
Investigation of the Effect of Therapeutic Plasma Exchange for TAFRO Syndrome: A Pilot Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Designs and Participants
2.2. Clinical Findings and Treatment
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
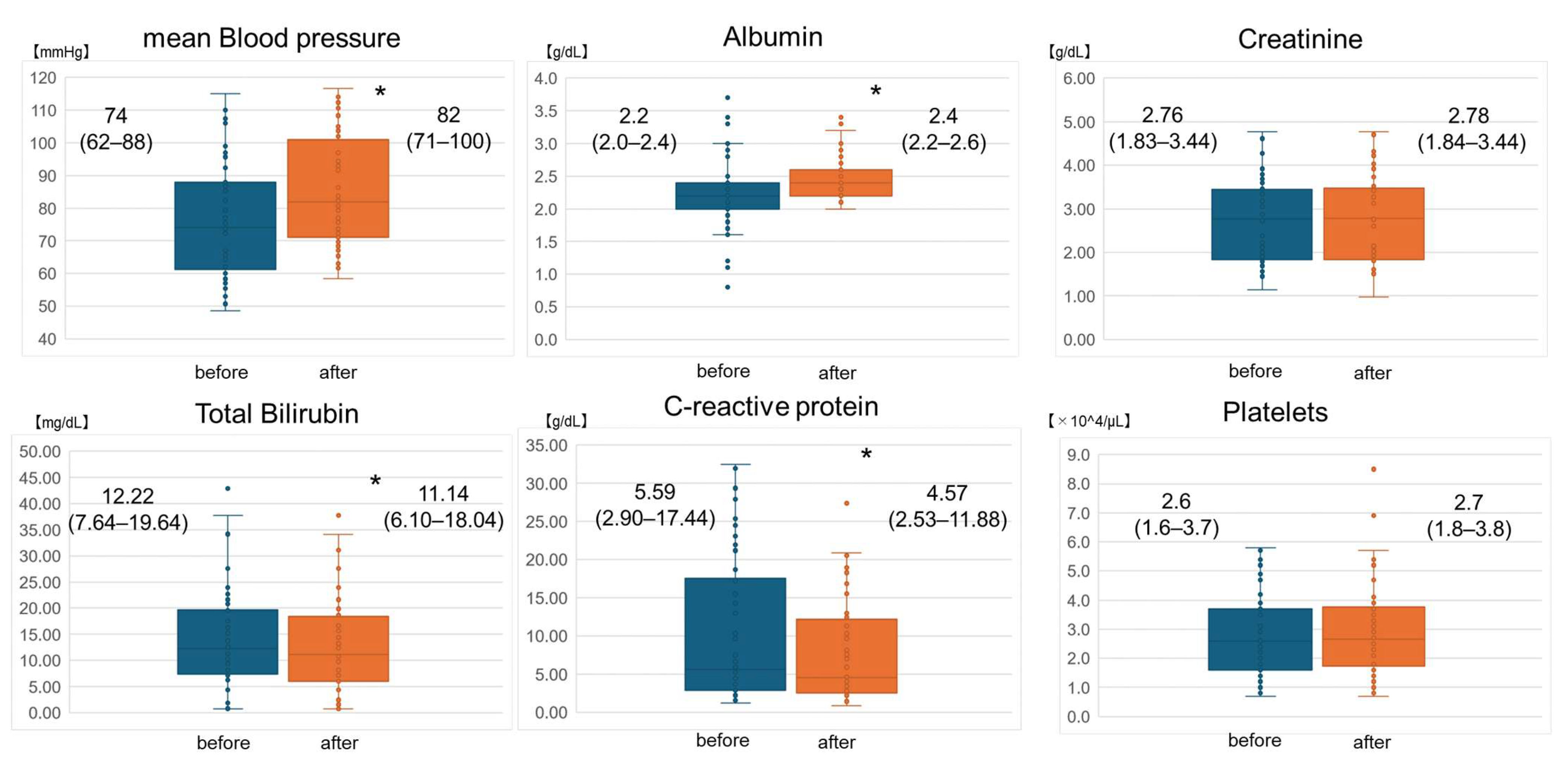
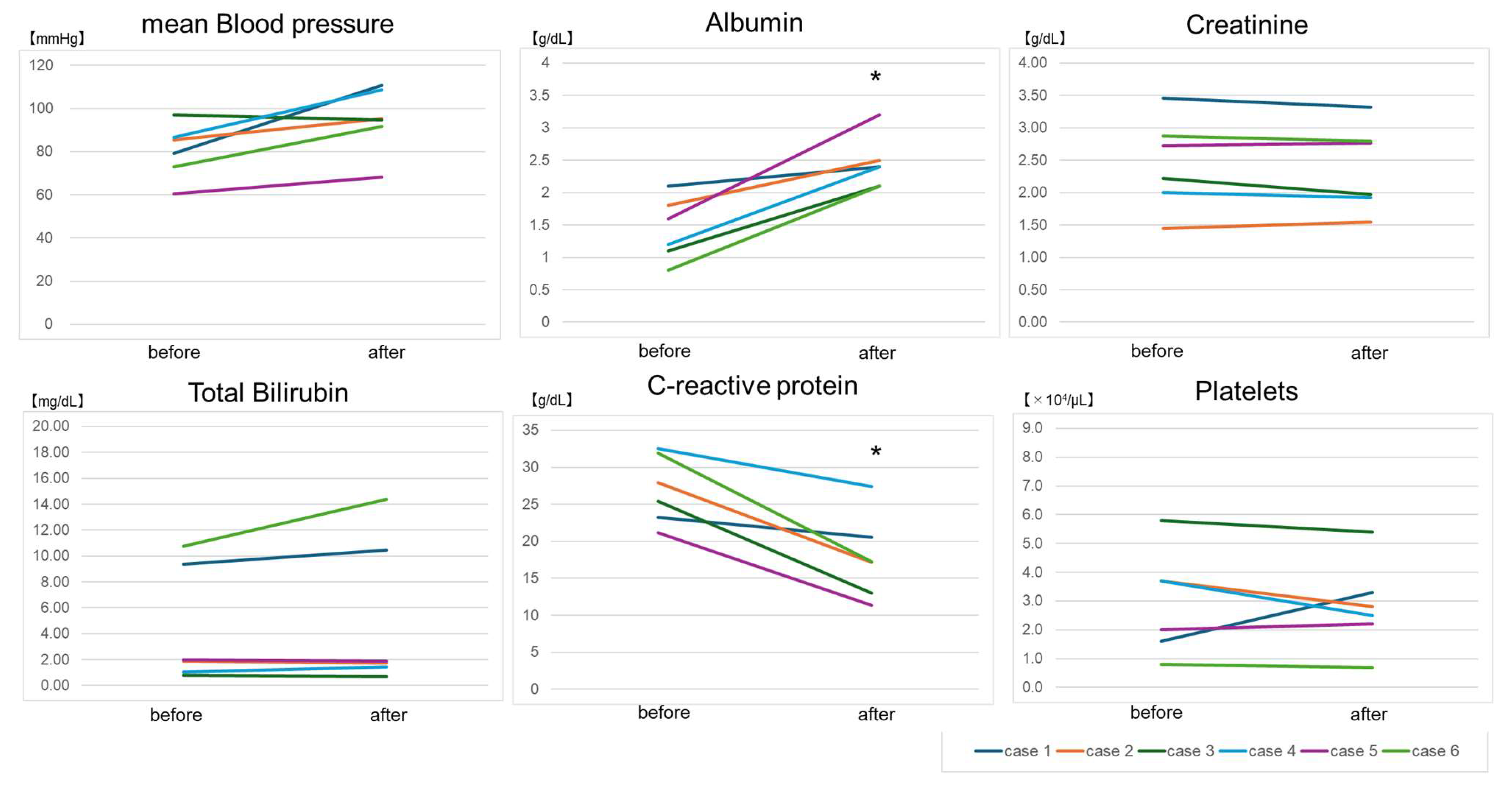
3.2. Changes in Clinical Data before and after TPE
3.3. Timing of Initiation of TPE and Pharmacotherapy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Takai, K.; Nikkuni, K.; Shibuya, H.; Hashidate, H. Thrombocytopenia with mild bone marrow fibrosis accompanied by fever, pleural effusion, ascites and hepatosplenomegaly. Rinsho Ketsueki 2010, 51, 320–325. [Google Scholar] [PubMed]
- Dispenzieri, A.; Fajgenbaum, D.C. Overview of Castleman disease. Blood 2020, 135, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Fajgenbaum, D.C.; Uldrick, T.S.; Bagg, A.; Frank, D.; Wu, D.; Srkalovic, G.; Simpson, D.; Liu, A.Y.; Menke, D.; Chandrakasan, S.; et al. International, evidence-based consensus diagnostic criteria for HHV-8-negative/idiopathic multicentric Castleman disease. Blood 2017, 129, 1646–1657. [Google Scholar] [CrossRef] [PubMed]
- Masaki, Y.; Kawabata, H.; Takai, K.; Kojima, M.; Tsukamoto, N.; Ishigaki, Y.; Kurose, N.; Ide, M.; Murakami, J.; Nara, K.; et al. Proposed diagnostic criteria, disease severity classification and treatment strategy for TAFRO syndrome, 2015 version. Int. J. Hematol. 2016, 103, 686–692. [Google Scholar] [CrossRef]
- Masaki, Y.; Kawabata, H.; Takai, K.; Tsukamoto, N.; Fujimoto, S.; Ishigaki, Y.; Kurose, N.; Miura, K.; Nakamura, S.; Aoki, S. 2019 Updated diagnostic criteria and disease severity classification for TAFRO syndrome. Int. J. Hematol. 2020, 111, 155–158. [Google Scholar] [CrossRef] [PubMed]
- Van Rhee, F.; Voorhees, P.; Dispenzieri, A.; Fosså, A.; Srkalovic, G.; Ide, M.; Munshi, N.; Schey, S.; Streetly, M.; Pierson, S.K.; et al. International, evidence-based consensus treatment guidelines for idiopathic multicentric Castleman disease. Blood 2018, 132, 2115–2124. [Google Scholar] [CrossRef]
- Cervantes, C.E.; Bloch, E.M.; Sperati, C.J. Therapeutic Plasma Exchange: Core Curriculum 2023. Am. J. Kidney Dis. 2023, 81, 475–492. [Google Scholar] [CrossRef]
- Ozawa, Y.; Yamamoto, H.; Yasuo, M.; Takahashi, H.; Tateishi, K.; Ushiki, A.; Kawakami, S.; Fujinaga, Y.; Asaka, S.; Sano, K.; et al. Two patients with TAFRO syndrome exhibiting strikingly similar anterior mediastinal lesions with predominantly fat attenuation on chest computed tomography. Respir. Investig. 2017, 55, 176–180. [Google Scholar] [CrossRef]
- Yasuda, S.; Tanaka, K.; Ichikawa, A.; Watanabe, K.; Uchida, E.; Yamamoto, M.; Yamamoto, K.; Mizuchi, D.; Miura, O.; Fukuda, T. Aggressive TAFRO syndrome with reversible cardiomyopathy successfully treated with combination chemotherapy. Int. J. Hematol. 2016, 104, 512–518. [Google Scholar] [CrossRef]
- Hiramatsu, S.; Ohmura, K.; Tsuji, H.; Kawabata, H.; Kitano, T.; Sogabe, A.; Hashimoto, M.; Murakami, K.; Imura, Y.; Yukawa, N.; et al. Successful treatment by rituximab in a patient with TAFRO syndrome with cardiomyopathy. Nihon Rinsho Meneki Gakkai Kaishi 2016, 39, 64–71. [Google Scholar] [CrossRef]
- Noda, Y.; Saka, Y.; Kato, A.; Mimura, T.; Naruse, T. Successful rituximab treatment of TAFRO syndrome with pathological findings of glomerular endothelial damage. Clin. Nephrol. Case Stud. 2018, 6, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, H.; Sekine, A.; Oguro, M.; Oshima, Y.; Kawada, M.; Sumida, K.; Yamanouchi, M.; Hayami, N.; Suwabe, T.; Hiramatsu, R.; et al. Renal histology in a patient with TAFRO syndrome: A case report. Hum. Pathol. 2018, 82, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Meguri, Y.; Asada, N.; Nakasako, Y.; Kondo, E.; Kambara, Y.; Yamamoto, A.; Masunari, T.; Sezaki, N.; Ikeda, G.; Toji, T.; et al. A case report of TAFRO syndrome successfully treated by immunosuppressive therapies with plasma exchange. Ann. Hematol. 2019, 98, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Nagai, M.; Uchida, T.; Yamada, M.; Komatsu, S.; Ota, K.; Mukae, M.; Iwamoto, H.; Hirano, H.; Karube, M.; Kaname, S.; et al. TAFRO Syndrome in a Kidney Transplant Recipient That Was Diagnosed on Autopsy: A Case Report. Front. Med. 2021, 8, 747678. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, Y.; Shirakabe, A.; Asayama, T.; Okazaki, H.; Shibata, Y.; Shigihara, S.; Sawatani, T.; Yokose, N.; Asai, K. Successful Treatment of Thrombocytopenia, Anasarca, Fever, Reticulin Myelofibrosis/Renal Insufficiency, and Organomegaly Syndrome Using Plasma Exchange Followed by Rituximab in the Intensive Care Unit. J. Med. Cases 2021, 12, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Sakaki, A.; Hosoi, H.; Kosako, H.; Furuya, Y.; Iwamoto, R.; Hiroi, T.; Murata, S.; Mushino, T.; Murata, S.I.; Sonoki, T. Successful combination treatment with rituximab, steroid pulse therapy, plasma exchange and romiplostim for very severe TAFRO syndrome. Leuk. Lymphoma 2022, 63, 2499–2502. [Google Scholar] [CrossRef] [PubMed]
- Bauer, P.R.; Ostermann, M.; Russell, L.; Robba, C.; David, S.; Ferreyro, B.L.; Cid, J.; Castro, P.; Juffermans, N.P.; Montini, L.; et al. Plasma exchange in the intensive care unit: A narrative review. Intensive Care Med. 2022, 48, 1382–1396. [Google Scholar] [CrossRef] [PubMed]
- Zwaginga, J.J.; van der Holt, B.; Te Boekhorst, P.A.; Biemond, B.J.; Levin, M.D.; van der Griend, R.; Brand, A.; Zweegman, S.; Pruijt, H.F.; Novotny, V.M.; et al. Multi-center randomized open label phase II trial on three rituximab dosing schemes in immune thrombocytopenia patients. Haematologica 2015, 100, e90–e92. [Google Scholar] [CrossRef] [PubMed]
- Cid, J.; Carbassé, G.; Andreu, B.; Baltanás, A.; Garcia-Carulla, A.; Lozano, M. Efficacy and safety of plasma exchange: Ann 11-year single-center experience of 2730 procedures in 317 patients. Transfus. Apher. Sci. 2014, 51, 209–214. [Google Scholar] [CrossRef]
- Matsuhisa, T.; Takahashi, N.; Nakaguro, M.; Sato, M.; Inoue, E.; Teshigawara, S.; Ozawa, Y.; Kondo, T.; Nakamura, S.; Sato, J.; et al. Fatal case of TAFRO syndrome associated with over-immunosuppression: A case report and review of the literature. Nagoya J. Med. Sci. 2019, 81, 519–528. [Google Scholar] [CrossRef]
- Fajgenbaum, D.C.; June, C.H. Cytokine Storm. N. Engl. J. Med. 2020, 383, 2255–2273. [Google Scholar] [CrossRef] [PubMed]
- Tu, K.H.; Fan, P.Y.; Chen, T.D.; Chuang, W.Y.; Wu, C.Y.; Ku, C.L.; Tian, Y.C.; Yang, C.W.; Fang, J.T.; Yang, H.Y. TAFRO Syndrome with Renal Thrombotic Microangiopathy: Insights into the Molecular Mechanism and Treatment Opportunities. Int. J. Mol. Sci. 2021, 22, 6286. [Google Scholar] [CrossRef] [PubMed]
- Uemura, T.; Matsui, M.; Kokubu, M.; Samejima, K.I.; Tsuruya, K. Renal histological continuum of TAFRO syndrome: A case report and literature review. Clin. Nephrol. 2022, 97, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Zhang, Y.; Zhou, G.; Zhu, J. Kidney biopsy findings in two patients with TAFRO syndrome: Case presentations and review of the literature. BMC Nephrol. 2020, 21, 499. [Google Scholar] [CrossRef] [PubMed]
- Adamski, J. Thrombotic microangiopathy and indications for therapeutic plasma exchange. Hematol. Am. Soc. Hematol. Educ. Program 2014, 2014, 444–449. [Google Scholar] [CrossRef]
- Connelly-Smith, L.; Alquist, C.R.; Aqui, N.A.; Hofmann, J.C.; Klingel, R.; Onwuemene, O.A.; Patriquin, C.J.; Pham, H.P.; Sanchez, A.P.; Schneiderman, J.; et al. Guidelines on the Use of Therapeutic Apheresis in Clinical Practice—Evidence-Based Approach from the Writing Committee of the American Society for Apheresis: The Ninth Special Issue. J. Clin. Apher. 2023, 38, 77–278. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Case | Age, Gender | Pharmacotherapy | SOFA Score on Hospital Admission | SOFA Score on TPE Initiation | Days from Onset to TPE Initiation | Type and Volume of Replacement Fluid for the First TPE | Total Number of TPE Procedures | Outcome |
|---|---|---|---|---|---|---|---|---|
| 1 | 43, male | GC | 5 | 13 | 41 | FFP, 0.76 PV | 35 | Died (multiple organ failure) |
| 2 | 46, male | GC | 3 | 7 | 18 | FFP, 1.49 PV | 8 | Survived |
| 3 | 74, male | GC, CsA | 3 | 8 | 28 | FFP, 1.31 PV | 4 | Survived |
| 4 | 46, female | GC, TCZ, CsA, RTX | 7 | 7 | 20 | Alb, 1.17 PV | 2 | Survived |
| 5 | 72, female | GC, TCZ | 1 | 11 | 22 | Alb, 1.25 PV | 2 | Survived |
| 6 | 60, female | GC, TCZ | 2 | 16 | 53 | FFP, 1.16 PV | 5 | Died (infection) |
| Age, Gender | Treatment | Response to TPE | Outcome | |
|---|---|---|---|---|
| Yasuda, 2016 [9] | 21, female | GC, CsA, Tac, R-CHOP,R-CEPP | Not effective | Survived |
| Hiramatsu, 2016 [10] | 48, male | GC, TCZ, RTX, IVIG | Not effective | Survived |
| Ozawa, 2017 [8] | 46, male | GC | Effective | Survived |
| Ozawa, 2017 [8] | 43, male | GC | Effective | Died (multiple organ failure) |
| Noda, 2018 [11] | 79, female | GC, RTX | Not effective | Survived |
| Mizuno, 2018 [12] | 84, male | GC, TCZ | Not effective | Died (Aspiration pneumonia) |
| Meguri, 2019 [13] | 52, female | GC, CY, TCZ, RTX | Effective | Survived |
| Nagai, 2021 [14] | 57, male | GC, Tac, MMF | Not effective | Died |
| Otsuka, 2021 [15] | 69, female | GC, TCZ, RTX | Effective | Survived |
| Sakaki, 2022 [16] | 51, female | GC, CsA, RTX | Effective | Survived |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sonoda, K.; Komatsu, M.; Ozawa, Y.; Yamamoto, H.; Kamijo, Y. Investigation of the Effect of Therapeutic Plasma Exchange for TAFRO Syndrome: A Pilot Study. Biomedicines 2024, 12, 849. https://doi.org/10.3390/biomedicines12040849
Sonoda K, Komatsu M, Ozawa Y, Yamamoto H, Kamijo Y. Investigation of the Effect of Therapeutic Plasma Exchange for TAFRO Syndrome: A Pilot Study. Biomedicines. 2024; 12(4):849. https://doi.org/10.3390/biomedicines12040849
Chicago/Turabian StyleSonoda, Kosuke, Masamichi Komatsu, Yoko Ozawa, Hiroshi Yamamoto, and Yuji Kamijo. 2024. "Investigation of the Effect of Therapeutic Plasma Exchange for TAFRO Syndrome: A Pilot Study" Biomedicines 12, no. 4: 849. https://doi.org/10.3390/biomedicines12040849