
Routinely Used and Emerging Diagnostic and Immunotherapeutic Approaches for Wheat Allergy


 ,
, 
Abstract
1. Introduction
2. Immune and Epigenetic Mechanism
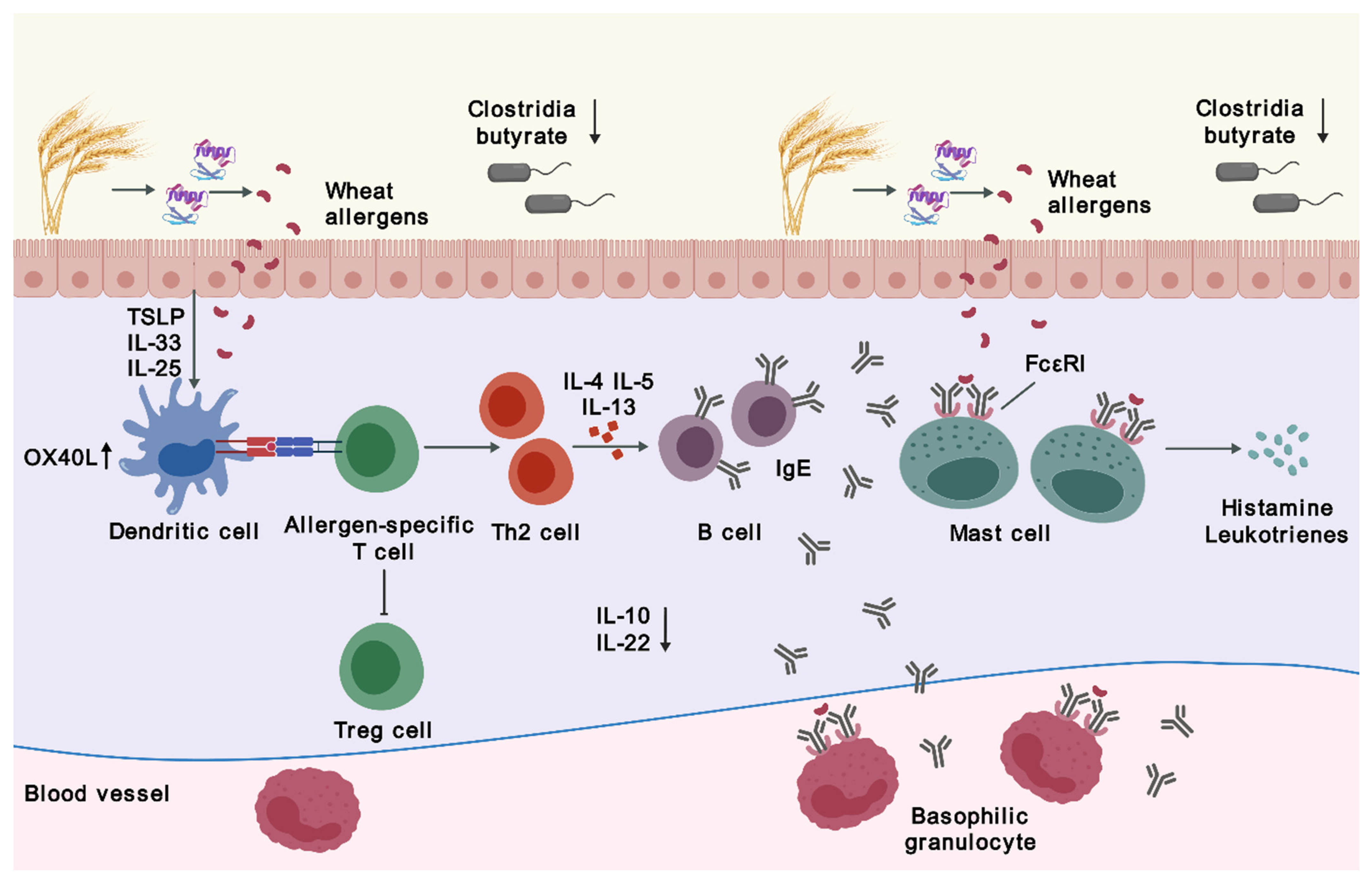
2.1. Sensitization
2.2. Desensitization via Immunotherapy
2.3. Epigenetics
3. Clinical Features and Related Disorders
4. Diagnosis
4.1. Conventional Diagnostic Strategies
4.2. Wheat Allergens and Component-Resolved Diagnosis
4.3. Cell-Based Diagnosis
5. Management
5.1. Natural History of Wheat Allergy
5.2. Therapeutic Strategies
5.3. Immunotherapy
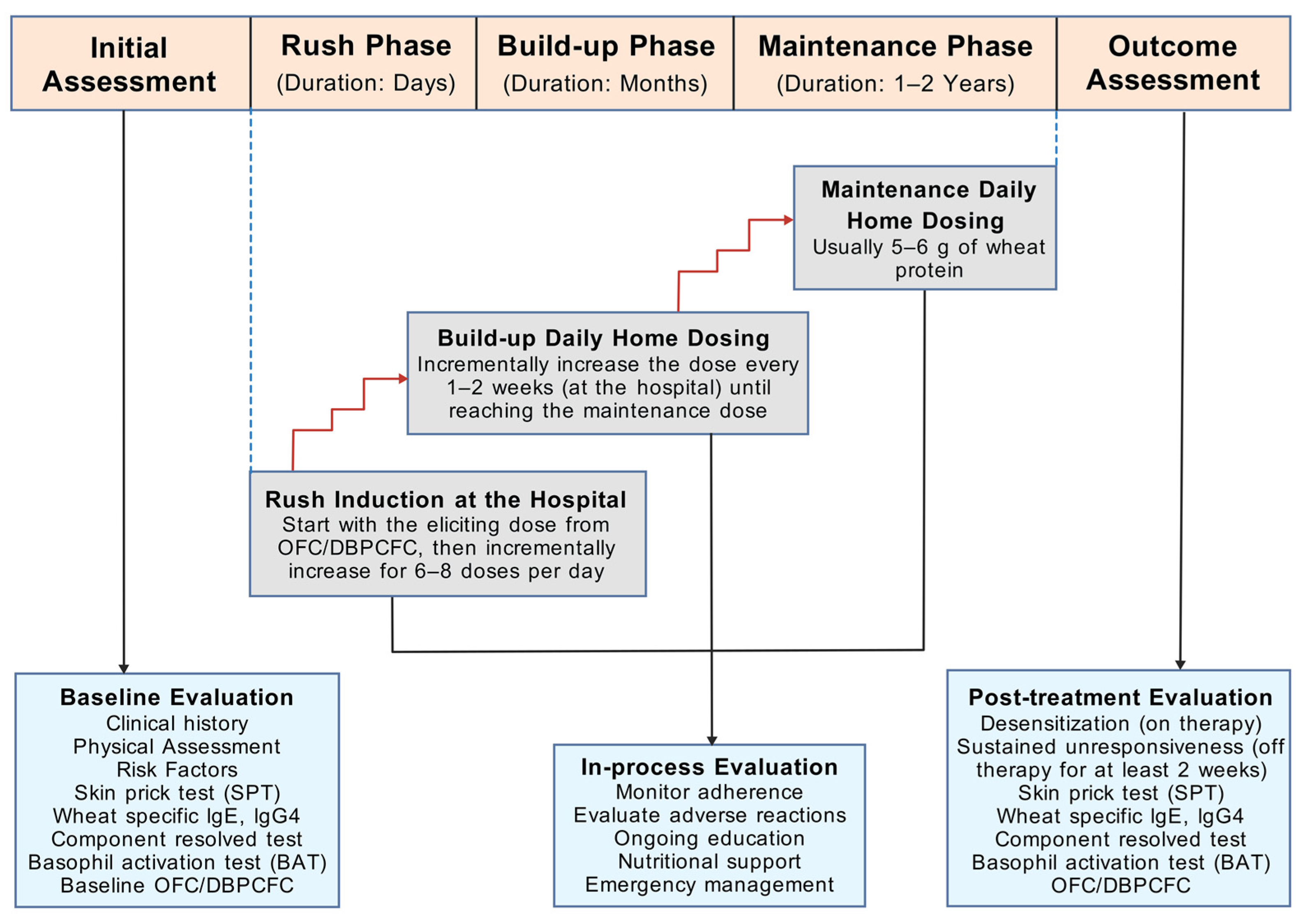
5.3.1. OIT Protocol
5.3.2. Clinical Trials
5.3.3. Precautions for OIT
5.4. Other Therapeutic Approaches
6. Conclusions and Future Trends
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Longo, G.; Berti, I.; Burks, A.W.; Krauss, B.; Barbi, E. IgE-mediated food allergy in children. Lancet 2013, 382, 1656–1664. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.S.Y.; Tham, E.H.; Pacharn, P.; Xing, Y.; Trinh, H.K.T.; Lee, S.; Ahn, K.; Chatchatee, P.; Sato, S.; Ebisawa, M.; et al. Disparities in pediatric anaphylaxis triggers and management across Asia. Allergy 2024, 79, 1317–1328. [Google Scholar] [CrossRef] [PubMed]
- Yu, W.; Freeland, D.M.H.; Nadeau, K.C. Food allergy: Immune mechanisms, diagnosis and immunotherapy. Nat. Rev. Immunol. 2016, 16, 751–765. [Google Scholar] [CrossRef]
- Spolidoro, G.C.I.; Ali, M.M.; Amera, Y.T.; Nyassi, S.; Lisik, D.; Ioannidou, A.; Rovner, G.; Khaleva, E.; Venter, C.; van Ree, R.; et al. Prevalence estimates of eight big food allergies in Europe: Updated systematic review and meta-analysis. Allergy 2023, 78, 2361–2417. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Huang, J.; Ma, S.; Yu, G.; Liao, A.; Pan, L.; Hou, Y. Allergenicity of wheat protein in diet: Mechanisms, modifications and challenges. Food Res. Int. 2023, 169, 112913. [Google Scholar] [CrossRef]
- Cabanillas, B. Gluten-related disorders: Celiac disease, wheat allergy, and nonceliac gluten sensitivity. Crit. Rev. Food Sci. Nutr. 2020, 60, 2606–2621. [Google Scholar] [CrossRef] [PubMed]
- Cianferoni, A. Wheat allergy: Diagnosis and management. J. Asthma Allergy 2016, 9, 13–25. [Google Scholar] [CrossRef]
- Tordesillas, L.; Berin, M.C.; Sampson, H.A. Immunology of Food Allergy. Immunity 2017, 47, 32–50. [Google Scholar] [CrossRef] [PubMed]
- Pacharn, P.; Vichyanond, P. Immunotherapy for IgE-mediated wheat allergy. Hum. Vaccin. Immunother. 2017, 13, 2462–2466. [Google Scholar] [CrossRef]
- Paul, W.E.; Zhu, J. How are TH2-type immune responses initiated and amplified? Nat. Rev. Immunol. 2010, 10, 225–235. [Google Scholar] [CrossRef]
- Lamiable, O.; Mayer, J.U.; Munoz-Erazo, L.; Ronchese, F. Dendritic cells in Th2 immune responses and allergic sensitization. Immunol. Cell Biol. 2020, 98, 807–818. [Google Scholar] [CrossRef] [PubMed]
- Ito, T.; Wang, Y.H.; Duramad, O.; Hori, T.; Delespesse, G.J.; Watanabe, N.; Qin, F.X.; Yao, Z.; Cao, W.; Liu, Y.J. TSLP-activated dendritic cells induce an inflammatory T helper type 2 cell response through OX40 ligand. J. Exp. Med. 2005, 202, 1213–1223. [Google Scholar] [CrossRef] [PubMed]
- Brandt, E.B.; Munitz, A.; Orekov, T.; Mingler, M.K.; McBride, M.; Finkelman, F.D.; Rothenberg, M.E. Targeting IL-4/IL-13 signaling to alleviate oral allergen-induced diarrhea. J. Allergy Clin. Immunol. 2009, 123, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, A. Mucosal dendritic cells. Annu. Rev. Immunol. 2007, 25, 381–418. [Google Scholar] [CrossRef] [PubMed]
- de Jong, N.W.; Wichers, H.J. Update on Nutrition and Food Allergy. Nutrients 2022, 14, 2137. [Google Scholar] [CrossRef] [PubMed]
- Eiwegger, T.; Hung, L.; San Diego, K.E.; O’Mahony, L.; Upton, J. Recent developments and highlights in food allergy. Allergy 2019, 74, 2355–2367. [Google Scholar] [CrossRef] [PubMed]
- Stone, K.D.; Prussin, C.; Metcalfe, D.D. IgE, mast cells, basophils, and eosinophils. J. Allergy Clin. Immunol. 2010, 125 (Suppl. 2), S73–S80. [Google Scholar] [CrossRef] [PubMed]
- Galli, S.J.; Tsai, M. IgE and mast cells in allergic disease. Nat. Med. 2012, 18, 693–704. [Google Scholar] [CrossRef]
- Oyoshi, M.K.; Oettgen, H.C.; Chatila, T.A.; Geha, R.S.; Bryce, P.J. Food allergy: Insights into etiology, prevention, and treatment provided by murine models. J. Allergy Clin. Immunol. 2014, 133, 309–317. [Google Scholar] [CrossRef]
- Rekabi, M.; Arshi, S.; Bemanian, M.H.; Rekabi, V.; Rajabi, A.; Fallahpour, M.; Molatefi, R.; Shokri, S.; Eslami, N.; Ahmadian, J.; et al. Evaluation of a new protocol for wheat desensitization in patients with wheat-induced anaphylaxis. Immunotherapy 2017, 9, 637–645. [Google Scholar] [CrossRef]
- Babaie, D.; Ebisawa, M.; Soheili, H.; Ghasemi, R.; Zandieh, F.; Sahragard, M.; Seifi, H.; Fallahi, M.; Khoshmirsafa, M.; Darougar, S.; et al. Oral Wheat Immunotherapy: Long-Term Follow-Up in Children with Wheat Anaphylaxis. Int. Arch. Allergy Immunol. 2022, 183, 306–314. [Google Scholar] [CrossRef] [PubMed]
- Nagakura, K.I.; Yanagida, N.; Sato, S.; Nishino, M.; Takahashi, K.; Asaumi, T.; Ogura, K.; Ebisawa, M. Low-dose-oral immunotherapy for children with wheat-induced anaphylaxis. Pediatr. Allergy Immunol. 2020, 31, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Burton, O.T.; Logsdon, S.L.; Zhou, J.S.; Medina-Tamayo, J.; Abdel-Gadir, A.; Noval Rivas, M.; Koleoglou, K.J.; Chatila, T.A.; Schneider, L.C.; Rachid, R.; et al. Oral immunotherapy induces IgG antibodies that act through FcγRIIb to suppress IgE-mediated hypersensitivity. J. Allergy Clin. Immunol. 2014, 134, 1310–1317.e6. [Google Scholar] [CrossRef]
- van de Veen, W.; Stanic, B.; Yaman, G.; Wawrzyniak, M.; Söllner, S.; Akdis, D.G.; Rückert, B.; Akdis, C.A.; Akdis, M. IgG4 production is confined to human IL-10-producing regulatory B cells that suppress antigen-specific immune responses. J. Allergy Clin. Immunol. 2013, 131, 1204–1212. [Google Scholar] [CrossRef]
- Nouri-Aria, K.T.; Wachholz, P.A.; Francis, J.N.; Jacobson, M.R.; Walker, S.M.; Wilcock, L.K.; Staple, S.Q.; Aalberse, R.C.; Till, S.J.; Durham, S.R. Grass pollen immunotherapy induces mucosal and peripheral IL-10 responses and blocking IgG activity. J. Immunol. 2004, 172, 3252–3259. [Google Scholar] [CrossRef] [PubMed]
- Gri, G.; Piconese, S.; Frossi, B.; Manfroi, V.; Merluzzi, S.; Tripodo, C.; Viola, A.; Odom, S.; Rivera, J.; Colombo, M.P.; et al. CD4+CD25+ regulatory T cells suppress mast cell degranulation and allergic responses through OX40-OX40L interaction. Immunity 2008, 29, 771–781. [Google Scholar] [CrossRef]
- Di Costanzo, M.; De Paulis, N.; Capra, M.E.; Biasucci, G. Nutrition during Pregnancy and Lactation: Epigenetic Effects on Infants’ Immune System in Food Allergy. Nutrients 2022, 14, 1766. [Google Scholar] [CrossRef]
- Cañas, J.A.; Núñez, R.; Cruz-Amaya, A.; Gómez, F.; Torres, M.J.; Palomares, F.; Mayorga, C. Epigenetics in Food Allergy and Immunomodulation. Nutrients 2021, 13, 4345. [Google Scholar] [CrossRef]
- Yang, F.; Zhang, X.; Xie, Y.; Yuan, J.; Gao, J.; Chen, H.; Li, X. The pathogenesis of food allergy and protection offered by dietary compounds from the perspective of epigenetics. J. Nutr. Biochem. 2024, 128, 109593. [Google Scholar] [CrossRef]
- Berni Canani, R.; Paparo, L.; Nocerino, R.; Cosenza, L.; Pezzella, V.; Di Costanzo, M.; Capasso, M.; Del Monaco, V.; D’Argenio, V.; Greco, L.; et al. Differences in DNA methylation profile of Th1 and Th2 cytokine genes are associated with tolerance acquisition in children with IgE-mediated cow’s milk allergy. Clin. Epigenetics 2015, 7, 38. [Google Scholar] [CrossRef]
- Paparo, L.; Nocerino, R.; Cosenza, L.; Aitoro, R.; D’Argenio, V.; Del Monaco, V.; Di Scala, C.; Amoroso, A.; Di Costanzo, M.; Salvatore, F.; et al. Epigenetic features of FoxP3 in children with cow’s milk allergy. Clin. Epigenetics 2016, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Han, X.; Lyu, S.C.; Bunning, B.; Kost, L.; Chang, I.; Cao, S.; Sampath, V.; Nadeau, K.C. Targeted DNA methylation profiling reveals epigenetic signatures in peanut allergy. JCI Insight 2021, 6, e143058. [Google Scholar] [CrossRef] [PubMed]
- Imran, S.; Neeland, M.R.; Peng, S.; Vlahos, A.; Martino, D.; Dharmage, S.C.; Tang, M.L.K.; Sawyer, S.; Dang, T.D.; McWilliam, V.; et al. Immuno-epigenomic analysis identifies attenuated interferon responses in naïve CD4 T cells of adolescents with peanut and multi-food allergy. Pediatr. Allergy Immunol. 2022, 33, e13890. [Google Scholar] [CrossRef]
- Hua, X.; Goedert, J.J.; Pu, A.; Yu, G.; Shi, J. Allergy associations with the adult fecal microbiota: Analysis of the American Gut Project. EBioMedicine 2016, 3, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Ling, Z.; Li, Z.; Liu, X.; Cheng, Y.; Luo, Y.; Tong, X.; Yuan, L.; Wang, Y.; Sun, J.; Li, L.; et al. Altered fecal microbiota composition associated with food allergy in infants. Appl. Environ. Microbiol. 2014, 80, 2546–2554. [Google Scholar] [CrossRef]
- Zubeldia-Varela, E.; Barker-Tejeda, T.C.; Obeso, D.; Villaseñor, A.; Barber, D.; Pérez-Gordo, M. Microbiome and Allergy: New Insights and Perspectives. J. Investig. Allergol. Clin. Immunol. 2022, 32, 327–344. [Google Scholar] [CrossRef]
- Berin, M.C.; Sampson, H.A. Mucosal immunology of food allergy. Curr. Biol. 2013, 23, R389–R400. [Google Scholar] [CrossRef]
- Iweala, O.I.; Nagler, C.R. The Microbiome and Food Allergy. Annu. Rev. Immunol. 2019, 37, 377–403. [Google Scholar] [CrossRef] [PubMed]
- Bunyavanich, S.; Berin, M.C. Food allergy and the microbiome: Current understandings and future directions. J. Allergy Clin. Immunol. 2019, 144, 1468–1477. [Google Scholar] [CrossRef]
- Tanaka, M.; Korenori, Y.; Washio, M.; Kobayashi, T.; Momoda, R.; Kiyohara, C.; Kuroda, A.; Saito, Y.; Sonomoto, K.; Nakayama, J. Signatures in the gut microbiota of Japanese infants who developed food allergies in early childhood. FEMS Microbiol. Ecol. 2017, 93, fix099. [Google Scholar] [CrossRef]
- Kanchongkittiphon, W.; Nopnipa, S.; Mathuranyanon, R.; Nonthabenjawan, N.; Sritournok, S.; Manuyakorn, W.; Wanapaisan, P. Characterization of gut microbiome profile in children with confirmed wheat allergy. Asian Pac. J. Allergy Immunol. 2024. [Google Scholar] [CrossRef]
- Lozano-Ojalvo, D.; Berin, C.; Tordesillas, L. Immune Basis of Allergic Reactions to Food. J. Investig. Allergol. Clin. Immunol. 2019, 29, 1–14. [Google Scholar] [CrossRef]
- Berni Canani, R.; Sangwan, N.; Stefka, A.T.; Nocerino, R.; Paparo, L.; Aitoro, R.; Calignano, A.; Khan, A.A.; Gilbert, J.A.; Nagler, C.R. Lactobacillus rhamnosus GG-supplemented formula expands butyrate-producing bacterial strains in food allergic infants. ISME J. 2016, 10, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Czaja-Bulsa, G.; Bulsa, M. What Do We Know Now about IgE-Mediated Wheat Allergy in Children? Nutrients 2017, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Pasha, I.; Saeed, F.; Sultan, M.T.; Batool, R.; Aziz, M.; Ahmed, W. Wheat Allergy and Intolerence; Recent Updates and Perspectives. Crit. Rev. Food Sci. Nutr. 2016, 56, 13–24. [Google Scholar] [CrossRef]
- Matsuo, H.; Dahlström, J.; Tanaka, A.; Kohno, K.; Takahashi, H.; Furumura, M.; Morita, E. Sensitivity and specificity of recombinant omega-5 gliadin-specific IgE measurement for the diagnosis of wheat-dependent exercise-induced anaphylaxis. Allergy 2008, 63, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Matricardi, P.M.; Kleine-Tebbe, J.; Hoffmann, H.J.; Valenta, R.; Hilger, C.; Hofmaier, S.; Aalberse, R.C.; Agache, I.; Asero, R.; Ballmer-Weber, B.; et al. EAACI Molecular Allergology User’s Guide. Pediatr. Allergy Immunol. 2016, 27 (Suppl. 23), 1–250. [Google Scholar] [CrossRef] [PubMed]
- Faihs, V.; Kugler, C.; Schmalhofer, V.; Scherf, K.A.; Lexhaller, B.; Mortz, C.G.; Bindslev-Jensen, C.; Biedermann, T.; Brockow, K. Wheat-dependent exercise-induced anaphylaxis: Subtypes, diagnosis, and management. J. Dtsch. Dermatol. Ges. 2023, 21, 1131–1135. [Google Scholar] [CrossRef]
- Ansley, L.; Bonini, M.; Delgado, L.; Del Giacco, S.; Du Toit, G.; Khaitov, M.; Kurowski, M.; Hull, J.H.; Moreira, A.; Robson-Ansley, P.J. Pathophysiological mechanisms of exercise-induced anaphylaxis: An EAACI position statement. Allergy 2015, 70, 1212–1221. [Google Scholar] [CrossRef]
- Matsuo, H.; Morimoto, K.; Akaki, T.; Kaneko, S.; Kusatake, K.; Kuroda, T.; Niihara, H.; Hide, M.; Morita, E. Exercise and aspirin increase levels of circulating gliadin peptides in patients with wheat-dependent exercise-induced anaphylaxis. Clin. Exp. Allergy 2005, 35, 461–466. [Google Scholar] [CrossRef]
- Mizuno, O.; Nomura, T.; Ohguchi, Y.; Suzuki, S.; Nomura, Y.; Hamade, Y.; Hoshina, D.; Sandilands, A.; Akiyama, M.; McLean, W.H.; et al. Loss-of-function mutations in the gene encoding filaggrin underlie a Japanese family with food-dependent exercise-induced anaphylaxis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.J.; Eller, E.; Mortz, C.G.; Brockow, K.; Bindslev-Jensen, C. Wheat-Dependent Cofactor-Augmented Anaphylaxis: A Prospective Study of Exercise, Aspirin, and Alcohol Efficacy as Cofactors. J. Allergy Clin. Immunol. Pract. 2019, 7, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Gao, X.; Li, J.; Li, L.; Liu, J.; Yin, J. Clinical features and outcomes of patients with wheat-dependent exercise-induced anaphylaxis: A retrospective study. Allergy Asthma Clin. Immunol. 2022, 18, 61. [Google Scholar] [CrossRef] [PubMed]
- Santos, A.F.; Riggioni, C.; Agache, I.; Akdis, C.A.; Akdis, M.; Alvarez-Perea, A.; Alvaro-Lozano, M.; Ballmer-Weber, B.; Barni, S.; Beyer, K.; et al. EAACI guidelines on the diagnosis of IgE-mediated food allergy. Allergy 2023, 78, 3057–3076. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Futamura, M.; Borres, M.P.; Takaoka, Y.; Dahlstrom, J.; Sakamoto, T.; Tanaka, A.; Kohno, K.; Matsuo, H.; Morita, E. IgE antibodies to omega-5 gliadin associate with immediate symptoms on oral wheat challenge in Japanese children. Allergy 2008, 63, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Scibilia, J.; Pastorello, E.A.; Zisa, G.; Ottolenghi, A.; Bindslev-Jensen, C.; Pravettoni, V.; Scovena, E.; Robino, A.; Ortolani, C. Wheat allergy: A double-blind, placebo-controlled study in adults. J. Allergy Clin. Immunol. 2006, 117, 433–439. [Google Scholar] [CrossRef]
- Mäkelä, M.J.; Eriksson, C.; Kotaniemi-Syrjänen, A.; Palosuo, K.; Marsh, J.; Borres, M.; Kuitunen, M.; Pelkonen, A.S. Wheat allergy in children—New tools for diagnostics. Clin. Exp. Allergy 2014, 44, 1420–1430. [Google Scholar] [CrossRef]
- Palosuo, K.; Varjonen, E.; Kekki, O.M.; Klemola, T.; Kalkkinen, N.; Alenius, H.; Reunala, T. Wheat omega-5 gliadin is a major allergen in children with immediate allergy to ingested wheat. J. Allergy Clin. Immunol. 2001, 108, 634–638. [Google Scholar] [CrossRef]
- Kulmala, P.; Pelkonen, A.S.; Kuitunen, M.; Paassilta, M.; Remes, S.; Schultz, R.; Dunder, T.; Turunen, S.; Mäkelä, M.J. Wheat oral immunotherapy was moderately successful but was associated with very frequent adverse events in children aged 6–18 years. Acta Paediatr. 2018, 107, 861–870. [Google Scholar] [CrossRef]
- Phisitbuntoon, T.; Jirapongsananuruk, O.; Pacharn, P.; Wangthan, U.; Srisuwatchari, W.; Reamtong, O.; Visitsunthorn, N.; Piboonpocanun, S. A potential role of gliadin extract skin prick test in IgE-mediated wheat allergy. Asian Pac. J. Allergy Immunol. 2023, 41, 37–44. [Google Scholar]
- Pacharn, P.; Siripipattanamongkol, N.; Pannakapitak, N.; Visitsunthorn, N.; Jirapongsananuruk, O.; Piboonpocanun, S.; Vichyanond, P. Accuracy of in-house alcohol-dissolved wheat extract for diagnosing IgE-mediated wheat allergy. Asian Pac. J. Allergy Immunol. 2020, 38, 102–107. [Google Scholar] [PubMed]
- Pacharn, P.; Kumjim, S.; Tattiyapong, P.; Jirapongsananuruk, O.; Piboonpocanun, S. Identification of wheat sensitization using an in-house wheat extract in Coca-10% alcohol solution in children with wheat anaphylaxis. Asian Pac. J. Allergy Immunol. 2016, 34, 153–158. [Google Scholar]
- Constantin, C.; Quirce, S.; Poorafshar, M.; Touraev, A.; Niggemann, B.; Mari, A.; Ebner, C.; Akerström, H.; Heberle-Bors, E.; Nystrand, M.; et al. Micro-arrayed wheat seed and grass pollen allergens for component-resolved diagnosis. Allergy 2009, 64, 1030–1037. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, N.; Nilsson, C.; Ekoff, H.; Wieser-Pahr, S.; Borres, M.P.; Valenta, R.; Hedlin, G.; Sjölander, S. Grass-Allergic Children Frequently Show Asymptomatic Low-Level IgE Co-Sensitization and Cross-Reactivity to Wheat. Int. Arch. Allergy Immunol. 2018, 177, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Keet, C.A.; Matsui, E.C.; Dhillon, G.; Lenehan, P.; Paterakis, M.; Wood, R.A. The natural history of wheat allergy. Ann. Allergy Asthma Immunol. 2009, 102, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Czaja-Bulsa, G.; Bulsa, M. The natural history of IgE mediated wheat allergy in children with dominant gastrointestinal symptoms. Allergy Asthma Clin. Immunol. 2014, 10, 12. [Google Scholar] [CrossRef] [PubMed]
- Tatham, A.S.; Shewry, P.R. Allergens to wheat and related cereals. Clin. Exp. Allergy 2008, 38, 1712–1726. [Google Scholar] [CrossRef]
- Park, H.J.; Kim, J.H.; Kim, J.E.; Jin, H.J.; Choi, G.S.; Ye, Y.M.; Park, H.S. Diagnostic value of the serum-specific IgE ratio of ω-5 gliadin to wheat in adult patients with wheat-induced anaphylaxis. Int. Arch. Allergy Immunol. 2012, 157, 147–150. [Google Scholar] [CrossRef]
- Scherf, K.A.; Brockow, K.; Biedermann, T.; Koehler, P.; Wieser, H. Wheat-dependent exercise-induced anaphylaxis. Clin. Exp. Allergy 2016, 46, 10–20. [Google Scholar] [CrossRef]
- Morita, E.; Matsuo, H.; Mihara, S.; Morimoto, K.; Savage, A.W.; Tatham, A.S. Fast omega-gliadin is a major allergen in wheat-dependent exercise-induced anaphylaxis. J. Dermatol. Sci. 2003, 33, 99–104. [Google Scholar] [CrossRef]
- Daengsuwan, T.; Palosuo, K.; Phankingthongkum, S.; Visitsunthorn, N.; Jirapongsananuruk, O.; Alenius, H.; Vichyanond, P.; Reunala, T. IgE antibodies to omega-5 gliadin in children with wheat-induced anaphylaxis. Allergy 2005, 60, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, N.; Sjölander, S.; Baar, A.; Berthold, M.; Pahr, S.; Vrtala, S.; Valenta, R.; Morita, E.; Hedlin, G.; Borres, M.P.; et al. Wheat allergy in children evaluated with challenge and IgE antibodies to wheat components. Pediatr. Allergy Immunol. 2015, 26, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Matsuo, H.; Chinuki, Y.; Kohno, K.; Tanaka, A.; Maruyama, N.; Morita, E. Recombinant high molecular weight-glutenin subunit-specific IgE detection is useful in identifying wheat-dependent exercise-induced anaphylaxis complementary to recombinant omega-5 gliadin-specific IgE test. Clin. Exp. Allergy 2012, 42, 1293–1298. [Google Scholar] [CrossRef] [PubMed]
- Gabler, A.M.; Gebhard, J.; Eberlein, B.; Biedermann, T.; Scherf, K.A.; Brockow, K. The basophil activation test differentiates between patients with wheat-dependent exercise-induced anaphylaxis and control subjects using gluten and isolated gluten protein types. Clin. Transl. Allergy 2021, 11, e12050. [Google Scholar] [CrossRef] [PubMed]
- Chinuki, Y.; Yagami, A.; Adachi, A.; Matsunaga, K.; Ugajin, T.; Yokozeki, H.; Hayashi, M.; Katayama, I.; Kohno, K.; Shiwaku, K.; et al. In vitro basophil activation is reduced by short-term omalizumab treatment in hydrolyzed wheat protein allergy. Allergol. Int. 2020, 69, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Chinuki, Y.; Kohno, K.; Hide, M.; Hanaoka, K.; Okabe, T.; Fukunaga, A.; Oda, Y.; Adachi, A.; Ugajin, T.; Yokozeki, H.; et al. Efficacy and safety of omalizumab in adult patients with wheat-dependent exercise-induced anaphylaxis: Reduction of in vitro basophil activation and allergic reaction to wheat. Allergol. Int. 2023, 72, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Sindher, S.B.; Long, A.; Chin, A.R.; Hy, A.; Sampath, V.; Nadeau, K.C.; Chinthrajah, R.S. Food allergy, mechanisms, diagnosis and treatment: Innovation through a multi-targeted approach. Allergy 2022, 77, 2937–2948. [Google Scholar] [CrossRef] [PubMed]
- Tokuda, R.; Nagao, M.; Hiraguchi, Y.; Hosoki, K.; Matsuda, T.; Kouno, K.; Morita, E.; Fujisawa, T. Antigen-induced expression of CD203c on basophils predicts IgE-mediated wheat allergy. Allergol. Int. 2009, 58, 193–199. [Google Scholar] [CrossRef] [PubMed]
- Wai, C.Y.Y.; Leung, P.S.C. Emerging approaches in the diagnosis and therapy in shellfish allergy. Curr. Opin. Allergy Clin. Immunol. 2022, 22, 202–212. [Google Scholar] [CrossRef]
- Wai, C.Y.Y.; Leung, N.Y.H.; Leung, A.S.Y.; Shum, Y.; Leung, P.S.C.; Chu, K.H.; Kwan, Y.W.; Lee, Q.U.; Wong, J.S.C.; Lam, I.C.S.; et al. Cell-Based Functional IgE Assays Are Superior to Conventional Allergy Tests for Shrimp Allergy Diagnosis. J. Allergy Clin. Immunol. Pract. 2021, 9, 236–244.e9. [Google Scholar] [CrossRef]
- Chinuki, Y.; Kaneko, S.; Dekio, I.; Takahashi, H.; Tokuda, R.; Nagao, M.; Fujisawa, T.; Morita, E. CD203c expression-based basophil activation test for diagnosis of wheat-dependent exercise-induced anaphylaxis. J. Allergy Clin. Immunol. 2012, 129, 1404–1406. [Google Scholar] [CrossRef] [PubMed]
- Bahri, R.; Custovic, A.; Korosec, P.; Tsoumani, M.; Barron, M.; Wu, J.; Sayers, R.; Weimann, A.; Ruiz-Garcia, M.; Patel, N.; et al. Mast cell activation test in the diagnosis of allergic disease and anaphylaxis. J. Allergy Clin. Immunol. 2018, 142, 485–496.e16. [Google Scholar] [CrossRef] [PubMed]
- Riggioni, C.; Ricci, C.; Moya, B.; Wong, D.; van Goor, E.; Bartha, I.; Buyuktiryaki, B.; Giovannini, M.; Jayasinghe, S.; Jaumdally, H.; et al. Systematic review and meta-analyses on the accuracy of diagnostic tests for IgE-mediated food allergy. Allergy 2024, 79, 324–352. [Google Scholar] [CrossRef] [PubMed]
- Dramburg, S.; Hilger, C.; Santos, A.F.; de Las Vecillas, L.; Aalberse, R.C.; Acevedo, N.; Aglas, L.; Altmann, F.; Arruda, K.L.; Asero, R.; et al. EAACI Molecular Allergology User’s Guide 2.0. Pediatr. Allergy Immunol. 2023, 34 (Suppl. 28), e13854. [Google Scholar] [CrossRef] [PubMed]
- Leeds, S.; Liu, E.G.; Nowak-Wegrzyn, A. Wheat oral immunotherapy. Curr. Opin. Allergy Clin. Immunol. 2021, 21, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Tomsitz, D.; Biedermann, T.; Brockow, K. Sublingual immunotherapy reduces reaction threshold in three patients with wheat-dependent exercise-induced anaphylaxis. Allergy 2021, 76, 3804–3806. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez del Río, P.; Díaz-Perales, A.; Sanchez-García, S.; Escudero, C.; do Santos, P.; Catarino, M.; Ibañez, M.D. Oral immunotherapy in children with IgE-mediated wheat allergy: Outcome and molecular changes. J. Investig. Allergol. Clin. Immunol. 2014, 24, 240–248. [Google Scholar] [PubMed]
- Sato, S.; Utsunomiya, T.; Imai, T.; Yanagida, N.; Asaumi, T.; Ogura, K.; Koike, Y.; Hayashi, N.; Okada, Y.; Shukuya, A.; et al. Wheat oral immunotherapy for wheat-induced anaphylaxis. J. Allergy Clin. Immunol. 2015, 136, 1131–1133.e7. [Google Scholar] [CrossRef] [PubMed]
- Khayatzadeh, A.; Gharaghozlou, M.; Ebisawa, M.; Shokouhi Shoormasti, R.; Movahedi, M. A Safe and Effective Method for Wheat Oral Immunotherapy. Iran. J. Allergy Asthma Immunol. 2016, 15, 525–535. [Google Scholar]
- Nowak-Węgrzyn, A.; Wood, R.A.; Nadeau, K.C.; Pongracic, J.A.; Henning, A.K.; Lindblad, R.W.; Beyer, K.; Sampson, H.A. Multicenter, randomized, double-blind, placebo-controlled clinical trial of vital wheat gluten oral immunotherapy. J. Allergy Clin. Immunol. 2019, 143, 651–661.e9. [Google Scholar] [CrossRef]
- Ogura, K.; Yanagida, N.; Sato, S.; Imai, T.; Ito, K.; Kando, N.; Ikeda, M.; Shibata, R.; Murakami, Y.; Fujisawa, T.; et al. Evaluation of oral immunotherapy efficacy and safety by maintenance dose dependency: A multicenter randomized study. World Allergy Organ. J. 2020, 13, 100463. [Google Scholar] [CrossRef] [PubMed]
- Nagakura, K.I.; Yanagida, N.; Miura, Y.; Itonaga, T.; Nishino, M.; Takahashi, K.; Ogura, K.; Sato, S.; Ebisawa, M. Long-term follow-up of fixed low-dose oral immunotherapy for children with wheat-induced anaphylaxis. J. Allergy Clin. Immunol. Pract. 2022, 10, 1117–1119.e2. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, S.; Kitamura, K.; Makino, A.; Matsui, T.; Furuta, T.; Takasato, Y.; Kando, N.; Ito, K. Slow low-dose oral immunotherapy: Threshold and immunological change. Allergol. Int. 2020, 69, 601–609. [Google Scholar] [CrossRef] [PubMed]
- Sharafian, S.; Amirzargar, A.; Gharagozlou, M.; Parvaneh, N.; Shariat, M.; Tavakol, M.; Movahedi, M. The Efficacy of a New Protocol of Oral Immunotherapy to Wheat for Desensitization and Induction of Tolerance. Iran. J. Allergy Asthma Immunol. 2022, 21, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Pourvali, A.; Arshi, S.; Nabavi, M.; Bemanian, M.H.; Shokri, S.; Khajoei, S.; Seif, F.; Fallahpour, M. Sustained unresponsiveness development in wheat oral immunotherapy: Predictive factors and flexible regimen in the maintenance phase. Eur. Ann. Allergy Clin. Immunol. 2023, 55, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.J.; Eller, E.; Mortz, C.G.; Brockow, K.; Bindslev-Jensen, C. Clinical and serological follow-up of patients with WDEIA. Clin. Transl. Allergy 2019, 9, 26. [Google Scholar] [CrossRef] [PubMed]
- Makita, E.; Yanagida, N.; Sato, S.; Asaumi, T.; Ebisawa, M. Long-term prognosis after wheat oral immunotherapy. J. Allergy Clin. Immunol. Pract. 2020, 8, 371–374.e5. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Tanaka, K.; Tagami, K.; Matsui, T.; Sugiura, S.; Kando, N.; Kanie, Y.; Naito, M.; Izumi, H.; Tanaka, A.; et al. Exercise-induced allergic reactions on desensitization to wheat after rush oral immunotherapy. Allergy 2020, 75, 1414–1422. [Google Scholar] [CrossRef] [PubMed]
- Kubota, S.; Kitamura, K.; Matsui, T.; Takasato, Y.; Sugiura, S.; Ito, K. Exercise-induced allergic reactions after achievement of desensitization to cow’s milk and wheat. Pediatr. Allergy Immunol. 2021, 32, 1048–1055. [Google Scholar] [CrossRef]
- Pacharn, P.; Siripipattanamongkol, N.; Veskitkul, J.; Jirapongsananuruk, O.; Visitsunthorn, N.; Vichyanond, P. Successful wheat-specific oral immunotherapy in highly sensitive individuals with a novel multirush/maintenance regimen. Asia Pac. Allergy 2014, 4, 180–183. [Google Scholar] [CrossRef]
- Loke, P.; Orsini, F.; Lozinsky, A.C.; Gold, M.; O’Sullivan, M.D.; Quinn, P.; Lloyd, M.; Ashley, S.E.; Pitkin, S.; Axelrad, C.; et al. Probiotic peanut oral immunotherapy versus oral immunotherapy and placebo in children with peanut allergy in Australia (PPOIT-003): A multicentre, randomised, phase 2b trial. Lancet Child. Adolesc. Health 2022, 6, 171–184. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Study | Design | Patients Treated with OIT, n | Age, Mean (Range) | Form of Wheat Use | Up-Dosing Phase | Maintenance Phase | Target Dose | Changes in SPT Scores (Mean/Median) | Changes in sIgE (Mean/Median) | Changes in sIgG (Mean/Median) | Efficacy after OIT, % Desensitization | Efficacy after OIT, % Sustained Unresponsiveness | Adverse Reaction (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Rodríguez del Río (2014) [87] | Open-label, nonrandomized, no control | 6 | 5.5 (5–11) years | Semolina porridge and boiled semolina pasta | 3–24 days | 6 months | 13 g of WP | No significant changes but showed a trend (6 mm vs. 2 mm) after 6 months | No significant changes in sIgE to wheat but showed a trend of increase after up-dosing, followed by a decrease after a 6-month follow-up (47.5 vs. 84.55 vs. 28.75 kUA/L) | Increased sIgG4 and sIgG1 to wheat and a panel of wheat proteins in all patients after 6 months | 83% | Not assessed | 6.25% of doses during up-dosing with none treated with IM epi |
| Sato (2015) [88] | Open-label, nonrandomized, historical control | 18 | 9.0 (5.9–13.6) years | Boiled udon noodles | 5 days | >3 months | 5.2 g of WP | Not assessed | Decreased sIgE to wheat (>100 vs. 43.5 kU/L) after 2 years | Not assessed | 88.9% | OIT: 61.1% Historical control: 9.1% | 26.4% of inpatient doses; 6.8% of outpatient doses with 1 treated with IM epi |
| Khayatzadeh (2016) [89] | Open-label, nonrandomized non-placebo control | Rush method: n = 8 Outpatient method: n = 5 | 7 (5.5–19) years | Bread | Rush method: 3–6 days Outpatient method: 66–87 days | 3 months | 5.2 g of WP | Rush method: decreased (9 mm vs. 6.6 mm) after 3 months; Outpatient method: decreased (9 mm vs. 6.8 mm) after 5 months | Not available | Not assessed | 92.3% | Not assessed | Rush method: 29.6% of doses during up-dosing with 5.6% treated with IM epi; Outpatient method: 2.5% of doses during up-dosing with none treated with IM epi |
| Rekabi (2017) [20] | Open-label, nonrandomized, no control | 12 | 2.25 (2–10) years | Semolina flour and spaghetti (containing pasta) | 6.5 months | 18 months | 70 g of pasta | Decreased (10 mm vs. 3 mm) after 2 years | Decreased total IgE (490 vs. 338.5 IU/mL) after 2 years. sIgE to wheat increased after desensitization, followed by a decrease after the follow-up phase (55.9 vs 65.1 vs. 4.6 IU/mL) | Not assessed | 100% | Not assessed | 0.06% of doses during up-dosing |
| Kulmala (2018) [59] | Multicenter, open-label, nonrandomized, no control | 100 | 11.6 (6.1–18.6) years | Boiled wheat spaghetti | 4.3 months | 12 months | 2 g of WP | Not assessed | The three samples available showed decreased sIgE to wheat, gluten, and ω-5 gliadin after OIT | Not assessed | 57% | Not assessed | 94% of patients; 11 patients used 12 doses of IM epi |
| Nowak-Węgrzyn (2019) [90] | Multicenter, double-blind, randomized, placebo-control | Low-dose group: n = 23 Placebo group: n = 23 and then crossed over to high dose after 1 year | 8.7 (4.2–22.3) years | Vital wheat gluten | 11 months | 2–14 months | Low dose: 1445 mg of WP High dose: 2748 mg of WP | No significant differences in SPT scores between groups at year 1 | No significant differences in sIgE to wheat and ω-5 gliadin between groups at year 1 | Increased sIgG4 to wheat and ω-5 gliadin in the OIT group at year 1 | Placebo group: 0% after 1 year Low dose: 30.4% after 2 years; High dose: 57.1% after 1 year | Low dose: 13.0% after 2 years | Low dose: 15.4% of doses at year 1 with 0.08% treated with IM epi; 3.1% at year 2 with none treated with IM epi; High dose: 13.4% of doses after 1 year with 0.07% treated with IM epi |
| Nagakura (2020) [22] | Open-label, nonrandomized, historical control | 16 | 6.7 (5.8–10.7) years | Boiled udon noodles | 1 month | 11 months | 53 mg of WP | Not assessed | Decreased sIgE to wheat (293 vs. 153.5 kUA/L) and ω-5 gliadin (7.5 vs. 4.1 kUA/L) after 1 year | Increased sIgG to wheat (19.8 vs. 24.1 mgA/L) and ω-5 gliadin (6.0 vs. 7.3 mgA/L) after 1 month. Increased sIgG4 to wheat (2.07 vs. 4.7 mgA/L) and ω-5 gliadin (0.07 vs. 0.09 mgA/L) after 1 month | 88% | OIT: 69% Historical control: 9% | 32.1% of inpatient doses and 4.1% of outpatient doses; none treated with IM epi |
| Ogura (2020) [91] | Multicenter, open-label, randomized, non-placebo control | Low-dose group: n = 12 High-dose group: n = 12 | Low dose group: 5.5 (4.5–5.8) years High dose group: 5.0 (3.7–5.5) years | Boiled udon noodles, boiled pasta, and bread | 24 months | Low dose: 650 mg of WP; High dose: 2.6 g of WP | Not assessed | Decreased sIgE to wheat after 1 year in both groups and decreased sIgE to ω-5 gliadin in the low-dose group | No changes in sIgG and sIgG4 to wheat or ω-5 gliadin in both groups | Low-dose group: 66.7%; High-dose group: 33.3% at year 1 | Low-dose group: 16.7% at year 1, 58.3% at year 2; High-dose group: 50.0% at year 1, 58.3% at year 2 | Low-dose group: 4.76% of doses with 0.02% treated with IM epi; High-dose group: 8.82% of doses with none treated with IM epi | |
| Sugiura (2020) [93] | Open-label, nonrandomized, non-placebo control | 35 | 5 (4–6) years | Boiled udon and somen noodles | 12 months | 10 times greater than the initial dose | Not assessed | Decreased sIgE to wheat (97.0 vs. 51.9 UA/mL) and ω-5 gliadin (4.8 vs. 1.4 UA/mL) after 12–15 months | Not assessed | OIT: 37.5% Control (wheat avoidance): 10.0% | Not assessed | 0.64% of doses with none treated with IM epi | |
| Babaie (2022) [21] | Open-label, nonrandomized, no control | 20 | 6 (2–17) years | Cake and bread | Not mentioned | 3–27 months | 5.28 g of WP | Decreased (9.8 mm vs. 4.3 mm) after a 3-month maintenance phase | sIgE to wheat increased after up-dosing, followed by a decrease after a 3-month maintenance phase | Not assessed | Not mentioned | 47.1% after 3 months, 82.4% after 15 months, and 100% after 27 months | 7.2% of doses during up-dosing with 0.4% treated with IM epi |
| Nagakura (2022) [92] | Open-label, nonrandomized, historical control | 29 | 6.7 (6.3–7.9) years | Boiled udon noodles | 1 month | 35 months | 53 mg of WP | Not assessed | Decreased sIgE to wheat (278 vs. 89.3 kUA/L), gluten (358 vs. 86.9 kUA/L), and ω-5 gliadin (12.7 vs. 3.5 kUA/L) after 3 years | Not assessed | 100% | OIT: 7% at year 1, 28% at year 2, and 41% at year 3; Historical control: 0% | 7.7% of doses at year 1, 3.9% at year 2, and 2.4% at year 3, and 0.03% treated with IM epi at year 1 |
| Sharafian (2022) [94] | Open-label, nonrandomized, no control | 26 | 6.2 (4–11) years | Bread | 6 days | 12 months | 5.2 g of WP | Not assessed | Decreased sIgE to wheat (90.4 vs. 66.5 IU/mL) after 1 year | Not assessed | 100% | 93.3% | 21.4% of doses; 23.8% of reactions treated with IM epi |
| Pourvali (2023) [95] | Open-label, nonrandomized, no control | 19 | 6.6 (2.4–16.6) years | Bread and boiled spaghetti | 6–7.5 months | 7–9 months | 5–10 g of WP | No changes after OIT | Decreased sIgE to wheat (108 vs. 24.6 kU/L) after OIT | No changes in sIgG4 to wheat after OIT | 68.4% | 68.4% | Not mentioned |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zheng, W.; Wai, C.Y.Y.; Sit, J.K.C.; Cheng, N.S.; Leung, C.W.M.; Leung, T.F. Routinely Used and Emerging Diagnostic and Immunotherapeutic Approaches for Wheat Allergy. Biomedicines 2024, 12, 1549. https://doi.org/10.3390/biomedicines12071549
Zheng W, Wai CYY, Sit JKC, Cheng NS, Leung CWM, Leung TF. Routinely Used and Emerging Diagnostic and Immunotherapeutic Approaches for Wheat Allergy. Biomedicines. 2024; 12(7):1549. https://doi.org/10.3390/biomedicines12071549
Chicago/Turabian StyleZheng, Wanqi, Christine Yee Yan Wai, Jason Ka Chun Sit, Nam Sze Cheng, Christy Wing Man Leung, and Ting Fan Leung. 2024. "Routinely Used and Emerging Diagnostic and Immunotherapeutic Approaches for Wheat Allergy" Biomedicines 12, no. 7: 1549. https://doi.org/10.3390/biomedicines12071549
APA StyleZheng, W., Wai, C. Y. Y., Sit, J. K. C., Cheng, N. S., Leung, C. W. M., & Leung, T. F. (2024). Routinely Used and Emerging Diagnostic and Immunotherapeutic Approaches for Wheat Allergy. Biomedicines, 12(7), 1549. https://doi.org/10.3390/biomedicines12071549