
Association of Moderate-to-Vigorous Physical Activity, Sedentary Time, Fat Percentage, and Physical Fitness with Gait Parameters in Women with Fibromyalgia: The Al-Ándalus Project
 , ,
, ,  , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
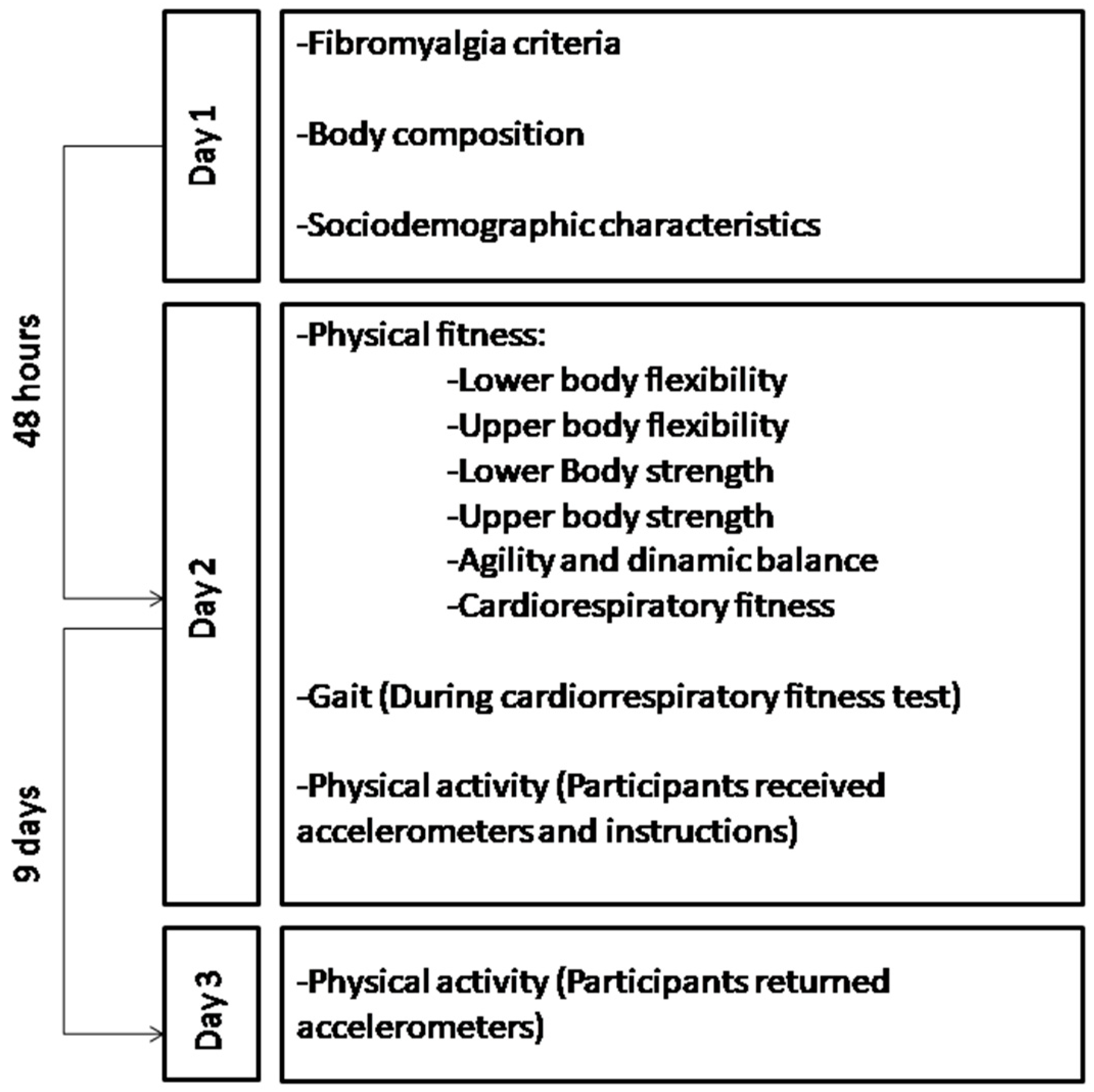
2.1. Study Design and Participants
2.2. Procedures
2.3. Measurements
2.3.1. Sociodemographic Characteristics
2.3.2. Inclusion and Exclusion Criteria Measurements
2.3.3. Physical Activity and Sedentary Time
2.3.4. Body Composition
2.3.5. Physical Fitness
2.3.6. Gait Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walitt, B.; Nahin, R.L.; Katz, R.S.; Bergman, M.J.; Wolfe, F. The prevalence and characteristics of fibromyalgia in the 2012 national health interview survey. PLoS ONE 2015, 10, e0138024. [Google Scholar] [CrossRef] [PubMed]
- Cabo-Meseguer, A.; Cerdá-Olmedo, G.; Trillo-Mata, L. Fibromialgia: Prevalencia, perfiles epidemiológicos y costes económicos. Med. Clin. 2017, 149, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Estévez-López, F.; Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Borges-Cosic, M.; Pulido-Martos, M.; Carbonell-Baeza, A.; Aparicio, V.A.; Geenen, R.; Delgado-Fernández, M. Adaptation profiles comprising objective and subjective measures in fibromyalgia: The al-Ándalus project. Rheumatology 2017, 56, 2015–2024. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Carrasco-Vega, E.; Ruiz-Muñoz, M.; Cuesta-Vargas, A.; Romero-Galisteo, R.P.; González-Sánchez, M. Individuals with fibromyalgia have a different gait pattern and a reduced walk functional capacity: A systematic review with meta-analysis. PeerJ 2022, 10, e12908. [Google Scholar] [CrossRef] [PubMed]
- Middleton, A.; Fritz, S.L.; Lusardi, M. Walking speed: The functional vital sign. J. Aging Phys. Act. 2015, 23, 314–322. [Google Scholar] [CrossRef] [PubMed]
- Pamoukdjian, F.; Paillaud, E.; Zelek, L.; Laurent, M.; Lévy, V.; Landre, T.; Sebbane, G. Measurement of gait speed in older adults to identify complications associated with frailty: A systematic review. J. Geriatr. Oncol. 2015, 6, 484–496. [Google Scholar] [CrossRef] [PubMed]
- Lamb, S.E.; Keene, D.J. Measuring physical capacity and performance in older people. Best Pract. Res. Clin. Rheumatol. 2017, 31, 243–254. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Sarquis-Adamson, Y.; Song, H.Y.; Bray, N.W.; Pieruccini-Faria, F.; Speechley, M. Polypharmacy, Gait Performance, and Falls in Community-Dwelling Older Adults. Results from the Gait and Brain Study. J. Am. Geriatr. Soc. 2019, 67, 1182–1188. [Google Scholar] [CrossRef]
- Kamide, N.; Sato, H.; Sakamoto, M.; Shiba, Y. The effect of the interaction between fall-related self-efficacy and gait function on the occurrence of falls in community-dwelling older people. Aging Clin. Exp. Res. 2021, 33, 2715–2722. [Google Scholar] [CrossRef]
- Abe, T.; Kitamura, A.; Taniguchi, Y.; Amano, H.; Seino, S.; Yokoyama, Y.; Nishi, M.; Narita, M.; Ikeuchi, T.; Fujiwara, Y.; et al. Pathway from gait speed to incidence of disability and mortality in older adults: A mediating role of physical activity. Maturitas 2019, 123, 32–36. [Google Scholar] [CrossRef]
- Scaturro, D.; Rizzo, S.; Sanfilippo, V.; Giustino, V.; Messina, G.; Martines, F.; Falco, V.; Cuntrera, D.; Moretti, A.; Iolascon, G.; et al. Effectiveness of Rehabilitative Intervention on Pain, Postural Balance, and Quality of Life in Women with Multiple Vertebral Fragility Fractures: A Prospective Cohort Study. J. Funct. Morphol. Kinesiol. 2021, 6, 24. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Mitra, S.; Palmer, M.; Kim, H.; Mont, D.; Groce, N. Extra costs of living with a disability: A review and agenda for research. Disabil. Health J. 2017, 10, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Riebe, D.; Blissmer, B.J.; Greaney, M.L.; Ewing Garber, C.; Lees, F.D.; Clark, P.G. The Relationship Between Obesity, Physical Activity, and Physical Function in Older Adults. J. Aging Health 2009, 21, 1159–1178. [Google Scholar] [CrossRef] [PubMed]
- Hlebichuk, J.L.; Gretebeck, R.J.; Garnier-Villarreal, M.; Piacentine, L.B.; Singh, M.; Gretebeck, K.A. Physical Activity, Inflammation, and Physical Function in Older Adults: Results From the Health & Retirement Study. Biol. Res. Nurs. 2023, 25, 24–32. [Google Scholar] [CrossRef] [PubMed]
- Izawa, K.P.; Shibata, A.; Ishii, K.; Miyawaki, R.; Oka, K. Associations of low-intensity light physical activity with physical performance in community-dwelling elderly Japanese: A cross-sectional study. PLoS ONE 2017, 12, e0178654. [Google Scholar] [CrossRef] [PubMed]
- Latorre Román, P.A.; García-Pinillos, F.; Huertas Herrador, J.A.; Cózar Barba, M.; Muñoz Jiménez, M. Relationship between sex, body composition, gait speed and body satisfaction in elderly people. Nutr. Hosp. 2014, 30, 851–857. [Google Scholar]
- Heredia-Jimenez, J.; Latorre-Roman, P.; Santos-Campos, M.; Orantes-Gonzalez, E.; Soto-Hermoso, V.M. Spatio-temporal gait disorder and gait fatigue index in a six-minute walk test in women with fibromyalgia. Clin. Biomech. 2016, 33, 1–6. [Google Scholar] [CrossRef]
- Heredia-Jimenez, J.; Orantes-Gonzalez, E.; Soto-Hermoso, V.M. Variability of gait, bilateral coordination, and asymmetry in women with fibromyalgia. Gait Posture 2016, 45, 41–44. [Google Scholar] [CrossRef]
- Auvinet, B.; Chaleil, D.; Cabane, J.; Dumolard, A.; Hatron, P.; Juvin, R.; Lanteri-Minet, M.; Mainguy, Y.; Negre-Pages, L.; Pillard, F.; et al. The interest of gait markers in the identification of subgroups among fibromyalgia patients. BMC Musculoskelet. Disord. 2011, 12, 258. [Google Scholar] [CrossRef] [PubMed]
- Heredia Jiménez, J.M.; Aparicio García-Molina, V.A.; Porres Foulquie, J.M.; Delgado Fernández, M.; Soto Hermoso, V.M. Spatial-temporal parameters of gait in women with fibromyalgia. Clin. Rheumatol. 2009, 28, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Pierrynowski, M.R.; Tiidus, P.M.; Galea, V. Women with fibromyalgia walk with an altered muscle synergy. Gait Posture 2005, 22, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Góes, S.M.; Leite, N.; de Souza, R.M.; Homann, D.; Osiecki, A.C.V.; Stefanello, J.M.F.; Rodacki, A.L.F. Gait characteristics of women with fibromyalgia: A premature aging pattern. Rev. Bras. Reumatol. 2014, 54, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Segura-Jiménez, V.; Álvarez-Gallardo, I.C.; Estévez-López, F.; Soriano-Maldonado, A.; Delgado-Fernández, M.; Ortega, F.B.; Aparicio, V.A.; Carbonell-Baeza, A.; Mota, J.; Silva, P.; et al. Differences in sedentary time and physical activity between female patients with fibromyalgia and healthy controls: The al-Ándalus project. Arthritis Rheumatol. 2015, 67, 3047–3057. [Google Scholar] [CrossRef] [PubMed]
- Lobo, M.M.M.T.; dos Santos Paiva, E.; Andretta, A.; Schieferdecker, M.E.M. Body composition by dual-energy X-ray absorptiometry in women with fibromyalgia. Rev. Bras. Reumatol. 2014, 54, 273–278. [Google Scholar] [CrossRef][Green Version]
- Jones, C.J.; Rakovski, C.; Rutledge, D.; Gutierrez, A. A comparison of women with fibromyalgia syndrome to criterion fitness standards: A pilot study. J. Aging Phys. Act. 2015, 23, 103–111. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Soriano-Maldonado, A.; Estévez-López, F.; Álvarez-Gallardo, I.C.; Delgado-Fernández, M.; Ruiz, J.R.; Aparicio, V.A. Independent and joint associations of physical activity and fitness with fibromyalgia symptoms and severity: The al-Ándalus project. J. Sports Sci. 2017, 35, 1565–1574. [Google Scholar] [CrossRef]
- Segura-Jiménez, V.; Borges-Cosic, M.; Soriano-Maldonado, A.; Estévez-López, F.; Álvarez-Gallardo, I.C.; Herrador-Colmenero, M.; Delgado-Fernández, M.; Ruiz, J.R. Association of sedentary time and physical activity with pain, fatigue, and impact of fibromyalgia: The al-Ándalus study. Scand. J. Med. Sci. Sports 2017, 27, 83–92. [Google Scholar] [CrossRef]
- Soriano-Maldonado, A.; Ruiz, J.R.; Aparicio, V.A.; Estevez-Lopez, F.; Segura-Jimenez, V.; Alvarez-Gallardo, I.C.; Carbonell-Baeza, A.; Delgado-Fernandez, M.; Ortega, F.B. Association of Physical Fitness with Pain in Women with Fibromyalgia: The al-Andalus project. Pain Med. 2016, 17, 1542–1552. [Google Scholar] [CrossRef]
- Soriano-Maldonado, A.; Artero, E.G.; Segura-Jiménez, V.; Aparicio, V.A.; Estévez-López, F.; Álvarez-Gallardo, I.C.; Munguía-Izquierdo, D.; Casimiro-Andújar, A.J.; Delgado-Fernández, M.; Ortega, F.B. Association of physical fitness and fatness with cognitive function in women with fibromyalgia. J. Sports Sci. 2016, 34, 1731–1739. [Google Scholar] [CrossRef]
- Pau, M.; Leban, B.; Collu, G.; Migliaccio, G.M. Effect of light and vigorous physical activity on balance and gait of older adults. Arch. Gerontol. Geriatr. 2014, 59, 568–573. [Google Scholar] [CrossRef]
- Yasunaga, A.; Shibata, A.; Ishii, K.; Koohsari, M.J.; Inoue, S.; Sugiyama, T.; Owen, N.; Oka, K. Associations of sedentary behavior and physical activity with older adults’ physical function: An isotemporal substitution approach. BMC Geriatr. 2017, 17, 280. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Pinillos, F.; Cozar-Barba, M.; Munoz-Jimenez, M.; Soto-Hermoso, V.; Latorre-Roman, P. Gait speed in older people: An easy test for detecting cognitive impairment, functional independence, and health state. Psychogeriatrics 2016, 16, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Carbonell-Baeza, A.; Ruiz, J.R.; Aparicio, V.A.; Ortega, F.B.; Munguía-Izquierdo, D.; Alvarez-Gallardo, I.C.; Segura-Jiménez, V.; Camiletti-Moirón, D.; Romero, A.; Estévez-López, F.; et al. Land- and water-based exercise intervention in women with fibromyalgia: The al-Andalus physical activity randomised controlled trial. BMC Musculoskelet. Disord. 2012, 13, 18. [Google Scholar] [CrossRef]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.L.; Mease, P.J.; Russell, A.S.; Russell, I.J.; Walitt, B. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin. Arthritis Rheum. 2016, 46, 319–329. [Google Scholar] [CrossRef] [PubMed]
- Llamas-Velasco, S.; Llorente-Ayuso, L.; Contador, I.; Bermejo-Pareja, F. Versiones en español del MMSE y cuestiones para su uso clínico. Rev. Neurol. 2015, 61, 363–371. [Google Scholar] [PubMed]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nyström, C.; Mora-Gonzalez, J.; Löf, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer Data Collection and Processing Criteria to Assess Physical Activity and Other Outcomes: A Systematic Review and Practical Considerations. Sport. Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef] [PubMed]
- Choi, L.; Ward, S.C.; Schnelle, J.F.; Buchowski, M.S. Assessment of Wear/Nonwear Time Classification Algorithms for Triaxial Accelerometer. Med. Sci. Sports Exerc. 2012, 44, 2009–2016. [Google Scholar] [CrossRef]
- Sasaki, J.E.; John, D.; Freedson, P.S. Validation and comparison of ActiGraph activity monitors. J. Sci. Med. Sport 2011, 14, 411–416. [Google Scholar] [CrossRef]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.M.E.E.G. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Malavolti, M.; Mussi, C.; Poli, M.; Fantuzzi, A.L.; Salvioli, G.; Battistini, N.; Bedogni, G. Cross-calibration of eight-polar bioelectrical impedance analysis versus dual-energy X-ray absorptiometry for the assessment of total and appendicular body composition in healthy subjects aged 21–82 years. Ann. Hum. Biol. 2003, 30, 380–391. [Google Scholar] [CrossRef] [PubMed]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Carbonell-Baeza, A.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Castro-Piñero, J.; Ruiz, J.R.; Delgado-Fernández, M.; Aparicio, V.A. Reliability and feasibility of physical fitness tests in female fibromyalgia patients. Int. J. Sports Med. 2015, 36, 157–162. [Google Scholar] [CrossRef]
- Balsalobre-Fernández, C.; Tejero-González, C.M.; Del Campo-Vecino, J.; Bavaresco, N. The concurrent validity and reliability of a low-cost, high-speed camera-based method for measuring the flight time of vertical jumps. J. Strength Cond. Res. 2014, 28, 528–533. [Google Scholar] [CrossRef] [PubMed]
- Puig-Diví, A.; Escalona-Marfil, C.; Padullés-Riu, J.M.; Busquets, A.; Padullés-Chando, X.; Marcos-Ruiz, D. Validity and reliability of the Kinovea program in obtaining angles and distances using coordinates in 4 perspectives. PLoS ONE 2019, 14, e0216448. [Google Scholar] [CrossRef]
- Egerton, T.; Paterson, K.; Helbostad, J.L. The association between gait characteristics and ambulatory physical activity in older people: A cross-sectional and longitudinal observational study using generation 100 data. J. Aging Phys. Act. 2017, 25, 10–19. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Bellettiere, J.; Gardiner, P.A.; Villarreal, V.N.; Crist, K.; Kerr, J. Independent Associations between Sedentary Behaviors and Mental, Cognitive, Physical, and Functional Health among Older Adults in Retirement Communities. J. Gerontol.—Ser. A Biol. Sci. Med. Sci. 2015, 71, 78–83. [Google Scholar] [CrossRef]
- Spartano, N.L.; Lyass, A.; Larson, M.G.; Tran, T.; Andersson, C.; Blease, S.J.; Esliger, D.W.; Vasan, R.S.; Murabito, J.M. Objective physical activity and physical performance in middle-aged and older adults. Exp. Gerontol. 2019, 119, 203–211. [Google Scholar] [CrossRef]
- Kasović, M.; Štefan, L.; Zvonař, M. Domain-specific and total sedentary behavior associated with gait velocity in older adults: The mediating role of physical fitness. Int. J. Environ. Res. Public Health 2020, 17, 593. [Google Scholar] [CrossRef]
- Ahsan, M. Determine the kinematics and kinetics parameters associated with bilateral gait patterns among healthy, overweight, and obese adults. Acta Biomed. 2022, 93, e2022228. [Google Scholar]
- Wearing, S.C.; Hennig, E.M.; Byrne, N.M.; Steele, J.R.; Hills, A.P. The biomechanics of restricted movement in obese. Victoria 2006, 7, 13–24. [Google Scholar]
- Gouveia, É.R.; Gouveia, B.R.; Ihle, A.; Kliegel, M.; Marques, A.; Freitas, D.L. Balance and mobility relationships in older adults: A representative population-based cross-sectional study in Madeira, Portugal. Arch. Gerontol. Geriatr. 2019, 80, 65–69. [Google Scholar] [CrossRef] [PubMed]
- Oh-Park, M.; Holtzer, R.; Mahoney, J.; Wang, C.; Verghese, J. Effect of treadmill training on specific gait parameters in older adults with frailty: Case series. J. Geriatr. Phys. Ther. 2013, 71, 233–236. [Google Scholar] [CrossRef]
- Oppewal, A.; Hilgenkamp, T.I.M. The association between gait and physical fitness in adults with intellectual disabilities. J. Intellect. Disabil. Res. 2018, 62, 454–466. [Google Scholar] [CrossRef] [PubMed]
- Uematsu, A.; Tsuchiya, K.; Kadono, N.; Kobayashi, H.; Kaetsu, T.; Hortobágyi, T.; Suzuki, S. A behavioral mechanism of how increases in leg strength improve old adults′ gait speed. PLoS ONE 2014, 9, e110350. [Google Scholar] [CrossRef] [PubMed]
- Vialleron, T.; Delafontaine, A.; Ditcharles, S.; Fourcade, P.; Yiou, E. Effects of stretching exercises on human gait: A systematic review and meta-analysis. F1000Research 2020, 9, 984. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Mean | SD |
|---|---|---|
| Age (years old) | 53.5 | 7.2 |
| Weight (kg) | 71.8 | 15.7 |
| Height (cm) | 157.5 | 6.2 |
| WPI (score) | 14.7 | 3.0 |
| SSS (score) | 7.8 | 1.9 |
| BMI (kg/m2) | 28.9 | 5.9 |
| MVPA (wear time %) | 4.8 | 3.6 |
| Sedentary time (wear time %) | 51.3 | 11.0 |
| Body fat (%) | 40.3 | 7.6 |
| Physical fitness | ||
| Lower-body flexibility (cm) | −11.5 | 10.4 |
| Upper-body flexibility (cm) | −14.5 | 10.5 |
| Lower-body strength (repetitions) | 11.4 | 3.3 |
| Agility and dynamic balance (s) | −6.4 | 1.3 |
| Upper-body strength (repetitions) | 16.4 | 4.9 |
| Cardiorespiratory fitness (m) | 520.2 | 67.3 |
| Gait | ||
| Velocity (m/s) | 1.6 | 0.2 |
| Cadence (step/s) | 132.8 | 12.3 |
| Step length (cm) | 44.2 | 6.2 |
| Step cycle duration (s) | 0.5 | 0.0 |
| Unipedal stance (s) | 0.4 | 0.0 |
| Bipedal stance (s) | 0.1 | 0.0 |
| Unipedal stance phase (% of step time) | 79.6 | 4.5 |
| Bipedal stance phase (% of step time) | 20.5 | 4.5 |
| n | % | |
| Marital Status | ||
| Married | 64.0 | 76.2 |
| Unmarried | 20.0 | 23.8 |
| Educational status | ||
| Non-universitary | 73.0 | 86.9 |
| Universitary | 11.0 | 13.1 |
| Current occupational status | ||
| Working | 19.0 | 22.6 |
| Housekeeper | 24.0 | 28.6 |
| Unemployed | 41.0 | 48.8 |
| Outcomes | Gait Parameters | |||||
|---|---|---|---|---|---|---|
| Velocity (m/s) | Cadence (Step/min) | Step Length (cm) | Step Cycle Duration (s) | Unipedal Stance Phase (% Step Cycle) | Bipedal Stance Phase (% Step Cycle) | |
| MVPA | 0.31 ** | 0.11 | 0.38 ** | −0.12 | 0.16 | −0.14 |
| Sedentary time | −0.29 ** | −0.18 | −0.34 ** | 0.16 | −0.29 ** | 0.28 * |
| Fat percentage | −0.32 ** | −0.16 | −0.34 ** | 0.12 | −0.35 ** | 0.37 ** |
| Lower-body flexibility | 0.40 ** | 0.35 ** | 0.35 ** | −0.35 ** | 0.07 | −0.06 |
| Upper-body flexibility | 0.16 | −0.01 | 0.29 ** | −0.02 | 0.21 | −0.22 * |
| Lower-body strength | 0.57 ** | 0.55 ** | 0.31 ** | −0.55 ** | 0.25 * | −0.23 * |
| Agility and dynamic balance | 0.64 ** | 0.52 ** | 0.46 ** | −0.57 ** | 0.40 ** | −0.37 ** |
| Upper-body strength | 0.60 ** | 0.54 ** | 0.38 ** | −0.53 ** | 0.13 | −0.13 |
| Cardiorespiratory fitness | 0.85 ** | 0.72 ** | 0.64 ** | −0.75 ** | 0.60 ** | −0.59 ** |
| Global PF | 0.79 ** | 0.66 ** | 0.59 ** | −0.69 ** | 0.44 ** | −0.43 ** |
| Models | B | 95% CI | β | p |
|---|---|---|---|---|
| Velocity (m/s) | ||||
| MVPA (% of wear time) | 0.01 | (0.00, 0.02) | 0.24 | 0.004 |
| Sedentary time (% of wear time) | 0.00 | (−0.00, 0.01) | 0.07 | 0.438 |
| Body Fat (%) | −0.00 | (−0.01, 0.00) | −0.08 | 0.301 |
| Global PF (z-score) | 0.22 | (0.18, 0.26) | 0.76 | <0.001 |
| Cadence (step/min) | ||||
| MVPA (% of wear time) | 0.05 | (−0.64, 0.74) | 0.01 | 0.888 |
| Sedentary time (% of wear time) | −0.03 | (−0.30, 0.23) | −0.03 | 0.809 |
| Body Fat (%) | 0.11 | (−0.21, 0.42) | 0.07 | 0.509 |
| Global PF (z-score) | 10.70 | (7.81, 13.60) | 0.66 | <0.001 |
| Step length (cm) | ||||
| MVPA (% of wear time) | 0.50 | (0.17, 0.83) | 0.29 | 0.004 |
| Sedentary time (% of wear time) | 0.01 | (−0.12, 0.14) | 0.02 | 0.866 |
| Body Fat (%) | −0.12 | (−0.27, 0.03) | −0.15 | 0.120 |
| Global PF (z-score) | 3.95 | (2.57, 5.33) | 0.48 | <0.001 |
| Step cycle duration (s) | ||||
| MVPA (% of wear time) | 0.00 | (−0.00, 0.00) | −0.03 | 0.734 |
| Sedentary time (% of wear time) | 0.00 | (−0.00, 0.00) | 0.00 | 0.990 |
| Body Fat (%) | −0.00 | (−0.00, 0.00) | −0.11 | 0.254 |
| Global PF (z-score) | −0.04 | (−0.05, −0.03) | −0.70 | <0.001 |
| Unipedal stance phase (% of Step cycle) | ||||
| MVPA (% of wear time) | 0.06 | (−0.25, 0.36) | 0.05 | 0.705 |
| Sedentary time (% of wear time) | −0.04 | (−0.16, 0.08) | −0.09 | 0.527 |
| Body Fat (%) | −0.12 | (−0.26, 0.02) | −0.20 | 0.098 |
| Global PF (z-score) | 2.18 | (0.90, 3.46) | 0.37 | 0.001 |
| Bipedal stance phase (% of Step cycle) | ||||
| MVPA (% of wear time) | −0.03 | (−0.34, 0.27) | −0.03 | 0.824 |
| Sedentary time (% of wear time) | 0.04 | (−0.08, 0.15) | 0.09 | 0.557 |
| Body Fat (%) | 0.14 | (0.00, 0.28) | 0.24 | 0.049 |
| Global PF (z-score) | −2.05 | (−3.34, −0.76) | −0.35 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llorente-Romero, S.; Herrador-Colmenero, M.; Acosta-Manzano, P.; Borges-Cosic, M.; Gavilán-Carrera, B.; Latorre Román, P.Á.; Delgado-Fernández, M.; Segura-Jiménez, V. Association of Moderate-to-Vigorous Physical Activity, Sedentary Time, Fat Percentage, and Physical Fitness with Gait Parameters in Women with Fibromyalgia: The Al-Ándalus Project. Biomedicines 2024, 12, 829. https://doi.org/10.3390/biomedicines12040829
Llorente-Romero S, Herrador-Colmenero M, Acosta-Manzano P, Borges-Cosic M, Gavilán-Carrera B, Latorre Román PÁ, Delgado-Fernández M, Segura-Jiménez V. Association of Moderate-to-Vigorous Physical Activity, Sedentary Time, Fat Percentage, and Physical Fitness with Gait Parameters in Women with Fibromyalgia: The Al-Ándalus Project. Biomedicines. 2024; 12(4):829. https://doi.org/10.3390/biomedicines12040829
Chicago/Turabian StyleLlorente-Romero, Sergio, Manuel Herrador-Colmenero, Pedro Acosta-Manzano, Milkana Borges-Cosic, Blanca Gavilán-Carrera, Pedro Ángel Latorre Román, Manuel Delgado-Fernández, and Víctor Segura-Jiménez. 2024. "Association of Moderate-to-Vigorous Physical Activity, Sedentary Time, Fat Percentage, and Physical Fitness with Gait Parameters in Women with Fibromyalgia: The Al-Ándalus Project" Biomedicines 12, no. 4: 829. https://doi.org/10.3390/biomedicines12040829
APA StyleLlorente-Romero, S., Herrador-Colmenero, M., Acosta-Manzano, P., Borges-Cosic, M., Gavilán-Carrera, B., Latorre Román, P. Á., Delgado-Fernández, M., & Segura-Jiménez, V. (2024). Association of Moderate-to-Vigorous Physical Activity, Sedentary Time, Fat Percentage, and Physical Fitness with Gait Parameters in Women with Fibromyalgia: The Al-Ándalus Project. Biomedicines, 12(4), 829. https://doi.org/10.3390/biomedicines12040829