Abstract
Multisystem inflammatory syndrome in children (MIS-C) is an immune-mediated complication of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection. Cardiovascular system is commonly involved. Acute heart failure (AHF) is the most severe complication of MIS-C, leading to cardiogenic shock. The aim of the study was to characterise the course of MIS-C with a focus on cardiovascular involvement, based on echocardiographic (echo) evaluation, in 498 children (median age 8.3 years, 63% boys) hospitalised in 50 cities in Poland. Among them, 456 (91.5%) had cardiovascular system involvement: 190 (48.2%) of patients had (most commonly atrioventricular) valvular insufficiency, 155 (41.0%) had contractility abnormalities and 132 (35.6%) had decreased left ventricular ejection fraction (LVEF < 55%). Most of these abnormalities improved within a few days. Analysis of the results obtained from two echo descriptions (a median of 5 days apart) revealed a >10% increase in LVEF even in children with primarily normal LVEF. Lower levels of lymphocytes, platelets and sodium and higher levels of inflammatory markers on admission were significantly more common among older children with contractility dysfunction, while younger children developed coronary artery abnormality (CAA) more often. The incidence of ventricular dysfunction might be underestimated. The majority of children with AHF improved significantly within a few days. CAAs were relatively rare. Children with impaired contractility as well as other cardiac abnormalities differed significantly from children without such conditions. Due to the exploratory nature of this study, these findings should be confirmed in further studies.
1. Introduction
Cardiac complications affect a significant percentage (from ~7 to >30%) of patients of all ages who are infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection [1]. It became clear that a history of cardiovascular disease is a risk factor for a severe course of coronavirus disease 2019 (COVID-19) soon after the pandemic began [2]. Further observations established that SARS-CoV-2 infection may be a risk factor for cardiac complications as well, even in previously healthy patients [3,4,5,6,7,8,9,10,11]. The most intriguing cardiological phenomena associated with the COVID-19 pandemic include cases of acute heart damage in patients who have multisystem inflammatory syndrome in children (MIS-C) [12,13,14]. This new disease appeared during the COVID-19 pandemic in children, most commonly of school age [14,15,16,17]. Isolated cases in young or middle-aged adults are referred to as multisystem inflammatory syndrome in adults (MIS-A) [18,19,20].
MIS-C is a late, immune-mediated complication occurring about 4 weeks after SARS-CoV-2 infection in 1 in 3000 unvaccinated children [21,22,23]. Due to the similarity of their clinical symptoms, MIS-C is compared with Kawasaki disease (KD), toxic shock, syndrome (TSS) and macrophage activation syndrome (MAS). Recently, however, it has become known as a separate and new disease entity [24,25,26]. The exact pathogenesis of changes in the course of MIS-C, including cardiac involvement, is yet to be known [22].
MIS-C includes gastrointestinal, mucocutaneous and neurological symptoms, as well as cardiac disorders. The most frequently observed cardiac abnormalities include ventricular dysfunctions, which may lead to cardiogenic shock. Pericardial effusion or coronary artery dilatation and aneurysms (CAAs) occur less frequently [12]. The acute and reversible nature of the heart failure in the course of MIS-C might resemble the picture of takotsubo syndrome (TTS) [27,28]. We have described such a case of TTS in the course of MIS-C before [29].
More precise characteristics of cardiovascular involvement come mostly from single-canter observation studies of relatively small groups of patients [14,30,31,32,33,34]. Regardless, the one undoubted conclusion from all the previous reports is that the involvement of the cardiovascular system is one of the most important features of MIS-C, and a paediatric cardiologist should be involved in the diagnostic and therapeutic process [35] to ensure optimal patient care.
The MultiOrgan Inflammatory Syndromes COVID-19 Related Study (MOIS-CoR) is a register of inflammatory diseases in children that captures and characterizes MIS-C cases in Poland [36,37]. Every wave of COVID-19 was followed by a wave of MIS-C cases of variable intensity. More than five hundred cases of MIS-C, defined according to the World Health Organization (WHO) [38], were reported by April 2022 [36]. Many paediatric centres struggled with limited access to paediatric cardiologists, as there are less than 200 such specialists in the country of 37 million people, including about 7 million children [39].
The main aims of our study were to (i) characterize cardiovascular involvement in MIS-C in our population and (ii) identify patients with MIS-C who should be prioritised for highly specialised cardiac referral and diagnostics. We specifically aimed to identify the differences between children with and without contraction dysfunction or CAAs and to investigate the incidence of TTS echocardiographic signs in the course of MIS-C in our population.
2. Materials and Methods
2.1. Study Sample
A detailed description of the MOIS-CoR Study was presented in our previous publication [37]. In this retrospective case series study, we report data covering the period from 4 March 2020 (when the first COVID-19 case was confirmed in Poland) to 14 April 2022, coming from 50 Polish cities. We concentrated particularly on cardiovascular involvement in MIS-C. Therefore, we only included children who:
- (1)
- Fulfilled the criteria for MIS-C adapted from the WHO;
- (2)
- Did not have any previous cardiovascular comorbidities (including congenital heart defects or hypertension);
- (3)
- Had at least one echocardiography (echo) result available (Figure 1).
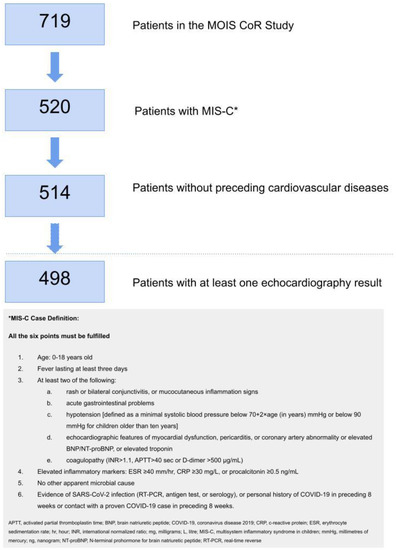 Figure 1. The flow chart for the study recruitment process and the MIS-C definition applied for the study. Study recruitment process.
Figure 1. The flow chart for the study recruitment process and the MIS-C definition applied for the study. Study recruitment process.
2.2. Study Design and Definitions
Anonymised patient data including demographic, clinical characteristics, laboratory test results, cardiovascular evaluation results and treatment data were analysed. Vital signs and laboratory parameters were obtained at admission and at their respective peaks. Body mass index (BMI) was converted into Z-scores based on the WHO reference standards for children younger than 5 years [40] and national reference standards for older children [41].
For the echocardiographic findings, we extracted information on:
- (1)
- Contractility abnormalities—the presence of any contractility dysfunction described by the cardiologist.
- (2)
- Valvular insufficiency—graded based on the interpreting physician’s qualitative assessment.
- (3)
- Left ventricular ejection fraction (LVEF)—evaluated using Simpson’s biplane method as normal (LVEF ≥ 55%) or decreased (LVEF < 55%).
- (4)
- Pericardial effusion—as graded by the interpreting physician’s assessment.
- (5)
- Coronary arteries abnormalities (CAAs)—CAAs were further categorised based on the Z-scores according to Dallaire [42] into dilation (a Z-score between 2 and 2.5), small aneurysms (a Z-score between 2.5 and 5), medium aneurysms (a Z-score between 5 and 10 and absolute dimension less than 8 mm) and large aneurysms (a Z-score ≥ 10 or absolute dimension ≥ 8 mm) [43]. If there were no precise measurements of the coronary artery diameter, but a CAA was diagnosed, it was categorised either as dilation or an aneurysm according to the description.
If a full description of echocardiographic findings was not available but information on normal results was provided, we categorised it as absence of listed abnormalities accordingly.
We introduced study definitions as follows:
- A.
- Laboratory findings for heart involvement—the presence of any of the listed abnormalities during the course of the hospitalisation:
- ○
- Elevated troponin (in respect to the type of troponin measured and the laboratory norm of the reporting site);
- ○
- Concentration of brain natriuretic peptide (BNP) ≥ 100 pg/mL;
- ○
- Concentration of N-terminal prohormone for brain natriuretic peptide (NT-proBNP) ≥ 300 pg/mL.
- B.
- Echocardiological findings for heart involvement—the presence of any of the listed abnormalities in any of the available echo results during hospitalisation:
- ○
- CAAs;
- ○
- Decreased LVEF;
- ○
- Contractility abnormalities;
- ○
- Valvular insufficiency (aortic valve insufficiency, IAoV; mitral valve insufficiency, IMV; pulmonary valve insufficiency, IPV; or tricuspid valve insufficiency, ITV);
- ○
- Pericardial effusion.
To determine the predictors and markers of echocardiographic abnormalities, we divided the study population into clusters, as presented on Figure 2.
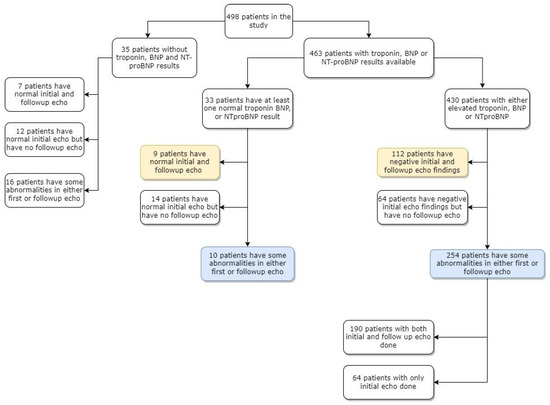
Figure 2.
Clustering the study population based on availability of cardiac tests and results. Yellow colour indicates patients with normal echo descriptions and blue colour indicates patients with abnormalities on echo descriptions. Abbreviations: BNP, brain natriuretic peptide; echo, echocardiography; NT-proBNP N-terminal prohormone for brain natriuretic peptide.
2.3. Statistical Methods
Variables were described in relation to the sum of non-missing observations for which the variable was recorded. Categorical variables were represented as counts and as percentages of non-missing values. Continuous data were represented as medians with upper (75th) and lower (25th) quartiles. Data were evaluated for normal distribution using density histograms overlaid with kernel density plots against a projected normal curve. Fisher’s exact test was used to assess independence between categorical variables. Student’s t-test and Kruskal–Wallis H test were used for categorical–continuous variable pairs. A significance level of 0.05 and two-sided testing were employed. We assumed missing values to be distributed randomly and independently from the data, and these missing data were treated through clinical definitions according to Łukasiewicz’s logic. A one-way analysis of variance (ANOVA) was used to compare our three major age groups (<5 years, 5–11 years and 12–18 years) against potential covariates that may vary with age. Bartlett’s test was calculated alongside the one-way ANOVA to check if variances were equal across groups or samples. To discern covariates that may predict echocardiological involvement in patients with MIS-C, patient characteristics, presenting symptoms and laboratory findings on admission were compared in two patient populations: patients with negative echocardiographic findings (consisting of patients who have normal cardiac lab markers with normal echo findings and patients with elevated cardiac lab markers) versus patients with positive echocardiographic findings (irrespective of having elevated or normal cardiac lab markers). Initial and follow-up echocardiographic characteristics of the overall cohort were evaluated using the abovementioned statistical methods. The subset of patients who had both initial and follow-up echo results were compared using McNemar’s test for categorical variables, and by paired-t-tests for continuous variables. Additionally, comparisons between patients with normal and reduced LVEF were made for both initial and follow-up echo findings. p-values were also calculated between initial and follow-up echo findings in patients with normal and reduced LVEF. To further assess cardiac involvement by specific cardiac abnormalities, variables such as patient demographics, laboratory and vital signs at admission and presenting symptoms were tested against study populations, defined as patients with and without CAAs at any time; patients with and without pericardial effusion at any time; patients with and without reduced LVEF at any time; and patients with and without contractility abnormalities at any time. All statistical analyses were performed in Stata 16.1 (College Station, TX, USA: StataCorp LLC.). MIS-C incidence was estimated based on the demographic data published by Statistics Poland.
2.4. Ethical Statement
Ethical approval was obtained from the Bioethics Committee at Wroclaw Medical University (CWN UMW BW: 313/2020). Waiver of informed consent was obtained with only deidentified data transmitted and analysed.
3. Results
3.1. Study Sample
Four hundred ninety-eight children (median age 8.3 years, 63% male, all of White ethnicity except for two Asian patients) were included in the analysis (Figure 1). Ninety percent of children were previously healthy, with the most common comorbidity being asthma (5%). Seven percent were obese. The characteristics of the study group and MIS-C presentation depending on age group (<5; 5–11; 12–18 years of age) are presented in Table 1 and Supplementary Table S1. Gastrointestinal (GI), mucocutaneous, neurological and cardiovascular systems were the most commonly involved overall. Clinical presentation differed by age with GI, with lower respiratory symptoms and osteoarticular and muscle involvement appearing more commonly in older children. A significant proportion of patients had abnormal vital signs. Overall, 49% of children developed hypotension, which was significantly more common in older age groups. The laboratory parameters of MIS-C encompassed lymphopenia, high concentrations of inflammatory markers such as C-reactive protein (CRP) and procalcitonin, hyponatremia, hypoalbuminemia, elevated concentration of D-dimers and BNP/NT-proBNP and less often, elevated troponin. There were significant differences between age groups in laboratory test results as well. Older children had lower lymphocyte counts, higher CRP and ferritin concentrations, lower sodium concentrations, more frequent occurrences of renal function impairment and elevated troponin.

Table 1.
The characteristics of the study group and multisystem inflammatory syndrome course by age group.
A total of 93% of patients had laboratory findings for heart involvement and 56.2% had echocardiographic findings for heart involvement.
3.2. Laboratory Markers for Cardiovascular Involvement
The majority of children had elevated levels of either BNP/NT-proBNP or troponin (Figure 2). Median BNP concentration on admission was 287 pg/mL (IQR 114–1006) and that of NT-proBNP was 2176 pg/mL (IQR 486–7526). Median values at the respective peak are presented in Table 1 and Supplementary Table S1. A total of 63 (26%) children had elevated troponin on admission and 100 children had elevated troponin (38%) at any point during the hospitalisation.
3.3. Echocardiography Findings
All children included in this analysis had an echo performed at least once during their hospitalisation. Median time from the disease symptoms onset to hospital admission was five (IQR 4–6) days and that to the initial echo examination was six (IQR 4–8) days. For 337 (68%) children, a follow-up echo was performed with a median of five (IQR 2–7) days passing from the initial echo and a median of 11 (IQR 8–14) days from the disease onset. Median hospital stay was 11 (IQR: 9–14) days.
The most common echo finding was valvular insufficiency, which was present in 48% of children. Atrioventricular valve insufficiency was the most common type, with mitral valve insufficiency (IMV) described in 43% and tricuspid valve insufficiency (ITV) in 19% of children. Pulmonary valve insufficiency (IPV) was described in 3% and aortic valve insufficiency (IAoV) only in three patients. Most of the cases of regurgitation were considered benign; 10% of children had valvular insufficiency assessed as moderate or severe at the initial echo and 8% in the follow-up echo (Table 2 and Supplementary Table S2).
Table 2.
Changes between the baseline and follow-up echocardiography findings in patients with multisystem inflammatory syndrome in children (MIS-C) and two available echo descriptions.
The second most common echo finding was contractility abnormality, which was described in 41% of children at any time of the hospitalisation, with decreased LVEF in 36%. Median LVEF was 55% (IQR 17) in the initial echo and 56% (IQR 17) in the follow-up echo. Twenty-six percent of patients had decreased LVEF in the initial echo and 14% in the follow-up echo (Table 2 and Supplementary Table S2).
CAAs (aneurysm or dilation) were found in 11% of children (8 dilations, 11 small, 5 medium, 1 large aneurysm and 1 of unspecified size in the initial echo, and 6 dilations, 8 small, 3 medium and 2 large aneurysms in the follow-up echo). CAAs were found significantly more often in younger age groups. The opposite was true for contractility abnormalities and decreased LVEF, which were more common in older age groups, as seen in Table 1 and Supplementary Table S1.
By the time of the follow-up echo, a significant improvement was noted for valve insufficiency, contractility abnormalities and LVEF. We did not find significant differences in CAAs and pericardial effusion between the initial and follow-up echoes (Table 2 and Supplementary Table S3). Interestingly, there were more children with segmental contraction abnormalities including apex rounding in the follow-up echo (20 cases) than in the initial one (11 cases), but the general number of children with this condition during hospitalisation was relatively low (31 cases).
The baseline median LVEF increased significantly from 56% (IQR 47–64) to 57% (IQR 50–69) in the follow-up echo (p < 0.01). Cases with an increase over 10% in LVEF was observed even in children who had a baseline echo described as normal (with LVEF > 55%; Figure 3).
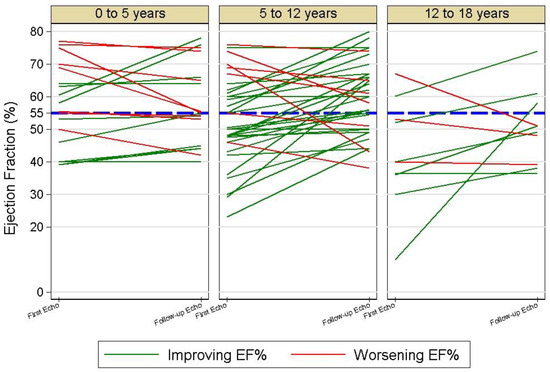
Figure 3.
Left ventricular ejection fraction changes during the hospitalisation with the multisystem inflammatory syndrome in children (MIS-C) in age groups.
Ejection fraction (EF)—left ventricular ejection fraction was evaluated using Simpson’s biplane method. The blue line indicates the value of 55%, which is considered as the norm for children.
Demographic and clinical features (signs and symptoms, laboratory test results and vital signs reported on admission) of children with and without echo findings were compared. From the 463 patients with laboratory and echo variables available, 264 children had any of the listed echo findings diagnosed. One hundred twenty-one patients had first and follow-up echoes performed and no echo abnormalities (Figure 2). Children with echo abnormalities more often presented neurological symptoms (including headache, lethargy or agitation) and breathing effort. They had lower systolic blood pressure and more often hypotension, and a higher respiratory rate on admission than children without any echo findings. Except for elevated troponin, they also had a higher procalcitonin concentration and lower sodium concentration (Table 3 and Supplementary Table S4).
Table 3.
Comparison between patients with and without echocardiographic abnormalities in the course of the multisystem inflammatory syndrome in children (MIS-C).
A similar comparison was performed between children with and without particular echo findings (Table 4 and Supplementary Table S5).
Table 4.
Comparison between children with and without coronary artery abnormalities (CAAs), contractility abnormalities and pericardial effusion in the course of the multisystem inflammatory syndrome in children.
We found that younger age, arthritis, conjunctivitis, eyelid swelling, a higher lymphocyte count and higher platelets on admission were predictive for CAAs. Children with abdominal pain, nausea or vomiting, conjunctivitis or swollen eyelids had CAAs less frequently than children without these signs.
Older age, the presence of neurological symptoms, breathing effort, chest pain, lower lymphocyte concentrations, lower platelet concentrations and higher CRP, higher procalcitonin, lower sodium, lower eGFR and higher BNP/NT-proBNP levels, as well as elevated troponin concentration on admission, were significantly more common in children with contractility dysfunction and decreased LVEF.
Children with contractility disorders and decreased LVEF more commonly had hypotension during their hospitalisation. Children with ventricular dysfunction required treatment at paediatric intensive care units more often.
Male sex and lower oxygen saturation were more often seen in children with pericardial effusion. Children with conjunctivitis, oral inflammation and diarrhoea had pericardial effusion less often.
4. Discussion
Several parallel definitions of MIS-C are used in the scientific literature [38,44,45]. In each of them, the diagnosis is based on clinical premises: fever, multiorgan damage including heart involvement, increased inflammatory markers and exclusion of other causes of the disease. Furthermore, they depend on epidemiological grounds, proven SARS-CoV-2 infection or contact with the virus preceding the disease. In our work, we adopted the WHO definition [38], which is the most rigorous one. Our study population did not differ significantly from those with MIS-C in previously published reports in terms of most common signs and symptoms as well as laboratory tests results [15,17,21,23,46].
The results of our study are in line with most of the previous findings and show that valvular insufficiency and myocardial dysfunction are the most common cardiological findings in children with MIS-C. The median LVEF in our study (55%) was comparable with the results presented in the meta-analysis of the studies concentrating on longitudinal cardiac outcomes in MIS-C (54%) [47]. IMV was slightly less common in our study (42.8% vs. 56.6%) and CAAs were definitively less common (10.5% vs. 23.7%) [47]. Such a discrepancy in the frequency of CAAs was noted before in our population [37] and may be explained by ethnic differences.
According to the previous reports, the most common cardiac abnormalities, which can be found in more than half of the patients with MIS-C, include features of acute myocardial injury in the form of mildly elevated cardiac troponins, significantly elevated BNP or NT-proBNP levels and echocardiographic features of myocardial contractility disorders, including reduced LVEF. Other possible cardiac disorders include acute valvular regurgitation, pericardial effusion, CAAs and disturbances in the electrophysiological function of the heart, such as arrhythmias, atrioventricular conduction disorders or changes in the ST segment and T wave [12,15,17,23,32,33,34,48,49]. The precise incidence of cardiac findings varies between previous reports and is hard to compare, as the authors used different, and sometimes not clearly specified definitions for cardiac parameters [15,17,23,46,49,50] or broad and unspecified study inclusion criteria [48]. More detailed cardiac characteristics come mostly from single-centre studies with relatively small study groups. To our knowledge, we present the largest cohort of patients with MIS-C characterised in terms of cardiac involvement so far.
Most of the studies presenting the acute phase of MIS-C concentrated on the values of LVEF at a single time point [15,17,32,46,49], while the studies with follow-ups presented the results from an interval of at least 2 weeks to a few months [30,47,51,52,53,54]. They all reported a significant improvement in children who had myocardial dysfunction. Our study supports these results. Within a median of five days, we found a significant reduction in the number of children with contraction abnormalities or decreased LVEF. Such a rapid improvement—within days—was described before by Belhadjer for a small group of very severely ill children hospitalised in intensive care units [14]. Due to having a broader group of MIS-C patients involved in the study, we could analyse the dynamics of LVEF changes among children who did not require intensive care. We observed that the real problem of left ventricular dysfunction in the acute phase of the disease might have been underestimated. This observation is in line with a previous report by Matsubara, who described the presence of cardiac strain abnormalities in children having normal LVEF [34]. In summary, acute heart failure observed in the course of MIS-C is transient, but the measurement of ventricular function in children with MIS-C should not rely on a single LVEF measure.
It has been already established that the picture of MIS-C depends on age, and older children have a higher risk for severe presentation [37,46,49]. In the context of cardiac involvement, Campanello showed that coronary artery involvement is more common in children aged less than 6 years while left ventricular dysfunction is more common in children aged at least 6 years of age [55]. Abrams also found that the risk for decreased cardiac function increased with each age group (0–5 vs. 5–12 vs. 12–18 years old) [49]. Our study is in line with these findings.
An increased hospitalisation incidence for patients with MIS-C followed the waves of COVID-19 in Poland [36,56]. The need for paediatric cardiologist evaluation exceeds the access in many Polish cities. Therefore, we looked for potential predictors of any echocardiographic findings and precise features, such as decreased LVEF, to facilitate decision making regarding which patient should be prioritised for paediatric cardiologist evaluation.
Previous studies revealed that increased concentrations of NT-proBNP correlated with worse left ventricular function and a higher risk of cardiogenic shock [49,57]. Raynor’s study showed that increased NT-proBNP correlated with the severity of left ventricular dysfunction and was a better marker than BNP [58]. On the other hand, Fridman found that higher troponin I, not NT-proBNP, was associated with decreased LVEF [59]. Campanello reported that fibrinogen concentration was increased in children with reduced LVEF [55]. Our results support the usefulness of all these laboratory cardiac markers, i.e., troponin, BNP and NT-proBNP, as laboratory features more common in children with contractility abnormalities. However, in looking for markers of any echo abnormalities, only troponin was identified to significantly more often be elevated in children with any echo changes as compared with children with a normal echo picture. Neither BNP nor NT-proBNP differed between these groups. We did not find significant differences in fibrinogen concentration between children with and without impaired ventricular function. Another finding of our study was that abnormalities in the laboratory tests results, such as in complete blood count results, inflammatory marker panels and sodium concentration, were significantly more common. Most importantly, these significant findings were already present at the time of patient admission. The broad availability of these simple tests makes them a very promising tool for the screening of children who are at risk of acute heart failure in the course of MIS-C, but further studies are definitely needed to evaluate their robustness as predictors.
While cases of takotsubo syndrome (TTS) in adults with COVID-19 have been described [60,61], data on this subject in the paediatric population are very scarce. Most of the documented cases of TTS in the paediatric population have been related to emotional experiences, psychiatric disorders or the use of psychoactive substances [28,62]. Severe disease can also be a stress factor for the body, resulting in strong activation of the adrenergic system. In the largest analysis of TTS in children so far, which included 153 cases aged up to 20 years, 22.3% of TTS cases occurred in patients with sepsis [28]. The immunological disorders observed in the course of MIS-C can be described as a cytokine storm [24,26,63,64]. MIS-C has a rapid course, often leading to the exhaustion of the body’s compensatory mechanisms. Such a strong inflammatory reaction can be seen as a sufficient trigger for the occurrence of TTS. Belhadjer mentioned an echocardiographic image resembling TTS in a patient with acute heart failure in the course of MIS-C [14]; we have also described a similar case before [29]. In this analysis, we extracted the cases with a description of apex rounding or other segmental contractility abnormality. Overall, 31 children had echo pictures that might have resembled TTS during hospitalisation. Interestingly, there were more such cases identified in the follow-up than in the initial echo, suggesting that such presentation is relatively late. Further studies are necessary to establish the connection between MIS-C and TTS.
5. Limitations
The relatively low number of available electrocardiography descriptions and inconsistencies in their descriptions did not allow us to include ECG analyses in this report. Diastolic dysfunction and right ventricular dysfunction echo measures were not included for the same reason. However, diastolic function assessment in children might be unreliable due to volume status, valve competency impact and poor interobserver agreement.
The MIS-C case report form did not include information on the temporality of the signs and symptoms presented by the patients; therefore, it was not clear whether these findings preceded, coincided or followed the development of echocardiological outcomes of interest. Therefore, we cannot rule out the possibility that these signs and symptoms may be markers of MIS-C, and not necessarily predictors of echo findings signalling potential cardiac dysfunction.
Our study also lacks records of long-term outcomes, and so we were not able to correlate our findings with specific clinical prognoses. However, this study was intended as exploratory research conducted to discover potential clinical markers, features or risk factors associated with MIS-C, to be later correlated with specific outcomes of interest. The strength of the study lies in the size of the cohort, as well as the depth of clinical variables, patient signs and symptoms investigated, especially in relation to echocardiological features for cardiac involvement.
6. Conclusions
Almost all children in our population had laboratory or echocardiographic features of cardiovascular involvement in the course of MIS-C. The incidence of left ventricular dysfunction might be underestimated if the assessment relies only on a single measurement of LVEF. The majority of children with acute heart failure improved significantly within a few days. Coronary artery abnormality was a relatively rare finding. We found simple clinical features were present more commonly in children with an impaired contractility as well as other cardiac findings that might facilitate decision making to assess the need for specialist paediatric cardiologist consultation. Due to the exploratory nature of this study, these findings should be confirmed in further association studies.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/biomedicines11051251/s1.
Author Contributions
Conceptualization, K.M.L., L.S. and M.S.; methodology, K.M.L., N.M. and M.S.; software, K.M.L. and N.M.; validation, K.M.L., N.M. and P.T.; formal analysis, N.M. and K.M.L.; investigation, K.M.L., P.T. and L.S.; resources, K.M.L., N.M., P.T. and L.S.; data curation, N.M.; writing—original draft preparation, K.M.L. and N.M.; writing—review and editing, L.S. and M.S.; visualization, K.M.L. and N.M.; supervision, L.S. and M.S.; project administration, K.M.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Bioethics Committee at Wroclaw Medical University (CWN UMW BW: 313/2020).
Informed Consent Statement
Waiver of informed consent was obtained from the Bioethics Committee at Wroclaw Medical University with only deidentified data transmitted and analysed.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, K.M.L., upon reasonable request.
Acknowledgments
We thank all the paediatricians who contributed to our work by reporting patients to the MOIS CoR study, including Barszcz Marta (Department of Pediatric Infectious Diseases, Medical University of Białystok, Waszyngtona 17, 15-274 Białystok, Poland), Berdej-Szczot Elżbieta (Department of Paediatrics and Paediatric Endocrinology, Upper-Silesian Paediatric Health Center School of Medicine in Katowice, Medical University of Silesia, Katowice, Poland), Brzuszkiewicz Sebastian (Provincial Specialist Children’s Hospital prof. S. Popowski in Olsztyn ul. Żołnierska 18a 10-651 Olsztyn, Poland), Buda Piotr (Department of Pediatrics, Nutrition and Metabolic Diseases, The Children’s Memorial Health Institute, Al. Dzieci Polskich 20, 04-730 Warsaw, Poland), Czajka Alicja (Department of Pediatrics, Children’s Hospital, ul. Niekłańska 4/24, 03-924 Warsaw, Poland), Czech Agnieszka (Department of Pediatric Infectious Diseases, Wroclaw Medical University, Chałubińskiego 2-2a, 50-368 Wroclaw, Poland), Chruszcz Joanna, Czerwińska Ewa (Department of Pediatric Infectious Diseases, Wroclaw Medical University, Chałubińskiego 2-2a, 50-368 Wroclaw, Poland), Figlerowicz Magdalena (Department of Infectious Diseases and Child Neurology, Poznan University of Medical Science, Szpitalna 27/33, 60-572 Poznan, Poland), Firek-Pędras Małgorzata (Department of Paediatrics and Paediatric Endocrinology, Upper-Silesian Paediatric Health Center School of Medicine in Katowice, Medical University of Silesia, Katowice, Poland), Gawlik Aneta (Department of Paediatrics and Paediatric Endocrinology, Upper-Silesian Paediatric Health Center School of Medicine in Katowice, Medical University of Silesia, Katowice, Poland), Gowin Ewelina (Poznan University of Medical Science, Smoluchowskiego 11, 60-179 Poznań, Poland), Izdebska Olga (Clinical Department of Paediatrics and Nephrology, Voivodeship Complex Hospital L. Rydygiera in Toruń, ul. św. Józefa 53-59, 87-100 Toruń, Poland), Jackowska Teresa (Department of Pediatrics, The Medical Centre of Postgraduate Education, Cegłowska 80, 01-809 Warsaw, Poland), Januszkiewicz-Lewandowska Danuta (Department of Pediatric Oncology, Hematology and Transplantation, Poznan University of Medical Sciences, Szpitalna 27/33, 60-572 Poznan, Poland), Kiepuszka Justyna (Specialist Hospital F. Ceynowy, ul. dr. A. Jagalskiego 10, 84-200 Wejherowo, Poland), Koczwara Agnieszka (Department of Pediatrics and Rheumatology, Specialist Hospital Antoniego Falkiewicza, Warszawska 2, 52-114 Wroclaw, Poland), Koszałko Danuta (Independent Public Health Care, ul. Sukiennicza 13, 64-500 Szamotuły, Poland), Kośmider-Żurawska Magdalena (Department of Anaesthesiology and Intensive Therapy, Wroclaw Medical University, ul. Borowska 213, 50-556 Wrocław, Poland), Książyk Janusz (Department of Pediatrics, Nutrition and Metabolic Diseases, The Children’s Memorial Health Institute, Al. Dzieci Polskich 20, 04-730 Warsaw, Poland), Kucińska Beata (Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Żwirki i Wigury 61, 02-091 Warsaw, Poland), Kukawska Martyna (Clinical Department of Pediatrics, Mazowiecki Specialist Hospital ul. Aleksandrowicza 5, Radom, Poland), Kwinta Przemko (Department of Paediatrics, Jagiellonian University Medical College, Wielicka 265, 30-663 Krakow, Poland), Lackowska Anita (Children’s Hospital “Polanki” Polanki 119, 80-308 Gdańsk, Poland), Łapacz Katarzyna (Department of Pediatrics, Children’s Hospital, ul. Niekłańska 4/24, 03-924 Warsaw, Poland), Maliszak Agnieszka (Pediatric Ward, Regional Specialist Hospital, ul. Iwaszkiewicza 5, 59-220 Legnica), Mania Anna (Department of Infectious Diseases and Child Neurology, Poznan University of Medical Science, Szpitalna 27/33, 60-572 Poznan, Poland), Mańdziuk Joanna (Department of Pediatrics with Clinical Assessment Unit, Medical University of Warsaw, Żwirki i Wigury 61, 02-091 Warsaw, Poland), Mazur Artur (Collegium Medicum University of Jan Kochanowski, ul. Grunwaldzka 45, 25-736 Kielce, Poland), Mazur-Melewska Katarzyna (Department of Infectious Diseases and Child Neurology, Poznan University of Medical Science, Szpitalna 27/33, 60-572 Poznan, Poland), Niszczota Cezary (Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Żwirki i Wigury 61, 02-091 Warsaw, Poland), Opalińska-Zielonka Paulina (Department of Pediatrics, Pediatric Endocrinology and Diabetes, University of Rzeszow, Lwowska 60, 35-301 Rzeszow, Poland), Pałyga-Bysiecka Ilona (Collegium Medicum University of Jan Kochanowski, ul. Grunwaldzka 45, 25-736 Kielce, Poland), Rojewska Katarzyna (Specialist Hospital F. Ceynowy, ul. dr. A. Jagalskiego 10, 84-200 Wejherowo, Poland), Rożnowska-Wójtowicz Anna (Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Żwirki i Wigury 61, 02-091 Warsaw, Poland), Siewert Bartosz (Department of Preventive Health, Poznan University of Medical Science, Smoluchowskiego 11, 60-179 Poznan, Poland), Sobiczewska Paulina (Multidiscyplinary Hospital in Nowa Sól, ul. Chałubińskiego 1, 67-100 Nowa Sól, Poland), Stopyra Lidia (Department of Infectious Diseases and Paediatrics, S. Zeromski Hospital in Krakow, Osiedle Na Skarpie 66, 31-913 Krakow, Poland), Stroba-Żelek Agnieszka (Pediatric Ward, City Hospital in Ruda Śląska, Medical University of Silesia, Chair and Department of Environmental Medicine and Epidemiology, ul. Wincentego Lipa 2, 41-703 Ruda Śląska, Poland), Stryczyńska-Kazubska Joanna (Department of Preventive Health, Poznan University of Medical Science, Smoluchowskiego 11, 60-179 Poznan, Poland), Sulik Artur (Department of Pediatric Infectious Diseases, Medical University of Bialystok, Waszyngtona 17, 15-274 Bialystok, Poland), Szatkowski Tomasz, Szczepańska Barbara, Szczukocki Maciej (Collegium Medicum University of Jan Kochanowski, ul. Grunwaldzka 45, 25-736 Kielce, Poland), Szylo Robert (Pediatric Ward, City Hospital in Ruda Śląska, Medical University of Silesia, Chair and Department of Environmental Medicine and Epidemiology, ul. Wincentego Lipa 2, 41-703 Ruda Śląska, Poland), Tyc Filip (Congenital Heart Disease and Pediatric Cardiology Department, Silesian Center for Heart Diseases in Zabrze, ul. Marii Curie Skłodowskiej 9, 41-800 Zabrze, Poland), Bożena Werner (Department of Pediatric Cardiology and General Pediatrics, Medical University of Warsaw, Żwirki i Wigury 61, 02-091 Warsaw, Poland), Wielgos Katarzyna (Department of Paediatrics, J. Gromkowski Regional Specialist Hospital in Wroclaw, Koszarowa 5, 51-149 Wrocław, Poland), Wołowska Ewa (Children’s Hospital “Polanki” Polanki 119, 80-308 Gdańsk, Poland), Wysocki Jacek (Department of Preventive Health, Poznan University of Medical Science, Smoluchowskiego 11, 60-179 Poznan, Poland; 2nd Infectious Diseases Ward, Children’s Hospital in Poznan, Nowowiejskiego 56/58, 61-734 Poznan, Poland), Zacharzewska Anna (University Clinical Center: Central Teaching Clinical Hospital, ul. Banacha 1A, 02-097 Warszawa, Poland), Zaniew Marcin (Department of Pediatrics, University of Zielona Góra, Zielona Góra, Poland), Zielińska Marzena (Department of Anaesthesiology and Intensive Therapy, Wroclaw Medical University, ul. Borowska 213, 50-556 Wrocław, Poland), Zięba-Glonek Katarzyna (District Hospital of the name of Doctor T. Chalubinski in Zakopane, ul. Kamieniec 10, Zakopane, Poland), and many more. We especially thank Ernest Kuchar, Magdalena Okarska-Napierała, Natalia Dudek (Department of Pediatric Infectious Diseases, Medical University of Bialystok, Waszyngtona 17, 15-274 Bialystok, Poland) and Miron Kursa, Marta Hallay-Suszek and Catherine Suski-Grabowski (Interdisciplinary Centre for Mathematical and Computational Modelling, University of Warsaw, Pawinskiego 5A, 02-106, Warsaw, Poland) for their contribution to building the database.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wu, L.; O’Kane, A.M.; Peng, H.; Bi, Y.; Motriuk-Smith, D.; Ren, J. SARS-CoV-2 and cardiovascular complications: From molecular mechanisms to pharmaceutical management. Biochem. Pharmacol. 2020, 178, 114114. [Google Scholar] [CrossRef]
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; The Northwell COVID-19 Research Consortium. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA 2020, 323, 2052. [Google Scholar] [CrossRef]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol. 2020, 5, 831–840. [Google Scholar] [CrossRef]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury with Mortality in Hospitalized Patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular Implications of Fatal Outcomes of Patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef]
- Xu, Z.; Shi, L.; Wang, Y.; Zhang, J.; Huang, L.; Zhang, C.; Liu, S.; Zhao, P.; Liu, H.; Zhu, L.; et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir. Med. 2020, 8, 420–422. [Google Scholar] [CrossRef] [PubMed]
- Lindner, D.; Fitzek, A.; Bräuninger, H.; Aleshcheva, G.; Edler, C.; Meissner, K.; Scherschel, K.; Kirchhof, P.; Escher, F.; Schultheiss, H.-P.; et al. Association of Cardiac Infection with SARS-CoV-2 in Confirmed COVID-19 Autopsy Cases. JAMA Cardiol. 2020, 5, 1281–1285. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhou, Y.; Wang, D.W. SARS-CoV-2: A potential novel etiology of fulminant myocarditis. Herz 2020, 45, 230–232. [Google Scholar] [CrossRef] [PubMed]
- Inciardi, R.M.; Lupi, L.; Zaccone, G.; Italia, L.; Raffo, M.; Tomasoni, D.; Cani, D.S.; Cerini, M.; Farina, D.; Gavazzi, E.; et al. Cardiac Involvement in a Patient with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 819–824. [Google Scholar] [CrossRef]
- Sokolski, M.; Sokolska, J.M.; Zymliński, R.; Biegus, J.; Banasiak, W.; Reczuch, K.; Ponikowski, P. Cardiac emergencies during the coronavirus disease 2019 pandemic in the light of the current evidence. Kardiol. Pol. (Pol. Heart J.) 2020, 78, 818–824. [Google Scholar] [CrossRef]
- Sokolski, M.; Trenson, S.; Sokolska, J.M.; D’Amario, D.; Meyer, P.; Poku, N.K.; Biering-Sørensen, T.; Lassen, M.C.H.; Skaarup, K.G.; Barge-Caballero, E.; et al. Heart failure in COVID-19: The multicentre, multinational PCHF-COVICAV registry. ESC Heart Fail. 2021, 17, 45. [Google Scholar] [CrossRef]
- Alsaied, T.; Tremoulet, A.H.; Burns, J.C.; Saidi, A.; Dionne, A.; Lang, S.M.; Newburger, J.W.; De Ferranti, S.; Friedman, K.G. Review of Cardiac Involvement in Multisystem Inflammatory Syndrome in Children. Circulation 2021, 143, 78–88. [Google Scholar] [CrossRef] [PubMed]
- McMurray, J.C.; May, J.W.; Cunningham, M.W.; Jones, O.Y. Multisystem Inflammatory Syndrome in Children (MIS-C), a Post-viral Myocarditis and Systemic Vasculitis—A Critical Review of Its Pathogenesis and Treatment. Front. Pediatr. 2020, 8, 626182. [Google Scholar] [CrossRef]
- Belhadjer, Z.; Méot, M.; Bajolle, F.; Khraiche, D.; Legendre, A.; Abakka, S.; Auriau, J.; Grimaud, M.; Oualha, M.; Beghetti, M.; et al. Acute heart failure in multisystem inflammatory syndrome in children (MIS-C) in the context of global SARS-CoV-2 pandemic. Circulation 2020, 142, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, E.; Bamford, A.; Kenny, J.; Kaforou, M.; Jones, C.; Shah, P.; Ramnarayan, P.; Fraisse, A.; Miller, O.; Davies, P.; et al. Clinical Characteristics of 58 Children with a Pediatric Inflammatory Multisystem Syndrome Temporally Associated with SARS-CoV-2. JAMA 2020, 324, 259–269. [Google Scholar] [CrossRef]
- Verdoni, L.; Mazza, A.; Gervasoni, A.; Martelli, L.; Ruggeri, M.; Ciuffreda, M.; Bonanomi, E.; D’Antiga, L. An outbreak of severe Kawasaki-like disease at the Italian epicentre of the SARS-CoV-2 epidemic: An observational cohort study. Lancet 2020, 395, 1771–1778. [Google Scholar] [CrossRef] [PubMed]
- Feldstein, L.R.; Rose, E.B.; Horwitz, S.M.; Collins, J.P.; Newhams, M.M.; Son, M.B.F.; Newburger, J.W.; Kleinman, L.C.; Heidemann, S.M.; Martin, A.A.; et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N. Engl. J. Med. 2020, 383, 334–346. [Google Scholar] [CrossRef]
- Sokolovsky, S.; Soni, P.; Hoffman, T.; Kahn, P.; Scheers-Masters, J. COVID-19 associated Kawasaki-like multisystem inflammatory disease in an adult. Am. J. Emerg. Med. 2021, 39, 253.e1–253.e2. [Google Scholar] [CrossRef]
- Kofman, A.D.; Sizemore, E.K.; Detelich, J.F.; Albrecht, B.; Piantadosi, A.L. A young adult with COVID-19 and multisystem inflammatory syndrome in children (MIS-C)-like illness: A case report. BMC Infect. Dis. 2020, 20, 716. [Google Scholar] [CrossRef] [PubMed]
- Morris, S.B.; Schwartz, N.G.; Patel, P.; Abbo, L.; Beauchamps, L.; Balan, S.; Lee, E.H.; Paneth-Pollak, R.; Geevarughese, A.; Lash, M.K.; et al. Case Series of Multisystem Inflammatory Syndrome in Adults Associated with SARS-CoV-2 Infection—United Kingdom and United States, March–August 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1450–1456. [Google Scholar] [CrossRef]
- Payne, A.B.; Gilani, Z.; Godfred-Cato, S.; Belay, E.D.; Feldstein, L.R.; Patel, M.M.; Randolph, A.G.; Newhams, M.; Thomas, D.; Magleby, R.; et al. Incidence of Multisystem Inflammatory Syndrome in Children among US Persons Infected with SARS-CoV-2. JAMA Netw. Open 2021, 4, e2116420. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Okarska-Napierała, M.; Buddingh, E.P.; Bloomfield, M.; Sediva, A.; Bautista-Rodriguez, C.; Brough, H.A.; Eigenmann, P.A.; Eiwegger, T.; Eljaszewicz, A.; et al. Pathogenesis, immunology, and immune-targeted management of the multisystem inflammatory syndrome in children (MIS-C) or pediatric inflammatory multisystem syndrome (PIMS): EAACI Position Paper. Pediatr. Allergy Immunol. 2023, 34, e13900. [Google Scholar] [CrossRef]
- Belot, A.; Antona, D.; Renolleau, S.; Javouhey, E.; Hentgen, V.; Angoulvant, F.; Delacourt, C.; Iriart, X.; Ovaert, C.; Bader-Meunier, B.; et al. SARS-CoV-2-related paediatric inflammatory multisystem syndrome, an epidemiological study, France, 1 March to 17 May 2020. Eurosurveillance 2020, 25, 2001010. [Google Scholar] [CrossRef] [PubMed]
- Loomba, R.S.; Villarreal, E.G.; Flores, S. COVID-19 and Hyperinflammatory Syndrome in Children: Kawasaki Disease with Macrophage Activation Syndrome in Disguise? Cureus 2020, 12, e9515. [Google Scholar] [CrossRef] [PubMed]
- Buonsenso, D.; Riitano, F.; Valentini, P. Pediatric Inflammatory Multisystem Syndrome Temporally Related with SARS-CoV-2: Immunological Similarities with Acute Rheumatic Fever and Toxic Shock Syndrome. Front. Pediatr. 2020, 8, 574. [Google Scholar] [CrossRef] [PubMed]
- Gruber, C.N.; Patel, R.S.; Trachtman, R.; Lepow, L.; Amanat, F.; Krammer, F.; Wilson, K.M.; Onel, K.; Geanon, D.; Tuballes, K.; et al. Mapping Systemic Inflammation and Antibody Responses in Multisystem Inflammatory Syndrome in Children (MIS-C). Cell 2020, 183, 982–995.e14. [Google Scholar] [CrossRef]
- ESC. Takotsubo Cardiomyopathy. Available online: https://www.escardio.org/Journals/E-Journal-of-Cardiology-Practice/Volume-8/Takotsubo-cardiomyopathy (accessed on 10 February 2021).
- Sendi, P.; Martinez, P.; Chegondi, M.; Totapally, B.R. Takotsubo cardiomyopathy in children. Cardiol. Young 2020, 30, 1711–1715. [Google Scholar] [CrossRef]
- Ludwikowska, K.M.; Tracewski, P.; Kusa, J. Takotsubo syndrome as a cardiac manifestation of multisystem inflammatory syndrome in children. Cardiol. Young 2022, 32, 1341–1343. [Google Scholar] [CrossRef]
- Patel, T.; Kelleman, M.; West, Z.; Peter, A.; Dove, M.; Butto, A.; Oster, M.E. Comparison of Multisystem Inflammatory Syndrome in Children—Related Myocarditis, Classic Viral Myocarditis, and COVID-19 Vaccine-Related Myocarditis in Children. J. Am. Heart Assoc. 2022, 11, e024393. [Google Scholar] [CrossRef]
- Blondiaux, E.; Parisot, P.; Redheuil, A.; Tzaroukian, L.; Levy, Y.; Sileo, C.; Schnuriger, A.; Lorrot, M.; Guedj, R.; Le Pointe, H.D. Cardiac MRI in children with multisystem inflammatory syndrome associated with COVID-19. Radiology 2020, 297, E283–E288. [Google Scholar] [CrossRef]
- Karabulut, M.; Aktas, D.; Yasar, B.; Petmezci, E.; Karabulut, N.D. Cardiac Evaluation in Children with Multisystem Inflammatory Syndrome Associated with SARS-CoV-2. Med. Bull. Sisli Etfal Hosp. 2022, 56, 461. [Google Scholar] [CrossRef]
- Mannarino, S.; Raso, I.; Garbin, M.; Ghidoni, E.; Corti, C.; Goletto, S.; Nespoli, L.; Santacesaria, S.; Zoia, E.; Camporesi, A.; et al. Cardiac dysfunction in Multisystem Inflammatory Syndrome in Children: An Italian single-center study. Ital. J. Pediatr. 2022, 48, 25. [Google Scholar] [CrossRef] [PubMed]
- Matsubara, D.; Kauffman, H.L.; Wang, Y.; Calderon-Anyosa, R.; Nadaraj, S.; Elias, M.D.; White, T.J.; Torowicz, D.L.; Yubbu, P.; Giglia, T.M.; et al. Echocardiographic Findings in Pediatric Multisystem Inflammatory Syndrome Associated with COVID-19 in the United States. J. Am. Coll. Cardiol. 2020, 76, 1947. [Google Scholar] [CrossRef]
- Niaz, T.; Hope, K.; Fremed, M.; Misra, N.; Altman, C.; Glickstein, J.; Sanchez-De-Toledo, J.; Fraisse, A.; Miller, J.; Snyder, C.; et al. Role of a Pediatric Cardiologist in the COVID-19 Pandemic. Pediatr. Cardiol. 2020, 1, 1. [Google Scholar] [CrossRef]
- MOIS CoR. Rejestr PIMS » Strona Głowna. Available online: https://pimsudzieci.pl/ (accessed on 1 February 2022).
- Ludwikowska, K.M.; Okarska-Napierała, M.; Dudek, N.; Tracewski, P.; Kusa, J.; Piwoński, K.P.; Afelt, A.; Cysewski, D.; Biela, M.; Werner, B.; et al. Distinct characteristics of multisystem inflammatory syndrome in children in Poland. Sci. Rep. 2021, 11, 23562. [Google Scholar] [CrossRef] [PubMed]
- WHO. Multisystem Inflammatory Syndrome in Children and Adolescents Temporally Related to COVID-19. Available online: https://www.who.int/news-room/commentaries/detail/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (accessed on 22 September 2021).
- NIL—Informacje Statystyczne. Available online: https://nil.org.pl/rejestry/centralny-rejestr-lekarzy/informacje-statystyczne (accessed on 13 February 2023).
- WHO. Body Mass Index-for-Age (BMI-for-Age). Available online: https://www.who.int/toolkits/child-growth-standards/standards/body-mass-index-for-age-bmi-for-age (accessed on 15 February 2023).
- Kułaga, Z.; Litwin, M.; Tkaczyk, M.; Palczewska, I.; Zajączkowska, M.; Zwolińska, D.; Krynicki, T.; Wasilewska, A.; Moczulska, A.; Morawiec-Knysak, A.; et al. Polish 2010 growth references for school-aged children and adolescents. Eur. J. Pediatr. 2011, 170, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Dallaire, F.; Dahdah, N. New equations and a critical appraisal of coronary artery Z scores in healthy children. J. Am. Soc. Echocardiogr. 2011, 24, 60–74. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Rowley, A.H.; Newburger, J.W.; Burns, J.C.; Bolger, A.F.; Gewitz, M.; Baker, A.L.; Jackson, M.A.; Takahashi, M.; Shah, P.B.; et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A scientific statement for health professionals from the American Heart Association. Circulation 2017, 135, e927–e999. [Google Scholar] [CrossRef]
- CDC. Multisystem Inflammatory Syndrome in Children (MIS-C)|CDC. Available online: https://www.cdc.gov/mis-c/ (accessed on 10 February 2021).
- Royal College of Paediatrics and Child Health. Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19 (PIMS)—Guidance for Clinicians|RCPCH. Available online: https://www.rcpch.ac.uk/resources/paediatric-multisystem-inflammatory-syndrome-temporally-associated-covid-19-pims-guidance (accessed on 4 November 2022).
- Godfred-Cato, S.; Bryant, B.; Leung, J.; Oster, M.E.; Conklin, L.; Abrams, J.; Roguski, K.; Wallace, B.; Prezzato, E.; Koumans, E.H.; et al. COVID-19–Associated Multisystem Inflammatory Syndrome in Children—United States, March–July 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1074–1080. [Google Scholar] [CrossRef]
- Yasuhara, J.; Masuda, K.; Watanabe, K.; Shirasu, T.; Takagi, H.; Sumitomo, N.; Lee, S.; Kuno, T. Longitudinal Cardiac Outcomes of Multisystem Inflammatory Syndrome in Children: A Systematic Review and Meta-Analysis. Pediatr. Cardiol. 2023, 44, 892–907. [Google Scholar] [CrossRef]
- Valverde, I.; Singh, Y.; Sanchez-De-Toledo, J.; Theocharis, P.; Chikermane, A.; Di Filippo, S.; Kuciñska, B.; Mannarino, S.; Tamariz-Martel, A.; Gutierrez-Larraya, F.; et al. Acute Cardiovascular Manifestations in 286 Children with Multisystem Inflammatory Syndrome Associated with COVID-19 Infection in Europe. Circulation 2021, 143, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.Y.; Oster, M.E.; Godfred-Cato, S.E.; Bryant, B.; Datta, S.D.; Campbell, A.P.; Leung, J.W.; Tsang, C.A.; Pierce, T.J.; Kennedy, J.L.; et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: A retrospective surveillance study. Lancet Child Adolesc. Health 2021, 5, 323. [Google Scholar] [CrossRef] [PubMed]
- Davies, P.; Evans, C.; Kanthimathinathan, H.K.; Lillie, J.; Brierley, J.; Waters, G.; Johnson, M.; Griffiths, B.; du Pré, P.; Mohammad, Z.; et al. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) in the UK: A multicentre observational study. Lancet Child Adolesc. Health 2020, 4, 669–677. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, A.; Philip, R.; Santoso, M.; Naik, R.; Merlocco, A.; Johnson, J.N. Cardiovascular Magnetic Resonance in Children with Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19: Institutional Protocol-Based Medium-Term Follow-up Study. Pediatr. Cardiol. 2022, 43, 1879–1887. [Google Scholar] [CrossRef] [PubMed]
- Dove, M.L.; Oster, M.E.; Hashemi, S.; Slesnick, T.C. Cardiac Magnetic Resonance Findings after Multisystem Inflammatory Syndrome in Children. J. Pediatr. 2022, 245, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, K.M.; Chan, A.; Weller, R.J.; Mi, J.; Jiang, P.; Abrahams, E.; Ferris, A.; Krishnan, U.S.; Pasumarti, N.; Suh, S.; et al. Longitudinal outcomes for multisystem inflammatory syndrome in children. Pediatrics 2021, 148, e2021051155. [Google Scholar] [CrossRef] [PubMed]
- Capone, C.A.; Misra, N.; Ganigara, M.; Epstein, S.; Rajan, S.; Acharya, S.S.; Hayes, D.A.; Kearney, M.B.; Romano, A.; Friedman, R.A.; et al. Six Month Follow-Up of Patients with Multi-System Inflammatory Syndrome in Children. Pediatrics 2021, 148, e2021050973. [Google Scholar] [CrossRef]
- Campanello, C.; Mercuri, C.; Derchi, M.; Trocchio, G.; Consolaro, A.; Caorsi, R.; Ravelli, A.; Rimini, A.; Marasini, M.; Gattorno, M. Cardiovascular Manifestations in Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with COVID-19 According to Age. Children 2022, 9, 583. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC COVID Data Tracker: Multisystem Inflammatory Syndrome in Children (MIS-C). Available online: https://covid.cdc.gov/covid-data-tracker/#mis-national-surveillance (accessed on 4 November 2022).
- Tibi, R.; Hadash, A.; Khoury, A.; Butbul-Aviel, Y.; Ben-Ari, J.; Shavit, I. Emergency department levels of NT-proBNP and inotropic/vasoactive support in multi-inflammatory syndrome in children (MIS-C). Am. J. Emerg Med. 2022, 56, 296. [Google Scholar] [CrossRef]
- Raynor, A.; Vallée, C.; Belkarfa, A.-L.; Lunte, K.; Laney, M.; Belhadjer, Z.; Vicca, S.; Boutten, A.; Bonnet, D.; Nivet-Antoine, V. Multisystem inflammatory syndrome in children: Inputs of BNP, NT-proBNP and Galectin-3. Clin. Chim. Acta 2022, 529, 109–113. [Google Scholar] [CrossRef] [PubMed]
- Fridman, M.D.; Tsoukas, P.; Jeewa, A.; Yeung, R.S.M.; Gamulka, B.D.; McCrindle, B.W. Differentiation of COVID-19–Associated Multisystem Inflammatory Syndrome from Kawasaki Disease with the Use of Cardiac Biomarkers. Can. J. Cardiol. 2022, 1, S0828-282X(22)01049-2. [Google Scholar] [CrossRef] [PubMed]
- Giustino, G.; Croft, L.B.; Oates, C.P.; Rahman, K.; Lerakis, S.; Reddy, V.Y.; Goldman, M. Takotsubo Cardiomyopathy in COVID-19. J. Am. Coll. Cardiol. 2020, 76, 628–629. [Google Scholar] [CrossRef] [PubMed]
- Roca, E.; Lombardi, C.; Campana, M.; Vivaldi, O.; Bigni, B.; Bertozzi, B.; Passalacqua, G. Takotsubo Syndrome Associated with COVID-19. Eur. J. Case Rep. Intern. Med. 2020, 7, 1. [Google Scholar] [CrossRef] [PubMed]
- Topal, Y.; Topal, H.; Doğan, C.; Tiryaki, S.B.; Biteker, M. Takotsubo (stress) cardiomyopathy in childhood. Eur. J. Pediatr. 2020, 179, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Consiglio, C.R.; Cotugno, N.; Sardh, F.; Pou, C.; Amodio, D.; Rodriguez, L.; Tan, Z.; Zicari, S.; Ruggiero, A.; Pascucci, G.R.; et al. The Immunology of Multisystem Inflammatory Syndrome in Children with COVID-19 Equal Contribution; Cold Spring Harbor Laboratory Press: Cold Spring Harbor, NY, USA, 2020. [Google Scholar] [CrossRef]
- Brodin, P. Immune determinants of COVID-19 disease presentation and severity. Nat. Med. 2021, 27, 28–33. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).