

SARS-CoV-2-Related Olfactory Dysfunction: Autopsy Findings, Histopathology, and Evaluation of Viral RNA and ACE2 Expression in Olfactory Bulbs

 , ,
, ,  , , , ,
, , , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Biosamples’ Collection, Autopsy, and Ethical Issues
2.2. SARS-CoV-2 Detection in Swab
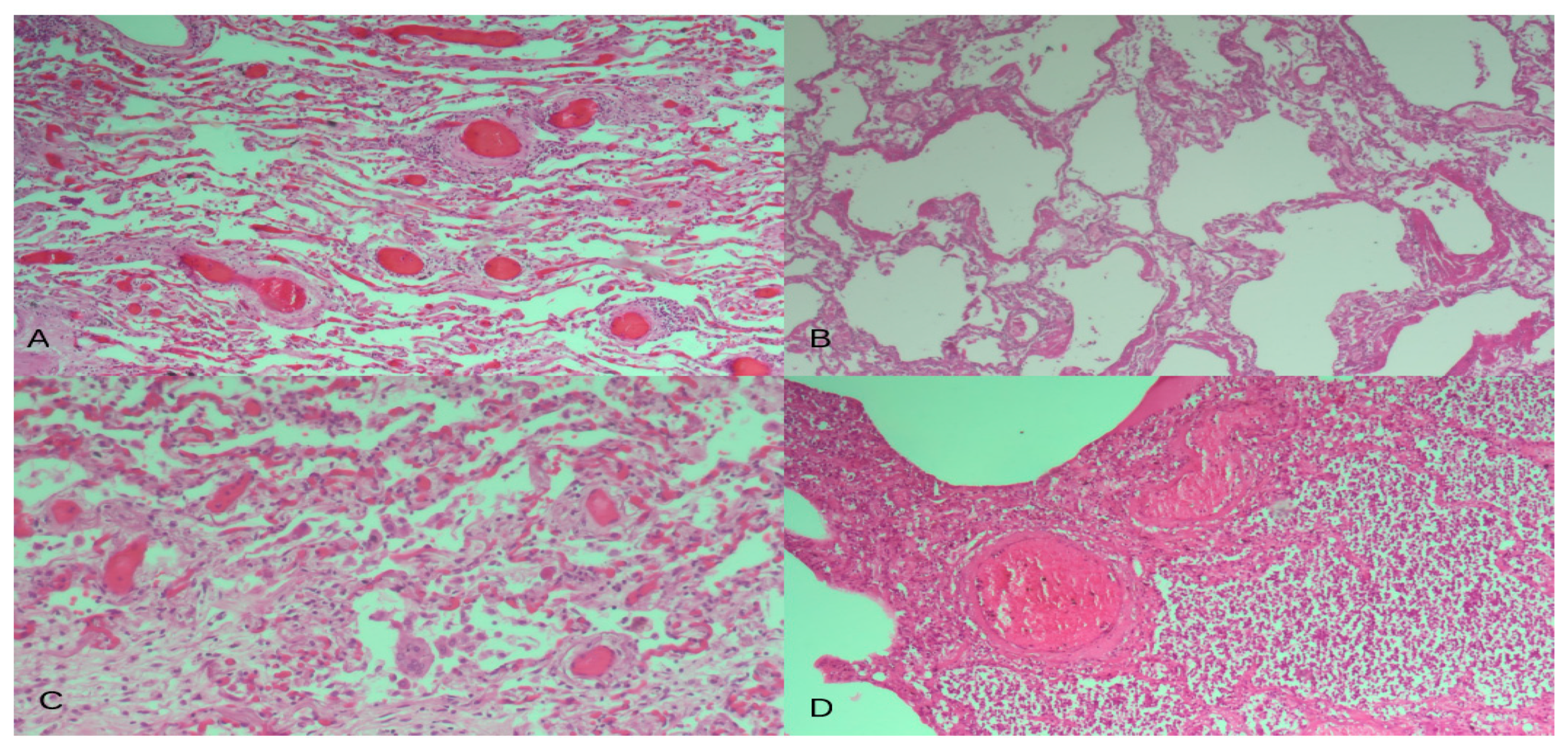
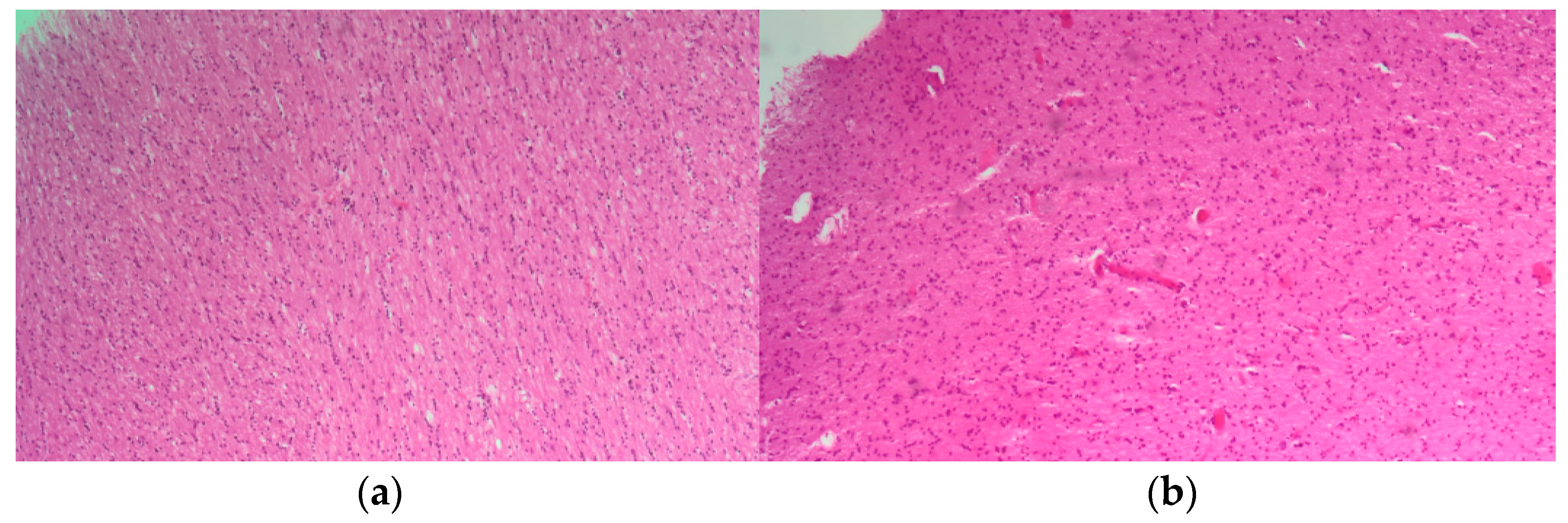
2.3. Histological Examination of Lung and Olfactory Bulb Sections
2.4. Molecular Analysis: SARS-CoV-2 Detection and ACE2 Receptor Transcript Expression
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/ (accessed on 6 January 2024).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef]
- Cafiero, C.; Rosapepe, F.; Palmirotta, R.; Re, A.; Ottaiano, M.P.; Benincasa, G.; Perone, R.; Varriale, E.; D’Amato, G.; Cacciamani, A.; et al. Angiotensin system polymorphisms’ in sars-cov-2 positive patients: Assessment between symptomatic and asymptomatic patients: A pilot study. Pharmacogenom. Pers. Med. 2021, 14, 621–629. [Google Scholar] [CrossRef] [PubMed]
- Cafiero, C.; Micera, A.; Re, A.; Postiglione, L.; Cacciamani, A.; Schiavone, B.; Benincasa, G.; Palmirotta, R. Could Small Neurotoxins-Peptides be Expressed during SARS-CoV-2 Infection? Curr. Genom. 2021, 22, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, M.; Cattani, P.; Fantoni, M.; Marchetti, S.; Aquila, I.; Stigliano, E.; Carbone, A.; Oliva, A.; Arena, V. Postmortem Swabs in the Severe Acute Respiratory Syndrome Coronavirus 2 Pandemic. Arch. Pathol. Lab. Med. 2020, 144, 1298–1302. [Google Scholar] [CrossRef] [PubMed]
- Dell’aquila, M.; Vetrugno, G.; Grassi, S.; Stigliano, E.; Oliva, A.; Rindi, G.; Arena, V. Postmodernism and the decline of the clinical autopsy. Virchows Arch. 2021, 479, 861–863. [Google Scholar] [CrossRef] [PubMed]
- Sperhake, J.P. Autopsies of COVID-19 deceased? Absolutely! Leg. Med. 2020, 47, 101769. [Google Scholar] [CrossRef] [PubMed]
- Barth, R.F.; Xu, X.; Buja, L.M. A call to action: The need for autopsies to determine the full extent of organ involvement associated with COVID-19 infections. Chest 2020, 158, 43–44. [Google Scholar] [CrossRef] [PubMed]
- Dell’Aquila, M.; Carbone, A.; Pennacchia, I.; Stigliano, E.; Oliva, A.; Arena, V. Sudden death by massive systemic embolism from cardiac myxoma. Role of the clinical autopsy and review of literature. Cardiovasc. Pathol. 2020, 49, 107244. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Matschke, J.; Lütgehetmann, M.; Hagel, C.; Sperhake, J.P.; Schröder, A.S.; Edler, C.; Mushumba, H.; Fitzek, A.; Allweiss, L.; Dandri, M.; et al. Neuropathology of patients with COVID-19 in Germany: A post-mortem case series. Lancet Neurol. 2020, 19, 919–929. [Google Scholar] [CrossRef] [PubMed]
- Porta-Etessam, J.; Núñez-Gil, I.J.; García, N.G.; Fernandez-Perez, C.; Viana-Llamas, M.C.; Eid, C.M.; Romero, R.; Molina, M.; Uribarri, A.; Becerra-Muñoz, V.M.; et al. COVID-19 anosmia and gustatory symptoms as a prognosis factor: A subanalysis of the HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID-19) registry. Infection 2021, 49, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Las Casas Lima, M.H.; de Cavalcante, A.L.B.; Leão, S.C. Pathophysiological relationship between COVID-19 and olfactory dysfunction: A systematic review. Braz. J. Otorhinolaryngol. 2021, 110, 697–700. [Google Scholar] [CrossRef] [PubMed]
- Solomon, I.H.; Normandin, E.; Bhattacharyya, S.; Mukerji, S.S.; Keller, K.; Ali, A.S.; Adams, G.; Hornick, J.L.; Padera, R.F., Jr.; Sabeti, P. Neuropathological Features of Covid-19. N. Engl. J. Med. 2020, 383, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Yoo, S.-J.; Clijsters, M.; Backaert, W.; Vanstapel, A.; Speleman, K.; Lietaer, C.; Choi, S.; Hether, T.D.; Marcelis, L.; et al. Visualizing in deceased COVID-19 patients how SARS-CoV-2 attacks the respiratory and olfactory mucosae but spares the olfactory bulb. Cell 2021, 184, 5932–5949. [Google Scholar] [CrossRef] [PubMed]
- Butowt, R.; Bilinska, K.; von Bartheld, C.S. Olfactory dysfunction in COVID-19: New insights into the underlying mechanisms. Trends Neurosci. 2023, 46, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Liang, F.; Wang, D.Y. COVID-19 Anosmia: High Prevalence, Plural Neuropathogenic Mechanisms, and Scarce Neurotropism of SARS-CoV-2? Viruses 2021, 13, 2225. [Google Scholar] [CrossRef] [PubMed]
- Maiese, A.; Manetti, A.C.; Bosetti, C.; Del Duca, F.; La Russa, R.; Frati, P.; Di Paolo, M.; Turillazzi, E.; Fineschi, V. SARS-CoV-2 and the brain: A review of the current knowledge on neuropathology in COVID-19. Brain Pathol. 2021, 31, e13013. [Google Scholar] [CrossRef]
- Brann, D.H.; Tsukahara, T.; Weinreb, C.; Lipovsek, M.; Van Den Berge, K.; Gong, B.; Chance, R.; Macaulay, I.C.; Chou, H.-J.; Fletcher, R.B.; et al. Non-neuronal expression of SARS-CoV-2 entry genes in the olfactory system suggests mechanisms underlying COVID-19-associated anosmia. Sci. Adv. 2020, 6, eabc5801. [Google Scholar] [CrossRef]
- Fabbri, V.P.; Foschini, M.P.; Lazzarotto, T.; Gabrielli, L.; Cenacchi, G.; Gallo, C.; Aspide, R.; Frascaroli, G.; Cortelli, P.; Riefolo, M.; et al. Brain ischemic injury in COVID-19-infected patients: A series of 10 post-mortem cases. Brain Pathol. 2021, 31, 205–210. [Google Scholar] [CrossRef]
- Glatzel, M. Neuropathology of COVID-19: Where are the neuropathologists? Brain Pathol. 2020, 30, 729. [Google Scholar] [CrossRef] [PubMed]
- Ramani, A.; Pranty, A.I.; Gopalakrishnan, J. Neurotropic Effects of SARS-CoV-2 Modeled by the Human Brain Organoids. Stem Cell Rep. 2021, 16, 373–384. [Google Scholar] [CrossRef] [PubMed]
- Lopez, G.; Tonello, C.; Osipova, G.; Carsana, L.; Biasin, M.; Cappelletti, G.; Pellegrinelli, A.; Lauri, E.; Zerbi, P.; Rossi, R.S.; et al. Olfactory bulb SARS-CoV-2 infection is not paralleled by the presence of virus in other central nervous system areas. Neuropathol. Appl. Neurobiol. 2022, 48, e12752. [Google Scholar] [CrossRef] [PubMed]
- E Serrano, G.; E Walker, J.; Tremblay, C.; Piras, I.S.; Huentelman, M.J.; Belden, C.M.; Goldfarb, D.; Shprecher, D.; Atri, A.; Adler, C.H.; et al. SARS-CoV-2 Brain Regional Detection, Histopathology, Gene Expression, and Immunomodulatory Changes in Decedents with COVID-19. J. Neuropathol. Exp. Neurol. 2022, 81, 666–695. [Google Scholar] [CrossRef] [PubMed]
- Kantonen, J.; Mahzabin, S.; Mäyränpää, M.I.; Tynninen, O.; Paetau, A.; Andersson, N.; Sajantila, A.; Vapalahti, O.; Carpén, O.; Kekäläinen, E.; et al. Neuropathologic features of four autopsied COVID-19 patients. Brain Pathol. 2020, 30, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Bryche, B.; St Albin, A.; Murri, S.; Lacôte, S.; Pulido, C.; Ar Gouilh, M.; Lesellier, S.; Servat, A.; Wasniewski, M.; Picard-Meyer, E.; et al. Massive transient damage of the olfactory epithelium associated with infection of sustentacular cells by SARS-CoV-2 in golden Syrian hamsters. Brain. Behav. Immun. 2020, 89, 579–586. [Google Scholar] [CrossRef]
- Gheware, A.; Ray, A.; Rana, D.; Bajpai, P.; Nambirajan, A.; Arulselvi, S.; Mathur, P.; Trikha, A.; Arava, S.; Das, P.; et al. ACE2 protein expression in lung tissues of severe COVID-19 infection. Sci. Rep. 2022, 12, 4058. [Google Scholar] [CrossRef] [PubMed]
- Salamanna, F.; Maglio, M.; Landini, M.P.; Fini, M. Body Localization of ACE-2: On the Trail of the Keyhole of SARS-CoV-2. Front. Med. 2020, 7, 594495. [Google Scholar] [CrossRef] [PubMed]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.-C.; Turner, A.J.; Raizada, M.K.; Grant, M.B.; Oudit, G.Y. Response by Gheblawi et al to Letter Regarding Article, “Angiotensin-Converting Enzyme 2: SARS-CoV-2 Receptor and Regulator of the Renin-Angiotensin System: Celebrating the 20th Anniversary of the Discovery of ACE2”. Circ. Res. 2020, 126, 1456–1474. [Google Scholar] [CrossRef]
- Ueha, R.; Ito, T.; Furukawa, R.; Kitabatake, M.; Ouji-Sageshima, N.; Ueha, S.; Koyama, M.; Uranaka, T.; Kondo, K.; Yamasoba, T. Oral SARS-CoV-2 Inoculation Causes Nasal Viral Infection Leading to Olfactory Bulb Infection: An Experimental Study. Front. Cell. Infect. Microbiol. 2022, 12, 924725. [Google Scholar] [CrossRef]
- Bertinato, L.; Brambilla, G.; Canevelli, M.; Calcagnini, G.; Censi, F.; Colaizzo, E.; Donfrancesco, C.; Lega, I.; Noce, C.L.; Manno, V. Gruppo di lavoro ISS Cause di morte COVID-19. In Procedura per L’esecuzione di Riscontri Diagnostici in Pazienti Deceduti con Infezione da SARS-CoV-2. Versione del 23 Marzo 2020; Rapporto ISS COVID-19, n. 6/2020; Istituto Superiore di Sanità: Roma, Italy, 2020. [Google Scholar]
- Stigliano, E.; Dell’aquila, M.; Vetrugno, G.; Grassi, S.; Amirhassankhani, S.; Amadoro, G.; Oliva, A.; Arena, V. Transdiaphragmatic autopsy approach: Our experience in the Sars-CoV-2 pandemic. Virchows Arch. 2023, 482, 773–776. [Google Scholar] [CrossRef] [PubMed]
- Hasmi, A.H.; Khoo, L.S.; Koo, Z.P.; Suriani, M.U.A.; Hamdan, A.N.; Yaro, S.W.M.; Arshad, S.; Siew, S.F.; Ibrahim, M.A.; Mahmood, M.S. The craniotomy box: An innovative method of containing hazardous aerosols generated during skull saw use in autopsy on a COVID-19 body. Forensic Sci. Med. Pathol. 2020, 16, 477–480. [Google Scholar] [CrossRef]
- Nava-Santana, C.; Rodríguez-Armida, M.; Jiménez, J.V.; Vargas-Parra, N.; León, D.E.A.; Campos-Murguia, A.; Macías-Rodriguez, R.; Arteaga-Garrido, A.; Hernández-Villegas, A.C.; Dominguez-Cherit, G.; et al. Clinicopathologic characteristics of severe COVID-19 patients in Mexico City: A post-mortem analysis using a minimally invasive autopsy approach. PLoS ONE 2022, 17, e0262783. [Google Scholar] [CrossRef]
- Remmelink, M.; De Mendonça, R.; D’haene, N.; De Clercq, S.; Verocq, C.; Lebrun, L.; Lavis, P.; Racu, M.-L.; Trépant, A.-L.; Maris, C.; et al. Unspecific post-mortem findings despite multiorgan viral spread in COVID-19 patients. Crit. Care 2020, 24, 495. [Google Scholar] [CrossRef]
- EpiCentro. Monitoraggio Delle Varianti del Virus SARS-CoV-2 di Interesse in Sanità Pubblica in Italia. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-monitoraggio-varianti-rapporti-periodici (accessed on 1 January 2024).
- Ziuzia-Januszewska, L.; Januszewski, M. Pathogenesis of Olfactory Disorders in COVID-19. Brain Sci. 2022, 12, 449. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.C.; Nallani, R.; Cass, L.; Bhalla, V.; Chiu, A.G.; Villwock, J.A. A Systematic Review of the Neuropathologic Findings of Post-Viral Olfactory Dysfunction: Implications and Novel Insight for the COVID-19 Pandemic. Am. J. Rhinol. Allergy 2021, 35, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Coelho, D.H.; Reiter, E.R.; French, E.; Costanzo, R.M. Decreasing Incidence of Chemosensory Changes by COVID-19 Variant. Otolaryngol. Head Neck Surg. 2023, 168, 704–706. [Google Scholar] [CrossRef] [PubMed]
- Freire-De-Lima, L.; Scovino, A.M.; da Fonseca, L.M.; Menezes, C.C.B.; Santos, C.A.D.N.; de Lima, M.E.F.; Decote-Ricardo, D.; Freire-De-Lima, M.; da Costa, K.M.; dos Reis, J.S.; et al. COVID-19 Infection and Neuropathological Features. Medicines 2021, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Saussez, S.; Lechien, J.R.; Hopkins, C. Anosmia: An evolution of our understanding of its importance in COVID-19 and what questions remain to be answered. Eur. Arch. Otorhinolaryngol. 2021, 278, 2187–2191. [Google Scholar] [CrossRef]
- Puelles, V.G.; Lütgehetmann, M.; Lindenmeyer, M.T.; Sperhake, J.P.; Wong, M.N.; Allweiss, L.; Chilla, S.; Heinemann, A.; Wanner, N.; Liu, S.; et al. Multiorgan and Renal Tropism of SARS-CoV-2. N. Engl. J. Med. 2020, 383, 590–592. [Google Scholar] [CrossRef]
- Ludlow, M.; Kortekaas, J.; Herden, C.; Hoffmann, B.; Tappe, D.; Trebst, C.; Griffin, D.E.; Brindle, H.E.; Solomon, T.; Brown, A.S.; et al. Neurotropic virus infections as the cause of immediate and delayed neuropathology. Acta Neuropathol. 2016, 3, 159–184. [Google Scholar] [CrossRef] [PubMed]
- Klingenstein, M.; Klingenstein, S.; Neckel, P.H.; Mack, A.F.; Wagner, A.P.; Kleger, A.; Liebau, S.; Milazzo, A. Evidence of SARS-CoV2 Entry Protein ACE2 in the Human Nose and Olfactory Bulb. Cells Tissues Organs 2020, 209, 155–164. [Google Scholar] [CrossRef] [PubMed]
- Cazzolla, A.P.; Lovero, R.; Muzio, L.L.; Testa, N.F.; Schirinzi, A.; Palmieri, G.; Pozzessere, P.; Procacci, V.; Di Comite, M.; Ciavarella, D.; et al. Taste and Smell Disorders in COVID-19 Patients: Role of Interleukin-6. ACS Chem. Neurosci. 2020, 11, 2774–2781. [Google Scholar] [CrossRef] [PubMed]
- Finlay, J.B.; Brann, D.H.; Hachem, R.A.; Jang, D.W.; Oliva, A.D.; Ko, T.; Gupta, R.; Wellford, S.A.; Moseman, E.A.; Jang, S.S.; et al. Persistent post-COVID-19 smell loss is associated with immune cell infiltration and altered gene expression in olfactory epithelium. Sci. Transl. Med. 2022, 14, eadd0484. [Google Scholar] [CrossRef]
- O’Brien, B.C.V.; Weber, L.; Hueffer, K.; Weltzin, M.M. SARS-CoV-2 spike ectodomain targets α7 nicotinic acetylcholine receptors. J. Biol. Chem. 2023, 299, 104707. [Google Scholar] [CrossRef] [PubMed]
- Chrestia, J.F.; Oliveira, A.S.; Mulholland, A.J.; Gallagher, T.; Bermúdez, I.; Bouzat, C. A Functional Interaction Between Y674-R685 Region of the SARS-CoV-2 Spike Protein and the Human α7 Nicotinic Receptor. Mol. Neurobiol. 2022, 59, 6076–6090. [Google Scholar] [CrossRef]
- Ogg, M.C.; Ross, J.M.; Bendahmane, M.; Fletcher, M.L. Olfactory bulb acetylcholine release dishabituates odor responses and reinstates odor investigation. Nat. Commun. 2018, 9, 1868. [Google Scholar] [CrossRef] [PubMed]
- Lin, T.P.H.; Ko, C.N.; Zheng, K.; Lai, K.H.W.; Wong, R.L.M.; Lee, A.; Zhang, S.; Huang, S.S.; Wan, K.H.; Lam, D.S.C. COVID-19: Update on Its Ocular Involvements, and Complications from Its Treatments and Vaccinations. Asia Pac. J. Ophthalmol. 2021, 10, 521–529. [Google Scholar] [CrossRef]
- Kopańska, M.; Batoryna, M.; Bartman, P.; Szczygielski, J.; Banaś-Ząbczyk, A. Disorders of the Cholinergic System in COVID-19 Era-A Review of the Latest Research. Int. J. Mol. Sci. 2022, 23, 672. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | Age | Sex | Comorbidities | Ante-Mortem Nasopharyngeal | Post-Mortem Nasopharyngeal | Post-Mortem Tracheal | Post-Mortem Right Lung | Post-Mortem Left Lung |
|---|---|---|---|---|---|---|---|---|
| 1 | 93 | F | hypertension, dementia | Positive | Negative | positive | positive | positive |
| 2 | 80 | F | dementia, T2D, epilepsy | Positive | Positive | positive | positive | positive |
| 3 | 84 | F | previous STEMI, CKD, COPD | Positive | Positive | negative | negative | negative |
| 4 | 78 | F | T2D, hypertension | Positive | Positive | negative | negative | positive |
| 5 | 90 | F | dementia, hypertension | Inconclusive | Positive | negative | negative | positive |
| 6 | 80 | M | AD, essential thrombocythemia, CHD | Positive | Positive | negative | negative | negative |
| 7 | 92 | F | CKD, T2D | Positive | Positive | negative | negative | negative |
| 8 | 81 | M | AF, dementia, T2D | Positive | Negative | positive | negative | negative |
| 9 | 75 | M | CKD, dialysis, T2D | negative | Positive | positive | positive | positive |
| 10 | 52 | M | CHD, CKD | negative | Positive | positive | positive | positive |
| 11 | 80 | M | CHD, CKD | negative | Positive | positive | positive | positive |
| 12 | 87 | F | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 13 | 61 | M | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 14 | 93 | M | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 15 | 64 | F | CKD, T2D, CKD, HF | positive | Positive | positive | positive | positive |
| 16 | 62 | M | previous myocardial infarction, stent, syncope, head trauma, subarachnoid hemorrhage | negative | Positive | positive | positive | positive |
| 17 | 96 | F | dementia, hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 18 | 94 | F | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 19 | 93 | M | hypertension, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 20 | 82 | M | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 21 | 92 | M | hypertension, CKD, AF, HF | positive | Positive | negative | positive | positive |
| 22 | 73 | M | hypertension, dyslipidemia, T2D, COPD, CKD, AF, HF | positive | Positive | positive | positive | positive |
| 23 | 87 | F | dementia, heart disease | positive | Positive | positive | positive | positive |
| 24 | 88 | M | hypertension, HF | positive | Positive | positive | positive | positive |
| 25 | 65 | M | hypertension, CHD | positive | Positive | positive | positive | positive |
| Case | Lung | |||||||
|---|---|---|---|---|---|---|---|---|
| DAD Phase | Thrombotic Micro-Angiopathy | Perivascular Lymphocytic Cuffs | Hyaline Membranes | Pneumocyte Hyperplasia | Superimposed Pneumonia | Alveolar Hemorrhages | Giant Cells | |
| 1 | exudative | diffuse | Present | Present | Present | bacterial | Present | present |
| 2 | exudative | diffuse | Present | Present | Present | bacterial | Present | absent |
| 3 | exudative | diffuse | Present | Present | Focal | bacterial | Absent | absent |
| 4 | organizing | diffuse | Diffuse | Focal | Diffuse | negative | Present | present |
| 5 | exudative | diffuse | Diffuse | Absent | Focal | negative | Focal | present |
| 6 | organizing | diffuse | Focal | Absent | Absent | negative | Absent | absent |
| 7 | exudative | diffuse | Present | Present | Present | bacterial | Present | present |
| 8 | exudative | diffuse | Present | Present | Focal | bacterial | Absent | present |
| 9 | exudative | diffuse | Present | Present | Focal | bacterial | Absent | absent |
| 10 | organizing | diffuse | Diffuse | Focal | Diffuse | bacterial | Present | absent |
| 11 | organizing | diffuse | Diffuse | Focal | Diffuse | negative | Present | present |
| 12 | exudative | diffuse | Diffuse | Absent | Focal | negative | Focal | present |
| 13 | exudative | diffuse | Diffuse | Absent | Focal | negative | Focal | present |
| 14 | fibrotic | focal | Absent | Focal | Absent | bacterial | Present | absent |
| 15 | fibrotic | focal | Absent | Focal | Absent | bacterial | Present | absent |
| 16 | fibrotic | focal | Absent | Focal | Absent | bacterial | Present | absent |
| 17 | fibrotic | focal | Absent | Diffuse | Absent | bacterial | Present | absent |
| 18 | exudative | diffuse | Diffuse | Absent | Focal | negative | Focal | present |
| 19 | fibrotic | focal | Absent | Diffuse | Absent | bacterial | Present | absent |
| 20 | fibrotic | focal | Focal | Diffuse | Absent | bacterial | Present | absent |
| 21 | exudative | focal | Diffuse | Absent | Focal | bacterial | Focal | absent |
| 22 | exudative | focal | Diffuse | Absent | Focal | bacterial | Focal | absent |
| 23 | fibrotic | focal | Absent | Diffuse | Absent | bacterial | Present | absent |
| 24 | fibrotic | focal | Absent | Diffuse | Absent | bacterial | Absent | absent |
| 25 | organizing | diffuse | Focal | Focal | Diffuse | bacterial | Present | present |
| Case | Ante-Mortem Nasopharyngeal Swab a | SARS-CoV-2 Lung | SARS-CoV-2 Olfactory Bulb | ACE2 Lung | ACE2 Olfactory Bulb |
|---|---|---|---|---|---|
| 1 | positive | 29 | negative | 29 | 39 |
| 2 | positive | 30 | negative | 26 | 36 |
| 3 | positive | 33 | negative | 30 | negative |
| 4 | positive | 31 | negative | 28 | 38 |
| 5 | inconclusive | 24 | 38 | 25 | 37 |
| 6 | positive | Negative | negative | 30 | 39 |
| 7 | positive | 34 | negative | 31 | 40 |
| 8 | positive | 29 | 37 | 28 | 38 |
| 9 | negative | Negative | negative | 29 | 39 |
| 10 | negative | 21 | negative | 25 | 40 |
| 11 | negative | 24 | negative | 24 | 38 |
| 12 | positive | 33 | negative | 29 | negative |
| 13 | positive | 24 | negative | 25 | 38 |
| 14 | positive | 31 | negative | 28 | 40 |
| 15 | positive | 29 | negative | 29 | 41 |
| 16 | negative | 31 | 39 | 27 | 27 |
| 17 | positive | 35 | negative | 26 | 26 |
| 18 | positive | 24 | negative | 27 | 39 |
| 19 | positive | 33 | negative | 29 | 38 |
| 20 | positive | 28 | negative | 30 | negative |
| 21 | positive | 29 | negative | 31 | 31 |
| 22 | positive | 27 | 39 | 26 | 36 |
| 23 | positive | 33 | negative | 29 | 38 |
| 24 | positive | 27 | negative | 27 | 36 |
| 25 | positive | 35 | negative | 30 | negative |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dell’Aquila, M.; Cafiero, C.; Micera, A.; Stigliano, E.; Ottaiano, M.P.; Benincasa, G.; Schiavone, B.; Guidobaldi, L.; Santacroce, L.; Pisconti, S.; et al. SARS-CoV-2-Related Olfactory Dysfunction: Autopsy Findings, Histopathology, and Evaluation of Viral RNA and ACE2 Expression in Olfactory Bulbs. Biomedicines 2024, 12, 830. https://doi.org/10.3390/biomedicines12040830
Dell’Aquila M, Cafiero C, Micera A, Stigliano E, Ottaiano MP, Benincasa G, Schiavone B, Guidobaldi L, Santacroce L, Pisconti S, et al. SARS-CoV-2-Related Olfactory Dysfunction: Autopsy Findings, Histopathology, and Evaluation of Viral RNA and ACE2 Expression in Olfactory Bulbs. Biomedicines. 2024; 12(4):830. https://doi.org/10.3390/biomedicines12040830
Chicago/Turabian StyleDell’Aquila, Marco, Concetta Cafiero, Alessandra Micera, Egidio Stigliano, Maria Pia Ottaiano, Giulio Benincasa, Beniamino Schiavone, Leo Guidobaldi, Luigi Santacroce, Salvatore Pisconti, and et al. 2024. "SARS-CoV-2-Related Olfactory Dysfunction: Autopsy Findings, Histopathology, and Evaluation of Viral RNA and ACE2 Expression in Olfactory Bulbs" Biomedicines 12, no. 4: 830. https://doi.org/10.3390/biomedicines12040830