, 38, 716–725. [Google Scholar] [CrossRef] [PubMed]
- Pevec, D.; Novinscak, T.; Brcic, L.; Sipos, K.; Jukic, I.; Staresinic, M.; Mise, S.; Brcic, I.; Kolenc, D.; Klicek, R.; et al. Impact of pentadecapeptide BPC 157 on muscle healing impaired by systemic corticosteroid application. Med. Sci. Monit. 2010, 16, 81–88. [Google Scholar]
- Mihovil, I.; Radic, B.; Brcic, L.; Brcic, I.; Vukoja, I.; Ilic, S.; Boban Blagaic, A.; Seiwerth, S.; Sikiric, P. Beneficial effect of pentadecapeptide BPC 157 on denervated muscle in rats. J. Physiol. Pharmacol. 2009, 60, 69. [Google Scholar]
- Cerovecki, T.; Bojanic, I.; Brcic, L.; Radic, B.; Vukoja, I.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 (PL 14736) improves ligament healing in the rat. J. Orthop. Res. 2010, 28, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Sebecic, B.; Nikolic, V.; Sikiric, P.; Seiwerth, S.; Sosa, T.; Patrlj, L.; Grabarević, Z.; Rucman, R.; Petek, M.; Konjevoda, P.; et al. Osteogenic effect of a gastric pentadecapeptide BPC 157, on the healing of segmental bone defect in rabbits. A comparison with bone marrow and autologous cortical bone implantation. Bone 1999, 24, 195–202. [Google Scholar] [CrossRef]
- Keremi, B.; Lohinai, Z.; Komora, P.; Duhaj, S.; Borsi, K.; Jobbagy-Ovari, G.; Kallo, K.; Szekely, A.D.; Fazekas, A.; Dobo-Nagy, C.; et al. Antiinflammatory effect of BPC 157 on experimental periodontitis in rats. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 115–122. [Google Scholar]
- Gamulin, O.; Serec, K.; Bilic, V.; Balarin, M.; Kosovic, M.; Drmic, D.; Brcic, L.; Seiwerth, S.; Sikiric, P. Monitoring the healing process of rat bones using Raman spectroscopy. J. Mol. Struct. 2013, 1044, 303–313. [Google Scholar] [CrossRef]
- Sikiric, P.; Drmic, D.; Sever, M.; Klicek, R.; Blagaic, A.B.; Tvrdeic, A.; Kralj, T.; Kovac, K.K.; Vukojevic, J.; Siroglavic, M.; et al. Fistulas healing. Stable gastric pentadecapeptide BPC 157 therapy. Curr. Pharm. Des. 2020, 26, 2991–3000. [Google Scholar] [CrossRef]
- Szekeres, L. Pharmacological induction of delayed and prolonged cardiac protection: The role of prostanoids. Exp. Clin. Cardiol. 2004, 9, 7–12. [Google Scholar]
- Szekeres, L. Cardioprotection by anti-ischaemic and cytoprotective drugs. Basic Res. Cardiol. 1987, 82 (Suppl. S2), 325–333. [Google Scholar]
- Szekeres, L.; Pataricza, J.; Szilvássy, Z.; Udvary, E.; Végh, A. Cardioprotection: Endogenous protective mechanisms promoted by prostacyclin. Basic Res. Cardiol. 1991, 86 (Suppl. S3), 215–221. [Google Scholar]
- Masnec, S.; Kokot, A.; Zlatar, M.; Kalauz, M.; Kunjko, K.; Radic, B.; Klicek, R.; Drmic, D.; Lazic, R.; Brcic, L.; et al. Perforating corneal injury in rat and pentadecapeptide BPC 157. Exp. Eye Res. 2015, 136, 9–15. [Google Scholar] [CrossRef]
- Wong, Z.W.; Thanikachalam, P.V.; Rohrer, U.; Ramamurthy, S. Molecular understanding of the protective role of natural products on isoproterenol-induced myocardial infarction: A review. Biomed. Pharmacother. 2017, 94, 1145–1166. [Google Scholar] [CrossRef]
- Kolesnik, E.; Scherr, D.; Rohrer, U.; Benedikt, M.; Manninger, M.; Sourij, H.; von Lewinski, D. SGLT2 inhibitors and their antiarrhythmic properties. Int. J. Mol. Sci. 2022, 23, 1678. [Google Scholar] [CrossRef]
- Smith, D.F. Lithium and motor activity of animals: Effects and possible mechanism of action. Int. Pharm. 1980, 15, 197–217. [Google Scholar] [CrossRef]
- Matussek, N.; Linsmayer, M. The effect of lithium and amphetamine on desmethylimipramine-Ro 4-1284 induced motor hyperactivity. Life Sci. 1968, 7, 371–375. [Google Scholar] [CrossRef]
- Berggren, U.; Tallstedt, L.; Ahlenius, S.; Engel, J. The effect of lithium on amphetamine-induced locomotor stimulation. Psychopharmacology 1978, 59, 41–45. [Google Scholar] [CrossRef]
- Petersen, K.P. Effect of age and route of administration on LD50 of lithium chloride in the rat. Acta Pharmacol. Toxicol. 1980, 47, 351–354. [Google Scholar] [CrossRef]
- Guidance for Industry, Estimating the Maximum Safe Starting Dose in Initial Clinical Trials for Therapeutics in Adult Healthy Volunteers, Pharmacology and Toxicology, U.S. Department of Health and Human Services Food and Drug Administration Center for Drug Evaluation and Research (CDER), July 2005. Available online: http://www.fda.gov/cder/guidance/index.htm (accessed on 29 August 2022).
- Temple, I.P.; Monfredi, O.; Quigley, G.; Schneider, H.; Zi, M.; Cartwright, E.J.; Boyett, M.R.; Mahadevan, V.S.; Hart, G. Macitentan treatment retards the progression of established pulmonary arterial hypertension in an animal model. Int. J. Cardiol. 2014, 177, 423–428. [Google Scholar] [CrossRef]
- Mouchaers, K.T.; Schalij, I.; de Boer, M.A.; Postmus, P.E.; van Hinsbergh, V.W.; van Nieuw Amerongen, G.P.; Vonk Noordegraaf, A.; van der Laarse, W.J. Fasudil reduces monocrotaline-induced pulmonary arterial hypertension: Comparison with bosentan and sildenafil. Eur. Respir. J. 2010, 36, 800–807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMurtry, M.S.; Bonnet, S.; Michelakis, E.D.; Bonnet, S.; Haromy, A.; Archer, S.L. Statin therapy, alone or with rapamycin, does not reverse monocrotaline pulmonary arterial hypertension: The rapamcyin-atorvastatin-simvastatin study. Am. J. Physiol. Lung Cell. Mol. Physiol. 2007, 293, 933–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, J.J.; Huston, J.; Kutty, S.; Hatton, N.D.; Bowman, L.; Tian, L.; Herr, J.E.; Johri, A.M.; Archer, S.L. Right ventricular adaptation and failure in pulmonary arterial hypertension. Can. J. Cardiol. 2015, 31, 391–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clozel, M.; Hess, P.; Rey, M.; Iglarz, M.; Binkert, C.; Qiu, C. Bosentan, sildenafil, and their combination in the monocrotaline model of pulmonary hypertension in rats. Exp. Biol. Med. 2006, 231, 967–973. [Google Scholar]
- Genovesi, S.; Giussani, M.; Orlando, A.; Lieti, G.; Viazzi, F.; Parati, G. Relationship between endothelin and nitric oxide pathways in the onset and maintenance of hypertension in children and adolescents. Pediatr. Nephrol. 2022, 37, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Podyacheva, E.Y.; Kushnareva, E.A.; Karpov, A.A.; Toropova, Y.G. Analysis of models of doxorubicin-induced cardiomyopathy in rats and mice. A modern view from the perspective of the pathophysiologist and the clinician. Front. Pharmacol. 2021, 12, 670479. [Google Scholar] [CrossRef]
- Cannan, C.R.; Burnett, J.C.; Lerman, A. Enhanced coronary vasoconstriction to endothelin B receptor activation in experimental chronic heart failure. Circulation 1996, 93, 646–651. [Google Scholar] [CrossRef]
- Cannan, C.R.; Verghese, M.; Lerman, A. New insight into coronary endothelial dysfunction. Role of endotehlin. J. Lab. Clin. Med. 1998, 131, 300–305. [Google Scholar] [CrossRef]
- Kiowski, W.; Sutsch, G.; Hunziker, P.; Müller, P.; Kim, J.; Oechslin, E.; Schmitt, R.; Jones, R.; Bertel, O. Evidence for endothelin-mediated vasoconstriction in severe chronic heart failure. Lancet 1995, 346, 732–736. [Google Scholar] [CrossRef]
- Berger, R.; Strecker, K.; Huelsmann, M.; Moser, P.; Frey, B.; Bojic, A.; Stanek, B.; Pacher, R. Prognostic power of neurohumoral parameters in chronic heart failure depends on clinical stage and observation period. J. Heart Lung Transpl. 2003, 22, 1037–1045. [Google Scholar] [CrossRef]
- Mulder, P.; Richard, V.; Derumeaux, G.; Hogie, M.; Henry, J.P.; Lallemand, F.; Compagnon, P.; Macé, B.; Comoy, E.; Letac, B.; et al. Role of endogenous endothelin in chronic heart failure. Circulation 1997, 96, 1976–1982. [Google Scholar] [CrossRef]
- Nakamura, M.; Saito, S.; Yoshida, H.; Arakawa, N.; Sugawara, S.; Hiramori, K. Effects of chronic subdepressor dose of angiotensin II type 1 receptor antagonist on endothelium-dependent vasodilatation in patients with congestive heart failure. J. Cardiovasc. Pharmacol. 2002, 40, 411–419. [Google Scholar] [CrossRef]
- Pacher, R.; Bergler-Klein, J.; Globits, S.; Teufelsbauer, H.; Schuller, M.; Krauter, A.; Ogris, E.; Rödler, S.; Wutte, M.; Hartter, E. Plasma big endothelin-1 concentrations in congestive heart failure compared to systemic hypertension. Am. J. Cardiol. 1993, 71, 1293–1299. [Google Scholar] [CrossRef]
- Trochu, J.N.; Bouhour, J.B.; Kaley, G.; Hintze, T.H. Role of endothelium- derived nitric oxide in the regulation of cardiac oxygen metabolism: Implications in health and disease. Circ. Res. 2000, 87, 1108–1117. [Google Scholar] [CrossRef] [Green Version]
- Vasku, A.; Spinarova, L.; Goldbergova, M.; Muzik, J.; Spinar, J.; Vítovec, J.; Toman, J.; Vácha, J. The double heterozygote of two endothelin-1 gene polymorphisms (G8002 and -3A/-4A) is related to big endothelin levels in chronic heart failure. Exp. Mol. Pathol. 2002, 73, 230–233. [Google Scholar] [CrossRef]
- Yamauchi, Y.; Kurosaki, E.; Azuma, H. Pathophysiological role of endothelin-1 in the vascular remodeling process. Folia Pharmacol. Jpn. Nippon. Yakurigaku Zasshi 2002, 120 (Suppl. S1), 79P–91P. [Google Scholar]
- Yoshizumi, M.; Kagami, S.; Suzaki, Y.; Tsuchiya, K.; Houchi, H.; Hisayama, T.; Fukui, H.; Tamaki, T. Effect of endothelin-1(1–31) on human mesangial cell proliferation. Jpn. J. Pharmacol. 2000, 84, 146–155. [Google Scholar] [CrossRef] [Green Version]
- Lavallee, M.; Takamura, M.; Parent, R.; Thorin, E. Crosstalk between endothelin and nitric oxide in the control of vascular tone. Heart Fail Rev. 2001, 6, 265–276. [Google Scholar] [CrossRef]
- Wittstein, I.S.; Kass, D.A.; Pak, P.H.; Maughan, W.L.; Fetics, B.; Hare, J.M. Cardiac nitric oxide production due to angiotensin-converting enzyme inhibition decreases beta-adrenergic myocardial contractility in patients with dilated cardiomyopathy. J. Am. Coll. Cardiol. 2001, 38, 429–435. [Google Scholar] [CrossRef] [Green Version]
- Hülsmann, M.; Stanek, B.; Frey, B.; Sturm, B.; Putz, D.; Kos, T.; Berger, R.; Woloszczuk, W.; Putz, D.; Kos, T.; et al. Value of cardiopulmonary exercise testing and big endothelin plasma levels to predict short-term prognosis of patients with chronic heart failure. J. Am. Coll. Cardiol. 1998, 32, 1695–1700. [Google Scholar] [CrossRef] [Green Version]
- Pacher, R.; Stanek, B.; Hulsmann, M.; Koller-Strametz, J.; Berger, R.; Schuller, M.; Hartter, E.; Ogris, E.; Frey, B.; Heinz, G.; et al. Prognostic impact of big endothelin-1 plasma concentrations compared with invasive hemodynamic evaluation in severe heart failure. J. Am. Coll. Cardiol. 1996, 27, 633–641. [Google Scholar] [CrossRef] [Green Version]
- Wexberg, P.; Pacher, R.; Rodler, S.; Kiss, K.; Beran, G.; Grimm, M.; Maurer, G.; Glogar, D. Intimal hyperplasia and coronary flow reserve after heart transplantation: Association with big endothelin-1. J. Heart Lung Transpl. 2002, 21, 1257–1263. [Google Scholar] [CrossRef]
- van Dalen, E.C.; Caron, H.N.; Dickinson, H.O.; Kremer, L.C.M. Cardioprotective interventions for cancer patients receiving anthracyclines. Cochrane Database Syst. Rev. 2008, 2, CD003917. [Google Scholar]
- Bonadonna, G.; Morfandini, S. Cardiac toxicity of daunorubicin. Lancet 1969, 1, 837. [Google Scholar] [CrossRef]
- Lefrak, E.A.; Pitha, J.; Rosenheim, S.; Gottlieb, J.A. A clinicopathologic analysis of adriamycin cardiotoxicity. Cancer 1973, 32, 302–314. [Google Scholar] [CrossRef]
- Keizer, H.G.; Pinedo, H.M.; Schuurhuis, G.J.; Joenje, H. Doxorubicin (adriamycin): A critical review of free radical dependent mechanisms of cytotoxicity. Pharmacol. Ther. 1990, 47, 219–231. [Google Scholar] [CrossRef]
- Myers, C. The role of iron in doxorubicin-induced cardiomyopathy. Semin. Oncol. 1998, 25 (Suppl. S10), 10–14. [Google Scholar]
- Luetic, K.; Sucic, M.; Vlainic, J.; Halle, Z.B.; Strinic, D.; Vidovic, T.; Luetic, F.; Marusic, M.; Gulic, S.; Pavelic, T.T.; et al. Cyclophosphamide induced stomach and duodenal lesions as a NO-system disturbance in rats: L-NAME, L-arginine, stable gastric pentadecapeptide BPC 157. Inflammopharmacology 2017, 25, 255–264. [Google Scholar] [CrossRef]
- Sucic, M.; Luetic, K.; Jandric, I.; Drmic, D.; Sever, A.Z.; Vuletic, L.B.; Halle, Z.B.; Strinic, D.; Kokot, A.; Seiwerth, R.S.; et al. Therapy of the rat hemorrhagic cystitis induced by cyclophosphamide. Stable gastric pentadecapeptide BPC 157, L-arginine, L-NAME. Eur. J. Pharmacol. 2019, 861, 172593. [Google Scholar] [CrossRef]
- Radeljak, S.; Seiwerth, S.; Sikiric, P. BPC 157 inhibits cell growth and VEGF signalling via the MAPK kinase pathway in the human melanoma cell line. Melanoma Res. 2004, 14, A14–A15. [Google Scholar] [CrossRef]
- Shantsila, E.; Wrigley, B.J.; Blann, A.D.; Gill, P.S.; Lip, G.Y. A contemporary view on endothelial function in heart failure. Eur. J. Heart Fail. 2012, 14, 873–881. [Google Scholar] [CrossRef]
- Obeidat, M.; Burgess, M.; Lip, G.Y.H. Atrial fibrillation in heart failure: Focus on antithrombotic management. Cardiol. Clin. 2022, 40, 245–258. [Google Scholar] [CrossRef]
- Prandoni, P. Venous, arterial thrombosis: Two aspects of the same disease? Eur. J. Intern. Med. 2009, 20, 660–661. [Google Scholar] [CrossRef] [Green Version]
- Prandoni, P. Venous and arterial thrombosis: Is there a link? Adv. Exp. Med. Biol. 2017, 906, 273–283. [Google Scholar]
- Oh, G.C.; Cho, H.J. Blood pressure and heart failure. Clin. Hypertens. 2020, 26, 1. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.E.; Lee, H.Y.; Cho, H.J.; Choe, W.S.; Kim, H.; Choi, J.O.; Jeon, E.S.; Kim, M.S.; Hwang, K.; Chae, S.C.; et al. Reverse J-curve relationship between on-treatment blood pressure and mortality in patients with heart failure. JACC Heart Fail. 2017, 5, 810–819. [Google Scholar] [CrossRef]
- Sikirić, P.; Petek, M.; Rucman, R.; Seiwerth, S.; Grabarević, Z.; Rotkvić, I.; Turković, B.; Jagić, V.; Mildner, B.; Duvnjak, M.; et al. A new gastric juice peptide, BPC. An overview of the stomach-stress-organoprotection hypothesis and beneficial effects of BPC. J. Physiol. Paris 1993, 87, 313–327. [Google Scholar] [CrossRef]
- Petrovic, I.; Dobric, I.; Drvis, P.; Shejbal, D.; Brcic, L.; Blagaic, A.B.; Batelja, L.; Kokic, N.; Tonkic, A.; Mise, S.; et al. An experimental model of prolonged esophagitis with sphincter failure in the rat and the therapeutic potential of gastric pentadecapeptide BPC 157. J. Pharmacol. Sci. 2006, 102, 269–277. [Google Scholar] [CrossRef] [Green Version]
- Cautela, J.; Tartiere, J.M.; Cohen-Solal, A.; Bellemain-Appaix, A.; Theron, A.; Tibi, T.; Januzzi, J.L., Jr.; Roubille, F.; Girerd, N. Management of low blood pressure in ambulatory heart failure with reduced ejection fraction patients. Eur. J. Heart Fail. 2020, 22, 1357–1365. [Google Scholar] [CrossRef]
- Dobric, I.; Drvis, P.; Petrovic, I.; Shejbal, D.; Brcic, L.; Blagaic, A.B.; Batelja, L.; Sever, M.; Kokic, N.; Tonkic, A.; et al. Prolonged esophagitis after primary dysfunction of the pyloric sphincter in the rat and therapeutic potential of the gastric pentadecapeptide BPC 157. J. Pharmacol. Sci. 2007, 104, 7–18. [Google Scholar] [CrossRef] [Green Version]
- Belosic Halle, Z.; Vlainic, J.; Drmic, D.; Strinic, D.; Luetic, K.; Sucic, M.; Medvidovic-Grubisic, M.; Pavelic Turudic, T.; Petrovic, I.; Seiwerth, S.; et al. Class side effects: Decreased pressure in the lower oesophageal and the pyloric sphincters after the administration of dopamine antagonists, neuroleptics, anti-emetics, L-NAME, pentadecapeptide BPC 157 and L-arginine. Inflammopharmacology 2017, 25, 511–522. [Google Scholar] [CrossRef] [PubMed]
- Cesarec, V.; Becejac, T.; Misic, M.; Djakovic, Z.; Olujic, D.; Drmic, D.; Brcic, L.; Rokotov, D.S.; Seiwerth, S.; Sikiric, P. Pentadecapeptide BPC 157 and the esophagocutaneous fistula healing therapy. Eur. J. Pharmacol. 2013, 701, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Skorjanec, S.; Kokot, A.; Drmic, D.; Radic, B.; Sever, M.; Klicek, R.; Kolenc, D.; Zenko, A.; Lovric Bencic, M.; Belosic Halle, Z.; et al. Duodenocutaneous fistula in rats as a model for “wound healing-therapy” in ulcer healing: The effect of pentadecapeptide BPC 157, L-nitro-arginine methyl ester and L-arginine. J. Physiol. Pharmacol. 2015, 66, 581–590. [Google Scholar] [PubMed]
- Becejac, T.; Cesarec, V.; Drmic, D.; Hirsl, D.; Madzarac, G.; Djakovic, Z.; Bunjevac, I.; Zenko Sever, A.; Sepac, A.; Batelja Vuletic, L.; et al. An endogeous defensive concept, renewed cytoprotection/adaptive cytoprotection: Intra(per)-oral/intragastric strong alcohol in rat. Involvement of pentadecapeptide BPC 157 and nitric oxide system. J. Physiol. Pharmacol. 2018, 69, 3. [Google Scholar] [CrossRef]
- Vitaic, S.; Stupnisek, M.; Drmic, D.; Bauk, L.; Kokot, A.; Klicek, R.; Vcev, A.; Luetic, K.; Seiwerth, S.; Sikiric, P. Nonsteroidal anti-inflammatory drugs-induced failure of lower esophageal and pyloric sphincter and counteraction of sphincters failure with stable gatric pentadecapeptide BPC 157 in rats. J. Physiol. Pharmacol. 2017, 68, 265–272. [Google Scholar] [PubMed]
- Djakovic, Z.; Djakovic, I.; Cesarec, V.; Madzarac, G.; Becejac, T.; Zukanovic, G.; Drmic, D.; Batelja, L.; Zenko Sever, A.; Kolenc, D.; et al. Esophagogastric anastomosis in rats: Improved healing by BPC 157 and L-arginine, aggravated by L-NAME. World J. Gastroenterol. 2016, 22, 9127–9140. [Google Scholar] [CrossRef]
- Kokot, A.; Zlatar, M.; Stupnisek, M.; Drmic, D.; Radic, R.; Vcev, A.; Seiwerth, S.; Sikiric, P. NO system dependence of atropine-induced mydriasis and L-NAME- and L-arginine-induced miosis: Reversal by the pentadecapeptide BPC 157 in rats and guinea pigs. Eur. J. Pharmacol. 2016, 771, 211–219. [Google Scholar] [CrossRef]
- Jandric, I.; Vrcic, H.; Jandric Balen, M.; Kolenc, D.; Brcic, L.; Radic, B.; Drmic, D.; Seiwerth, S.; Sikiric, P. Salutary effect of gastric pentadecapeptide BPC 157 in two different stress urinary incontinence models in female rats. Med. Sci. Monit. Basic Res. 2013, 19, 93–102. [Google Scholar] [CrossRef] [Green Version]
- Rasic, D.; Zenko Sever, A.; Rasic, F.; Strbe, S.; Rasic, Z.; Djuzel, A.; Duplancic, B.; Boban Blagaic, A.; Skrtic, A.; Seiwerth, S.; et al. Stable gastric pentadecapeptide BPC 157 heals established vesicovaginal fistula and counteracts stone formation in rats. Biomedicines 2021, 9, 1206. [Google Scholar] [CrossRef]
- Harris, A.S.; Kokernot, R.H. Effects of diphenylhydantoin sodium (dilantin sodium) and phenobarbital sodium upon ectopic ventricular tachycardia in acute myocardial infarction. Am. J. Physiol. 1950, 163, 505–516. [Google Scholar] [CrossRef]
- Clausen, T. Hormonal and pharmacological modification of plasma potassium homeostasis. Fundam. Clin. Pharmacol. 2010, 5, 595–605. [Google Scholar] [CrossRef]
- Medvidovic-Grubisic, M.; Stambolija, V.; Kolenc, D.; Katancic, J.; Murselovic, T.; Plestina-Borjan, I.; Strbe, S.; Drmic, D.; Barisic, I.; Sindic, A.; et al. Hypermagnesemia disturbances in rats, NO-related: Pentadecapeptide BPC 157 abrogates, L-NAME and L-arginine worsen. Inflammopharmacology 2017, 25, 439–449. [Google Scholar] [CrossRef]
- Klicek, R.; Kolenc, D.; Suran, J.; Drmic, D.; Brcic, L.; Aralica, G.; Sever, M.; Holjevac, J.; Radic, B.; Turudic, T.; et al. Stable gastric pentadecapeptide BPC 157 heals cysteamine-colitis and colon-colon-anastomosis and counteracts cuprizone brain injuries and motor disability. J. Physiol. Pharmacol. 2013, 64, 597–612. [Google Scholar]
- Sikiric, P.; Marovic, A.; Matoz, W.; Anic, T.; Buljat, G.; Mikus, D.; Stancic-Rokotov, D.; Separovic, J.; Seiwerth, S.; Grabarevic, Z.; et al. A behavioural study of the effect of pentadecapeptide BPC 157 in Parkinson’s disease models in mice and gastric lesions induced by 1-methyl-4-phenyl-1,2,3,6-tetrahydrophyridine. J. Physiol. Paris 1999, 93, 505–512. [Google Scholar] [CrossRef]
- Zemba Cilic, A.; Zemba, M.; Cilic, M.; Balenovic, I.; Strbe, S.; Ilic, S.; Vukojevic, J.; Zoricic, Z.; Filipcic, I.; Kokot, A.; et al. Pentadecapeptide BPC 157 counteracts L-NAME-induced catalepsy. BPC 157, L-NAME, L-arginine, NO-relation, in the suited rat acute and chronic models resembling ‘positive-like’ symptoms of schizophrenia. Behav. Brain Res. 2021, 396, 112919. [Google Scholar] [CrossRef]
- Butterworth, J.F., IV. Models and mechanisms of local anesthetic cardiac toxicity. Reg. Anesth. Pain. Med. 2010, 35, 167–176. [Google Scholar] [CrossRef]
- Castle, N.A. Bupivacaine inhibits the transient outward K+ current but not the inward rectifier in rat ventricular myocytes. J. Pharmacol. Exp. Ther. 1990, 255, 1038–1046. [Google Scholar]
- Clarkson, C.W.; Hondeghem, L.M. Mechanism for bupivacaine depression of cardiac conduction: Fast block of sodium channels during the action potential with slow recovery from block during diastole. Anesthesiology 1985, 62, 396–405. [Google Scholar] [CrossRef]
- Bernardi, J.; Aromolaran, K.A.; Aromolaran, A.S. Neurological disorders and risk of arrhythmia. Int. J. Mol. Sci. 2021, 22, 188. [Google Scholar] [CrossRef]
- Jelovac, N.; Sikiric, P.; Rucman, R.; Petek, M.; Marovic, A.; Perovic, D.; Seiwerth, S.; Mise, S.; Turkovic, B.; Dodig, G.; et al. Pentadecapeptide BPC 157 attenuates disturbances induced by neuroleptics: The effect on catalepsy and gastric ulcers in mice and rats. Eur. J. Pharmacol. 1999, 379, 19–31. [Google Scholar] [CrossRef]
- Sikiric, P.; Seiwerth, S.; Rucman, R.; Kolenc, D.; Vuletic, L.B.; Drmic, D.; Grgic, T.; Strbe, S.; Zukanovic, G.; Crvenkovic, D.; et al. Brain-gut axis and pentadecapeptide BPC 157: Theoretical and practical implications. Curr. Neuropharmacol. 2016, 14, 857–865. [Google Scholar] [CrossRef] [PubMed]
- Tohyama, Y.; Sikiric, P.; Diksic, M. Effects of pentadecapeptide BPC157 on regional serotonin synthesis in the rat brain: Alpha-methyl-L-tryptophan autoradiographic measurements. Life Sci. 2004, 76, 345–357. [Google Scholar] [CrossRef] [PubMed]
- Zemba Cilic, A.; Zemba, M.; Cilic, M.; Strbe, S.; Ilic, S.; Vukojevic, J.; Zoricic, Z.; Filipcic, I.; Kokot, A.; Smoday, I.M.; et al. BPC 157, L-NAME, L-arginine, NO-relation, in the suited rat ketamine models resembling “negative-like” symptoms of schizophrenia. Biomedicines 2022, 10, 1462. [Google Scholar] [CrossRef] [PubMed]
- Blagaic, A.B.; Blagaic, V.; Romic, Z.; Sikiric, P. The influence of gastric pentadecapeptide BPC 157 on acute and chronic ethanol administration in mice. Eur. J. Pharmacol. 2004, 499, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Boban Blagaic, A.; Blagaic, V.; Mirt, M.; Jelovac, N.; Dodig, G.; Rucman, R.; Petek, M.; Turkovic, B.; Anic, T.; Dubovecak, M.; et al. Gastric pentadecapeptide BPC 157 effective against serotonin syndrome in rats. Eur. J. Pharmacol. 2005, 512, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Mirković, I.; Kralj, T.; Lozić, M.; Stambolija, V.; Kovačević, J.; Vrdoljak, L.; Zlatar, M.; Milanović, K.; Drmić, D.; Predović, J.; et al. Pentadecapeptide BPC 157 shortens duration of tetracaine- and oxybuprocaine-induced corneal anesthesia in rats. Acta Clin. Croat. 2020, 59, 394–406. [Google Scholar] [CrossRef]
- Sikiric, P.; Gyires, K.; Seiwerth, S.; Grabarevic, Z.; Rucman, R.; Petek, M.; Rotkvic, I.; Turkovic, B.; Udovicic, I.; Jagic, V.; et al. The effect of pentadecapeptide BPC 157 on inflammatory, non-inflammatory, direct and indirect pain and capsaicin neurotoxicity. Inflammopharmacology 1993, 2, 121–127. [Google Scholar] [CrossRef]
- Jung, Y.H.; Kim, H.; Kim, H.; Kim, E.; Baik, J.; Kang, H. The anti-nociceptive effect of BPC-157 on the incisional pain model in rats. J. Dent. Anesth. Pain Med. 2022, 22, 97–105. [Google Scholar] [CrossRef]
- Lee, E.; Padgett, B. Intra-articular injection of BPC 157 for multiple types of knee pain. Altern. Ther. Health Med. 2021, 27, 8–13. [Google Scholar]
- Park, S.Y.; Choi, S.R.; Kim, J.H.; Lee, S.C.; Jeong, S.Y.; Jeong, J.H.; Lee, T.Y. Antinociceptive Effect of BPC-157 in the formalin-induced pain model. Kosin Med. J. 2021, 36, 1147042. [Google Scholar] [CrossRef]
- Boban Blagaic, A.; Turcic, P.; Blagaic, V.; Dubovecak, M.; Jelovac, N.; Zemba, M.; Radic, B.; Becejac, T.; Stancic Rokotov, D.; Sikiric, P. Gastric pentadecapeptide BPC 157 counteracts morphine-induced analgesia in mice. J. Physiol. Pharmacol. 2009, 60 (Suppl. S7), 177–181. [Google Scholar]
- Tlak Gajger, I.; Ribaric, J.; Smodis Skerl, M.; Vlainic, J.; Sikiric, P. Stable gastric pentadecapeptide BPC 157 in honeybee (Apis mellifera) therapy, to control Nosema ceranae invasions in apiary conditions. J. Vet. Pharmacol. Ther. 2018, 41, 614–621. [Google Scholar] [CrossRef]
- Tlak Gajger, I.; Smodis Skerl, M.I.; Sostaric, P.; Suran, J.; Sikiric, P.; Vlainic, J. Physiological and immunological status of Adult honeybees (Apis mellifera) fed sugar syrup supplemented with pentadecapeptide BPC 157. Biology 2021, 10, 891. [Google Scholar] [CrossRef]
- Xu, C.; Sun, L.; Ren, F.; Huang, P.; Tian, Z.; Cui, J.; Zhang, W.; Wang, S.; Zhang, K.; He, L.; et al. Preclinical safety evaluation of body protective compound-157, a potential drug for treating various wounds. Regul. Toxicol. Pharmacol. 2020, 114, 104665. [Google Scholar] [CrossRef]


{kind=link}
| Noxious Procedure | BPC 157 Therapy Effects |
|---|---|
| Initial heart infarct induction and re-infarction, isoprenaline one or two application Escalated general peripheral and central syndrome [38] | Reduced levels of all necrosis markers, CK, CK-MB, LDH, and cTnT, and attenuated gross (no visible infarcted area) and histological damage, ECG (no ST-T ischemic changes), and echocardiography (preservation of systolic left ventricular function) damage induced by isoprenaline. Decrease in oxidative stress parameters and likely maintained NO-system function evidenced that BPC 157 interacted with eNOS and COX2 gene expression in a particular way and counteracted the noxious effect of the NOS-blocker, L-NAME. Early vessel and multiorgan failure (brain, heart, lung, liver, kidney, and gastrointestinal lesions), thrombosis, intracranial (superior sagittal sinus) hypertension, portal and caval hypertension, and aortal hypotension, ECG disturbances), in its full presentation was attenuated/eliminated by BPC 157 therapy (given at 5 min after isoprenaline) via activation of the azygos vein). |
| Intragastric administration of 96% alcohol Escalated general peripheral and central syndrome acute subendocardial infarct [40] | Intragastric administration of absolute alcohol-induced gastric lesions, intracranial (superior sagittal sinus) hypertension, severe brain swelling and lesions (i.e., intracerebral hemorrhage with degenerative changes of cerebral and cerebellar neurons), portal and vena caval hypertension, aortal hypotension, severe thrombosis, inferior vena cava and superior mesenteric vein congestion, azygos vein failure (as a failed collateral pathway), electrocardiogram disturbances, and heart (acute subendocardial infarct), lung (parenchymal hemorrhage), liver (congestion), and kidney (congestion) lesions. BPC 157 therapy (10 µg/kg or 10 ng/kg given intraperitoneally 1 min after alcohol) counteracted these deficits rapidly. Specifically, BPC 157 reversed brain swelling and superior mesenteric vein and inferior vena caval congestion and helped the azygos vein to recover, which improved the collateral blood flow pathway. |
| Lithium sulfate regimen in rats (500 mg/kg/day, ip, for three days, with assessment at 210 min after each administration of lithium) Escalated general peripheral and central syndrome Severe myocardial congestion, along with subendocardial infarcts [39] | BPC 157 counteracted the lithium-induced occlusive-like syndrome; rapidly counteracted brain swelling and intracranial (superior sagittal sinus) hypertension, portal hypertension, and aortal hypotension, which otherwise would persist; counteracted vessel failure; abrogated congestion of the inferior caval and superior mesenteric veins; reversed azygos vein failure; and mitigated thrombosis (superior mesenteric vein and artery), congestion of the stomach, and major hemorrhagic lesions. Both regimens of BPC 157 administration also counteracted the muscular weakness and prostration (as shown in microscopic and ECG recordings), myocardial congestion and infarction, in addition to edema and lesions in various brain areas; counteracted marked dilatation and central venous congestion in the liver; large areas of congestion and hemorrhage in the lung; and degeneration of proximal and distal tubules with cytoplasmic vacuolization in the kidney, attenuating oxidative stress. |
| Abdominal compartment syndrome (intra-abdominal pressure in thiopental-anesthetized rats at 25 mmHg (60 min), 30 mmHg (30 min), 40 mmHg (30 min), and 50 mmHg (15 min), and, in esketamine-anesthetized rats (25 mmHg for 120 min)) as a model of multiple occlusion syndrome Escalated general peripheral and central syndrome Severe myocardial congestion, along with subendocardial infarcts [31] | BPC 157 administration recovered the azygos vein via the inferiorsuperior caval vein rescue pathway. Additionally, intracranial (superior sagittal sinus), portal, and caval hypertension and aortal hypotension were reduced, as were the grossly congested stomach and major hemorrhagic lesions, brain swelling, venous and arterial thrombosis, congested inferior caval and superior mesenteric veins, and collapsed azygos vein; thus, the failed collateral pathway was fully recovered. Severe ECG disturbances (i.e., severe bradycardia and ST-elevation until asystole) were also reversed. Microscopically, transmural hyperemia of the gastrointestinal tract, intestinal mucosa villi reduction, crypt reduction with focal denudation of superficial epithelia, and large bowel dilatation were all inhibited. In the liver, BPC 157 reduced congestion and severe sinusoid enlargement. In the lung, a normal presentation was observed, with no alveolar membrane focal thickening and no lung congestion or edema, and severe intra-alveolar hemorrhage was absent. Moreover, severe heart congestion, subendocardial infarction, renal hemorrhage, brain edema, hemorrhage, and neural damage were prevented. |
| Bile duct ligation acute pancreatitis as local disturbances (i.e., improved gross and microscopy presentation, decreased amylase level) Escalated general peripheral and central syndrome Severe myocardial congestion, along with subendocardial infarcts [37] | Bile duct-ligated rats commonly presented intracranial (superior sagittal sinus), portal and caval hypertension and aortal hypotension, gross brain swelling, hemorrhage and lesions, heart dysfunction, lung lesions, liver and kidney failure, gastrointestinal lesions, and severe arterial and venous thrombosis, peripherally and centrally. Unless antagonized with the key effect of BPC 157 regimens, reversal of the inferior caval and superior mesenteric vein congestion and reversal of the failed azygos vein activated azygos vein-recruited direct delivery to rescue the inferior-superior caval vein pathway; these were all antecedent to acute pancreatitis major lesions (i.e., acinar, fat necrosis, hemorrhage). These lesions appeared in the later period but were markedly attenuated/eliminated (i.e., hemorrhage) in BPC 157-treated rats. To summarize, while the innate vicious cycle may be peripheral (bile duct ligation), or central (rapidly developed brain disturbances), or peripheral and central, BPC 157 resolved acute pancreatitis and its adjacent syndrome. |
| Superior mesenteric artery permanent occlusion Escalated general peripheral and central syndrome Severe myocardial congestion [19] | BPC 157 rapidly recruits collateral vessels (inferior anterior pancreaticoduodenal artery and inferior mesenteric artery) that circumvent occlusion and ascertains blood flow distant from the occlusion in the superior mesenteric artery. Portal and caval hypertension, aortal hypotension, and, centrally, superior sagittal sinus hypertension were attenuated or eliminated, and ECG disturbances were markedly mitigated. BPC 157 therapy almost annihilated venous and arterial thrombosis. Multiple organ lesions and disturbances (i.e., heart, lung, liver, and gastrointestinal tract, in particular, as well as brain) were largely attenuated. |
| Irremovable occlusion of the end of the superior mesenteric vein Escalated general peripheral and central syndrome Severe myocardial congestion [24] | BPC 157 rapidly activated the superior mesenteric vein-inferior anterior pancreaticoduodenal vein-superior anterior pancreaticoduodenal vein-pyloric vein-portal vein pathway, reestablished superior mesenteric vein and portal vein connection and reestablished blood flow. Simultaneously, toward inferior caval vein, an additional pathway appears via the inferior mesenteric vein, united with the middle colic vein, throughout its left colic branch to ascertain alternative bypassing blood flow. Consequently, BPC 157 acts peripherally and centrally and counteracts the intracranial (superior sagittal sinus), portal and caval hypertension, aortal hypotension, ECG disturbances attenuated, abolished progressing venous and arterial thrombosis. Additionally, BPC 157 counteracted multiorgan dysfunction syndrome, heart (severe myocardial congestion), lung, liver, kidney, gastrointestinal tract, brain lesions, and oxidative stress in tissues. |
| Permanently occluded essential vessel tributaries, both arterial and venous, occluded superior mesenteric vein and artery in rats Escalated general peripheral and central syndrome Severe myocardial congestion, along with subendocardial infarcts [29] | BPC 157 rapidly activated collateral pathways. These collateral loops were the superior mesenteric vein-inferior anterior pancreaticoduodenal vein-superior anterior pancreaticoduodenal vein-pyloric vein-portal vein pathway, an alternative pathway toward inferior caval vein via the united middle colic vein and inferior mesenteric vein through the left colic vein, and the inferior anterior pancreaticoduodenal artery and inferior mesenteric artery. Consequently, BPC 157 counteracted the superior sagittal sinus, portal and caval hypertension, aortal hypotension, progressing venous and arterial thrombosis peripherally and centrally, ECG disturbances attenuated. Markedly, the multiple organ lesions, heart, lung, liver, kidney, and gastrointestinal tract, in particular, as well as brain lesions and oxidative stress in tissues, were attenuated. |
| Complex syndrome of the occluded superior sagittal sinus, brain swelling and lesions, and multiple peripheral organs lesions in rat Escalated general peripheral and central syndrome Severe myocardial congestion [27] | The increased pressure in the superior sagittal sinus, portal and caval hypertension, aortal hypotension, arterial and venous thrombosis, severe brain swelling and lesions (cortex (cerebral, cerebellar), hypothalamus/thalamus, hippocampus), particular veins (azygos, superior mesenteric, inferior caval) dysfunction, heart dysfunction, lung congestion as acute respiratory distress syndrome, kidney disturbances, liver failure, and hemorrhagic lesions in gastrointestinal tract were all assessed. Rats received BPC 157 medication (10 µg/kg, 10 ng/kg) intraperitoneally, intragastrically, or topically to the swollen brain at 1 min ligation time or at 15 min, 24 h, and 48 h ligation time. BPC 157 therapy rapidly attenuates the brain swelling, rapidly eliminates the increased pressure in the ligated superior sagittal sinus and the severe portal and caval hypertension and aortal hypotension, and rapidly recruits collateral vessels, centrally ((para)sagittal venous collateral circulation) and peripherally (left superior caval vein azygos vein-inferior caval vein). BPC 157 therapy rapidly overwhelms the permanent occlusion of the superior sagittal sinus in rats and counteracts the brain, heart, lung, liver, kidney, and gastrointestinal lesions, and annihilates thrombosis, given at 1 min, 15 min, 24 h, or 48 h ligation-time. |
| Monocrotaline-induced pulmonary arterial hypertension in rats (wall thickness, total vessel area, heart frequency, QRS axis deviation, QT interval prolongation, increase in right ventricle systolic pressure, and body weight loss) [41] | After monocrotaline (80 mg/kg subcutaneously), BPC 157 (10 μg/kg or 10 ng/kg, days 1–14 or days 1–30 (early regimens), or days 14–30 (delayed regimen)) was given once daily intraperitoneally (last application 24 h before sacrifice) or continuously in drinking water until sacrifice (day 14 or 30). Without therapy, the outcome was the full monocrotaline syndrome, marked by right-side heart hypertrophy and massive thickening of the precapillary artery’s smooth muscle layer, clinical deterioration, and sometimes death due to pulmonary hypertension and right-heart failure during the fourth week after monocrotaline injection. With all BPC 157 regimens, monocrotaline-induced pulmonary arterial hypertension (including all disturbed parameters) was counteracted, and consistent beneficial effects were documented during the whole course of the disease. Pulmonary hypertension was not even developed (early regimens) as quickly as advanced pulmonary hypertension was rapidly attenuated and then completely eliminated (delayed regimen). |
| Congestive heart failure after doxorubicin regimen (total dose of 15 mg/kg intraperitoneally, divided at six time points, every third day for 14 days to induce congestive heart failure). After four weeks of rest, assessed in mice and rats with advanced disease course, the increased big endothelin-1 (BET-1) and plasma enzyme levels (CK, MBCK, LDH, AST, ALT), before and after next subsequent fourteen days of therapy, and clinical status (hypotension, increased heart rate and respiratory rate, and ascites) every two days [84]. | Without therapy, throughout 14 days, both rats and mice further raised BET-1 serum values and aggravated clinical status, while enzyme values maintained their initial increase. BPC 157 (10 µg/kg) and amlodipine treatment reversed the increased BET-1 (rats, mice), AST, ALT, CK (rats, mice), and LDH (mice) values. BPC 157 (10 ng/kg) and losartan opposed further increase of BET-1 (rats, mice). Losartan reduces AST, ALT, CK, and LDH serum values. BPC 157 (10 ng/kg) reduces AST and ALT serum values. Clinical status of chronic heart failure in rats and in mice is accordingly improved by the BPC 157 regimens and amlodipine. However, indicatively, translation to the counteracted hypotension, no dyspnea with increased heart and respiratory occurred in BPC 157 treated animals, whereas hypotension and dyspnea with increased heart rate and respiratory rate persisted in the losartan and amlodipine treated animals. |
| Applied Noxious Procedure and BPC 157 Therapy Effect | |
|---|---|
| Attenuated/Eliminated Arterial and Venous Thrombosis | Attenuated/Eliminated Bleeding |
| Abdominal aorta anastomosis in rats. J. Physiol. Pharmacol. 2009, 60 Suppl 7, 161–165. [18] | Infrarenal inferior caval vein occlusion in rats. Vascul. Pharmacol. 2018, 106, 54–66. [18] |
| Infrarenal inferior caval vein occlusion in rats. Vascul. Pharmacol. 2018, 106, 54–66. [22] | Suprahepatic occlusion of the inferior caval vein, Budd-Chiari syndrome model in rats. World J. Gastrointest. Pathophysiol. 2020, 11, 1–19. [23] |
| Suprahepatic occlusion of the inferior caval vein, Budd-Chiari syndrome model in rats. World J. Gastrointest. Pathophysiol. 2020, 11, 1–19. [23] | Pringle maneuver in rats, both ischemia and reperfusion. World J. Hepatol. 2020, 12, 184–206. [28] |
| Pringle maneuver in rats, both ischemia and reperfusion. World J. Hepatol. 2020, 12, 184–206. [28] | Occlusion of the superior mesenteric artery in rats. Biomedicines 2021, 9, 609. [19] |
| Occlusion of the superior mesenteric artery in rats. Biomedicines 2021, 9, 609. [19] | Occlusion of the end of the superior mesenteric vein in rats. Biomedicines 2021, 9, 1029. [24] |
| Occlusion of the end of the superior mesenteric vein in rats. Biomedicines 2021, 9, 1029. [24] | Occluded superior mesenteric artery and vein in rats. Biomedicines 2021, 9, 792. [29] |
| Occluded superior mesenteric artery and vein in rats. Biomedicines 2021, 9, 792. [29] | Occlusion of the superior sagittal sinus in rats. Biomedicines 2021, 9, 744. [27] |
| Occlusion of the superior sagittal sinus in rats. Biomedicines 2021, 9, 744. [27] | Perforated cecum lesions in rats. World J. Gastroenterol. 2018, 24, 5462–5476. [32] |
| Acute pancreatitis as vascular failure-induced severe peripheral and central syndrome in rats. Biomedicines. 2022, 10, 1299. [31] | Perforated stomach lesions in rats. J. Physiol. Pharmacol. 2021, 72(6). [33] |
| Primary abdominal compartment syndrome in rats. Front. Pharmacol. 2021, 12, 718147. [31] | Acute pancreatitis as vascular failure-induced severe peripheral and central syndrome in rats. Biomedicines. 2022, 10, 1299. [37] |
| Myocardial infarction induced by isoprenaline in rats. Biomedicines. 2022, 10, 265. [38] | Primary abdominal compartment syndrome in rats. Front. Pharmacol. 2021, 12, 718147. [31] |
| Over-dose lithium toxicity as an occlusive-like syndrome in rats. Biomedicines 2021, 9, 1506. [39] | Myocardial infarction induced by isoprenaline in rats. Biomedicines. 2022, 10, 265. [38] |
| Robert’s intragastric alcohol-induced gastric lesion model as an escalated general peripheral and central syndrome. Biomedicines. 2021, 9, 1300. [40] | Overdose lithium toxicity as an occlusive-like syndrome in rats. Biomedicines 2021, 9, 1506. [39] |
| Robert’s intragastric alcohol-induced gastric lesion model as an escalated general peripheral and central syndrome. Biomedicines. 2021, 9, 1300. [40] | |
| Definitive and early spinal cord injury in rats. Curr. Issues Mol. Biol. 2022, 44, 1901–1927. [36] | |
| Amputation in rats treated with heparin, warfarin or aspirin. Thromb. Res. 2012, 129, 652–659. [58] | |
| Amputation in rats treated with heparin, warfarin, L-NAME and L-arginine. PLoS ONE 2015, 10, e0123454. [59] | |
| Specifically maintained function of thrombocytes (aggregometry and thromboelastometry studies) | |
| Intragastric application of aspirin, clopidogrel, cilostazol, and BPC 157 in rats: Platelet aggregation and blood clot. Oxid. Med. Cell. Longev. 2019, 2019, 9084643. [60] | |
| Noxious Procedure | BPC 157 Therapy Effects |
|---|---|
| Cumulative intravenous digitalis toxicity, methyldigoxin increment regimen (2.0/1.5/1.5/1.0 mg/kg at 15 min-intervals, total dose 6.0 mg/kg/45 min Advanced methyldigoxin toxicity (6.0 mg/kg i.v. bolus) [66]. | BPC 157 (50 µg, 10 µg, 10 ng/kg) applied intravenously immediately before a methyldigoxin increment reduced the number of ventricular premature beats, prolonged the time before onset of ventricular tachycardia, reduced ventricular tachycardia and AV-block duration (µg-regimes) or reduced mainly the AV-block duration (ng-regimen). With the advanced methyldigoxin toxicity, BPC 157 applied at the 20th second of the grade 3 AV-block shortened AV-blocks, mitigated a further digitalis toxicity course. Ventricular tachycardias were either avoided (50 µg) or markedly reduced (10 µg, 10 ng). Fatal outcome was either avoided (50 µg), reduced (10 µg), or only delayed (10 ng). |
| Intraperitoneal KCl-solution application (9 mEq/kg). Promptly unrelenting hyperkalemia (>12 mmol/L), arrhythmias (and muscular weakness, hypertension, low pressure in lower esophageal and pyloric sphincter) with an ultimate and a regularly inevitable lethal outcome within 30 min. Intragastric KCl-solution application (27 mEq/kg)–(hyperkalemia 7 mmol/L): severe stomach mucosal lesions, sphincter failure, and peaked T waves HEK293 cells, hyperkalemic conditions (18.6 mM potassium concentrations), the effect on membrane potential, and depolarizations caused by hyperkalemic conditions [67]. | Life-saving effect in severe hyperkalemia without affecting the extremely high level of potassium in blood. Given 30 min before KCl, all BPC 157 regimens regained sinus rhythm, had less prolongation of QRS, and had no asystolic pause. BPC 157 therapy, given 10 min after KCl-application, starts the rescue within 5–10 min, completely restoring normal sinus rhythm at 1 h. Likewise, other hyperkalemia disturbances (muscular weakness, hypertension, low sphincteric pressure) were also counteracted. Intragastric BPC 157 (10 ng, 10 μg) application, given 30 min before or 10 min after intragastric KCl, fully counteracted the severe stomach mucosal lesions, sphincter failure, and peaked T waves. In HEK293 cells, in hyperkalemic conditions (18.6 mM potassium concentrations), BPC 157 directly affects potassium conductance, counteracting the effect on membrane potential and depolarizations caused by hyperkalemic conditions. |
| Succinylcholine administration (1.0 mg/kg into the right anterior tibial muscle). Assessments were made at 3 and 30 min and one, three, five, and seven days after. The local paralytic effect Systemic muscle disability (and consequent muscle damage), Hyperkalemia, arrhythmias, and a rise in serum enzyme values [68] | BPC 157 successfully antagonized the depolarizing neuromuscular blocker effects of succinylcholine. BPC 157 (10 µg/kg, 10 ng/kg) (given intraperitoneally 30 min before or immediately after succinylcholine or per-orally in drinking water through 24 h until succinylcholine administration) mitigated both local and systemic disturbances. BPC 157 completely eliminated hyperkalemia and arrhythmias, markedly attenuated or eradicated behavioral agitation, muscle twitches, motionless resting, and completely eliminated post-succinylcholine hyperalgesia. BPC 157 immediately eliminated leg contractures and counteracted both edema and the decrease in muscle fibers in the diaphragm and injected/non-injected anterior tibial muscles. |
| Furosemide (100 mg/kg intraperitoneally)-diuresis-hypokalemia mortal course in rats Deadly hypokalemia (<2.7 mmol/L) Severe arrhythmias (i.e., polymorphic ventricular tachycardia („torsades de pointes“)) Lethal outcome occurred within 90–150 min [69]. Membrane voltages (Vm) of HEK293 cells (the slow-whole cell patch clamp technique). Hypokalemic conditions (0.4 mM) cells hyperpolarized for −6.1 ± 1.1 mV [69]. | Life-saving effect in severe hypokalemia without affecting the extremely low level of potassium in blood. With prophylactic application (BPC 157 given 15 min before furosemide), all BPC 157 regimens maintained sinus rhythm, had no ventricular premature beats, ventricular tachycardia, AV block, no prolongation of intervals and waves without reduction of amplitude. With delayed application (BPC 157 given 90 min after furosemide, with hypokalemia, 3rd grade AV block and/ or ventricular tachycardia being present), within 5–10 min, BPC 157 regimens normalized P, R, S, T waves, PR, RR, QRS, QT interval duration, R, S, T wave amplitude, total AV block, and terminated ventricular tachycardia. Likewise, BPC 157 eliminated skeletal muscle myoclonus. HEK293 cell in hypokaliemic conditions. In hypokalemic conditions (0.4 mM) cells hyperpolarized for −6.1 ± 1.1 mV. After first hypokalemic step, the solution 1 μM BPC-157 depolarized cells for 4.6 ± 1.6 mV. Repeating hypokalemic step in the presence of BPC 157, cells did not hyperpolarize (3.1 ± 1.6 mV). After washing BPC 157 from bath solution, under hypokalemic conditions, cells hyperpolarized again. |
| Bupivacaine (100 mg/kg IP) in rats Bradycardia, AV-block, ventricular ectopies, ventricular tachycardia, T-wave elevation, and asystole. All of the fatalities with T-wave elevation, high-degree AV-block, respiratory arrest, and asystole. Membrane voltages (Vm) in HEK293 cells. Bupivacaine (1 mM) alone caused depolarization of the cells [70]. | BPC 157 as potential antidote for bupivacaine cardiotoxicity. Bradycardia, AV-block, ventricular ectopies, ventricular tachycardia, T-wave elevation, and asystole. All of the fatalities had developed T-wave elevation, high-degree AV-block, respiratory arrest, and asystole. These were largely counteracted by BPC 157 administration (50 µg/kg, 10 µg/kg, 10 ng/kg, or 10 pg/kg IP) given 30 min before or 1 min after the bupivacaine injection. When BPC 157 was given 6 min after bupivacaine administration and after the development of prolonged QRS intervals (20 ms), the fatal outcome was markedly postponed. Membrane voltages (Vm) in HEK293 cells demonstrated that in combination with BPC 157 (1 µm), the bupivacaine-induced depolarization was inhibited. |
| Lidocaine-induced local anesthesia via intraplantar application and axillary and spinal (L4-L5) intrathecal block, Lidocaine-induced arrhythmias, Lidocaine-induced convulsions, Lidocaine-induced HEK293 cell depolarization [71] | BPC 157 as antidote in its own against lidocaine and local anesthetics BPC 157 was applied immediately after lidocaine or 5 min before the application of lidocaine considerably ameliorated plantar presentation. BPC 157 medication considerably counteracted lidocaine-induced limb function failure. BPC 157 antagonized the lidocaine-induced bradycardia and eliminated tonic-clonic convulsions. Moreover, BPC 157 counteracted the lidocaine-induced depolarization of HEK293 cells. |
| During seven days, haloperidol (0.625, 6.25, 12.5, and 25.0 mg/kg ip), fluphenazine (0.5, 5.0 mg/kg ip), clozapine (1.0, 10.0 mg/kg ip), quetiapine (1.0, 10.0 mg/kg ip), sulpiride (1.6, 16.0 mg/kg ip), metoclopramide (2.5, 25.0 mg/kg ip) or (1.0, 10.0 mg/kg ip). Since very early, a prolonged QTc interval has been continually noted with haloperidol, fluphenazine, clozapine, olanzapine, quetiapine, sulpiride, and metoclopramide in rats as a common central effect not seen with domperidone [72]. | To counteract neuroleptic- or prokinetic-induced prolongation of the QTc interval, rats were given a BPC 157 regimen once daily over seven days (10 μg, 10 ng/kg ip) immediately after each administration of haloperidol, fluphenazine, clozapine, quetiapine, sulpiride, metoclopramide or domperidone. Consistent counteraction appears with the stable gastric pentadecapeptide BPC 157. Thus, BPC 157 rapidly and permanently counteracts the QTc prolongation induced by neuroleptics and prokinetics. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikiric, P.; Udovicic, M.; Barisic, I.; Balenovic, D.; Zivanovic Posilovic, G.; Strinic, D.; Uzun, S.; Sikiric, S.; Krezic, I.; Zizek, H.; et al. Stable Gastric Pentadecapeptide BPC 157 as Useful Cytoprotective Peptide Therapy in the Heart Disturbances, Myocardial Infarction, Heart Failure, Pulmonary Hypertension, Arrhythmias, and Thrombosis Presentation. Biomedicines 2022, 10, 2696. https://doi.org/10.3390/biomedicines10112696
Sikiric P, Udovicic M, Barisic I, Balenovic D, Zivanovic Posilovic G, Strinic D, Uzun S, Sikiric S, Krezic I, Zizek H, et al. Stable Gastric Pentadecapeptide BPC 157 as Useful Cytoprotective Peptide Therapy in the Heart Disturbances, Myocardial Infarction, Heart Failure, Pulmonary Hypertension, Arrhythmias, and Thrombosis Presentation. Biomedicines. 2022; 10(11):2696. https://doi.org/10.3390/biomedicines10112696
Chicago/Turabian StyleSikiric, Predrag, Mario Udovicic, Ivan Barisic, Diana Balenovic, Gordana Zivanovic Posilovic, Dean Strinic, Sandra Uzun, Suncana Sikiric, Ivan Krezic, Helena Zizek, and et al. 2022. "Stable Gastric Pentadecapeptide BPC 157 as Useful Cytoprotective Peptide Therapy in the Heart Disturbances, Myocardial Infarction, Heart Failure, Pulmonary Hypertension, Arrhythmias, and Thrombosis Presentation" Biomedicines 10, no. 11: 2696. https://doi.org/10.3390/biomedicines10112696
APA StyleSikiric, P., Udovicic, M., Barisic, I., Balenovic, D., Zivanovic Posilovic, G., Strinic, D., Uzun, S., Sikiric, S., Krezic, I., Zizek, H., Yago, H., Gojkovic, S., Smoday, I. M., Kalogjera, L., Vranes, H., Sola, M., Strbe, S., Koprivanac, A., Premuzic Mestrovic, I., ... Seiwerth, S. (2022). Stable Gastric Pentadecapeptide BPC 157 as Useful Cytoprotective Peptide Therapy in the Heart Disturbances, Myocardial Infarction, Heart Failure, Pulmonary Hypertension, Arrhythmias, and Thrombosis Presentation. Biomedicines, 10(11), 2696. https://doi.org/10.3390/biomedicines10112696