Abstract
Once-weekly semaglutide is a widely used glucagon-like peptide-1 receptor agonist (GLP-1RA) used for the treatment of type 2 diabetes (T2D). In clinical trials, semaglutide improved glycemic control and obesity, and reduced major cardiovascular events. However, the reports are limited on its real-world efficacy relating to various metabolic factors such as dyslipidemia or metabolic dysfunction-associated steatotic liver disease (MASLD) in Asian patients with T2D. In our retrospective longitudinal study, we selected patients with T2D who were given once-weekly semaglutide and compared metabolic parameters before and after the start of semaglutide. Seventy-five patients were eligible. HbA1c decreased significantly, by 0.7–0.9%, and body weight by 1.4–1.7 kg during the semaglutide treatment. Non-HDL cholesterol decreased significantly at 3, 6 and 12 months after the initiation of semaglutide; LDL cholesterol decreased at 3 and 6 months; and HDL cholesterol increased at 12 months. The effects on body weight, HbA1c and lipid profile were pronounced in patients who were given semaglutide as a first GLP-1RA (GLP-1R naïve), whereas improvements in HbA1c were also observed in patients who were given semaglutide after being switched from other GLP-1RAs. During a 12-month semaglutide treatment, the hepatic steatosis index (HSI) tended to decrease. Moreover, a significant decrease in the AST-to-platelet ratio index (APRI) was observed in GLP-1RA naïve patients. Our real-world study confirmed the beneficial effects of once-weekly semaglutide, namely, improved body weight, glycemic control and atherogenic lipid profile. The beneficial effects on MASLD were also suggested.
1. Introduction
The global prevalence of diabetes is estimated to be 463 million people, rising to 578 million by 2030 [1], and more than 60% of people with diabetes live in Asia [2]. Obesity is a major driver of the epidemic of type 2 diabetes (T2D) [3], and the presence of T2D is associated with an elevated risk of cardiovascular (CV) diseases in the Asian population [4,5]. Interventions against multiple CV risk factors, such as diabetes, dyslipidemia, hypertension and obesity, can play a key role in the prevention of CV diseases [6].
Obesity and T2D also relate to the development and progression of metabolic dysfunction-associated steatotic liver disease (MASLD), which comprises simple steatosis, metabolic dysfunction-associated steatohepatitis (MASH), fibrosis/cirrhosis, and hepatocellular carcinoma [7]. The progression of MASLD is not only a risk factor for liver-related death but also for CV diseases and T2D comorbidities such as chronic kidney disease [8,9]. Preventing MASLD progression is considered one of the important factors in diabetic treatments.
Glucagon-like peptide-1 (GLP-1) is an intestinal hormone that stimulates insulin secretion and inhibits glucagon secretion from pancreatic islets. GLP-1 receptor agonists (GLP-1RAs) have been demonstrated to improve glycemic control and reduce body weight in various clinical trials [10,11]. Our previous study of once-weekly dulaglutide showed positive effects of GLP-1RAs on various metabolic factors such as dyslipidemia, blood pressure and liver dysfunction [12]. Once-weekly semaglutide is a subcutaneous GLP-1RA, and widely used for the treatment of T2D. In a randomized controlled study, the use of once-weekly semaglutide was associated with a lower incidence of CV events in patients with T2D who were at high CV risk [13]. Comparisons of previous clinical studies suggested that once-weekly semaglutide could have stronger effects in lowering glucose levels or body weight [14]. Nevertheless, most of the insights on semaglutide are based on clinical trials conducted mainly in Western regions, and only a limited number of reports have studied the real-world effects of once-weekly semaglutide on various metabolic factors in Asian patients with T2D, a group characterized by relatively lower body mass index (BMI) and a more severe insulin secretion deficiency [15]. This study aimed to examine the real-world efficacy of once-weekly semaglutide on various CV risk factors and MASLD in Japanese patients with T2D.
2. Materials and Methods
2.1. Study Population
The retrospective longitudinal study based on medical charts was conducted at the National Center for Global Health and Medicine, Kohnodai Hospital, Japan. We enrolled patients with T2D who had been prescribed once-weekly semaglutide for at least 3 months or longer between 1 June 2020 and 30 June 2022. We excluded the patients who did not visit our hospital regularly. The patients for whom semaglutide prescription was suspended within 3 months were also excluded from the analysis.
2.2. Data Collection
We collected the relevant data on various metabolic factors, including results from blood tests and urine tests and anthropometric parameters, and compared the data before and after the initiation of semaglutide treatment. Information on concomitant treatments was also collected from medical charts. Body weight, height, waist circumference and blood pressure were measured according to the clinical standards. Body mass index (BMI) was calculated by dividing body weight in kilograms by body height squared in meters. The measurements of serum hemoglobin A1c (HbA1c), total cholesterol (TC), triglyceride (TG), creatinine, and uric acid were performed using enzymatic assays. The hexokinase method was indicated for the evaluation of plasma glucose. A direct method was used for the measurements of serum low-density lipoprotein cholesterol (LDL-C) and HDL-C. Serum transaminases, including aspartate aminotransferase (AST), alanine aminotransferase (ALT) and γ-glutamyl transferase (GGTP) were measured using the Japan Society of Clinical Chemistry transferable method. A turbidimetric immunoassay was used for the measurement of urinary albumin, and the albumin-to-creatinine ratio (UACR) was calculated. UACR stage (A1–A3) was determined based on the Kidney Disease Improving Global Outcomes (KDIGO) risk categories [16]. The estimated glomerular filtration rate (eGFR) was calculated by age and serum creatinine based on the estimation equation for Japanese patients [17]. Non-HDL-C was calculated by subtracting HD-C from TC. The hepatic steatosis index (HSI) was calculated using the following formula: 8 × (ALT/AST) + BMI + (2, if diabetes mellitus) + (2, if female) [18]. The AST-to-platelet ratio index (APRI) and fibrosis -4 (FIB-4) index are markers for hepatic fibrosis. The APRI was calculated as follows: AST (IU/L)/Upper limit of the normal range of AST: 40 (IU/L)/Platelet count (109/L) × 100 [19]. FIB-4 index was calculated as follows: (age × AST)/(platelet counts (×109/L) × (ALT)1/2 [20,21].
2.3. Statistical Analysis
Data obtained in this study were tested for normality using the Shapiro–Wilk test. Comparisons of the variables with normal distribution were analyzed by paired t-tests. Variables without normal distribution were compared using the Wilcoxon signed-rank test. Spearman’s rank correlation coefficient was used to determine the correlations between the parameters. Missing data were excluded from analyses. All data are expressed as mean ± SD, and p < 0.05 was considered to be statistically significant. We used SPSS version 29 (IBM Corp, Armonk, NY, USA) for statistical analysis.
3. Results
3.1. Characteristics of Patients
During the observation period, 83 patients were prescribed once-weekly semaglutide. In five patients, semaglutide prescription was suspended, due to either injection-site pain (n = 3), gastrointestinal symptoms (n = 1) or unavailability due to supply shortage (n = 1). Three patients were excluded due to lack of regular visits to our hospital. Thus, we examined 75 patients in this study. All patients were under standard care, including recommendations for diet and physical activities according to the guidelines of the Japan Diabetes Society.
Table 1 shows the baseline characteristics of the patients. The mean age of the patients was 55.8 ± 13.3 years, and the mean BMI was 31.4 ± 5.2 kg/m2. A total of 36 patients were prescribed semaglutide as a first GLP-1RA (GLP-1RA naïve). Thirty-nine patients were given semaglutide switched from other GLP-1RAs (thirty patients from once-weekly dulaglutide 0.75mg, five patients from once-daily liraglutide 0.9 mg, and one patient from oral semaglutide 3mg). In 16 patients, DPP-4 inhibitors were switched to semaglutide. Among hypoglycemic agents, for the most part, SGLT2 inhibitors (SGLT2is) were used (91%), followed by metformin (69%) and Thiazolidinedione (24%). Insulin was used in 13 patients (17%). Angiotensin II receptor blockers (ARB) were used in 38 patients (51%) and calcium channel blockers in 35 patients (47%). Statins were given for 44 patients (59%). Antiplatelet drugs were prescribed in 14 patients (19%).

Table 1.
The baseline characteristics of the patients (n = 75).
The initial dose of once-weekly semaglutide was 0.25 mg in 68 patients. In seven patients who were given semaglutide switched from other GLP1Ras, semaglutide was started at 0.5 mg. At 3 months after the initiation of semaglutide, the doses of semaglutide were 0.25 mg in sixteen patients, 0.5 mg in fifty-seven patients and 1.0 mg in two patients. At 6 months, seven patients received semaglutide at 0.25 mg, forty-one patients at 0.5 mg and six patients at 1.0 mg. At 12 months, semaglutide was given at 0.25 mg in three patients, 0.5 mg in twenty-seven patients and 1.0 mg in ten patients.
3.2. Changes in Metabolic Parameters during Semaglutide Treatment
Table 2 provides the changes in metabolic parameters during semaglutide treatments. Overall, HbA1c decreased significantly, by 0.7–0.9%, and body weight by 1.4–1.7 kg. Improvements in lipid profile were also observed. There were significant decreases in non-HDL-C at 3, 6 and 12 months, LDL-C at 3 and 6 months and TG at 12 months. HDL-C increased at 12 months. AST and ALT decreased at 3, 6 and 12 months and GGTP decreased at 3 months. There were no significant changes in eGFR and UACR. The mean eGFR slope was calculated as 0.55 mL/min/1.73 m2/year.
Table 2.
The changes in metabolic parameters during the semaglutide treatment in all patients.
Figure 1 shows the changes in body weight, HbA1c, AST and non-HDL-C in patients who were continuously prescribed semaglutide for 12 months. Body weight, HbA1c and AST decreased at 3 months after the initiation of semaglutide and maintained these significant differences until the 12-month point.
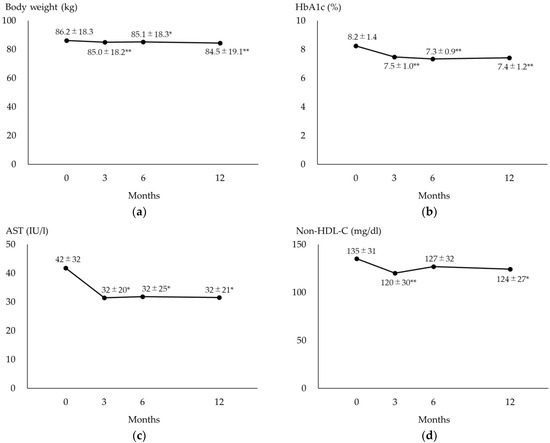
Figure 1.
Changes in measured values in patients who were continuously prescribed semaglutide for 12 months. (a) The changes in body weight during the 12-month semaglutide treatment. (b) The changes in HbA1c during the 12-month semaglutide treatment. (c) The changes in AST during the 12-month semaglutide treatment. (d) The changes in non-HDL-C during the 12-month semaglutide treatment. * p < 0.05 vs. baseline, ** p < 0.01 vs. baseline. Values show mean ± SD. AST, aspartate aminotransferase; HbA1c, hemoglobin A1c; HDL-C, high-density lipoprotein cholesterol.
3.3. Changes in Metabolic Parameters in GLP-1 RA Naïve Patients or Patients Given Semaglutide Switched from Other GLP-1RAs
We compared the patients who were given semaglutide as a first GLP-1RA (Group A) with those switched from other GLP-1RAs (Group B) at 12 months after the initiation of semaglutide (Table 3). In group B, there were significant decreases in HbA1c, by 0.5%. Body weight and BMI also tended to decrease. Nevertheless, there were no significant changes in liver transaminases and serum lipids, except for HDL-C. In group A, a significant decrease was observed in HbA1c, of 1.3%, and there was the same tendency in body weight, by 2.0 kg. There were significant improvements in non-HDL-C at 12 months. Moreover, AST, ALT and GGTP decreased significantly. Overall, the results at 3 and 6 months after the initiation of semaglutide resembled were similar to those at 12 months (Table S1).
Table 3.
The changes in metabolic parameters during the 12-month semaglutide treatment in patients who were GLP-1RA naïve or given semaglutide switched from other GLP-1RAs.
3.4. Changes in MASLD Indices during 12-Month Semaglutide Treatment
Table 4 provides the changes in MASLD indices at 12 months after the initiation of semaglutide treatment. There was a tendency towards a decrease in HSI, whereas the APRI and FIB4-index showed no significant changes (Table 4a).
Table 4.
The changes in the indices of MASLD during the 12-month semaglutide treatment.
In patients given semaglutide switched from other GLP-1RAs (Group B), there were no differences in the HSI, APRI or FIB-4 index (Table 4 (b)). In GLP-1RA naïve patients (Group A), the APRI was improved significantly, and the HSI and FIB-4 index also tended to decrease.
To elucidate the effects of semaglutide in patients in the presence of liver damage, we divided the patients into groups according to the baseline values of ALT levels. In patients with a higher degree of liver damage (baseline ALT ≥ 30 IU/L), there was a significant decrease in the APRI and the FIB-4 index, whereas the APRI and FIB-4 index increased significantly in patients with a baseline ALT < 30 (Table 4c).
We also divided the patients into groups according to baseline LDL-C levels (Table 4d). The HSI showed a significant decrease only in patients with higher LDL-C levels (Baseline LDL-C ≥ 100 mg/dL). Moreover, we examined the changes in MASLD indices in patients divided by concomitant use of statins and ARB (Table 4e,f). The HSI decreased significantly in patients with statins or ARB, whereas there were no significant changes in the APRI or FIB-4 index.
3.5. Correlations between the Baseline and the Changes in MASLD Indices
Figure 2 shows the correlations between the baseline values and the changes in MASLD indices during 12-month semaglutide treatment. Significant correlations were found between the baseline values and changes in HSI (R = −0.332, p = 0.036), FIB-4 index (R = −0.333, p = 0.047) and APRI (R = −0.417, p = 0.007).
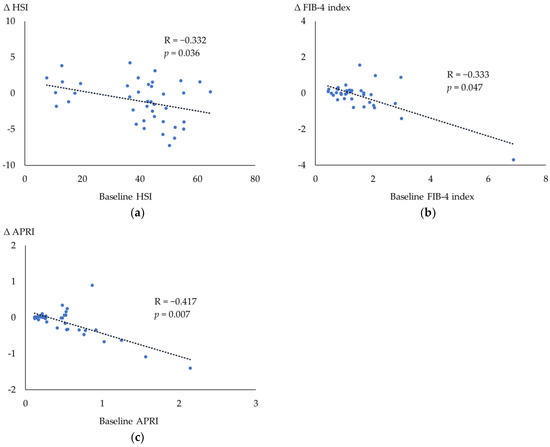
Figure 2.
Spearman’s rank correlation coefficient among the parameters during the 12 months after the initiation of semaglutide. (a) The correlation between the changes in the HSI and the baseline HSI. (b) The correlation between the changes in the FIB-4 index and the baseline FIB-4 index. (c) The correlation between the changes in the APRI and the baseline. APRI. APRI, AST-to-platelet ratio index; AST, aspartate aminotransferase; FIB-4 index, fibrosis-4 index; HSI, hepatic steatosis index.
3.6. Correlations among the Changes in Metabolic Parameters
Table 5 provides the correlations between the changes in metabolic parameters during the 12 months of semaglutide treatment. The changes in the HSI were correlated with the changes in BMI (R = 0.536, p = 0.002), but not correlated with the changes in HbA1c (R = −0.002, p = 0.991). There were significant correlations between the changes in HbA1c and the changes in the FIB-4 index (R = 0.511, p = 0.001) and the APRI (R = 0.494, p = 0.001), whereas the changes in BMI were not correlated with the changes in the FIB-4 index and APRI.
Table 5.
Spearman’s rank correlation coefficient among the changes in metabolic parameters during the 12-month semaglutide treatment. (* p < 0.05, ** p < 0.01).
3.7. Changes in UACR Stages during 12-Month Semaglutide Treatment
Table 6 shows the changes in the UACR stage between baseline and 12 months after the initiation of semaglutide treatment. Remission in the UACR stage was observed in five patients (A2–A1: 3 patients, A3–A2: 2 patients), whereas deterioration was observed in one patient.
Table 6.
The changes in the UACR stage in patients who were prescribed semaglutide for 12 months.
4. Discussion
In this real-world study, treatment with once-weekly semaglutide reduced body weight and improved hyperglycemia and atherogenic dyslipidemia in Japanese patients with T2D. It was also suggested that semaglutide had beneficial effects on preventing the progression of MASLD in high-risk patients.
Clinical trials already provided consistent evidence of the effects of the weekly semaglutide as to improvements in obesity and glycemic control. In Japanese patients with T2D, semaglutide treatment at a dose of 0.5 mg or 1.0 mg reduced HbA1c by 1.7–2.2% and body weight by 1.4 kg–3.9 kg [10,11]. Our real-world data confirmed the improvements in glycemic control and body weight associated with once-weekly semaglutide. However, the degrees of the changes in HbA1c and body weight were smaller. Compared to the clinical trials, most of the patients in our study had already been treated with other anti-diabetic agents such as SGLT2is or metformin. Moreover, our data included the patients who had been given other GLP-1RAs before the initiation of semaglutide. As shown in Table 3, the changes in HbA1c and body weight were greater in GLP-1RA naïve patients. A real-world study examining the effects of once-weekly semaglutide in Japanese patients reported changes in HbA1c and body weight similar to those observed in the present study [22]. Furthermore, our study demonstrated the multifactorial benefits of semaglutide against CV risk factors.
Once-weekly semaglutide has already been suggested to have stronger effects on improving glycemic control and obesity, compared with other GLP-1Ras, in a comparison of clinical trials [14]. Direct comparisons of once-weekly semaglutide and dulaglutide revealed the pronounced glucose-lowering and body-mass-index-lowering effects of semaglutide in Japanese patients with T2D [23,24]. Switching from liraglutide to once-weekly semaglutide also resulted in significant improvements in HbA1c and body weight, despite no significant changes being observed in patients given dulaglutide who had switched from liraglutide [25]. Our results also revealed a significant improvement in HbA1c as well as a tendency towards a decrease in body weight, even in patients who had been given other GLP-1RAs before the initiation of once-weekly semaglutide, which confirmed the stronger effects of once-weekly semaglutide on glycemia and body weight in the real world. Compared with the average BMI of around 24 kg/m2 [26], the patients in our study had higher BMI and coexisting metabolic disorders, including dyslipidemia and hypertension, suggesting that in clinical practice, once-weekly semaglutide was preferably prescribed for obese patients with a higher risk for CV diseases.
Insulin resistance is a common feature of T2D, dyslipidemia and MASLD. MASLD is characterized by the liver’s accumulation of TG, which is synthesized from fatty acyl coenzyme A (CoA). The concentration of fatty acyl CoA in the liver depends on the balance of the formation and utilization of free fatty acid. When the formation of FFAs from circulating FFAs, de novo lipogenesis, lipoprotein uptake and TG breakdown exceed lipid synthesis and oxidation, the fatty acyl CoA concentration rises, resulting in the accumulation of TG. Insulin resistance in adipose tissue activates hormone-sensitive lipase, which, in turn, promotes lipolysis and the release of FFA and proinflammatory cytokines which aggravate insulin resistance [7,27,28]. Circulating FFA levels are further augmented by dietary lipids, resulting in an increased influx of FFA into the liver, which, in turn, inhibits the degradation of apolipoprotein B 100 and promotes TG-rich, very low-density lipoprotein (VLDL) secretion, weheras the TG export is insufficient to normalize the hepatic TG content. De novo lipogenesis in the liver is also elevated by hyperinsulinemia resulting from insulin resistance, leading to further production of FFA and VLDL. Lipid overload in the liver increases mitochondrial beta-oxidation and TCA cycle activity, which can potentially induce oxidative stress, promoting liver damage and the progression of fibrosis. GLP-1RAs induce postprandial insulin secretion and improve insulin resistance, which inhibits lipolysis and FFA release in adipose tissue. The reduction of FFA release to the bloodstream results in decreased FFA influx to the liver. GLP-1RAs can also inhibit hepatic de novo lipogenesis and VLDL-TG secretion [29]. These effects of GLP-1RAs can lead to a reduction in hepatic TG content and improvements in atherogenic lipid profiles.
We used the HSI, APRI and FIB-4 index for the evaluation of MASLD. A previous study revealed the usefulness of the HSI for the detection of non-alcoholic fatty liver disease (NAFLD) [18]. It was also reported that the APRI and FIB-4 index were associated with the degree of hepatic fibrosis and the outcome of NAFLD [30,31,32,33]. Although the fatty liver index is also frequently used for the assessments of hepatic steatosis [34], it was impossible to use it for our study, since the regular measurements of waist circumference were not common in clinical practice in Japan. It should also be noted that there are few reports assessing the association between these indices and the severity or outcome of newly defined MASLD.
In our study, once-weekly semaglutide reduced the hepatic steatosis index. The attenuation of liver fat accumulation by semaglutide was also reported in a study using magnetic resonance imaging [35]. There was also a significant improvement in the APRI and the same tendency was seen in the FIB-4 index in GLP-1RA naïve patients in our study, suggesting the possible effects of once-weekly semaglutide, not only on hepatic steatosis, but also on hepatic fibrosis. The associations between the baseline values and changes in the APRI and FIB-4 index suggested that semaglutide can improve hepatic fibrosis in patients with advanced fibrosis at baseline. A randomized controlled study reported that 72 weeks of semaglutide yielded more patients with MASH resolution compared with placebo, nevertheless, there was no difference in the improvement of the fibrosis stage [36]. Interestingly, significant associations were observed between the changes in HbA1c and the changes in the APRI or FIB-4 index in our study, suggesting that enhanced insulin action may be a common mechanism in improving glycemic control and preventing the development of liver fibrosis.
SGLT2is, metformin, pioglitazone, statins and ARB have been reported to have beneficial effects on the progression of MASLD [37,38,39,40,41,42,43]. Thus, our results might be influenced by these concomitant agents. In our sub-analysis, the HSI decreased significantly only in patients with statins or ARB but not in patients without these drugs. According to a previous report, the use of a statin prevented the progression of MASLD to MASH but did not reduce liver fat accumulation [41]. It was also reported that ARB contributed to preventing the progression of MASLD to MASH [42,43]. Furthermore, an animal study showed that ARB could reduce liver fat accumulation [44]. Thus, the improvements in the HSI in our study could have been especially influenced by the use of ARB. Nevertheless, the APRI tended to decrease regardless of concomitant use of statins or ARB, which suggested the effects of semaglutide on the prevention of the progression of fibrosis in the liver. On the other hand, we could not compare the changes in MASLD indices in patients with or without SGLT2is and metformin, since most patients took them. Our results should be further examined in patients without these drugs.
Insulin resistance reduces the activity of lipoprotein lipase (LPL), leading to increases in intermediate-density lipoprotein (IDL) and VLDL and decreases in HDL concentration. Semaglutide can stimulate insulin action, reduce the influx of FFA to the liver and enhance LPL activities, leading to improvements in the lipoprotein profile, such as reductions in IDL and VLDL, which could be observed as siginificant decreases in non-HDL-C in our study. Previous studies also reported significant improvements in non-HDL-C, LDL-C, HDL-C and TG [45,46], findings which were consistent with our results. Improvements in the atherogenic lipid profile can assist in the protective role played by semaglutide as to CV diseases, which was demonstrated in the SUSTAIN 6 trial [14].
Although there were no significant differences in UACR during semaglutide treatment, remission in the UACR stage was observed in several patients. Previous studies also reported that once-weekly semaglutide reduced UACR and suggested the renoprotective effects of semaglutide [47,48]. The limited availability of data might have influenced our results.
In our study, 91% of the patients also took SGLT2 inhibitors, which have been reported to improve glycemia, lipid profile and obesity, as well as MASLD [37,49]. Adding once-weekly semaglutide to SGLT2 inhibitors resulted in greater reductions in body weight and HbA1c and was generally well tolerated [50]. A meta-analysis also revealed that a combination therapy comprising SGLT2i and GLP-1RA had beneficial effects on the progression of MASLD, and once-weekly semaglutide had a greatest advantage compared with other GLP-1RA [51].
Our study has several limitations. First, due to the retrospective design with the limited number of patients, our study could not avoid possible influences by various confounding factors. Second, although all patients were recommended to comply with appropriate diet and physical activity according to Japanese clinical standards, we could not take diet and physical activities into account due to difficulties in obtaining sufficient data. Third, our study lacked information on the diabetic duration and the state of coexisting diabetic complications. Lastly, our study lacked histological evaluations of the liver. Further study will be needed with the larger number of patients as well as a control group.
Despite these limitations, our study confirmed the results of previous clinical trials showing the effects of once-weekly semaglutide on body weight, HbA1c and atherogenic lipid profiles, which can be generalized to real-world patients with T2D.
5. Conclusions
Our real-world study showed that once-weekly semaglutide improved body weight, glycemic control and atherogenic lipidemia in Japanese patients with T2D. Moreover, it was suggested that semaglutide reduces hepatic fat content and has a preventative role against the progression of MASLD.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/biomedicines12051001/s1, Table S1: The changes in metabolic parameters during the semaglutide treatment in patients who were GLP-1RA naïve or given semaglutide after being switched from other GLP-1RAs.
Author Contributions
H.K.: Conceptualization, Data curation, Formal analysis, Writing—original draft, editing. H.Y.: Supervision, Writing—review and editing, Data curation. M.H., E.K. (Emika Kaji), M.M., E.K. (Eiji Kakazu), S.I., H.A. and T.K.: Formal analysis, Data curation. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Ethics Committee of the National Center for Global Health and Medicine (NCGM-S-004524) and was performed in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained by the opt-out approach because this study was a retrospective observational study.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Ayano Sakakibara and Yukie Kawamura of the Division of Research Support, National Center for Global Health and Medicine, Kohnodai Hospital, for their great support in data collection.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef]
- Nanditha, A.; Ma, R.C.; Ramachandran, A.; Snehalatha, C.; Chan, J.C.; Chia, K.S.; Shaw, J.E.; Zimmet, P.Z. Diabetes in Asia and the Pacific: Implications for the Global Epidemic. Diabetes Care 2016, 39, 472–485. [Google Scholar] [CrossRef]
- Ma, R.C.; Chan, J.C. Type 2 diabetes in East Asians: Similarities and differences with populations in Europe and the United States. Ann. N. Y. Acad. Sci. 2013, 1281, 64–91. [Google Scholar] [CrossRef] [PubMed]
- Woodward, M.; Zhang, X.; Barzi, F.; Pan, W.; Ueshima, H.; Rodgers, A.; MacMahon, S.; Asia Pacific Cohort Studies Collaboration. The effects of diabetes on the risks of major cardiovascular diseases and death in the Asia-Pacific region. Diabetes Care 2003, 26, 360–366. [Google Scholar] [PubMed]
- Kanaya, A.M.; Adler, N.; Moffet, H.H.; Liu, J.; Schillinger, D.; Adams, A.; Ahmed, A.T.; Karter, A.J. Heterogeneity of diabetes outcomes among asians and pacific islanders in the US: The diabetes study of northern california (DISTANCE). Diabetes Care 2011, 34, 930–937. [Google Scholar] [CrossRef]
- Ueki, K.; Sasako, T.; Okazaki, Y.; Kato, M.; Okahata, S.; Katsuyama, H.; Haraguchi, M.; Morita, A.; Ohashi, K.; Hara, K.; et al. Effect of an intensified multifactorial intervention on cardiovascular outcomes and mortality in type 2 diabetes (J-DOIT3): An open-label, randomised controlled trial. Lancet Diabetes Endocrinol. 2017, 5, 951–964. [Google Scholar] [CrossRef]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Iida, S.; Katsuyama, H. Metabolic-Dysfunction-Associated Steatotic Liver Disease-Its Pathophysiology, Association with Atherosclerosis and Cardiovascular Disease, and Treatments. Int. J. Mol. Sci. 2023, 24, 15473. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Chonchol, M.; Bertolini, L.; Rodella, S.; Zenari, L.; Lippi, G.; Franchini, M.; Zoppini, G.; Muggeo, M. Increased risk of CKD among type 2 diabetics with nonalcoholic fatty liver disease. J. Am. Soc. Nephrol. 2008, 19, 1564–1570. [Google Scholar] [CrossRef]
- Seino, Y.; Terauchi, Y.; Osonoi, T.; Yabe, D.; Abe, N.; Nishida, T.; Zacho, J.; Kaneko, S. Safety and efficacy of semaglutide once weekly vs. sitagliptin once daily, both as monotherapy in Japanese people with type 2 diabetes. Diabetes Obes. Metab. 2018, 20, 378–388. [Google Scholar] [CrossRef]
- Kaku, K.; Yamada, Y.; Watada, H.; Abiko, A.; Nishida, T.; Zacho, J.; Kiyosue, A. Safety and efficacy of once-weekly semaglutide vs. additional oral antidiabetic drugs in Japanese people with inadequately controlled type 2 diabetes: A randomized trial. Diabetes Obes. Metab. 2018, 20, 1202–1212. [Google Scholar] [CrossRef] [PubMed]
- Katsuyama, H.; Hakoshima, M.; Umeyama, S.; Iida, S.; Adachi, H.; Yanai, H. Real-World Efficacy of Glucagon-like Peptide-1 (GLP-1) Receptor Agonist, Dulaglutide, on Metabolic Parameters in Japanese Patients with Type 2 Diabetes: A Retrospective Longitudinal Study. Biomedicines 2023, 11, 869. [Google Scholar] [CrossRef] [PubMed]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Rørth, R.; Jhund, P.S.; Docherty, K.F.; Sattar, N.; Preiss, D.; Køber, L.; Petrie, M.C.; McMurray, J.J.V. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019, 7, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Fukushima, M.; Usami, M.; Ikeda, M.; Nakai, Y.; Taniguchi, A.; Matsuura, T.; Suzuki, H.; Kurose, T.; Yamada, Y.; Seino, Y. Insulin secretion and insulin sensitivity at different stages of glucose tolerance: A cross-sectional study of Japanese type 2 diabetes. Metabolism 2004, 53, 831–835. [Google Scholar] [CrossRef] [PubMed]
- Levey, A.S.; de Jong, P.E.; Coresh, J.; El Nahas, M.; Astor, B.C.; Matsushita, K.; Gansevoort, R.T.; Kasiske, B.L.; Eckardt, K.U. The definition, classification, and prognosis of chronic kidney disease: A KDIGO Controversies Conference report. Kidney Int. 2011, 80, 17–28. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A.; et al. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Kim, D.; Kim, H.J.; Lee, C.-H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.-H.; Cho, S.-H.; Sung, M.-W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef]
- Shah, A.; Lydecker, A.; Murray, K.; Tetri, B.N.; Contos, M.J.; Sanyal, A.J.A. Use of the Fib4 index for non-invasive evaluation of fibrosis in nonalcoholic fatty liver disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1104–1112. [Google Scholar] [CrossRef]
- Sumida, Y.; Yoneda, M.; Hyogo, H.; Itoh, Y.; Ono, M.; Fujii, H.; Eguchi, Y.; Suzuki, Y.; Aoki, N.; Kanemasa, K. Validation of the FIB4 index in a Japanese nonalcoholic fatty liver disease population. BMC Gastroenterol. 2012, 12, 2. [Google Scholar] [CrossRef]
- Yamada, H.; Yoshida, M.; Suzuki, D.; Funazaki, S.; Nagashima, S.; Masahiko, K.; Kiyoshi, O.; Hara, K. Effectiveness and Safety of Once-Weekly Semaglutide in Japanese Patients with Type 2 Diabetes in Treatment Intensification: A Retrospective Observational Single-Center Study. Diabetes Ther. 2022, 13, 1779–1788. [Google Scholar] [CrossRef]
- Webb, N.; Orme, M.; Witkowski, M.; Nakanishi, R.; Langer, J. A Network Meta-Analysis Comparing Semaglutide Once-Weekly with Other GLP-1 Receptor Agonists in Japanese Patients with Type 2 Diabetes. Diabetes Ther. 2018, 9, 973–986. [Google Scholar] [CrossRef]
- Kimura, T.; Katakura, Y.; Shimoda, M.; Kawasaki, F.; Yamabe, M.; Tatsumi, F.; Matsuki, M.; Iwamoto, Y.; Anno, T.; Fushimi, Y.; et al. Comparison of clinical efficacy and safety of weekly glucagon-like peptide-1 receptor agonists dulaglutide and semaglutide in Japanese patients with type 2 diabetes: Randomized, parallel-group, multicentre, open-label trial (COMING study). Diabetes Obes. Metab. 2023, 25, 3632–3647. [Google Scholar] [CrossRef]
- Iijima, T.; Shibuya, M.; Ito, Y.; Terauchi, Y. Effects of switching from liraglutide to semaglutide or dulaglutide in patients with type 2 diabetes: A randomized controlled trial. J. Diabetes Investig. 2023, 14, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Shirabe, S.; Yamazaki, K.; Oishi, M.; Arai, K.; Yagi, N.; Sato, M.; Takeuchi, M.; Kai, T.; Maegawa, H. Changes in prescription patterns and doses of oral antidiabetic drugs in Japanese patients with type 2 diabetes (JDDM70). J. Diabetes Investig. 2023, 14, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Moschen, A.R.; Roden, M. NAFLD and diabetes mellitus. Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 32–42. [Google Scholar] [CrossRef]
- Sakurai, Y.; Kubota, N.; Yamauchi, T.; Kadowaki, T. Role of Insulin Resistance in MAFLD. Int. J. Mol. Sci. 2021, 22, 4156. [Google Scholar] [CrossRef]
- Yabut, J.M.; Drucker, D.J. Glucagon-like Peptide-1 Receptor-based Therapeutics for Metabolic Liver Disease. Endocr. Rev. 2023, 44, 14–32. [Google Scholar] [CrossRef]
- Angulo, P.; Bugianesi, E.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Barrera, F.; Haflidadottir, S.; Day, C.P.; George, J. Simple noninvasive systems predict long-term outcomes of patients with nonalcoholic fatty liver disease. Gastroenterology 2013, 145, 782–789. [Google Scholar] [CrossRef]
- Wong, S.; Huynh, D.; Zhang, F.; Nguyen, N.Q. Use of aspartate aminotransferase to platelet ratio to reduce the need for FibroScan in the evaluation of liver fibrosis. World J. Hepatol. 2017, 9, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Bril, F.; McPhaul, M.J.; Caulfield, M.P.; Clark, V.C.; Soldevilla-Pico, C.; Firpi-Morell, R.J.; Lai., J.; Shiffman, D.; Rowland, C.M.; Cusi, K. Performance of Plasma Biomarkers and Diagnostic Panels for Nonalcoholic Steatohepatitis and Advanced Fibrosis in Patients with Type 2 Diabetes. Diabetes Care 2020, 43, 290–297. [Google Scholar] [CrossRef]
- Mózes, F.E.; Lee, J.A.; Selvaraj, E.A.; Jayaswal, A.N.A.; Trauner, M.; Boursier, J.; Fournier, C.; Staufer, K.; Stauber, R.E.; Bugianesi, E.; et al. Diagnostic accuracy of non-invasive tests for advanced fibrosis in patients with NAFLD: An individual patient data meta-analysis. Gut 2022, 71, 1006–1019. [Google Scholar] [CrossRef] [PubMed]
- Castellana, M.; Donghia, R.; Guerra, V.; Procino, F.; Lampignano, L.; Castellana, F.; Zupo, R.; Sardone, R.; De Pergola, G.; Romanelli, F.; et al. Performance of Fatty Liver Index in Identifying Non-Alcoholic Fatty Liver Disease in Population Studies. A Meta-Analysis. J. Clin. Med. 2021, 10, 1877. [Google Scholar] [CrossRef]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Sundby Palle, M.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised clinical trial: Semaglutide versus placebo reduced liver steatosis but not liver stiffness in subjects with non-alcoholic fatty liver disease assessed by magnetic resonance imaging. Aliment. Pharmacol. Ther. 2021, 54, 1150–1161. [Google Scholar] [CrossRef]
- Newsome, P.N.; Buchholtz, K.; Cusi, K.; Linder, M.; Okanoue, T.; Ratziu, V.; Sanyal, A.J.; Sejling, A.S.; Harrison, S.A.; NN9931-4296 Investigators. A Placebo-Controlled Trial of Subcutaneous Semaglutide in Nonalcoholic Steatohepatitis. N. Engl. J. Med. 2021, 384, 1113–1124. [Google Scholar] [CrossRef]
- Kahl, S.; Gancheva, S.; Straßburger, K.; Herder, C.; Machann, J.; Katsuyama, H.; Kabisch, S.; Henkel, E.; Kopf, S.; Lagerpusch, M.; et al. Empagliflozin Effectively Lowers Liver Fat Content in Well-Controlled Type 2 Diabetes: A Randomized, Double-Blind, Phase 4, Placebo-Controlled Trial. Diabetes Care 2020, 43, 298–305. [Google Scholar] [CrossRef]
- Torres, D.M.; Jones, F.J.; Shaw, J.C.; Williams, C.D.; Ward, J.A.; Harrison, S.A. Rosiglitazone versus rosiglitazone and metformin versus rosiglitazone and losartan in the treatment of nonalcoholic steatohepatitis in humans: A 12-month randomized, prospective, open-label trial. Hepatology 2011, 54, 1631–1639. [Google Scholar] [CrossRef]
- Bugianesi, E.; Gentilcore, E.; Manini, R.; Natale, S.; Vanni, E.; Villanova, N.; David, E.; Rizzetto, M.; Marchesini, G. A randomized controlled trial of metformin versus vitamin E or prescriptive diet in nonalcoholic fatty liver disease. Am. J. Gastroenterol. 2005, 100, 1082–1090. [Google Scholar] [CrossRef]
- Belfort, R.; Harrison, S.A.; Brown, K.; Darland, C.; Finch, J.; Hardies, J.; Balas, B.; Gastaldelli, A.; Tio, F.; Pulcini, J.; et al. A placebo-controlled trial of pioglitazone in subjects with nonalcoholic steatohepatitis. N. Engl. J. Med. 2006, 355, 2297–2307. [Google Scholar] [CrossRef]
- Ayada, I.; van Kleef, L.A.; Zhang, H.; Liu, K.; Li, P.; Abozaid, Y.J.; Lavrijsen, M.; Janssen, H.L.A.; van der Laan, L.J.W.; Ghanbari, M.; et al. Dissecting the multifaceted impact of statin use on fatty liver disease: A multidimensional study. eBioMedicine 2023, 87, 104392. [Google Scholar] [CrossRef]
- Pelusi, S.; Petta, S.; Rosso, C.; Borroni, V.; Fracanzani, A.L.; Dongiovanni, P.; Craxi, A.; Bugianesi, E.; Fargion, S.; Valenti, L. Renin-Angiotensin System Inhibitors, Type 2 Diabetes and Fibrosis Progression: An Observational Study in Patients with Nonalcoholic Fatty Liver Disease. PLoS ONE 2016, 11, e0163069. [Google Scholar] [CrossRef]
- Alam, S.; Kabir, J.; Mustafa, G.; Gupta, U.; Hasan, S.K.; Alam, A.K. Effect of telmisartan on histological activity and fibrosis of non-alcoholic steatohepatitis: A 1-year randomized control trial. Saudi J. Gastroenterol. 2016, 22, 69–76. [Google Scholar] [CrossRef]
- Zhong, J.; Gong, W.; Lu, L.; Chen, J.; Lu, Z.; Li, H.; Liu, W.; Liu, Y.; Wang, M.; Hu, R.; et al. Irbesartan ameliorates hyperlipidemia and liver steatosis in type 2 diabetic db/db mice via stimulating PPAR-γ, AMPK/Akt/mTOR signaling and autophagy. Int. Immunopharmacol. 2017, 42, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Di Folco, U.; Vallecorsa, N.; Nardone, M.R.; Pantano, A.L.; Tubili, C. Effects of semaglutide on cardiovascular risk factors and eating behaviors in type 2 diabetes. Acta Diabetol. 2022, 59, 1287–1294. [Google Scholar] [CrossRef] [PubMed]
- Patti, A.M.; Giglio, R.V.; Allotta, A.; Bruno, A.; Di Bella, T.; Pantea Stoian, A.; Ciaccio, M.; Rizzo, M. Effect of Semaglutide on Subclinical Atherosclerosis and Cardiometabolic Compensation: A Real-World Study in Patients with Type 2 Diabetes. Biomedicines 2023, 11, 1362. [Google Scholar] [CrossRef]
- Mann, J.F.E.; Hansen, T.; Idorn, T.; Leiter, L.A.; Marso, S.P.; Rossing, P.; Seufert, J.; Tadayon, S.; Vilsbøll, T. Effects of once-weekly subcutaneous semaglutide on kidney function and safety in patients with type 2 diabetes: A post-hoc analysis of the SUSTAIN 1-7 randomised controlled trials. Lancet Diabetes Endocrinol. 2020, 8, 880–893. [Google Scholar] [CrossRef]
- Heerspink, H.J.L.; Apperloo, E.; Davies, M.; Dicker, D.; Kandler, K.; Rosenstock, J.; Sørrig, R.; Lawson, J.; Zeuthen, N.; Cherney, D. Effects of Semaglutide on Albuminuria and Kidney Function in People with Overweight or Obesity with or without Type 2 Diabetes: Exploratory Analysis From the STEP 1, 2, and 3 Trials. Diabetes Care 2023, 46, 801–810. [Google Scholar] [CrossRef]
- Mino, M.; Kakazu, E.; Sano, A.; Katsuyama, H.; Hakoshima, M.; Yanai, H.; Aoki, Y.; Imamura, M.; Yamazoe, T.; Mori, T.; et al. Effects of sodium glucose cotransporter 2 inhibitors and pioglitazone on FIB-4 index in metabolic-associated fatty liver disease. Hepatol. Res. 2023, 53, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B.; Bhosekar, V.; Busch, R.; Holst, I.; Ludvik, B.; Thielke, D.; Thrasher, J.; Woo, V.; Philis-Tsimikas, A. Semaglutide once weekly as add-on to SGLT-2 inhibitor therapy in type 2 diabetes (SUSTAIN 9): A randomised, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 356–367. [Google Scholar] [CrossRef]
- Gu, Y.; Sun, L.; Zhang, W.; Kong, T.; Zhou, R.; He, Y.; Deng, C.; Yang, L.; Kong, J.; Chen, Y.; et al. Comparative efficacy of 5 sodium-glucose cotransporter protein-2 (SGLT-2) inhibitor and 4 glucagon-like peptide-1 (GLP-1) receptor agonist drugs in non-alcoholic fatty liver disease: A GRADE-assessed systematic review and network meta-analysis of randomized controlled trials. Front. Pharmacol. 2023, 14, 1102792. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).