
Interleukin-6 and Lymphocyte-to-Monocyte Ratio Indices Identify Patients with Intrahepatic Cholangiocarcinoma

Abstract
1. Introduction
2. Methods
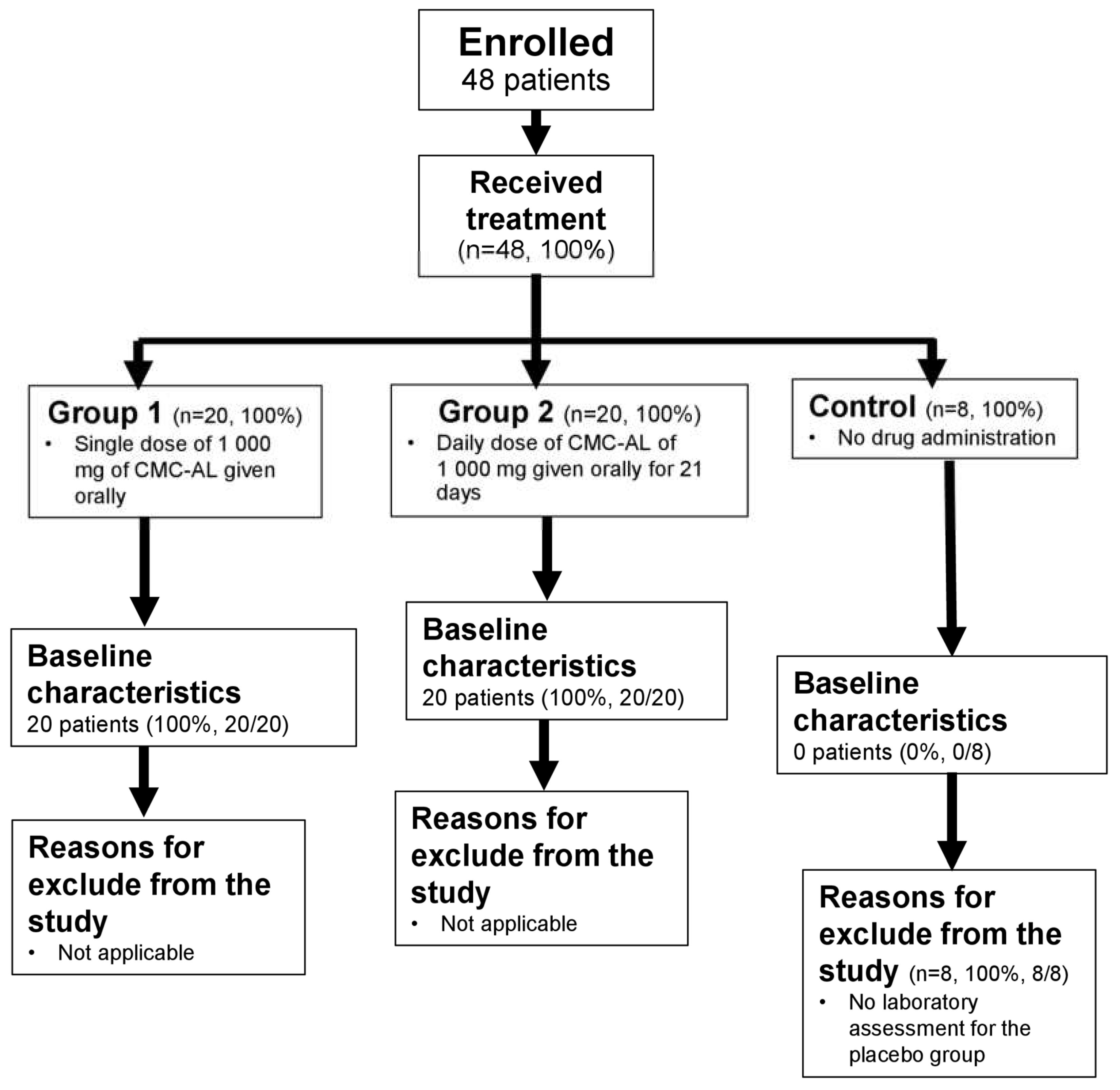
2.1. Healthy Subjects
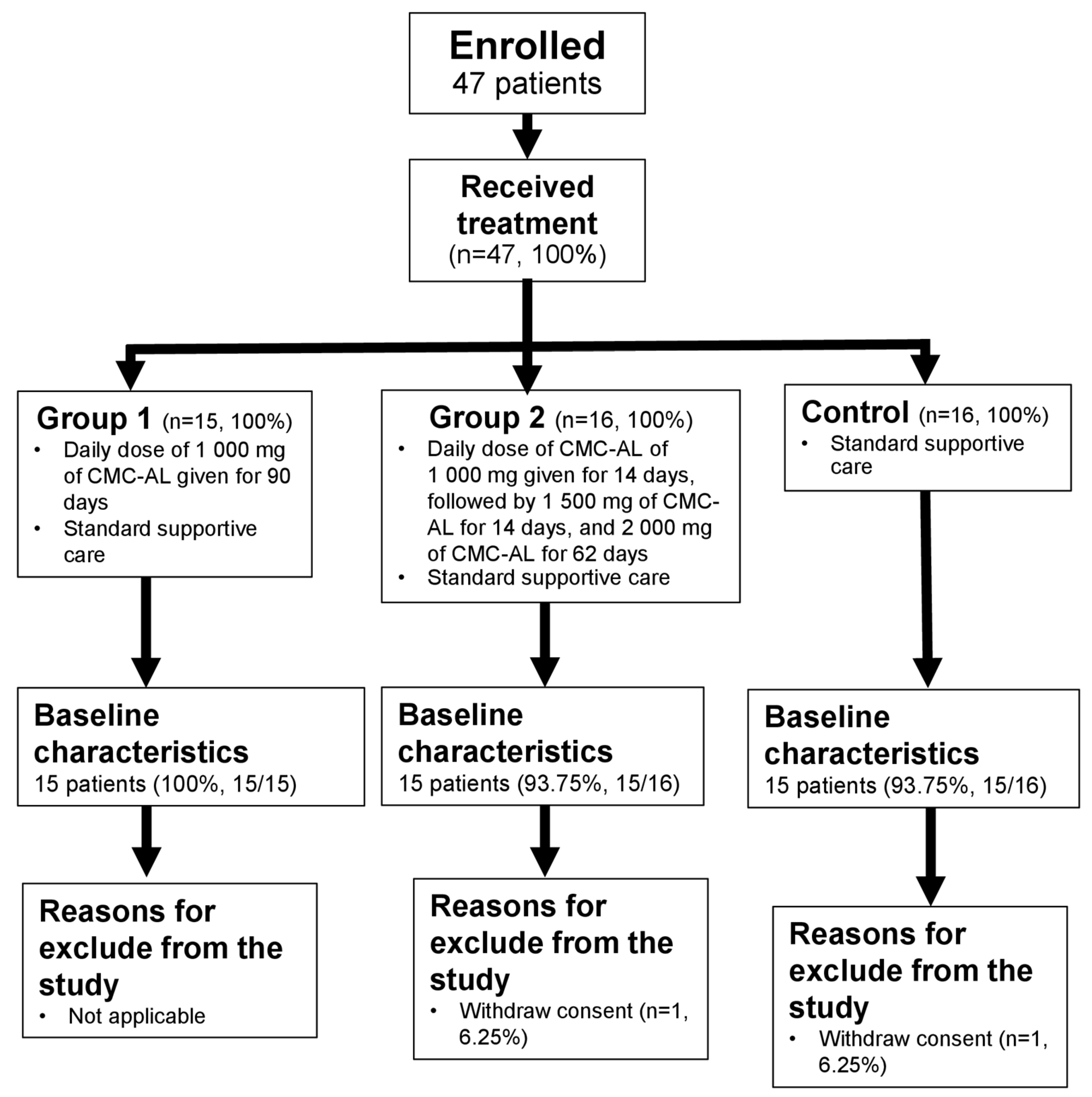
2.2. iCCA Patients
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Laboratory Procedures
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Interplay between Peripheral Blood Cytokines
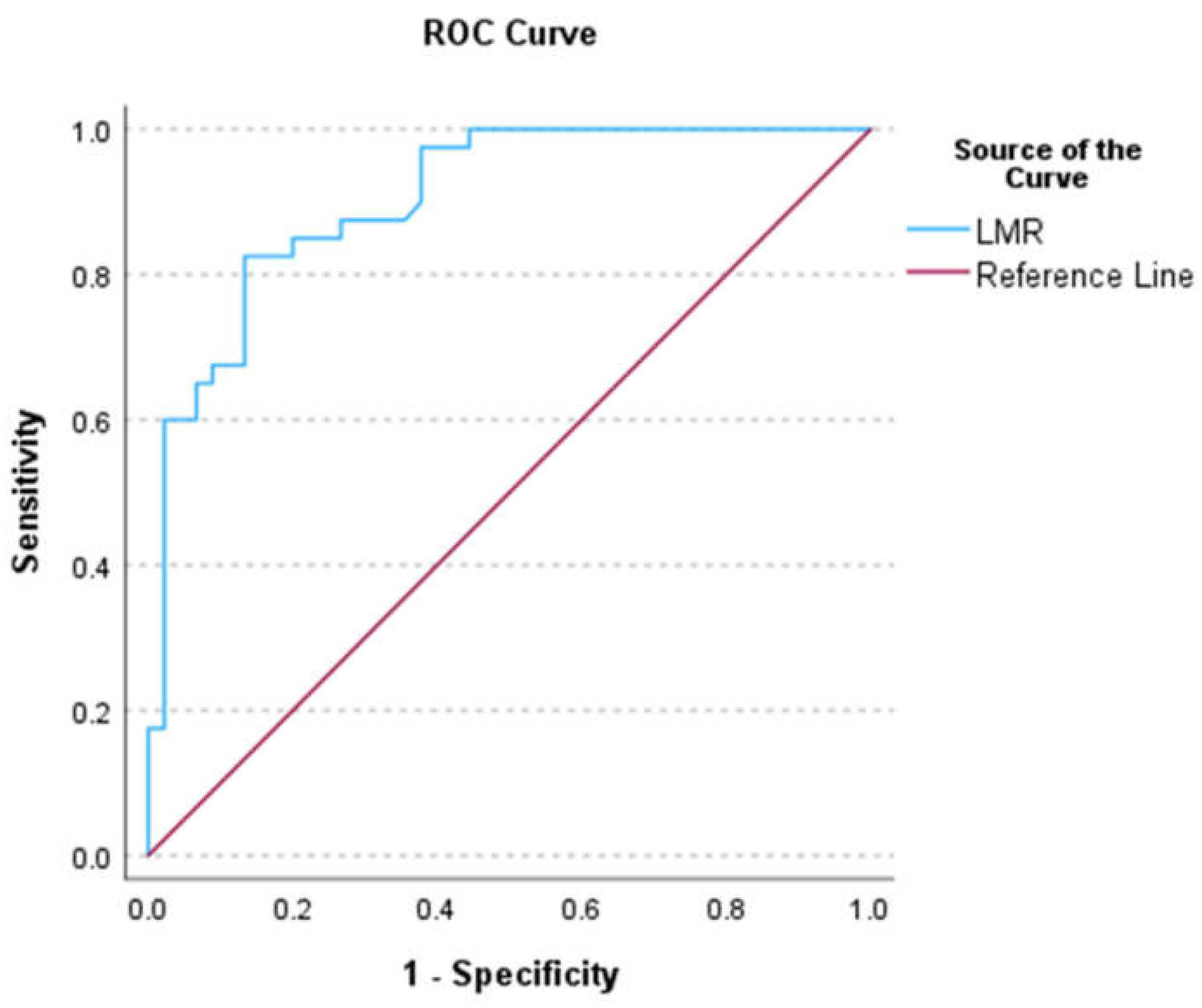
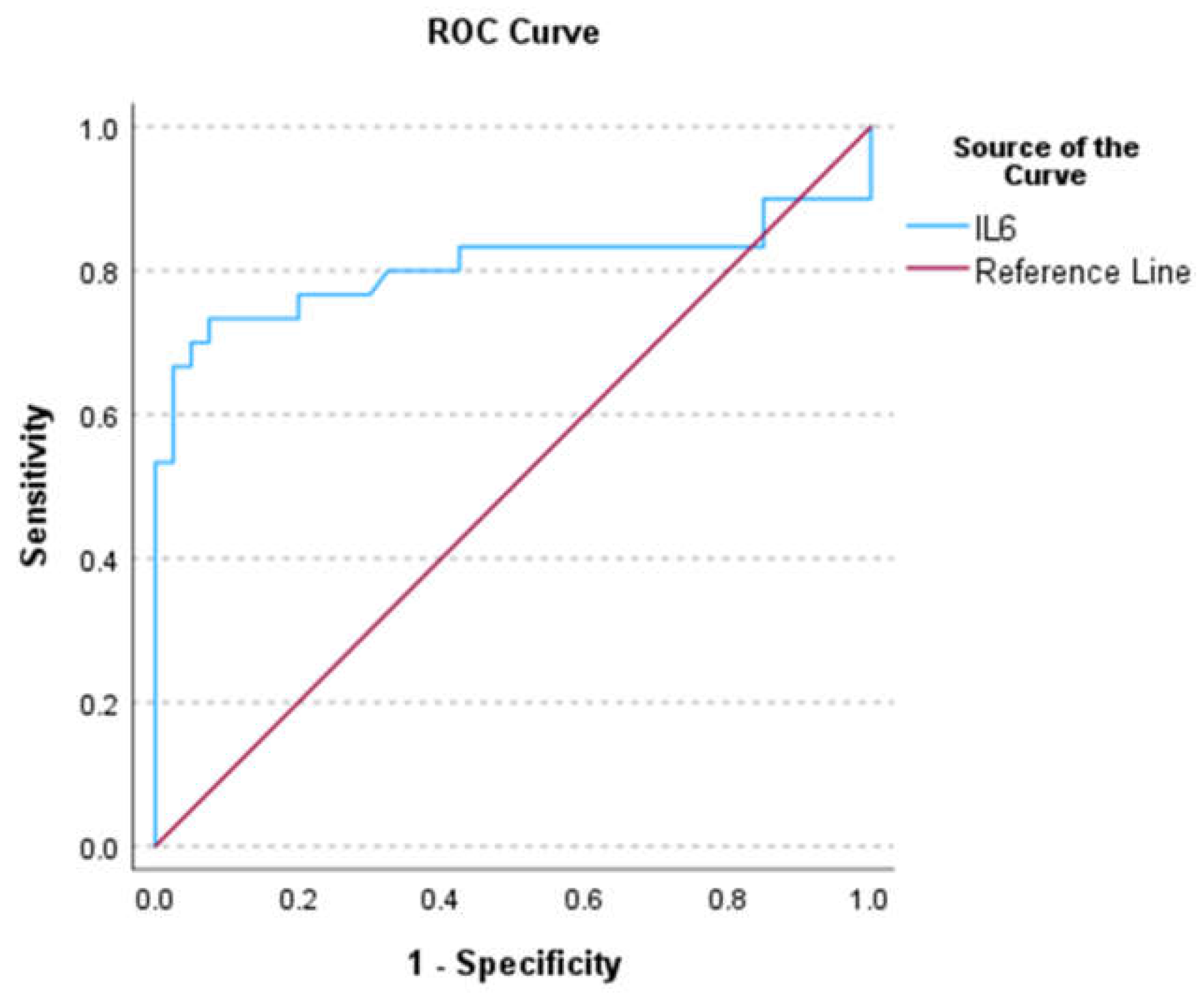
3.3. ROC Analysis
3.4. Univariate Analysis of Differential Peripheral Blood Indices and Serum Cytokines
3.5. Regression Analysis
3.6. Probability Risk of iCCA
4. Discussion
4.1. Peripheral Blood Indices
4.2. Demographic Data
4.3. Peripheral Cytokines
4.4. LMR and IL6 Are Potential Diagnostic Markers for iCCA
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Urban, O.; Vanek, P.; Zoundjiekpon, V.; Falt, P. Endoscopic Perspective in Cholangiocarcinoma Diagnostic Process. Gastroenterol. Res. Pract. 2019, 2019, 9704870. [Google Scholar] [CrossRef] [PubMed]
- Wongkham, S.; Silsirivanit, A. State of serum markers for detection of cholangiocarcinoma. Asian Pac. J. Cancer Prev. 2012, 13, 17–27. [Google Scholar] [PubMed]
- Kulma, I.; Panrit, L.; Plengsuriyakarn, T.; Chaijaroenkul, W.; Warathumpitak, S.; Na-Bangchang, K. A randomized placebo-controlled phase I clinical trial to evaluate the immunomodulatory activities of Atractylodes lancea (Thunb) DC. in healthy Thai subjects. BMC Complement. Med. Ther. 2021, 21, 61. [Google Scholar] [CrossRef]
- Na-Bangchang, K.; Tongsiri, N.; Plengsuriyakarn, T.; Sae-heng, T.; Kongjam, P.; Kulma, I.; Worrabannnakorn, S.; Karbwang, J. Phase II-a clinical trial to evaluate safety and efficacy of capsule formulation of the standardized extract of Atractylodes lancea (Thunb.) DC. in patients with advanced stage intrahepatic cholangiocarcinoma. J. Tradit. Complement. Med. 2023, in press. [Google Scholar]
- Wu, C.E.; Chou, W.C.; Hsieh, C.H.; Chang, J.W.; Lin, C.Y.; Yeh, C.N.; Chen, J.S. Prognostic and predictive factors for Taiwanese patients with advanced biliary tract cancer undergoing frontline chemotherapy with gemcitabine and cisplatin: A real-world experience. BMC Cancer 2020, 20, 422. [Google Scholar] [CrossRef]
- Sellers, C.M.; Uhlig, J.; Ludwig, J.M.; Stein, S.M.; Kim, H.S. Inflammatory markers in intrahepatic cholangiocarcinoma: Effects of advanced liver disease. Cancer Med. 2019, 8, 5916–5929. [Google Scholar] [CrossRef] [PubMed]
- Tsilimigras, D.I.; Moris, D.; Mehta, R.; Paredes, A.Z.; Sahara, K.; Guglielmi, A.; Aldrighetti, L.; Weiss, M.; Bauer, T.W.; Alexandrescu, S.; et al. The systemic immune-inflammation index predicts prognosis in intrahepatic cholangiocarcinoma: An international multi-institutional analysis. HPB 2020, 22, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Kim, N.Y.; Na, S.H.; Youn, Y.H.; Shin, C.S. Reference values of neutrophil-lymphocyte ratio, lymphocyte-monocyte ratio, platelet-lymphocyte ratio, and mean platelet volume in healthy adults in South Korea. Medicine 2018, 97, e11138. [Google Scholar] [CrossRef] [PubMed]
- Bai, Y.-Y.; Xi, Y.; Yin, B.-B.; Zhang, J.-H.; Chen, F.; Zhu, B. Reference intervals of systemic immune- inflammation index, neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio, and platelet-to-lymphocyte ratio during normal pregnancy in China. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 1033–1044. [Google Scholar] [CrossRef] [PubMed]
- Wongkham, S.; Chalermwat, C.; Silsirivanit, A.; Saentaweesuk, W.; Bhudisawasdi, V.; Pairojkul, C.; Khahmahpahte, S.; Thanong, T.; Changtrakul, Y.; Pintaraks, K.; et al. Neutrophil-to-Lymphocyte Ratio: A Systemic Inflammatory Index for Primary Diagnosis and Prognosis of Cholangiocarcinoma. Biomed. J. Sci. Tech. Res. 2019, 13, 8. [Google Scholar] [CrossRef]
- Miyahara, Y.; Takashi, S.; Shimizu, Y.; Ohtsuka, M. The prognostic impact of neutrophil-to-lymphocyte ratio (NLR) and lymphocyte-to-monocyte ratio (LMR) in patients with distal bile duct cancer. World J. Surg. Oncol. 2020, 18, 78. [Google Scholar] [CrossRef]
- Kitano, Y.; Yamashita, Y.-I.; Yamamura, K.; Arima, K.; Kaida, T.; Miyata, T.; Nakagawa, S.; Mima, K.; Imai, K.; Hashimoto, D.; et al. Effects of Preoperative Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios on Survival in Patients with Extrahepatic Cholangiocarcinoma. Anticancer Res. 2017, 37, 3229–3237. [Google Scholar] [CrossRef] [PubMed]
- Buettner, S.; Spolverato, G.; Kimbrough, C.W.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; et al. The impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio among patients with intrahepatic cholangiocarcinoma. Surgery 2018, 164, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Cuenco, J.; Wehnert, N.; Blyuss, O.; Kazarian, A.; Whitwell, H.J.; Menon, U.; Dawnay, A.; Manns, M.P.; Pereira, S.P.; Timms, J.F. Identification of a serum biomarker panel for the differential diagnosis of cholangiocarcinoma and primary sclerosing cholangitis. Oncotarget 2018, 9, 17430–17442. [Google Scholar] [CrossRef]
- Surapaitoon, A.; Suttiprapa, S.; Khuntikeo, N.; Pairojkul, C.; Sripa, B. Cytokine profiles in Opisthorchis viverrini stimulated peripheral blood mononuclear cells from cholangiocarcinoma patients. Parasitol. Int. 2017, 66, 889–892. [Google Scholar] [CrossRef]
- Kittirat, Y.; Suksawat, M.; Thongchot, S.; Padthaisong, S.; Phetcharaburanin, J.; Wangwiwatsin, A.; Klanrit, P.; Sangkhamanon, S.; Titapun, A.; Loilome, W.; et al. Interleukin-6-derived cancer-associated fibroblasts activate STAT3 pathway contributing to gemcitabine resistance in cholangiocarcinoma. Front. Pharmacol. 2022, 13, 897368. [Google Scholar] [CrossRef]
- Goydos, J.S.; Brumfield, A.M.; Frezza, E.; Booth, A.; Lotze, M.T.; Carty, S.E. Marked elevation of serum interleukin-6 in patients with cholangiocarcinoma: Validation of utility as a clinical marker. Ann. Surg. 1998, 227, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Liao, B.; Shen, W.; Sui, C.; Yang, J. Expression of Programmed Death Ligand 1 Is Associated with the Prognosis of Intrahepatic Cholangiocarcinoma. Dig. Dis. Sci. 2020, 65, 480–488. [Google Scholar] [CrossRef]
- Feng, K.; Liu, Y.; Zhao, Y.; Yang, Q.; Dong, L.; Liu, J.; Li, X.; Zhao, Z.; Mei, Q.; Han, W. Efficacy and biomarker analysis of nivolumab plus gemcitabine and cisplatin in patients with unresectable or metastatic biliary tract cancers: Results from a phase II study. J. Immunother. Cancer 2020, 8, e000367. [Google Scholar] [CrossRef] [PubMed]
- Rink, L.; Cakman, I.; Kirchner, H. Altered cytokine production in the elderly. Mech. Ageing Dev. 1998, 102, 199–209. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Y.; Su, M.; Liu, L.; Tang, Y.; Pan, Y.; Sun, J. Clinical Application of Cytokines in Cancer Immunotherapy. Drug Des. Dev. Ther. 2021, 15, 2269–2287. [Google Scholar] [CrossRef]
- Job, S.; Rapoud, D.; Dos Santos, A.; Gonzalez, P.; Desterke, C.; Pascal, G.; Elarouci, N.; Ayadi, M.; Adam, R.; Azoulay, D.; et al. Identification of Four Immune Subtypes Characterized by Distinct Composition and Functions of Tumor Microenvironment in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 72, 965–981. [Google Scholar] [CrossRef]
- Permpoon, U.; Khan, F.; Vadevoo, S.M.P.; Gurung, S.; Gunassekaran, G.R.; Kim, M.-J.; Kim, S.-H.; Thuwajit, P.; Lee, B. Inhibition of Tumor Growth against Chemoresistant Cholangiocarcinoma by a Proapoptotic Peptide Targeting Interleukin-4 Receptor. Mol. Pharm. 2020, 17, 4077–4088. [Google Scholar] [CrossRef] [PubMed]
- Thepmalee, C.; Panya, A.; Junking, M.; Chieochansin, T.; Yenchitsomanus, P.-T. Inhibition of IL-10 and TGF-β receptors on dendritic cells enhances activation of effector T-cells to kill cholangiocarcinoma cells. Hum. Vaccines Immunother. 2018, 14, 1423–1431. [Google Scholar] [CrossRef]
- Li, W.; Wu, F.; Zhao, S.; Shi, P.; Wang, S.; Cui, D. Correlation between PD-1/PD-L1 expression and polarization in tumor-associated macrophages: A key player in tumor immunotherapy. Cytokine Growth Factor Rev. 2022, 67, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Fourcade, J.; Pagliano, O.; Chauvin, J.M.; Sander, C.; Kirkwood, J.M.; Zarour, H.M. IL10 and PD-1 Cooperate to Limit the Activity of Tumor-Specific CD8+ T Cells. Cancer Res. 2015, 75, 1635–1644. [Google Scholar] [CrossRef] [PubMed]
- Zhao, S.; Wu, D.; Wu, P.; Wang, Z.; Huang, J. Serum IL-10 Predicts Worse Outcome in Cancer Patients: A Meta-Analysis. PLoS ONE 2015, 10, e0139598. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Li, Z.; Hu, G. Prognostic role of intratumoral IL-17A expression by immunohistochemistry in solid tumors: A meta-analysis. Oncotarget 2017, 8, 66382–66391. [Google Scholar] [CrossRef] [PubMed]
- Lotti, F.; Jarrar, A.M.; Pai, R.K.; Hitomi, M.; Lathia, J.; Mace, A.; Gantt, G.A., Jr.; Sukhdeo, K.; DeVecchio, J.; Vasanji, A.; et al. Chemotherapy activates cancer-associated fibroblasts to maintain colorectal cancer-initiating cells by IL-17A. J. Exp. Med. 2013, 210, 2851–2872. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, J.; Herjan, T.; Hong, L.; Liao, Y.; Liu, C.; Vasu, K.; Wang, H.; Thompson, A.; Fox, P.L.; et al. IL-17-induced HIF1α drives resistance to anti-PD-L1 via fibroblast-mediated immune exclusion. J. Exp. Med. 2022, 219, e20210693. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lu, Q.; Zhang, W.; Cao, J.; Dong, Y.; Wang, W. Preoperative Differentiation of Combined Hepatocellular-Cholangiocarcinoma from Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: A Nomogram Based on Ultrasonographic Features and Clinical Indicators. Front. Oncol. 2022, 12, 757774. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.F.; Chen, Z.H.; Wei, L.; Ma, X.K.; Li, X.; Wen, J.Y.; Wang, T.-T.; Cai, X.-R.; Wu, D.-H.; Chen, J.; et al. Identification of the prognostic value of lymphocyte-to-monocyte ratio in patients with HBV-associated advanced hepatocellular carcinoma. Oncol. Lett. 2017, 14, 2089–2096. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Zeng, F.; Yao, L.; Fang, T.; Liao, M.; Long, J.; Xiao, L.; Deng, G. Nomogram based on inflammatory indices for differentiating intrahepatic cholangiocarcinoma from hepatocellular carcinoma. Cancer Med. 2020, 9, 1451–1461. [Google Scholar] [CrossRef] [PubMed]
- Felkle, D.; Jarczyński, M.; Kaleta, K.; Zięba, K.; Nazimek, K. The immunomodulatory effects of antihypertensive therapy: A review. Biomed. Pharmacother. 2022, 153, 113287. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Healthy Individuals (n = 40) | Patients (n = 45) |
|---|---|---|
| Gender | Male: 20; Female: 20 | Male: 24; Female: 21 |
| Age (years) | 22.5 (19–43) | 65.5 (45–84) |
| BMI | 22.88 (18.47–26.78) | 22.02 (13.03–28.03) |
| Body temperature (°C) | 36.5 (35.7–37.6) | 36.6 (36–37.2) |
| Concomitant medication | ||
| Antihypertensive (enalapril, amlodipine, spironolactone, furosemide, lercannidine, losartan, and doxazosin), Dyslipidemia (simvastatin), Antibiotics (cefixime, ciproflex, and metronidazole), Antidiabetics (metformin), Analgesics (tramadol, paracetamol, and morphine), Antihistamine (dimenhydrinate), Others (morphine, omeprazole, domperidone/Gabapentin/Amitryptiline, and senoside) | ||
| NO | - | 35 |
| PT (seconds) | 11.6 (±0.72) * | 13.49 (±1.66) * |
| INR | 0.98 (±0.06) * | 1.15 (±0.15) * |
| PTT (seconds) | 26.95(22.3–31.8) | 29.4 (8.7–35.9) |
| Creatinine (mg/dL) | 0.86 (0.5–1.11) | 0.89 (0.5–1.98) |
| BUN (mg/dL) | 10.2 (5.4–19.7) | 13.55 (0.5–31) |
| BUN/Cr ratios | 13.66 (7.01–31.77) | 15.04 (1–30.78) |
| AST (IU/L) | 14 (7–32) | 37.5 (13–98) |
| ALT (IU/L) | 30 (16–68) | 28 (11–98) |
| Direct bilirubin (mg/dL) | 0.2 (0.1–0.3) | 0.2 (0.1–3.5) |
| Total bilirubin (mg/dL) | 0.6 (0.2–1.5) | 0.65 (0.2–8) |
| Total protein (g/dL) | 7.9 (7.2–8.8) * | 8.06 (±0.71) * |
| Albumin (g/dL) | 4.2 (3.4–4.9) | 3.28 (3.04–3.52) |
| CEA (ng/mL) | - | 6.1 (0.5–1111.30) |
| CA19–9 (ng/mL) | - | 116 (0.5–140,000) |
| NLR | 1.55 (±0.45) * | 3.22 (0.84–15.16) |
| LMR | 10.10 (4.48–18.26) | 3.8 (1–14.90) |
| PLR | 117.87 (±33.43) * | 161.85 (10.12–623.79) |
| SIII (×109/L) | 370.36 (189.37–691.11) | 918.86 (42.5–6354.83) |
| IFN-ꝩ (pg/mL) | 9.85 (4.4–20.48) | 0 (0–3.44) |
| TNF-α (pg/mL) | 6.82 (±1.38) * | 0 (0–4.54) |
| IL2 (pg/mL) | 8.49 (0–25.56) | 0 (0–5.38) |
| IL4 (pg/mL) | 4.27 (0–14.25) | 0.02 (0–2.02) |
| IL6 (pg/mL) | 8.45 (5.08–19.39) | 20.91 (3–119.51) |
| IL10 (pg/mL) | 5.91 (2.06–8.63) | 1.75 (0–7.15) |
| IL17A (pg/mL) | 75.55 (27.61–214.62) | 0 (0–33.37) |
| Cytokines | IL2 | IL4 | IL10 | IL17A | TNF-α | IFN-γ |
|---|---|---|---|---|---|---|
| AUC [median (min–max)] | 0.91 (0.84–0.98) | 0.84 (0.75–0.93) | 0.93 (0.86–0.99) | 0.99 (0.99–1.0) | 0.99 (0.99–1.0) | 0.99 (0.99–1.0) |
| Sensitivity | 0.82 | 0.74 | 0.74 | 0.97 | 0.97 | 1.0 |
| Specificity | 0.97 | 0.97 | 0.97 | 0.98 | 0.98 | 0.98 |
| PPV | 0.96 | 0.97 | 0.97 | 0.97 | 0.97 | 0.97 |
| NPV | 0.85 | 0.74 | 0.75 | 0.98 | 0.98 | 1 |
| AI | 0.9 | 0.84 | 0.84 | 0.97 | 0.97 | 0.98 |
| YI | 0.8 | 0.71 | 0.71 | 0.94 | 0.94 | 0.97 |
| Cut-off value for risk of iCCA (pg/mL) | <3.24 | <1.89 | <4.66 | <28.10 | <4.47 | <2.21 |
| OR ratios [Mean ± 95%CI] | 183.7 (24.24–1911, p < 0.001) | 77.33 (12.21–813.1, p < 0.001) | 50 (11.92–161.9, p < 0.001) | 1247 (79.50–12,511) | 1247 (79.50–12,511) | ∞ |
| Risk Level | LMR | IL6 (pg/mL) |
|---|---|---|
| Low risk | >7.18 | <8.8 |
| Intermediate risk | 5.78–7.18 | 8.8–15.94 |
| High risk | 3.38–5.77 | 15.93–21.83 |
| Very high risk | 1–3.38 | >21.83 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeheng, T.; Karbwang, J.; Na-Bangchang, K. Interleukin-6 and Lymphocyte-to-Monocyte Ratio Indices Identify Patients with Intrahepatic Cholangiocarcinoma. Biomedicines 2024, 12, 844. https://doi.org/10.3390/biomedicines12040844
Saeheng T, Karbwang J, Na-Bangchang K. Interleukin-6 and Lymphocyte-to-Monocyte Ratio Indices Identify Patients with Intrahepatic Cholangiocarcinoma. Biomedicines. 2024; 12(4):844. https://doi.org/10.3390/biomedicines12040844
Chicago/Turabian StyleSaeheng, Teerachat, Juntra Karbwang, and Kesara Na-Bangchang. 2024. "Interleukin-6 and Lymphocyte-to-Monocyte Ratio Indices Identify Patients with Intrahepatic Cholangiocarcinoma" Biomedicines 12, no. 4: 844. https://doi.org/10.3390/biomedicines12040844
APA StyleSaeheng, T., Karbwang, J., & Na-Bangchang, K. (2024). Interleukin-6 and Lymphocyte-to-Monocyte Ratio Indices Identify Patients with Intrahepatic Cholangiocarcinoma. Biomedicines, 12(4), 844. https://doi.org/10.3390/biomedicines12040844