
Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions


 ,
, 

 and
and 
Abstract

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Vascular Diseases
2.1. Pathophysiology and Causes of Vascular Diseases
2.2. Effects on Blood Flow and Nutrient Delivery
2.3. Consequences for Brain and Muscle Health
2.4. Current Treatments and Management Strategies
3. Sarcopenia
3.1. Pathophysiology and Contributing Factors
3.2. Sarcopenic Obesity
3.3. Relationship between Vascular Disease and Sarcopenia
3.4. Impact on Physical Function and Quality of Life
3.5. Strategies for Prevention and Treatment
4. Neurodegeneration
4.1. Pathophysiology and Risk Factors
4.2. Link between Vascular Health and Neurodegeneration
4.3. Impact on Cognitive and Motor Functions
4.4. Current Therapeutic Approaches
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
List of Abbreviations
References
- Erkkinen, M.G.; Kim, M.O.; Geschwind, M.D. Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2018, 10, a033118. [Google Scholar] [CrossRef] [PubMed]
- Gonzales, M.M.; Garbarino, V.R.; Pollet, E.; Palavicini, J.P.; Kellogg, D.L., Jr.; Kraig, E.; Orr, M.E. Biological aging processes underlying cognitive decline and neurodegenerative disease. J. Clin. Investig. 2022, 132, e158453. [Google Scholar] [CrossRef] [PubMed]
- Ricci, C. Neurodegenerative Disease: From Molecular Basis to Therapy. Int. J. Mol. Sci. 2024, 25, 967. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Vécsei, L. Revolutionizing our understanding of Parkinson’s disease: Dr. Heinz Reichmann’s pioneering research and future research direction. J. Neural. Transm. 2024. [Google Scholar] [CrossRef]
- Dugger, B.N.; Dickson, D.W. Pathology of Neurodegenerative Diseases. Cold Spring Harb. Perspect. Biol. 2017, 9, a028035. [Google Scholar] [CrossRef]
- Rey, F.; Ottolenghi, S.; Zuccotti, G.V.; Samaja, M.; Carelli, S. Mitochondrial dysfunctions in neurodegenerative diseases: Role in disease pathogenesis, strategies for analysis and therapeutic prospects. Neural Regen. Res. 2022, 17, 754–758. [Google Scholar] [CrossRef]
- Wilson, D.M., 3rd; Cookson, M.R.; Van Den Bosch, L.; Zetterberg, H.; Holtzman, D.M.; Dewachter, I. Hallmarks of neurodegenerative diseases. Cell 2023, 186, 693–714. [Google Scholar] [CrossRef]
- Bhat, A.H.; Dar, K.B.; Anees, S.; Zargar, M.A.; Masood, A.; Sofi, M.A.; Ganie, S.A. Oxidative stress, mitochondrial dysfunction and neurodegenerative diseases; a mechanistic insight. Biomed. Pharmacother. 2015, 74, 101–110. [Google Scholar] [CrossRef]
- Kovacs, G.G. Concepts and classification of neurodegenerative diseases. Handb. Clin. Neurol. 2017, 145, 301–307. [Google Scholar] [CrossRef]
- Samudra, N.; Lane-Donovan, C.; VandeVrede, L.; Boxer, A.L. Tau pathology in neurodegenerative disease: Disease mechanisms and therapeutic avenues. J. Clin. Investig. 2023, 133, e168553. [Google Scholar] [CrossRef]
- Levit, A.; Hachinski, V.; Whitehead, S.N. Neurovascular unit dysregulation, white matter disease, and executive dysfunction: The shared triad of vascular cognitive impairment and Alzheimer disease. Geroscience 2020, 42, 445–465. [Google Scholar] [CrossRef] [PubMed]
- Hayes, G.; Pinto, J.; Sparks, S.N.; Wang, C.; Suri, S.; Bulte, D.P. Vascular smooth muscle cell dysfunction in neurodegeneration. Front. Neurosci. 2022, 16, 1010164. [Google Scholar] [CrossRef] [PubMed]
- Arosio, B.; Calvani, R.; Ferri, E.; Coelho-Junior, H.J.; Carandina, A.; Campanelli, F.; Ghiglieri, V.; Marzetti, E.; Picca, A. Sarcopenia and Cognitive Decline in Older Adults: Targeting the Muscle-Brain Axis. Nutrients 2023, 15, 1853. [Google Scholar] [CrossRef] [PubMed]
- Scarian, E.; Viola, C.; Dragoni, F.; Di Gerlando, R.; Rizzo, B.; Diamanti, L.; Gagliardi, S.; Bordoni, M.; Pansarasa, O. New Insights into Oxidative Stress and Inflammatory Response in Neurodegenerative Diseases. Int. J. Mol. Sci. 2024, 25, 2698. [Google Scholar] [CrossRef]
- Olufunmilayo, E.O.; Gerke-Duncan, M.B.; Holsinger, R.M.D. Oxidative Stress and Antioxidants in Neurodegenerative Disorders. Antioxidants 2023, 12, 517. [Google Scholar] [CrossRef]
- Houldsworth, A. Role of oxidative stress in neurodegenerative disorders: A review of reactive oxygen species and prevention by antioxidants. Brain Commun. 2024, 6, fcad356. [Google Scholar] [CrossRef]
- McGinigle, K.L. Peripheral Vascular Disease. Prim. Care 2024, 51, 83–93. [Google Scholar] [CrossRef]
- Burtscher, J.; Millet, G.P.; Fresa, M.; Lanzi, S.; Mazzolai, L.; Pellegrin, M. The link between impaired oxygen supply and cognitive decline in peripheral artery disease. Prog. Cardiovasc. Dis. 2023, 85, 63–73. [Google Scholar] [CrossRef]
- Sweeney, M.D.; Kisler, K.; Montagne, A.; Toga, A.W.; Zlokovic, B.V. The role of brain vasculature in neurodegenerative disorders. Nat. Neurosci. 2018, 21, 1318–1331. [Google Scholar] [CrossRef]
- Hainsworth, A.H.; Markus, H.S.; Schneider, J.A. Cerebral small vessel disease, hypertension, and vascular contributions to cognitive impairment and dementia. Hypertension 2024, 81, 75–86. [Google Scholar] [CrossRef]
- Hamilton, O.K.L.; Backhouse, E.V.; Janssen, E.; Jochems, A.C.C.; Maher, C.; Ritakari, T.E.; Stevenson, A.J.; Xia, L.; Deary, I.J.; Wardlaw, J.M. Cognitive impairment in sporadic cerebral small vessel disease: A systematic review and meta-analysis. Alzheimer’s Dement. 2021, 17, 665–685. [Google Scholar] [CrossRef] [PubMed]
- Pala, D.; Barbosa, P.O.; Silva, C.T.; de Souza, M.O.; Freitas, F.R.; Volp, A.C.P.; Maranhão, R.C.; Freitas, R.N. Açai (Euterpe oleracea Mart.) dietary intake affects plasma lipids, apolipoproteins, cholesteryl ester transfer to high-density lipoprotein and redox metabolism: A prospective study in women. Clin. Nutr. 2018, 37, 618–623. [Google Scholar] [CrossRef] [PubMed]
- Pasi, M.; Cordonnier, C. Clinical Relevance of Cerebral Small Vessel Diseases. Stroke 2020, 51, 47–53. [Google Scholar] [CrossRef]
- Mena Romo, L.; Gómez-Choco, M. Neuroimaging in small vessel disease. Hipertens. Riesgo Vasc. 2023, 40, 25–33. [Google Scholar] [CrossRef]
- Karvelas, N.; Oh, B.; Wang, E.; Cobigo, Y.; Tsuei, T.; Fitzsimons, S.; Younes, K.; Ehrenberg, A.; Geschwind, M.D.; Schwartz, D.; et al. Enlarged perivascular spaces are associated with white matter injury, cognition and inflammation in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy. Brain Commun. 2024, 6, fcae071. [Google Scholar] [CrossRef] [PubMed]
- Backhouse, E.V.; Boardman, J.P.; Wardlaw, J.M. Cerebral Small Vessel Disease: Early-Life Antecedents and Long-Term Implications for the Brain, Aging, Stroke, and Dementia. Hypertension 2024, 81, 54–74. [Google Scholar] [CrossRef]
- Hoiland, R.L.; Robba, C.; Menon, D.K.; Citerio, G.; Sandroni, C.; Sekhon, M.S. Clinical targeting of the cerebral oxygen cascade to improve brain oxygenation in patients with hypoxic–ischaemic brain injury after cardiac arrest. Intensive Care Med. 2023, 49, 1062–1078. [Google Scholar] [CrossRef]
- Lin, Z.; Lim, C.; Jiang, D.; Soldan, A.; Pettigrew, C.; Oishi, K.; Zhu, Y.; Moghekar, A.; Liu, P.; Albert, M. Longitudinal changes in brain oxygen extraction fraction (OEF) in older adults: Relationship to markers of vascular and Alzheimer’s pathology. Alzheimer’s Dement. 2023, 19, 569–577. [Google Scholar] [CrossRef]
- Mikkelsen, A.C.D.; Thomsen, K.L.; Mookerjee, R.P.; Hadjihambi, A. The role of brain inflammation and abnormal brain oxygen homeostasis in the development of hepatic encephalopathy. Metab. Brain Dis. 2023, 38, 1707–1716. [Google Scholar] [CrossRef]
- Gąsecki, D.; Kwarciany, M.; Nyka, W.; Narkiewicz, K. Hypertension, brain damage and cognitive decline. Curr. Hypertens. Rep. 2013, 15, 547–558. [Google Scholar] [CrossRef]
- Canavan, M.; O’Donnell, M.J. Hypertension and Cognitive Impairment: A Review of Mechanisms and Key Concepts. Front. Neurol. 2022, 13, 821135. [Google Scholar] [CrossRef] [PubMed]
- Pacholko, A.; Iadecola, C. Hypertension, Neurodegeneration, and Cognitive Decline. Hypertension 2024, 81, 991–1007. [Google Scholar] [CrossRef] [PubMed]
- Ungvari, Z.; Toth, P.; Tarantini, S.; Prodan, C.I.; Sorond, F.; Merkely, B.; Csiszar, A. Hypertension-induced cognitive impairment: From pathophysiology to public health. Nat. Rev. Nephrol. 2021, 17, 639–654. [Google Scholar] [CrossRef] [PubMed]
- Meissner, A. Hypertension and the Brain: A Risk Factor for More Than Heart Disease. Cerebrovasc. Dis. 2016, 42, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Baggeroer, C.E.; Cambronero, F.E.; Savan, N.A.; Jefferson, A.L.; Santisteban, M.M. Basic Mechanisms of Brain Injury and Cognitive Decline in Hypertension. Hypertension 2024, 81, 34–44. [Google Scholar] [CrossRef]
- Totoń-Żurańska, J.; Mikolajczyk, T.P.; Saju, B.; Guzik, T.J. Vascular remodelling in cardiovascular diseases: Hypertension, oxidation, and inflammation. Clin. Sci. 2024, 138, 817–850. [Google Scholar] [CrossRef]
- Cai, Z.; Gong, Z.; Li, Z.; Li, L.; Kong, W. Vascular Extracellular Matrix Remodeling and Hypertension. Antioxid. Redox Signal. 2021, 34, 765–783. [Google Scholar] [CrossRef]
- Prado, A.F.; Batista, R.I.M.; Tanus-Santos, J.E.; Gerlach, R.F. Matrix Metalloproteinases and Arterial Hypertension: Role of Oxidative Stress and Nitric Oxide in Vascular Functional and Structural Alterations. Biomolecules 2021, 11, 585. [Google Scholar] [CrossRef]
- Romay, M.C.; Knutsen, R.H.; Ma, F.; Mompeón, A.; Hernandez, G.E.; Salvador, J.; Mirkov, S.; Batra, A.; Sullivan, D.P.; Procissi, D.; et al. Age-related loss of Notch3 underlies brain vascular contractility deficiencies, glymphatic dysfunction, and neurodegeneration in mice. J. Clin. Investig. 2024, 134, e166134. [Google Scholar] [CrossRef]
- Huang, G.; Chen, L.; Lin, Y.; Tang, F.; Huang, H.; Chen, Q.; Cui, L.; Xu, F.; Shen, C. Comparative proteomic analysis of retinal hypoxia-ischemia in an acute ocular hypertension model using tandem mass tag-based quantitative proteomics. Exp. Eye Res. 2024, 247, 110063. [Google Scholar] [CrossRef]
- Ciurică, S.; Lopez-Sublet, M.; Loeys, B.L.; Radhouani, I.; Natarajan, N.; Vikkula, M.; Maas, A.; Adlam, D.; Persu, A. Arterial Tortuosity. Hypertension 2019, 73, 951–960. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Valdés Hernández, M.C.; Muñoz-Maniega, S. What are white matter hyperintensities made of? Relevance to vascular cognitive impairment. J. Am. Heart Assoc. 2015, 4, 001140. [Google Scholar] [CrossRef]
- Shih, A.Y.; Blinder, P.; Tsai, P.S.; Friedman, B.; Stanley, G.; Lyden, P.D.; Kleinfeld, D. The smallest stroke: Occlusion of one penetrating vessel leads to infarction and a cognitive deficit. Nat. Neurosci. 2013, 16, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Wolf, G.; Lotan, A.; Lifschytz, T.; Ben-Ari, H.; Kreisel Merzel, T.; Tatarskyy, P.; Valitzky, M.; Mernick, B.; Avidan, E.; Koroukhov, N.; et al. Differentially Severe Cognitive Effects of Compromised Cerebral Blood Flow in Aged Mice: Association with Myelin Degradation and Microglia Activation. Front. Aging Neurosci. 2017, 9, 191. [Google Scholar] [CrossRef]
- Nakada, T.; Kwee, I.L. Fluid Dynamics Inside the Brain Barrier: Current Concept of Interstitial Flow, Glymphatic Flow, and Cerebrospinal Fluid Circulation in the Brain. Neuroscientist 2019, 25, 155–166. [Google Scholar] [CrossRef] [PubMed]
- Rajeev, V.; Fann, D.Y.; Dinh, Q.N.; Kim, H.A.; De Silva, T.M.; Lai, M.K.P.; Chen, C.L.; Drummond, G.R.; Sobey, C.G.; Arumugam, T.V. Pathophysiology of blood brain barrier dysfunction during chronic cerebral hypoperfusion in vascular cognitive impairment. Theranostics 2022, 12, 1639–1658. [Google Scholar] [CrossRef] [PubMed]
- Mierzwa, A.J.; Marion, C.M.; Sullivan, G.M.; McDaniel, D.P.; Armstrong, R.C. Components of myelin damage and repair in the progression of white matter pathology after mild traumatic brain injury. J. Neuropathol. Exp. Neurol. 2015, 74, 218–232. [Google Scholar] [CrossRef] [PubMed]
- Pavuluri, K.; Huston, J., 3rd; Ehman, R.L.; Manduca, A.; Jack, C.R., Jr.; Senjem, M.L.; Vemuri, P.; Murphy, M.C. Associations between vascular health, brain stiffness and global cognitive function. Brain Commun. 2024, 6, fcae073. [Google Scholar] [CrossRef]
- Vints, W.A.J.; Kušleikienė, S.; Sheoran, S.; Valatkevičienė, K.; Gleiznienė, R.; Himmelreich, U.; Pääsuke, M.; Česnaitienė, V.J.; Levin, O.; Verbunt, J.; et al. Body fat and components of sarcopenia relate to inflammation, brain volume, and neurometabolism in older adults. Neurobiol. Aging 2023, 127, 1–11. [Google Scholar] [CrossRef]
- Rosbergen, M.T.; Wolters, F.J.; Vinke, E.J.; Mattace-Raso, F.U.S.; Roshchupkin, G.V.; Ikram, M.A.; Vernooij, M.W. Cluster-Based White Matter Signatures and the Risk of Dementia, Stroke, and Mortality in Community-Dwelling Adults. Neurology 2024, 103, e209864. [Google Scholar] [CrossRef]
- Gurholt, T.P.; Borda, M.G.; Parker, N.; Fominykh, V.; Kjelkenes, R.; Linge, J.; van der Meer, D.; Sønderby, I.E.; Duque, G.; Westlye, L.T.; et al. Linking sarcopenia, brain structure and cognitive performance: A large-scale UK Biobank study. Brain Commun. 2024, 6, fcae083. [Google Scholar] [CrossRef] [PubMed]
- Larsson, L.; Degens, H.; Li, M.; Salviati, L.; Lee, Y.I.; Thompson, W.; Kirkland, J.L.; Sandri, M. Sarcopenia: Aging-Related Loss of Muscle Mass and Function. Physiol. Rev. 2019, 99, 427–511. [Google Scholar] [CrossRef] [PubMed]
- Kara, M.; Kaymak, B.; Frontera, W.; Ata, A.M.; Ricci, V.; Ekiz, T.; Chang, K.V.; Han, D.S.; Michail, X.; Quittan, M.; et al. Diagnosing sarcopenia: Functional perspectives and a new algorithm from the ISarcoPRM. J. Rehabil. Med. 2021, 53, jrm00209. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Ding, P.; Wu, H.; Yang, P.; Guo, H.; Tian, Y.; Meng, L.; Zhao, Q. Sarcopenia: Molecular regulatory network for loss of muscle mass and function. Front. Nutr. 2023, 10, 1037200. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Cawthon, P.M.; Orwoll, E.S.; Peters, K.E.; Ensrud, K.E.; Cauley, J.A.; Kado, D.M.; Stefanick, M.L.; Shikany, J.M.; Strotmeyer, E.S.; Glynn, N.W. Strong relation between muscle mass determined by D3-creatine dilution, physical performance, and incidence of falls and mobility limitations in a prospective cohort of older men. J. Gerontol. Ser. A 2019, 74, 844–852. [Google Scholar] [CrossRef]
- Yuan, S.; Larsson, S.C. Epidemiology of sarcopenia: Prevalence, risk factors, and consequences. Metabolism 2023, 144, 155533. [Google Scholar] [CrossRef]
- Barazzoni, R.; Cederholm, T.; Zanetti, M.; Cappellari, G.G. Defining and diagnosing sarcopenia: Is the glass now half full? Metabolism 2023, 143, 155558. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Gonzalez, M.C.; Prado, C.M. Sarcopenia ≠ low muscle mass. Eur. Geriatr. Med. 2023, 14, 225–228. [Google Scholar] [CrossRef]
- Donato, A.J.; Machin, D.R.; Lesniewski, L.A. Mechanisms of Dysfunction in the Aging Vasculature and Role in Age-Related Disease. Circ. Res. 2018, 123, 825–848. [Google Scholar] [CrossRef]
- Mengozzi, A.; Pugliese, N.R.; Chiriacò, M.; Masi, S.; Virdis, A.; Taddei, S. Microvascular Ageing Links Metabolic Disease to Age-Related Disorders: The Role of Oxidative Stress and Inflammation in Promoting Microvascular Dysfunction. J. Cardiovasc. Pharmacol. 2021, 78, S78–S87. [Google Scholar] [CrossRef] [PubMed]
- Damluji, A.A.; Alfaraidhy, M.; AlHajri, N.; Rohant, N.N.; Kumar, M.; Al Malouf, C.; Bahrainy, S.; Ji Kwak, M.; Batchelor, W.B.; Forman, D.E.; et al. Sarcopenia and Cardiovascular Diseases. Circulation 2023, 147, 1534–1553. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.K.; Shin, M.J.; Saini, S.K.; Custodero, C.; Aggarwal, M.; Anton, S.D.; Leeuwenburgh, C.; Mankowski, R.T. Vascular dysfunction as a potential culprit of sarcopenia. Exp. Gerontol. 2021, 145, 111220. [Google Scholar] [CrossRef] [PubMed]
- El Assar, M.; Álvarez-Bustos, A.; Sosa, P.; Angulo, J.; Rodríguez-Mañas, L. Effect of Physical Activity/Exercise on Oxidative Stress and Inflammation in Muscle and Vascular Aging. Int. J. Mol. Sci. 2022, 23, 8713. [Google Scholar] [CrossRef]
- Purnamasari, D.; Tetrasiwi, E.N.; Kartiko, G.J.; Astrella, C.; Husam, K.; Laksmi, P.W. Sarcopenia and Chronic Complications of Type 2 Diabetes Mellitus. Rev. Diabet. Stud. 2022, 18, 157–165. [Google Scholar] [CrossRef]
- Banks, N.F.; Rogers, E.M.; Church, D.D.; Ferrando, A.A.; Jenkins, N.D.M. The contributory role of vascular health in age-related anabolic resistance. J. Cachexia Sarcopenia Muscle 2022, 13, 114–127. [Google Scholar] [CrossRef]
- Gallinoro, E.; Paolisso, P.; Candreva, A.; Bermpeis, K.; Fabbricatore, D.; Esposito, G.; Bertolone, D.; Fernandez Peregrina, E.; Munhoz, D.; Mileva, N.; et al. Microvascular Dysfunction in Patients with Type II Diabetes Mellitus: Invasive Assessment of Absolute Coronary Blood Flow and Microvascular Resistance Reserve. Front. Cardiovasc. Med. 2021, 8, 765071. [Google Scholar] [CrossRef]
- Jahn, L.A.; Hartline, L.; Liu, Z.; Barrett, E.J. Metformin improves skeletal muscle microvascular insulin resistance in metabolic syndrome. Am. J. Physiol. Endocrinol. Metab. 2022, 322, E173–E180. [Google Scholar] [CrossRef]
- Ou, Q.; Pan, D. Sarcopenia and risk of cardio-cerebrovascular disease: A two-sample Mendelian randomization study. Biosci. Trends 2023, 17, 413–414. [Google Scholar] [CrossRef]
- Fang, M.; Liu, C.; Liu, Y.; Tang, G.; Li, C.; Guo, L. Association between sarcopenia with incident cardio-cerebrovascular disease: A systematic review and meta-analysis. Biosci. Trends 2023, 17, 293–301. [Google Scholar] [CrossRef]
- Zhang, X.; Ding, L.; Hu, H.; He, H.; Xiong, Z.; Zhu, X. Associations of Body-Roundness Index and Sarcopenia with Cardiovascular Disease among Middle-Aged and Older Adults: Findings from CHARLS. J. Nutr. Health Aging 2023, 27, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.H.; Yang, C.C.; Tu, S.J.; Huang, I.J.; Ganbat, D.; Guo, L.Y. Characteristics of the Electrophysiological Properties of Neuromuscular Motor Units and Its Adaptive Strategy Response in Lower Extremity Muscles for Seniors with Pre-Sarcopenia: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 3063. [Google Scholar] [CrossRef] [PubMed]
- Mosole, S.; Carraro, U.; Kern, H.; Loefler, S.; Zampieri, S. Use it or lose it: Tonic activity of slow motoneurons promotes their survival and preferentially increases slow fiber-type groupings in muscles of old lifelong recreational sportsmen. Eur. J. Transl. Myol. 2016, 26, 5972. [Google Scholar] [CrossRef] [PubMed]
- Barberi, L.; Scicchitano, B.M.; Musaro, A. Molecular and cellular mechanisms of muscle aging and sarcopenia and effects of electrical stimulation in seniors. Eur. J. Transl. Myol. 2015, 25, 5227. [Google Scholar] [CrossRef] [PubMed]
- Sui, S.X.; Williams, L.J.; Holloway-Kew, K.L.; Hyde, N.K.; Pasco, J.A. Skeletal Muscle Health and Cognitive Function: A Narrative Review. Int. J. Mol. Sci. 2020, 22, 255. [Google Scholar] [CrossRef]
- Gustafsson, T.; Ulfhake, B. Sarcopenia: What Is the Origin of This Aging-Induced Disorder? Front. Genet. 2021, 12, 688526. [Google Scholar] [CrossRef]
- Coletti, C.; Acosta, G.F.; Keslacy, S.; Coletti, D. Exercise-mediated reinnervation of skeletal muscle in elderly people: An update. Eur. J. Transl. Myol. 2022, 32, 10416. [Google Scholar] [CrossRef]
- Mosole, S.; Rossini, K.; Kern, H.; Löfler, S.; Fruhmann, H.; Vogelauer, M.; Burggraf, S.; Grim-Stieger, M.; Cvečka, J.; Hamar, D. Reinnervation of Vastus lateralis is increased significantly in seniors (70-years old) with a lifelong history of high-level exercise (2013, revisited here in 2022). Eur. J. Transl. Myol. 2022, 32, 10420. [Google Scholar] [CrossRef]
- Wilkinson, D.J.; Piasecki, M.; Atherton, P. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef]
- Kern, H.; Hofer, C.; Loefler, S.; Zampieri, S.; Gargiulo, P.; Baba, A.; Marcante, A.; Piccione, F.; Pond, A.; Carraro, U. Atrophy, ultra-structural disorders, severe atrophy and degeneration of denervated human muscle in SCI and Aging. Implications for their recovery by Functional Electrical Stimulation, updated 2017. Neurol. Res. 2017, 39, 660–666. [Google Scholar] [CrossRef]
- Li, J.; Lin, Y.; Deng, H.; Su, X.; Feng, W.; Shao, Q.; Zou, K. Association of visceral adiposity index with sarcopenia based on NHANES data. Sci. Rep. 2024, 14, 21169. [Google Scholar] [CrossRef] [PubMed]
- Inoue, D.S.; Janini Gomes, M. Integrative insights into PNI: Low-grade chronic inflammation, skeletal muscle wasting, and brain impairments. Brain Behav. Immun.—Health 2024, 40, 100838. [Google Scholar] [CrossRef]
- Taubert, M.; Roggenhofer, E.; Melie-Garcia, L.; Muller, S.; Lehmann, N.; Preisig, M.; Vollenweider, P.; Marques-Vidal, P.; Lutti, A.; Kherif, F.; et al. Converging patterns of aging-associated brain volume loss and tissue microstructure differences. Neurobiol. Aging 2020, 88, 108–118. [Google Scholar] [CrossRef] [PubMed]
- Trost, W.; Hars, M.; Fernandez, N.; Herrmann, F.; Chevalley, T.; Ferrari, S.; Gold, G.; Rizzoli, R.; Vuilleumier, P.; Trombetti, A. Functional brain changes in sarcopenia: Evidence for differential central neural mechanisms in dynapenic older women. Aging Clin. Exp. Res. 2023, 35, 1015–1025. [Google Scholar] [CrossRef]
- Li, Z.; Wu, X.; Yan, Z.; Cui, Y.; Liu, Y.; Cui, S.; Wang, Y.; Liu, T. Unveiling the muscle-brain axis: A bidirectional mendelian randomization study investigating the causal relationship between sarcopenia-related traits and brain aging. Arch. Gerontol. Geriatr. 2024, 123, 105412. [Google Scholar] [CrossRef]
- Lu, C.-f.; Liu, W.-s.; Cang, X.-m.; Sun, X.; Wang, X.-q.; Wang, C.-h.; Xu, F. The bidirectional associations between sarcopenia-related traits and cognitive performance. Sci. Rep. 2024, 14, 7591. [Google Scholar] [CrossRef]
- Carda, S.; Cisari, C.; Invernizzi, M. Sarcopenia or muscle modifications in neurologic diseases: A lexical or patophysiological difference? Eur. J. Phys. Rehabil. Med. 2013, 49, 119–130. [Google Scholar]
- Meng, S.; He, X.; Fu, X.; Zhang, X.; Tong, M.; Li, W.; Zhang, W.; Shi, X.; Liu, K. The prevalence of sarcopenia and risk factors in the older adult in China: A systematic review and meta-analysis. Front. Public Health 2024, 12, 1415398. [Google Scholar] [CrossRef]
- Beeri, M.S.; Leugrans, S.E.; Delbono, O.; Bennett, D.A.; Buchman, A.S. Sarcopenia is associated with incident Alzheimer’s dementia, mild cognitive impairment, and cognitive decline. J. Am. Geriatr. Soc. 2021, 69, 1826–1835. [Google Scholar] [CrossRef]
- Ladang, A.; Kovacs, S.; Lengelé, L.; Locquet, M.; Beaudart, C.; Reginster, J.-Y.; Bruyère, O.; Cavalier, E. Neurofilament-light chains (NF-L), a biomarker of neuronal damage, is increased in patients with severe sarcopenia: Results of the SarcoPhAge study. Aging Clin. Exp. Res. 2023, 35, 2029–2037. [Google Scholar] [CrossRef]
- Pratt, J.; Pessanha, L.; Narici, M.; Boreham, C.; De Vito, G. Handgrip strength asymmetry as a new biomarker for sarcopenia and individual sarcopenia signatures. Aging Clin. Exp. Res. 2023, 35, 2563–2571. [Google Scholar] [CrossRef] [PubMed]
- Gurholt, T.; Borda, M.G.; Parker, N.; Duque, G.; Westlye, L.T.; Aarsland, D.; Andreassen, O.A. 366. Connecting Sarcopenia, Brain Structure, and Cognitive Performance: Large-Scale Evidence from the UK Biobank. Biol. Psychiatry 2023, 93, S241–S242. [Google Scholar] [CrossRef]
- Arnold, W.D.; Clark, B.C. Neuromuscular junction transmission failure in aging and sarcopenia: The nexus of the neurological and muscular systems. Ageing Res. Rev. 2023, 89, 101966. [Google Scholar] [CrossRef]
- Qian, Z.; Huang, Y.; Zhang, Y.; Yang, N.; Fang, Z.; Zhang, C.; Zhang, L. Metabolic clues to aging: Exploring the role of circulating metabolites in frailty, sarcopenia and vascular aging related traits and diseases. Front. Genet. 2024, 15, 1353908. [Google Scholar] [CrossRef]
- Li, Y.; Hong, M.; Shi, H. Premorbid sarcopenia and functional outcome after acute stroke: A meta-analysis. Asia Pac. J. Clin. Nutr. 2023, 32, 330–338. [Google Scholar] [CrossRef]
- Kopylova, V.; Boronovskiy, S.; Nartsissov, Y. Approaches to vascular network, blood flow, and metabolite distribution modeling in brain tissue. Biophys. Rev. 2023, 15, 1335–1350. [Google Scholar] [CrossRef] [PubMed]
- Wälchli, T.; Bisschop, J.; Carmeliet, P.; Zadeh, G.; Monnier, P.P.; De Bock, K.; Radovanovic, I. Shaping the brain vasculature in development and disease in the single-cell era. Nat. Rev. Neurosci. 2023, 24, 271–298. [Google Scholar] [CrossRef] [PubMed]
- Tayler, H.M.; MacLachlan, R.; Güzel, Ö.; Miners, J.S.; Love, S. Elevated late-life blood pressure may maintain brain oxygenation and slow amyloid-β accumulation at the expense of cerebral vascular damage. Brain Commun. 2023, 5, fcad112. [Google Scholar] [CrossRef]
- Seto, M.; Dumitrescu, L.; Mahoney, E.R.; Sclafani, A.M.; De Jager, P.L.; Menon, V.; Koran, M.E.; Robinson, R.A.; Ruderfer, D.M.; Cox, N.J. Multi-omic characterization of brain changes in the vascular endothelial growth factor family during aging and Alzheimer’s disease. Neurobiol. Aging 2023, 126, 25–33. [Google Scholar] [CrossRef]
- Humphrey, J.D.; Schwartz, M.A. Vascular Mechanobiology: Homeostasis, Adaptation, and Disease. Annu. Rev. Biomed. Eng. 2021, 23, 1–27. [Google Scholar] [CrossRef]
- Tomiyama, H. Vascular function: A key player in hypertension. Hypertens. Res. 2023, 46, 2145–2158. [Google Scholar] [CrossRef] [PubMed]
- Trimm, E.; Red-Horse, K. Vascular endothelial cell development and diversity. Nat. Rev. Cardiol. 2023, 20, 197–210. [Google Scholar] [CrossRef] [PubMed]
- Simionescu, M. Implications of early structural-functional changes in the endothelium for vascular disease. Arterioscler. Thromb. Vasc. Biol. 2007, 27, 266–274. [Google Scholar] [CrossRef]
- Xu, J.; Shi, G.P. Vascular wall extracellular matrix proteins and vascular diseases. Biochim. Biophys. Acta 2014, 1842, 2106–2119. [Google Scholar] [CrossRef]
- Fraile-Martinez, O.; De Leon-Oliva, D.; Boaru, D.L.; De Castro-Martinez, P.; Garcia-Montero, C.; Barrena-Blázquez, S.; García-García, J.; García-Honduvilla, N.; Alvarez-Mon, M.; Lopez-Gonzalez, L. Connecting epigenetics and inflammation in vascular senescence: State of the art, biomarkers and senotherapeutics. Front. Genet. 2024, 15, 1345459. [Google Scholar] [CrossRef]
- Sutton, N.R.; Malhotra, R.; St. Hilaire, C.; Aikawa, E.; Blumenthal, R.S.; Gackenbach, G.; Goyal, P.; Johnson, A.; Nigwekar, S.U.; Shanahan, C.M. Molecular mechanisms of vascular health: Insights from vascular aging and calcification. Arterioscler. Thromb. Vasc. Biol. 2023, 43, 15–29. [Google Scholar] [CrossRef]
- Cheng, J.; Wen, J.; Wang, N.; Wang, C.; Xu, Q.; Yang, Y. Ion Channels and Vascular Diseases. Arterioscler. Thromb. Vasc. Biol. 2019, 39, e146–e156. [Google Scholar] [CrossRef]
- Sacchetti, S.; Puricelli, C.; Mennuni, M.; Zanotti, V.; Giacomini, L.; Giordano, M.; Dianzani, U.; Patti, G.; Rolla, R. Research into New Molecular Mechanisms in Thrombotic Diseases Paves the Way for Innovative Therapeutic Approaches. Int. J. Mol. Sci. 2024, 25, 2523. [Google Scholar] [CrossRef] [PubMed]
- Rajendran, P.; Rengarajan, T.; Thangavel, J.; Nishigaki, Y.; Sakthisekaran, D.; Sethi, G.; Nishigaki, I. The vascular endothelium and human diseases. Int. J. Biol. Sci. 2013, 9, 1057–1069. [Google Scholar] [CrossRef]
- Erusalimsky, J.D. Vascular endothelial senescence: From mechanisms to pathophysiology. J. Appl. Physiol. 2009, 106, 326–332. [Google Scholar] [CrossRef]
- Bloom, S.I.; Islam, M.T.; Lesniewski, L.A.; Donato, A.J. Mechanisms and consequences of endothelial cell senescence. Nat. Rev. Cardiol. 2023, 20, 38–51. [Google Scholar] [CrossRef] [PubMed]
- Direito, R.; Barbalho, S.M.; Sepodes, B.; Figueira, M.E. Plant-Derived Bioactive Compounds: Exploring Neuroprotective, Metabolic, and Hepatoprotective Effects for Health Promotion and Disease Prevention. Pharmaceutics 2024, 16, 577. [Google Scholar] [CrossRef]
- Han, Y.; Kim, S.Y. Endothelial senescence in vascular diseases: Current understanding and future opportunities in senotherapeutics. Exp. Mol. Med. 2023, 55, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Rahman, M.S.; Islam, R.; Bhuiyan, M.I.H. Ion transporter cascade, reactive astrogliosis and cerebrovascular diseases. Front. Pharmacol. 2024, 15, 1374408. [Google Scholar] [CrossRef] [PubMed]
- Coste, B.; Delmas, P. PIEZO Ion Channels in Cardiovascular Functions and Diseases. Circ. Res. 2024, 134, 572–591. [Google Scholar] [CrossRef] [PubMed]
- Kalaria, R.N. Cerebrovascular disease and mechanisms of cognitive impairment: Evidence from clinicopathological studies in humans. Stroke 2012, 43, 2526–2534. [Google Scholar] [CrossRef]
- Zimmerman, B.; Rypma, B.; Gratton, G.; Fabiani, M. Age-related changes in cerebrovascular health and their effects on neural function and cognition: A comprehensive review. Psychophysiology 2021, 58, e13796. [Google Scholar] [CrossRef]
- Erickson, M.A.; Dohi, K.; Banks, W.A. Neuroinflammation: A common pathway in CNS diseases as mediated at the blood-brain barrier. Neuroimmunomodulation 2012, 19, 121–130. [Google Scholar] [CrossRef]
- Lacoste, B.; Prat, A.; Freitas-Andrade, M.; Gu, C. The Blood-Brain Barrier: Composition, Properties, and Roles in Brain Health. Cold Spring Harb. Perspect. Biol. 2024; early release. [Google Scholar] [CrossRef]
- Archie, S.R.; Al Shoyaib, A.; Cucullo, L. Blood-Brain Barrier Dysfunction in CNS Disorders and Putative Therapeutic Targets: An Overview. Pharmaceutics 2021, 13, 1779. [Google Scholar] [CrossRef]
- Kumar, P.; Kumar, D.; Jha, S.K.; Jha, N.K.; Ambasta, R.K. Ion Channels in Neurological Disorders. Adv. Protein Chem. Struct. Biol. 2016, 103, 97–136. [Google Scholar] [CrossRef] [PubMed]
- Song, S.; Luo, L.; Sun, B.; Sun, D. Roles of glial ion transporters in brain diseases. Glia 2020, 68, 472–494. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Collier, J.M.; Abdul-Rahman, N.-H.; Capuk, O.; Zhang, Z.; Begum, G. Dysregulation of Ion Channels and Transporters and Blood-Brain Barrier Dysfunction in Alzheimer’s Disease and Vascular Dementia. Aging Dis. 2024, 15, 1748–1770. [Google Scholar]
- Korszun-Karbowniczak, J.; Krysiak, Z.J.; Saluk, J.; Niemcewicz, M.; Zdanowski, R. The Progress in Molecular Transport and Therapeutic Development in Human Blood–Brain Barrier Models in Neurological Disorders. Cell. Mol. Neurobiol. 2024, 44, 34. [Google Scholar] [CrossRef]
- Khor, S.L.Q.; Ng, K.Y.; Koh, R.Y.; Chye, S.M. Blood-brain Barrier and Neurovascular Unit Dysfunction in Parkinson’s Disease: From Clinical Insights to Pathogenic Mechanisms and Novel Therapeutic Approaches. CNS Neurol. Disord.-Drug Targets (Former. Curr. Drug Targets-CNS Neurol. Disord.) 2024, 23, 315–330. [Google Scholar] [CrossRef]
- Mendelson, S.J.; Prabhakaran, S. Diagnosis and management of transient ischemic attack and acute ischemic stroke: A review. JAMA 2021, 325, 1088–1098. [Google Scholar] [CrossRef]
- Shao, C.; Wang, J.; Tian, J.; Tang, Y.-d. Coronary artery disease: From mechanism to clinical practice. In Coronary Artery Disease: Therapeutics and Drug Discovery. Advances in Experimental Medicine and Biology; Springer: Singapore, 2020; Volume 1177, pp. 1–36. [Google Scholar]
- Weintraub, N.L. Understanding abdominal aortic aneurysm. N. Engl. J. Med. 2009, 361, 1114. [Google Scholar] [CrossRef]
- Anagnostakos, J.; Lal, B.K. Abdominal aortic aneurysms. Progress Cardiovasc. Dis. 2021, 65, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Chen, G.; Lin, B.; Zhong, L.; Jiang, X.; Lu, H. Integrative analysis of single-Cell RNA sequencing and experimental validation in the study of abdominal aortic aneurysm progression. Gene 2024, 929, 148820. [Google Scholar] [CrossRef]
- Tao, J.; Cao, X.; Yu, B.; Qu, A. Vascular stem/progenitor cells in vessel injury and repair. Front. Cardiovasc. Med. 2022, 9, 845070. [Google Scholar] [CrossRef]
- Paloschi, V.; Pauli, J.; Winski, G.; Wu, Z.; Li, Z.; Botti, L.; Meucci, S.; Conti, P.; Rogowitz, F.; Glukha, N. Utilization of an Artery-on-a-Chip to Unravel Novel Regulators and Therapeutic Targets in Vascular Diseases. Adv. Healthc. Mater. 2024, 13, 2302907. [Google Scholar] [CrossRef] [PubMed]
- Qadura, M.; Syed, M.H.; Anand, S.; Bosch, J.; Connolly, S.; Aboyans, V.; Muehlhofer, E.; Yusuf, S.; Eikelboom, J. The predictive value of interarm systolic blood pressure differences in patients with vascular disease: Sub-analysis of the COMPASS trial. Atherosclerosis 2023, 372, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Sillesen, H.H. Peripheral vascular disease. In Textbook of Diabetes; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2024; pp. 755–767. [Google Scholar]
- Villa-Bellosta, R. Vascular calcification: Key roles of phosphate and pyrophosphate. Int. J. Mol. Sci. 2021, 22, 13536. [Google Scholar] [CrossRef] [PubMed]
- Bessueille, L.; Magne, D. Inflammation: A culprit for vascular calcification in atherosclerosis and diabetes. Cell. Mol. Life Sci. 2015, 72, 2475–2489. [Google Scholar] [CrossRef]
- Pescatore, L.A.; Gamarra, L.F.; Liberman, M. Multifaceted mechanisms of vascular calcification in aging. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1307–1316. [Google Scholar] [CrossRef]
- Ren, S.-C.; Mao, N.; Yi, S.; Ma, X.; Zou, J.-Q.; Tang, X.; Fan, J.-M. Vascular calcification in chronic kidney disease: An update and perspective. Aging Dis. 2022, 13, 673. [Google Scholar] [CrossRef]
- Zhang, H.; Dhalla, N.S. The role of pro-Inflammatory cytokines in the pathogenesis of cardiovascular disease. Int. J. Mol. Sci. 2024, 25, 1082. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.-Y.; Lim, S.; Park, S. Role of inflammation in arterial calcification. Korean Circ. J. 2021, 51, 114–125. [Google Scholar] [CrossRef]
- Hao, N.; Zhou, Z.; Zhang, F.; Li, Y.; Hu, R.; Zou, J.; Zheng, R.; Wang, L.; Xu, L.; Tan, W. Interleukin-29 Accelerates Vascular Calcification via JAK2/STAT3/BMP2 Signaling. J. Am. Heart Assoc. 2023, 12, e027222. [Google Scholar] [CrossRef]
- Russo, M.P.; Grande-Ratti, M.F.; Burgos, M.A.; Molaro, A.A.; Bonella, M.B. Prevalence of diabetes, epidemiological characteristics and vascular complications. Arch. Cardiol. México 2023, 93, 30–36. [Google Scholar] [CrossRef]
- Sadat, N.; Lojenburg, J.H.; Scharfschwerdt, M.; Klinger, M.; Fujita, B.; Ensminger, S. Characteristic calcification behavior of five surgical aortic valve bioprostheses models: An in vitro study. Health Sci. Rep. 2024, 7, e2304. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.-H.; Kawano, T.; Murata, M.; Toita, R. Vascular calcification and cellular signaling pathways as potential therapeutic targets. Life Sci. 2023, 336, 122309. [Google Scholar] [CrossRef] [PubMed]
- Izzo, C.; Secondulfo, C.; Bilancio, G.; Visco, V.; Virtuoso, N.; Migliarino, S.; Ciccarelli, M.; Di Pietro, P.; La Mura, L.; Damato, A. Chronic Kidney Disease with Mineral Bone Disorder and Vascular Calcification: An Overview. Life 2024, 14, 418. [Google Scholar] [CrossRef]
- Tousoulis, D.; Kampoli, A.-M.; Tentolouris Nikolaos Papageorgiou, C.; Stefanadis, C. The role of nitric oxide on endothelial function. Curr. Vasc. Pharmacol. 2012, 10, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Suvorava, T.; Metry, S.; Pick, S.; Kojda, G. Alterations in endothelial nitric oxide synthase activity and their relevance to blood pressure. Biochem. Pharmacol. 2022, 205, 115256. [Google Scholar] [CrossRef]
- Castellon, X.; Bogdanova, V. Chronic inflammatory diseases and endothelial dysfunction. Aging Dis. 2016, 7, 81. [Google Scholar] [CrossRef] [PubMed]
- Higashi, Y. Roles of oxidative stress and inflammation in vascular endothelial dysfunction-related disease. Antioxidants 2022, 11, 1958. [Google Scholar] [CrossRef]
- Schulman, I.H.; Zhou, M.-S. Vascular insulin resistance: A potential link between cardiovascular and metabolic diseases. Curr. Hypertens. Rep. 2009, 11, 48–55. [Google Scholar] [CrossRef]
- Wu, H.; Ballantyne, C.M. Metabolic inflammation and insulin resistance in obesity. Circ. Res. 2020, 126, 1549–1564. [Google Scholar] [CrossRef]
- Claassen, J.A.; Thijssen, D.H.; Panerai, R.B.; Faraci, F.M. Regulation of cerebral blood flow in humans: Physiology and clinical implications of autoregulation. Physiol. Rev. 2021, 101, 1487–1559. [Google Scholar] [CrossRef]
- Wang, S.; Tang, C.; Liu, Y.; Border, J.J.; Roman, R.J.; Fan, F. Impact of impaired cerebral blood flow autoregulation on cognitive impairment. Front. Aging 2022, 3, 1077302. [Google Scholar] [CrossRef] [PubMed]
- Tohirova, J.; Shernazarov, F. Atherosclerosis: Causes, symptoms, diagnosis, treatment and prevention. Sci. Innov. 2022, 1, 7–12. [Google Scholar]
- Alfarisi, H.A.H.; Mohamed, Z.B.H.; Ibrahim, M.B. Basic pathogenic mechanisms of atherosclerosis. Egypt. J. Basic Appl. Sci. 2020, 7, 116–125. [Google Scholar] [CrossRef]
- BUILDER, V. Cardiovascular Pathologies and Disorders. In Mosby’s Pathology for Massage Professionals-E-Book; Elsevier: Amsterdam, The Netherlands, 2021; p. 234. [Google Scholar]
- Golledge, J. Update on the pathophysiology and medical treatment of peripheral artery disease. Nat. Rev. Cardiol. 2022, 19, 456–474. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, K.; Ninomiya, T. Stroke and cerebrovascular diseases in patients with chronic kidney disease. Lancet Neurol. 2014, 13, 823–833. [Google Scholar] [CrossRef]
- Zhao, Q.; Yan, T.; Chopp, M.; Venkat, P.; Chen, J. Brain–kidney interaction: Renal dysfunction following ischemic stroke. J. Cereb. Blood Flow Metab. 2020, 40, 246–262. [Google Scholar] [CrossRef]
- Makrantonaki, E.; Wlaschek, M.; Scharffetter-Kochanek, K. Pathogenesis of wound healing disorders in the elderly. JDDG J. Der Dtsch. Dermatol. Ges. 2017, 15, 255–275. [Google Scholar] [CrossRef]
- Bowers, S.; Franco, E. Chronic wounds: Evaluation and management. Am. Fam. Physician 2020, 101, 159–166. [Google Scholar]
- Haller, H.L.; Sander, F.; Popp, D.; Rapp, M.; Hartmann, B.; Demircan, M.; Nischwitz, S.P.; Kamolz, L.P. Oxygen, pH, lactate, and metabolism—How old knowledge and new insights might be combined for new wound treatment. Medicina 2021, 57, 1190. [Google Scholar] [CrossRef]
- Chen, Y.; Ding, B.-S. Comprehensive review of the vascular niche in regulating organ regeneration and fibrosis. Stem Cells Transl. Med. 2022, 11, 1135–1142. [Google Scholar] [CrossRef]
- Gardener, H.; Wright, C.B.; Rundek, T.; Sacco, R.L. Brain health and shared risk factors for dementia and stroke. Nat. Rev. Neurol. 2015, 11, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Bir, S.C.; Khan, M.W.; Javalkar, V.; Toledo, E.G.; Kelley, R.E. Emerging concepts in vascular dementia: A review. J. Stroke Cerebrovasc. Dis. 2021, 30, 105864. [Google Scholar] [CrossRef] [PubMed]
- Chojdak-Łukasiewicz, J.; Dziadkowiak, E.; Zimny, A.; Paradowski, B. Cerebral small vessel disease: A review. Adv. Clin. Exp. Med. 2021, 30, 349–356. [Google Scholar] [CrossRef]
- Khan, A.; Kalaria, R.N.; Corbett, A.; Ballard, C. Update on vascular dementia. J. Geriatr. Psychiatry Neurol. 2016, 29, 281–301. [Google Scholar] [CrossRef]
- Vasilijević, S.R.; Vuković, M.; Jerkić, L. Cognitive and language deficits in vascular dementia. Acta Medica Median. 2021, 60. [Google Scholar] [CrossRef]
- D’Onofrio, G.; Sancarlo, D.; Addante, F.; Ciccone, F.; Cascavilla, L.; Paris, F.; Picoco, M.; Nuzzaci, C.; Elia, A.C.; Greco, A. Caregiver burden characterization in patients with Alzheimer’s disease or vascular dementia. Int. J. Geriatr. Psychiatry 2015, 30, 891–899. [Google Scholar] [CrossRef]
- Xu, J.; Qiu, C. Worldwide economic costs and societal burden of dementia. Biomark. Preclin. Alzheimer’s Dis. 2018, 1, 3–13. [Google Scholar]
- Béjot, Y.; Daubail, B.; Giroud, M. Epidemiology of stroke and transient ischemic attacks: Current knowledge and perspectives. Rev. Neurol. 2016, 172, 59–68. [Google Scholar] [CrossRef]
- Lioutas, V.-A.; Ivan, C.S.; Himali, J.J.; Aparicio, H.J.; Leveille, T.; Romero, J.R.; Beiser, A.S.; Seshadri, S. Incidence of transient ischemic attack and association with long-term risk of stroke. JAMA 2021, 325, 373–381. [Google Scholar] [CrossRef]
- Schorr, E.N.; Peden-McAlpine, C.; Treat-Jacobson, D.; Lindquist, R. Characterization of the peripheral artery disease symptom experience. Geriatr. Nurs. 2015, 36, 293–300. [Google Scholar] [CrossRef]
- Abola, M.T.B.; Evans, N.S.; Ratchford, E.V. Vascular disease patient information page: Leg cramps. Vasc. Med. 2022, 27, 415–417. [Google Scholar] [CrossRef]
- Gardner, A.W.; Montgomery, P.S.; Wang, M.; Shen, B. Association between calf muscle oxygen saturation with ambulatory function and quality of life in symptomatic patients with peripheral artery disease. J. Vasc. Surg. 2020, 72, 632–642. [Google Scholar] [CrossRef] [PubMed]
- Cerqueira, M.S.; Do Nascimento, J.D.S.; Maciel, D.G.; Barboza, J.A.M.; Vieira, W.H.D.B. Effects of blood flow restriction without additional exercise on strength reductions and muscular atrophy following immobilization: A systematic review. J. Sport Health Sci. 2020, 9, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Blebea, J.; Fukaya, E.; Moore, K.S.; Lurie, F. Mechanochemical chemically assisted ablation of varicose veins for venous insufficiency: American vein and lymphatic society position statement. Phlebology, 2024; online first. [Google Scholar] [CrossRef]
- Guo, S.a.; DiPietro, L.A. Factors affecting wound healing. J. Dent. Res. 2010, 89, 219–229. [Google Scholar] [CrossRef]
- Wilkinson, H.N.; Hardman, M.J. Wound healing: Cellular mechanisms and pathological outcomes. Open Biol. 2020, 10, 200223. [Google Scholar] [CrossRef] [PubMed]
- Hess, D.A.; Verma, S.; Bhatt, D.; Bakbak, E.; Terenzi, D.C.; Puar, P.; Cosentino, F. Vascular repair and regeneration in cardiometabolic diseases. Eur. Heart J. 2022, 43, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Evans, C.E.; Iruela-Arispe, M.L.; Zhao, Y.-Y. Mechanisms of endothelial regeneration and vascular repair and their application to regenerative medicine. Am. J. Pathol. 2021, 191, 52–65. [Google Scholar] [CrossRef]
- Marco, M.; Valentina, I.; Daniele, M.; Valerio, D.R.; Andrea, P.; Roberto, G.; Laura, G.; Luigi, U. Peripheral arterial disease in persons with diabetic foot ulceration: A current comprehensive overview. Curr. Diabetes Rev. 2021, 17, 474–485. [Google Scholar] [CrossRef]
- Doughty, K.N.; Del Pilar, N.X.; Audette, A.; Katz, D.L. Lifestyle medicine and the management of cardiovascular disease. Curr. Cardiol. Rep. 2017, 19, 116. [Google Scholar] [CrossRef]
- Blumenthal, J.A.; Hinderliter, A.L.; Smith, P.J.; Mabe, S.; Watkins, L.L.; Craighead, L.; Ingle, K.; Tyson, C.; Lin, P.-H.; Kraus, W.E. Effects of lifestyle modification on patients with resistant hypertension: Results of the TRIUMPH randomized clinical trial. Circulation 2021, 144, 1212–1226. [Google Scholar] [CrossRef]
- Sadat-Ebrahimi, S.R.; Parnianfard, N.; Vahed, N.; Babaei, H.; Ghojazadeh, M.; Tang, S.; Azarpazhooh, A. An evidence-based systematic review of the off-label uses of lisinopril. Br. J. Clin. Pharmacol. 2018, 84, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Beltran Romero, L.M.; Vallejo-Vaz, A.J.; Muniz Grijalvo, O. Cerebrovascular disease and statins. Front. Cardiovasc. Med. 2021, 8, 778740. [Google Scholar] [CrossRef] [PubMed]
- Liao, X.-Z.; Fu, Y.-H.; Ma, J.-Y.; Zhu, W.-G.; Yuan, P. Non-vitamin K antagonist oral anticoagulants versus warfarin in patients with atrial fibrillation and peripheral artery disease: A systematic review and meta-analysis. Cardiovasc. Drugs Ther. 2020, 34, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Mogul, A.; Leppien, E.E.; Laughlin, E.; Spinler, S.A. Aspirin for primary prevention of cardiovascular disease: A review of recent literature and updated guideline recommendations. Expert Opin. Pharmacother. 2021, 22, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mishima, E.; Suzuki, T.; Ito, S. Selection of patients for angioplasty for treatment of atherosclerotic renovascular disease: Predicting responsive patients. Am. J. Hypertens. 2020, 33, 391–401. [Google Scholar] [CrossRef]
- Zhao, K.; Zeng, Z.; He, Y.; Zhao, R.; Niu, J.; Sun, H.; Li, S.; Dong, J.; Jing, Z.; Zhou, J. Recent advances in targeted therapy for inflammatory vascular diseases. J. Control. Release 2024, 372, 730–750. [Google Scholar] [CrossRef]
- Yu, X.; Wang, B.; Qiu, C.; He, Y.; Chen, T.; Zhu, Q.; Li, Z.; Wu, Z. A systematic review and meta-analysis of primary bypass surgery compared with bypass surgery after endovascular treatment in peripheral artery disease patients. J. Vasc. Surg. 2023, 78, 1335–1345.e4. [Google Scholar] [CrossRef]
- Minniti, G.; Laurindo, L.F.; Machado, N.M.; Duarte, L.G.; Guiguer, E.L.; Araujo, A.C.; Dias, J.A.; Lamas, C.B.; Nunes, Y.C.; Bechara, M.D. Mangifera indica L., By-Products, and Mangiferin on Cardio-Metabolic and Other Health Conditions: A Systematic Review. Life 2023, 13, 2270. [Google Scholar] [CrossRef]
- Nunes, Y.C.; de Oliveira Santos, G.; Machado, N.M.; Otoboni, A.M.; Laurindo, L.F.; Bishayee, A.; Fimognari, C.; Bishayee, A.; Barbalho, S.M. Peanut (Arachis hypogaea L.) seeds and by-products in metabolic syndrome and cardiovascular disorders: A systematic review of clinical studies. Phytomedicine 2023, 123, 155170. [Google Scholar] [CrossRef]
- Takeda, L.N.; Laurindo, L.F.; Guiguer, E.L.; Bishayee, A.; Araújo, A.C.; Ubeda, L.C.C.; Goulart, R.d.A.; Barbalho, S.M. Psidium guajava L.: A systematic review of the multifaceted health benefits and economic importance. Food Rev. Int. 2023, 39, 4333–4363. [Google Scholar] [CrossRef]
- Laurindo, L.; Barbalho, S.; Araújo, A. Açaí (Euterpe oleracea Mart.) in health and disease: A critical review. Nutrients 2023, 15, 989. [Google Scholar] [CrossRef] [PubMed]
- Imaizumi, V.M.; Laurindo, L.F.; Manzan, B.; Guiguer, E.L.; Oshiiwa, M.; Otoboni, A.M.M.B.; Araujo, A.C.; Tofano, R.J.; Barbalho, S.M. Garlic: A systematic review of the effects on cardiovascular diseases. Crit. Rev. Food Sci. Nutr. 2023, 63, 6797–6819. [Google Scholar] [CrossRef] [PubMed]
- Pagotto, G.L.d.O.; Santos, L.M.O.d.; Osman, N.; Lamas, C.B.; Laurindo, L.F.; Pomini, K.T.; Guissoni, L.M.; Lima, E.P.d.; Goulart, R.d.A.; Catharin, V.M.S. Ginkgo biloba: A Leaf of Hope in the Fight against Alzheimer’s Dementia: Clinical Trial Systematic Review. Antioxidants 2024, 13, 651. [Google Scholar] [CrossRef]
- Lu, M.; Zhang, L.; Pan, J.; Shi, H.; Zhang, M.; Li, C. Advances in the study of the vascular protective effects and molecular mechanisms of hawthorn (Crataegus anamesa Sarg.) extracts in cardiovascular diseases. Food Funct. 2023, 14, 5870–5890. [Google Scholar] [CrossRef]
- Cloud, A.; Vilcins, D.; McEwen, B. The effect of hawthorn (Crataegus spp.) on blood pressure: A systematic review. Adv. Integr. Med. 2020, 7, 167–175. [Google Scholar] [CrossRef]
- Dwivedi, S.; Chopra, D. Revisiting Terminalia arjuna–an ancient cardiovascular drug. J. Tradit. Complement. Med. 2014, 4, 224–231. [Google Scholar] [CrossRef]
- Thakur, S.; Kaurav, H.; Chaudhary, G. Terminalia arjuna: A potential ayurvedic cardio tonic. Int. J. Res. Appl. Sci. Biotechnol. 2021, 8, 227–236. [Google Scholar] [CrossRef]
- Dutta, A.; Das, M. Terminalia arjuna and Cardiovascular Protection: A Comprehensive Overview. In Ancient and Traditional Foods, Plants, Herbs and Spices Used in Cardiovascular Health and Disease; CRC Press: Boca Raton, FL, USA, 2023; pp. 93–110. [Google Scholar]
- Trombetti, A.; Reid, K.; Hars, M.; Herrmann, F.; Pasha, E.; Phillips, E.; Fielding, R. Age-associated declines in muscle mass, strength, power, and physical performance: Impact on fear of falling and quality of life. Osteoporos. Int. 2016, 27, 463–471. [Google Scholar] [CrossRef]
- Kim, H.; Ranjit, R.; Claflin, D.R.; Georgescu, C.; Wren, J.D.; Brooks, S.V.; Miller, B.F.; Ahn, B. Unacylated Ghrelin Protects Against Age-Related Loss of Muscle Mass and Contractile Dysfunction in Skeletal Muscle. Aging cell 2024, e14323. [Google Scholar] [CrossRef]
- Rodrigues, F.; Domingos, C.; Monteiro, D.; Morouço, P. A review on aging, sarcopenia, falls, and resistance training in community-dwelling older adults. Int. J. Environ. Res. Public Health 2022, 19, 874. [Google Scholar] [CrossRef]
- Marzetti, E.; Calvani, R.; Bernabei, R.; Leeuwenburgh, C. Apoptosis in skeletal myocytes: A potential target for interventions against sarcopenia and physical frailty—A mini-review. Gerontology 2012, 58, 99–106. [Google Scholar] [CrossRef]
- Dao, T.; Green, A.E.; Kim, Y.A.; Bae, S.-J.; Ha, K.-T.; Gariani, K.; Lee, M.-r.; Menzies, K.J.; Ryu, D. Sarcopenia and muscle aging: A brief overview. Endocrinol. Metab. 2020, 35, 716–732. [Google Scholar] [CrossRef]
- Wiedmer, P.; Jung, T.; Castro, J.P.; Pomatto, L.C.; Sun, P.Y.; Davies, K.J.; Grune, T. Sarcopenia–Molecular mechanisms and open questions. Ageing Res. Rev. 2021, 65, 101200. [Google Scholar] [CrossRef]
- Ranieri, F.; Di Lazzaro, V. The role of motor neuron drive in muscle fatigue. Neuromuscul. Disord. 2012, 22, S157–S161. [Google Scholar] [CrossRef]
- Lepley, A.S.; Lepley, L.K. Mechanisms of arthrogenic muscle inhibition. J. Sport Rehabil. 2021, 31, 707–716. [Google Scholar] [CrossRef]
- Morley, J.E. Hormones and sarcopenia. Curr. Pharm. Des. 2017, 23, 4484–4492. [Google Scholar] [CrossRef]
- Tezze, C.; Sandri, M.; Tessari, P. Anabolic resistance in the pathogenesis of sarcopenia in the elderly: Role of nutrition and exercise in young and old people. Nutrients 2023, 15, 4073. [Google Scholar] [CrossRef]
- Pan, L.; Xie, W.; Fu, X.; Lu, W.; Jin, H.; Lai, J.; Zhang, A.; Yu, Y.; Li, Y.; Xiao, W. Inflammation and sarcopenia: A focus on circulating inflammatory cytokines. Exp. Gerontol. 2021, 154, 111544. [Google Scholar] [CrossRef]
- Wang, J.; Leung, K.-S.; Chow, S.K.-H.; Cheung, W.-H. Inflammation and age-associated skeletal muscle deterioration (sarcopaenia). J. Orthop. Transl. 2017, 10, 94–101. [Google Scholar] [CrossRef]
- Sharma, B.; Dabur, R. Role of pro-inflammatory cytokines in regulation of skeletal muscle metabolism: A systematic review. Curr. Med. Chem. 2020, 27, 2161–2188. [Google Scholar] [CrossRef]
- Mahmoodi, M.; Shateri, Z.; Nazari, S.A.; Nouri, M.; Nasimi, N.; Sohrabi, Z.; Dabbaghmanesh, M.H. Association between oxidative balance score and sarcopenia in older adults. Sci. Rep. 2024, 14, 5362. [Google Scholar] [CrossRef] [PubMed]
- Alhmly, H.F.; Fielding, R.A. A critical review of current worldwide definitions of sarcopenia. Calcif. Tissue Int. 2024, 114, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Nishikawa, H.; Asai, A.; Fukunishi, S.; Nishiguchi, S.; Higuchi, K. Metabolic syndrome and sarcopenia. Nutrients 2021, 13, 3519. [Google Scholar] [CrossRef] [PubMed]
- Capel, F.; Pinel, A.; Walrand, S. Accumulation of intramuscular toxic lipids, a link between fat mass accumulation and sarcopenia. OCL Oilseeds Fats Crop. Lipids 2019, 26, 24. [Google Scholar] [CrossRef]
- de Lima, E.P.; Moretti, R.C.; Torres Pomini, K., Jr.; Laurindo, L.F.; Sloan, K.P.; Sloan, L.A.; Castro, M.V.M.d.; Baldi, E., Jr.; Ferraz, B.F.R.; de Souza Bastos Mazuqueli Pereira, E. Glycolipid Metabolic Disorders, Metainflammation, Oxidative Stress, and Cardiovascular Diseases: Unraveling Pathways. Biology 2024, 13, 519. [Google Scholar] [CrossRef] [PubMed]
- Masenga, S.K.; Kabwe, L.S.; Chakulya, M.; Kirabo, A. Mechanisms of oxidative stress in metabolic syndrome. Int. J. Mol. Sci. 2023, 24, 7898. [Google Scholar] [CrossRef]
- Gu, X.; Lu, S.; Fan, M.; Xu, S.; Lin, G.; Zhao, Y.; Zhao, W.; Liu, X.; Dong, X.; Zhang, X. Compound Z526 alleviates chemotherapy-induced cachectic muscle loss by ameliorating oxidative stress-driven protein metabolic imbalance and apoptosis. Eur. J. Pharmacol. 2024, 974, 176538. [Google Scholar] [CrossRef]
- Delafontaine, P.; Yoshida, T. The renin-angiotensin system and the biology of skeletal muscle: Mechanisms of muscle wasting in chronic disease states. Trans. Am. Clin. Climatol. Assoc. 2016, 127, 245. [Google Scholar] [PubMed]
- Sasaki, K.-I.; Fukumoto, Y. Sarcopenia as a comorbidity of cardiovascular disease. J. Cardiol. 2022, 79, 596–604. [Google Scholar] [CrossRef]
- He, Y.; Xie, W.; Li, H.; Jin, H.; Zhang, Y.; Li, Y. Cellular senescence in sarcopenia: Possible mechanisms and therapeutic potential. Front. Cell Dev. Biol. 2022, 9, 793088. [Google Scholar] [CrossRef]
- Granic, A.; Suetterlin, K.; Shavlakadze, T.; Grounds, M.D.; Sayer, A.A. Hallmarks of ageing in human skeletal muscle and implications for understanding the pathophysiology of sarcopenia in women and men. Clin. Sci. 2023, 137, 1721–1751. [Google Scholar] [CrossRef] [PubMed]
- Priego, T.; Martín, A.; González-Hedström, D.; Granado, M.; López-Calderón, A. Role of hormones in sarcopenia. In Vitamins and Hormones; Elsevier: Amsterdam, The Netherlands, 2021; Volume 115, pp. 535–570. [Google Scholar]
- White, T.A.; LeBrasseur, N.K. Myostatin and sarcopenia: Opportunities and challenges-a mini-review. Gerontology 2014, 60, 289–293. [Google Scholar] [CrossRef] [PubMed]
- Yasar, E.; Tek, N.A.; Tekbudak, M.Y.; Yurtdaş, G.; Gülbahar, Ö.; Uyar, G.Ö.; Ural, Z.; Çelik, Ö.M.; Erten, Y. The relationship between myostatin, inflammatory markers, and sarcopenia in patients with chronic kidney disease. J. Ren. Nutr. 2022, 32, 677–684. [Google Scholar] [CrossRef]
- Kwon, Y.N.; Yoon, S.S. Sarcopenia: Neurological point of view. J. Bone Metab. 2017, 24, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Delbono, O.; Rodrigues, A.C.Z.; Bonilla, H.J.; Messi, M.L. The emerging role of the sympathetic nervous system in skeletal muscle motor innervation and sarcopenia. Ageing Res. Rev. 2021, 67, 101305. [Google Scholar] [CrossRef]
- Daily, J.W.; Park, S. Sarcopenia is a cause and consequence of metabolic dysregulation in aging humans: Effects of gut dysbiosis, glucose dysregulation, diet and lifestyle. Cells 2022, 11, 338. [Google Scholar] [CrossRef]
- Antuña, E.; Cachán-Vega, C.; Bermejo-Millo, J.C.; Potes, Y.; Caballero, B.; Vega-Naredo, I.; Coto-Montes, A.; Garcia-Gonzalez, C. Inflammaging: Implications in sarcopenia. Int. J. Mol. Sci. 2022, 23, 15039. [Google Scholar] [CrossRef]
- Ooi, H.; Welch, C. Obstacles to the Early Diagnosis and Management of Sarcopenia: Current Perspectives. Clin. Interv. Aging 2024, 12, 323–332. [Google Scholar] [CrossRef]
- Qiu, C.; Yang, X.; Yu, P. Sarcopenia: Pathophysiology and Treatment Strategies. Endocr. Metab. Immune Disord.-Drug Targets (Former. Curr. Drug Targets-Immune Endocr. Metab. Disord.) 2024, 24, 31–38. [Google Scholar] [CrossRef]
- Hirsch, C.H.; Hategan, A. Physiology and pathology of aging. In Geriatric Psychiatry: A Case-Based Textbook; Springer: Berlin/Heidelberg, Germany, 2024; pp. 3–29. [Google Scholar]
- Rubin, J.; Nambi, V.; Chambless, L.E.; Steffes, M.W.; Juraschek, S.P.; Coresh, J.; Sharrett, A.R.; Selvin, E. Hyperglycemia and arterial stiffness: The atherosclerosis risk in the communities study. Atherosclerosis 2012, 225, 246–251. [Google Scholar] [CrossRef]
- Kim, H.L.; Jo, S.H. Arterial Stiffness and Heart Failure with Preserved Ejection Fraction. J. Korean Med. Sci. 2024, 39, e195. [Google Scholar] [CrossRef] [PubMed]
- Laurindo, L.F.; Barbalho, S.M.; Guiguer, E.L.; da Silva Soares de Souza, M.; de Souza, G.A.; Fidalgo, T.M.; Araújo, A.C.; de Souza Gonzaga, H.F.; de Bortoli Teixeira, D.; de Oliveira Silva Ullmann, T.; et al. GLP-1a: Going beyond Traditional Use. Int. J. Mol. Sci. 2022, 23, 739. [Google Scholar] [CrossRef] [PubMed]
- Laurindo, L.F.; Laurindo, L.F.; Rodrigues, V.D.; Catharin, V.; Simili, O.A.G.; Barboza, G.O.; Catharin, V.C.S.; Sloan, K.P.; Barbalho, S.M. Unraveling the rationale and conducting a comprehensive assessment of AdipoRon (adiponectin receptor agonist) as a candidate drug for diabetic nephropathy and cardiomyopathy prevention and intervention—A systematic review. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2024. [Google Scholar] [CrossRef]
- Ikonomidis, I.; Thymis, J. The vicious circle of arterial elasticity, blood pressure, glycemia, and renal function. Hypertens. Res. 2023, 46, 1599–1602. [Google Scholar] [CrossRef]
- Laurent, S.; Agabiti-Rosei, C.; Bruno, R.M.; Rizzoni, D. Microcirculation and macrocirculation in hypertension: A dangerous cross-link? Hypertension 2022, 79, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Tsuchikura, S.; Shoji, T.; Kimoto, E.; Shinohara, K.; Hatsuda, S.; Koyama, H.; Emoto, M.; Nishizawa, Y. Central versus peripheral arterial stiffness in association with coronary, cerebral and peripheral arterial disease. Atherosclerosis 2010, 211, 480–485. [Google Scholar] [CrossRef]
- Yu, S.; McEniery, C.M. Central versus peripheral artery stiffening and cardiovascular risk. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1028–1033. [Google Scholar] [CrossRef]
- Fantin, F.; Giani, A.; Manzato, G.; Zampieri, A.; Comellato, G.; Urbani, S.; Zoico, E.; Mazzali, G.; Zamboni, M. Sarcopenia, sarcopenic obesity, and arterial stiffness among older adults. Front. Cardiovasc. Med. 2024, 11, 1272854. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Ozcan, S.G.G.; Bekircavusoglu, A.F.; Catalkaya, S. Sarcopenia is Associated with Aortic Arch Calcification on Chest X-ray in Unselected Middle-and Older-Aged Patients. Res. Sq. 2024. [Google Scholar] [CrossRef]
- Aziz, M.; Jacob, A.; Matsuda, A.; Wang, P. milk fat globule-EGF factor 8 expression, function and plausible signal transduction in resolving inflammation. Apoptosis 2011, 16, 1077–1086. [Google Scholar] [CrossRef]
- Ni, Y.-Q.; Zhan, J.-K.; Liu, Y.-S. Roles and mechanisms of MFG-E8 in vascular aging-related diseases. Ageing Res. Rev. 2020, 64, 101176. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Jiang, M.; Fang, Z.T.; Chen, Z.; Li, L.; Liu, Z.; Wang, J.; Yin, X.; Wang, J.; Wu, M. Current evidence of synaptic dysfunction after stroke: Cellular and molecular mechanisms. CNS Neurosci. Ther. 2024, 30, e14744. [Google Scholar] [CrossRef] [PubMed]
- Danese, E.; Montagnana, M.; Lippi, G. Proteomics and frailty: A clinical overview. Expert Rev. Proteom. 2018, 15, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Tuo, Q.z.; Zhang, S.t.; Lei, P. Mechanisms of neuronal cell death in ischemic stroke and their therapeutic implications. Med. Res. Rev. 2022, 42, 259–305. [Google Scholar] [CrossRef] [PubMed]
- Gunsch, G.; Paradie, E.; Townsend, K.L. Peripheral nervous system glia in support of metabolic tissue functions. Trends Endocrinol. Metab. 2023, 34, 622–639. [Google Scholar] [CrossRef]
- Kuzuya, M. Drug-related sarcopenia as a secondary sarcopenia. Geriatr. Gerontol. Int. 2024, 24, 195–203. [Google Scholar] [CrossRef]
- Swidan, S. Drug-Related Sarcopenia. In Metabolic Therapies in Orthopedics, 2nd ed.; CRC Press: Boca Raton, FL, USA, 2018; pp. 239–249. [Google Scholar]
- Matsumoto, A.; Yoshimura, Y.; Nagano, F.; Shimazu, S.; Shiraishi, A.; Kido, Y.; Bise, T. Potentially inappropriate medications are negatively associated with functional recovery in patients with sarcopenia after stroke. Aging Clin. Exp. Res. 2022, 34, 2845–2855. [Google Scholar] [CrossRef]
- Saied, S.; Prokopidis, K.; Adenaya, A.; Isanejad, M.; Sankaranarayanan, R. Is sarcopenia an associated factor of increased administration of specific medications in patients with heart failure? A systematic review and meta-analysis. Front. Cardiovasc. Med. 2024, 11, 1293537. [Google Scholar] [CrossRef]
- Zamboni, M.; Mazzali, G.; Brunelli, A.; Saatchi, T.; Urbani, S.; Giani, A.; Rossi, A.P.; Zoico, E.; Fantin, F. The role of crosstalk between adipose cells and myocytes in the pathogenesis of sarcopenic obesity in the elderly. Cells 2022, 11, 3361. [Google Scholar] [CrossRef]
- Ciudin, A.; Simó-Servat, A.; Palmas, F.; Barahona, M.J. Sarcopenic obesity: A new challenge in the clinical practice. Endocrinol. Diabetes Nutr. (Engl. Ed.) 2020, 67, 672–681. [Google Scholar] [CrossRef]
- Benz, E.; Pinel, A.; Guillet, C.; Capel, F.; Pereira, B.; De Antonio, M.; Pouget, M.; Cruz-Jentoft, A.J.; Eglseer, D.; Topinkova, E.; et al. Sarcopenia and Sarcopenic Obesity and Mortality Among Older People. JAMA Netw. Open 2024, 7, e243604. [Google Scholar] [CrossRef] [PubMed]
- Silveira, E.A.; da Silva Filho, R.R.; Spexoto, M.C.B.; Haghighatdoost, F.; Sarrafzadegan, N.; de Oliveira, C. The role of sarcopenic obesity in cancer and cardiovascular disease: A synthesis of the evidence on pathophysiological aspects and clinical implications. Int. J. Mol. Sci. 2021, 22, 4339. [Google Scholar] [CrossRef]
- Evans, K.; Abdelhafiz, D.; Abdelhafiz, A.H. Sarcopenic obesity as a determinant of cardiovascular disease risk in older people: A systematic review. Postgrad. Med. 2021, 133, 831–842. [Google Scholar] [CrossRef] [PubMed]
- Bellafronte, N.T.; de Queirós Mattoso Ono, A.; Chiarello, P.G. Sarcopenic obesity in chronic kidney disease: Challenges in diagnosis using different diagnostic criteria. Med. Princ. Pract. 2021, 30, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Lynch, G.; Murphy, C.; de Marco Castro, E.; Roche, H. Inflammation and metabolism: The role of adiposity in sarcopenic obesity. Proc. Nutr. Soc. 2020, 79, 435–447. [Google Scholar] [CrossRef]
- Gonzalez, A.; Simon, F.; Achiardi, O.; Vilos, C.; Cabrera, D.; Cabello-Verrugio, C. The critical role of oxidative stress in sarcopenic obesity. Oxidative Med. Cell. Longev. 2021, 2021, 4493817. [Google Scholar] [CrossRef]
- Hong, S.-h.; Choi, K.M. Sarcopenic obesity, insulin resistance, and their implications in cardiovascular and metabolic consequences. Int. J. Mol. Sci. 2020, 21, 494. [Google Scholar] [CrossRef]
- Jurdana, M.; Cemazar, M. Sarcopenic obesity in cancer. Radiol. Oncol. 2024, 58, 1–8. [Google Scholar] [CrossRef]
- Carneiro, I.P.; Mazurak, V.C.; Prado, C.M. Clinical implications of sarcopenic obesity in cancer. Curr. Oncol. Rep. 2016, 18, 62. [Google Scholar] [CrossRef]
- Chou, H.-H.; Lai, T.-J.; Yen, C.-H.; Chang, P.-S.; Pan, J.-C.; Lin, P.-T. Sarcopenic obesity tendency and nutritional status is related to the risk of sarcopenia, frailty, depression and quality of life in patients with dementia. Int. J. Environ. Res. Public Health 2022, 19, 2492. [Google Scholar] [CrossRef]
- Zhang, J.; Na, X.; Li, Z.; Ji, J.S.; Li, G.; Yang, H.; Yang, Y.; Tan, Y.; Zhang, J.; Xi, M. Sarcopenic obesity is part of obesity paradox in dementia development: Evidence from a population-based cohort study. BMC Med. 2024, 22, 133. [Google Scholar] [CrossRef]
- Long, D.; Liu, M.; Li, H.; Song, J.; Jiang, X.; Wang, G.; Yang, X. Dysbacteriosis induces abnormal neurogenesis via LPS in a pathway requiring NF-κB/IL-6. Pharmacol. Res. 2021, 167, 105543. [Google Scholar] [CrossRef] [PubMed]
- Lyra e Silva, N.M.; Gonçalves, R.A.; Pascoal, T.A.; Lima-Filho, R.A.; Resende, E.d.P.F.; Vieira, E.L.; Teixeira, A.L.; de Souza, L.C.; Peny, J.A.; Fortuna, J.T. Pro-inflammatory interleukin-6 signaling links cognitive impairments and peripheral metabolic alterations in Alzheimer’s disease. Transl. Psychiatry 2021, 11, 251. [Google Scholar] [CrossRef]
- Mucher, P.; Batmyagmar, D.; Perkmann, T.; Repl, M.; Radakovics, A.; Ponocny-Seliger, E.; Lukas, I.; Fritzer-Szekeres, M.; Lehrner, J.; Knogler, T. Basal myokine levels are associated with quality of life and depressed mood in older adults. Psychophysiology 2021, 58, e13799. [Google Scholar] [CrossRef] [PubMed]
- Sadier, N.S.; El Hajjar, F.; Al Sabouri, A.A.K.; Abou-Abbas, L.; Siomava, N.; Almutary, A.G.; Tambuwala, M.M. Irisin: An unveiled bridge between physical exercise and a healthy brain. Life Sci. 2024, 339, 122393. [Google Scholar] [CrossRef] [PubMed]
- Pignataro, P.; Dicarlo, M.; Zerlotin, R.; Zecca, C.; Dell’Abate, M.T.; Buccoliero, C.; Logroscino, G.; Colucci, S.; Grano, M. FNDC5/Irisin system in neuroinflammation and neurodegenerative diseases: Update and novel perspective. Int. J. Mol. Sci. 2021, 22, 1605. [Google Scholar] [CrossRef]
- Zheng, S.; Chen, N.; Kang, X.; Hu, Y.; Shi, S. Irisin alleviates FFA induced β-cell insulin resistance and inflammatory response through activating PI3K/AKT/FOXO1 signaling pathway. Endocrine 2022, 75, 740–751. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, M.; Tan, J.; Pei, X.; Lu, C.; Xin, Y.; Deng, S.; Zhao, F.; Gao, Y.; Gong, Y. Irisin ameliorates neuroinflammation and neuronal apoptosis through integrin αVβ5/AMPK signaling pathway after intracerebral hemorrhage in mice. J. Neuroinflamm. 2022, 19, 82. [Google Scholar] [CrossRef]
- Hou, L.; Wang, X.; Li, P.; Zhang, H.; Yao, Y.; Liu, Z.; Wang, J.; Liu, W. Adiposity modifies the association between heart failure risk and glucose metabolic disorder in older individuals: A community-based prospective cohort study. Cardiovasc. Diabetol. 2024, 23, 318. [Google Scholar] [CrossRef]
- Khadra, D.; Itani, L.; Tannir, H.; Kreidieh, D.; El Masri, D.; El Ghoch, M. Association between sarcopenic obesity and higher risk of type 2 diabetes in adults: A systematic review and meta-analysis. World J. Diabetes 2019, 10, 311. [Google Scholar] [CrossRef]
- Pilati, I.; Slee, A.; Frost, R. Sarcopenic obesity and depression: A systematic review. J. Frailty Aging 2022, 11, 51–58. [Google Scholar] [CrossRef]
- Kueck, P.J.; Morris, J.K.; Stanford, J.A. Current Perspectives: Obesity and Neurodegeneration-Links and Risks. Degener. Neurol. Neuromuscul. Dis. 2024, 13, 111–129. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.-H.; Mok, J.-O. Recent Updates on Associations among Various Obesity Metrics and Cognitive Impairment: From Body Mass Index to Sarcopenic Obesity. J. Obes. Metab. Syndr. 2022, 31, 287. [Google Scholar] [CrossRef] [PubMed]
- Mastelić, T.; Višić, V.; Marasović, T.B.; Milanović, M.; Kralj, Ž.; Burilović, E.; Pernat, M.; Vukorepa, D.; Rančić, N.; Baković, M. Sarkopenija kod osoba oboljelih od demencije/Sarcopenia in Persons Suffering from Dementia. Soc. Psihijat. 2023, 51, 40–353. [Google Scholar]
- Booranasuksakul, U.; Macdonald, I.A.; Stephan, B.C.; Siervo, M. Body Composition, Sarcopenic Obesity, and Cognitive Function in Older Adults: Findings from the National Health and Nutrition Examination Survey (NHANES) 1999–2002 and 2011–2014. J. Am. Nutr. Assoc. 2024, 43, 539–552. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, H.; Izumiya, Y.; Hayashi, O.; Ichii, M.; Tsujimoto, Y.; Yoshiyama, M. Dynapenia is an independent predictor of cardio-cerebrovascular events in patients undergoing hemodialysis. Heart Vessel. 2022, 37, 1066–1074. [Google Scholar] [CrossRef]
- He, N.; Zhang, Y.; Zhang, L.; Zhang, S.; Ye, H. Relationship between sarcopenia and cardiovascular diseases in the elderly: An overview. Front. Cardiovasc. Med. 2021, 8, 743710. [Google Scholar] [CrossRef]
- Pizzimenti, M.; Meyer, A.; Charles, A.L.; Giannini, M.; Chakfé, N.; Lejay, A.; Geny, B. Sarcopenia and peripheral arterial disease: A systematic review. J. Cachexia Sarcopenia Muscle 2020, 11, 866–886. [Google Scholar] [CrossRef]
- Cretoiu, S.M.; Zugravu, C.A. Nutritional considerations in preventing muscle atrophy. In Muscle Atrophy; Xiao, J., Ed.; Springer: Singapore, 2018; Volume 1088, pp. 497–528. [Google Scholar]
- Muñoz-Cánoves, P.; Neves, J.; Sousa-Victor, P. Understanding muscle regenerative decline with aging: New approaches to bring back youthfulness to aged stem cells. FEBS J. 2020, 287, 406–416. [Google Scholar] [CrossRef]
- Mojikon, F.D.; Kasimin, M.E.; Molujin, A.M.; Gansau, J.A.; Jawan, R. Probiotication of Nutritious Fruit and Vegetable Juices: An Alternative to Dairy-Based Probiotic Functional Products. Nutrients 2022, 14, 3457. [Google Scholar] [CrossRef]
- Kim, K.; Anderson, E.M.; Scali, S.T.; Ryan, T.E. Skeletal muscle mitochondrial dysfunction and oxidative stress in peripheral arterial disease: A unifying mechanism and therapeutic target. Antioxidants 2020, 9, 1304. [Google Scholar] [CrossRef] [PubMed]
- Damiano, S.; Muscariello, E.; La Rosa, G.; Di Maro, M.; Mondola, P.; Santillo, M. Dual role of reactive oxygen species in muscle function: Can antioxidant dietary supplements counteract age-related sarcopenia? Int. J. Mol. Sci. 2019, 20, 3815. [Google Scholar] [CrossRef] [PubMed]
- Thoma, A.; Akter-Miah, T.; Reade, R.L.; Lightfoot, A.P. Targeting reactive oxygen species (ROS) to combat the age-related loss of muscle mass and function. Biogerontology 2020, 21, 475–484. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Mendes, I.; Ong, B.; Prado, C.M.; Mocciaro, G.; Mazidi, M.; Lubrano, C.; Lenzi, A.; Donini, L.M.; Siervo, M. Sarcopenic obesity and insulin resistance: Application of novel body composition models. Nutrition 2020, 75, 110765. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.-j.; Zhu, C.-f. Causal relationship between insulin resistance and sarcopenia. Diabetol. Metab. Syndr. 2023, 15, 46. [Google Scholar] [CrossRef] [PubMed]
- Cleasby, M.E.; Jamieson, P.; Atherton, P.J. Insulin resistance and sarcopenia: Mechanistic links between common co-morbidities. J. Endocrinol. 2016, 229, R67–R81. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Flato, U.A.P.; Tofano, R.J.; Goulart, R.d.A.; Guiguer, E.L.; Detregiachi, C.R.P.; Buchaim, D.V.; Araújo, A.C.; Buchaim, R.L.; Reina, F.T.R. Physical exercise and myokines: Relationships with sarcopenia and cardiovascular complications. Int. J. Mol. Sci. 2020, 21, 3607. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Camargo, F.C.; Perfeito, A.; Ciano, B.B.; Coelho, C.T.; Apolinário, G.A.; Vicentin, I.D.N.; Andreasi, J.C.; Boaro, B.L.; Tofano, R.J. Examining the Correlations between the Visceral Adiposity Index and Various Anthropometric, Biochemical, and Insulin Resistance Parameters in Brazilians: Findings from a Cross-Sectional Study. Preprints 2024, 2024050699. [Google Scholar] [CrossRef]
- Lopez-Candales, A.; Burgos, P.M.H.; Hernandez-Suarez, D.F.; Harris, D. Linking chronic inflammation with cardiovascular disease: From normal aging to the metabolic syndrome. J. Nat. Sci. 2017, 3, e341. [Google Scholar]
- Pansuria, M.; Xi, H.; Li, L.; Yang, X.-F.; Wang, H. Insulin resistance, metabolic stress, and atherosclerosis. Front. Biosci. (Sch. Ed.) 2012, 4, 916. [Google Scholar]
- Poznyak, A.; Grechko, A.V.; Poggio, P.; Myasoedova, V.A.; Alfieri, V.; Orekhov, A.N. The diabetes mellitus–atherosclerosis connection: The role of lipid and glucose metabolism and chronic inflammation. Int. J. Mol. Sci. 2020, 21, 1835. [Google Scholar] [CrossRef] [PubMed]
- Silveira Rossi, J.L.; Barbalho, S.M.; Reverete de Araujo, R.; Bechara, M.D.; Sloan, K.P.; Sloan, L.A. Metabolic syndrome and cardiovascular diseases: Going beyond traditional risk factors. Diabetes/Metab. Res. Rev. 2022, 38, e3502. [Google Scholar] [CrossRef] [PubMed]
- Wakabayashi, H.; Sakuma, K. Comprehensive approach to sarcopenia treatment. Curr. Clin. Pharmacol. 2014, 9, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T. Selected methods of resistance training for prevention and treatment of sarcopenia. Cells 2022, 11, 1389. [Google Scholar] [CrossRef] [PubMed]
- Malafarina, V.; Uriz-Otano, F.; Iniesta, R.; Gil-Guerrero, L. Effectiveness of nutritional supplementation on muscle mass in treatment of sarcopenia in old age: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.Y.; Kwon, K.-S. Pharmacological interventions for treatment of sarcopenia: Current status of drug development for sarcopenia. Ann. Geriatr. Med. Res. 2019, 23, 98. [Google Scholar] [CrossRef]
- Ispoglou, T.; Wilson, O.; McCullough, D.; Aldrich, L.; Ferentinos, P.; Lyall, G.; Stavropoulos-Kalinoglou, A.; Duckworth, L.; Brown, M.A.; Sutton, L. A narrative review of non-pharmacological strategies for managing sarcopenia in older adults with cardiovascular and metabolic diseases. Biology 2023, 12, 892. [Google Scholar] [CrossRef]
- Rivera, F.B.; Escolano, B.T.; Nifas, F.M.; Choi, S.; Carado, G.P.; Lerma, E.; Vijayaraghavan, K.; Yu, M.G. Interrelationship of Sarcopenia and Cardiovascular Diseases: A review of potential mechanisms and management. J. ASEAN Fed. Endocr. Soc. 2024, 39, 69. [Google Scholar] [CrossRef]
- Fábrega-Cuadros, R.; Hita-Contreras, F.; Martínez-Amat, A.; Jiménez-García, J.D.; Achalandabaso-Ochoa, A.; Lavilla-Lerma, L.; García-Garro, P.A.; Álvarez-Salvago, F.; Aibar-Almazán, A. Associations between the severity of sarcopenia and health-related quality of life in community-dwelling middle-aged and older adults. Int. J. Environ. Res. Public Health 2021, 18, 8026. [Google Scholar] [CrossRef]
- Reis, J.M.S.; Alves, L.S.; Vogt, B.P. According to revised EWGSOP sarcopenia consensus cut-off points, low physical function is associated with nutritional status and quality of life in maintenance hemodialysis patients. J. Ren. Nutr. 2022, 32, 469–475. [Google Scholar] [CrossRef]
- Haider, S.; Luger, E.; Kapan, A.; Titze, S.; Lackinger, C.; Schindler, K.E.; Dorner, T.E. Associations between daily physical activity, handgrip strength, muscle mass, physical performance and quality of life in prefrail and frail community-dwelling older adults. Qual. Life Res. 2016, 25, 3129–3138. [Google Scholar] [CrossRef] [PubMed]
- Swan, L.; Martin, N.; Horgan, N.F.; Warters, A.; O’Sullivan, M. Assessing Sarcopenia, Frailty, and Malnutrition in Community-Dwelling Dependant Older Adults—An Exploratory Home-Based Study of an Underserved Group in Research. Int. J. Environ. Res. Public Health 2022, 19, 16133. [Google Scholar] [CrossRef] [PubMed]
- Liguori, I.; Russo, G.; Aran, L.; Bulli, G.; Curcio, F.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D. Sarcopenia: Assessment of disease burden and strategies to improve outcomes. Clin. Interv. Aging 2018, 13, 913–927. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Chen, C. Towards a mechanistic understanding of depression, anxiety, and their comorbidity: Perspectives from cognitive neuroscience. Front. Media SA 2023, 17, 1268156. [Google Scholar] [CrossRef]
- Nogueira, G.; Fidelix, Y.L.; Nascimento, J.R.A.d.; Oliveira, D.V.d. Physical activity and sedentary behavior as predictors of fear of falling and risk of sarcopenia in older adults. Fisioter. Mov. 2023, 36, e36118. [Google Scholar] [CrossRef]
- Öztürk, G.B.; Kiliç, C.; Bozkurt, M.; Karan, M.A. Prevalence and associates of fear of falling among community-dwelling older adults. J. Nutr. Health Aging 2021, 25, 433–439. [Google Scholar] [CrossRef]
- Manrique-Espinoza, B.; Salinas-Rodríguez, A.; Rosas-Carrasco, O.; Gutiérrez-Robledo, L.M.; Avila-Funes, J.A. Sarcopenia is associated with physical and mental components of health-related quality of life in older adults. J. Am. Med. Dir. Assoc. 2017, 18, 636.e1–636.e5. [Google Scholar] [CrossRef]
- Bruyère, O.; Beaudart, C.; Ethgen, O.; Reginster, J.-Y.; Locquet, M. The health economics burden of sarcopenia: A systematic review. Maturitas 2019, 119, 61–69. [Google Scholar] [CrossRef]
- Mijnarends, D.; Schols, J.; Halfens, R.; Meijers, J.; Luiking, Y.; Verlaan, S.; Evers, S. Burden-of-illness of Dutch community-dwelling older adults with sarcopenia: Health related outcomes and costs. Eur. Geriatr. Med. 2016, 7, 276–284. [Google Scholar] [CrossRef]
- Denison, H.J.; Cooper, C.; Sayer, A.A.; Robinson, S.M. Prevention and optimal management of sarcopenia: A review of combined exercise and nutrition interventions to improve muscle outcomes in older people. Clin. Interv. Aging 2015, 10, 859–869. [Google Scholar] [CrossRef]
- Negm, A.M.; Lee, J.; Hamidian, R.; Jones, C.A.; Khadaroo, R.G. Management of sarcopenia: A network meta-analysis of randomized controlled trials. J. Am. Med. Dir. Assoc. 2022, 23, 707–714. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.-Q.; Xiao, G.-L.; Hu, P.-W.; He, Y.-Q.; Lv, S.; Xiao, W.-F. Possible sarcopenia: Early screening and intervention-narrative review. Ann. Palliat. Med. 2020, 9, 4283293–4284293. [Google Scholar] [CrossRef] [PubMed]
- Cannataro, R.; Cione, E.; Bonilla, D.A.; Cerullo, G.; Angelini, F.; D’Antona, G. Strength training in elderly: An useful tool against sarcopenia. Front. Sports Act. Living 2022, 4, 950949. [Google Scholar] [CrossRef]
- Barbalho, S.M.; de Alvares Goulart, R.; Minniti, G.; Bechara, M.D.; de Castro, M.V.M.; Dias, J.A.; Laurindo, L.F. Unraveling the rationale and conducting a comprehensive assessment of KD025 (Belumosudil) as a candidate drug for inhibiting adipogenic differentiation—A systematic review. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2024, 397, 2681–2699. [Google Scholar] [CrossRef] [PubMed]
- Mellen, R.; Girotto, O.; Marques, E.; Laurindo, L.; Grippa, P.; Mendes, C. Insights into Pathogenesis, Nutritional and Drug Approach in Sarcopenia: A Systematic Review. Biomedicines 2023, 11, 136. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Calvani, R.; Picca, A.; Tosato, M.; Landi, F.; Marzetti, E. Engagement in aerobic exercise is associated with a reduced prevalence of sarcopenia and severe sarcopenia in Italian older adults. J. Pers. Med. 2023, 13, 655. [Google Scholar] [CrossRef]
- Aoki, K.; Konno, M.; Honda, K.; Abe, T.; Nagata, T.; Takehara, M.; Sugasawa, T.; Takekoshi, K.; Ohmori, H. Habitual aerobic exercise diminishes the effects of sarcopenia in senescence-accelerated mice Prone8 model. Geriatrics 2020, 5, 48. [Google Scholar] [CrossRef]
- Hickson, M. Nutritional interventions in sarcopenia: A critical review. Proc. Nutr. Soc. 2015, 74, 378–386. [Google Scholar] [CrossRef]
- Damanti, S.; Azzolino, D.; Roncaglione, C.; Arosio, B.; Rossi, P.; Cesari, M. Efficacy of nutritional interventions as stand-alone or synergistic treatments with exercise for the management of sarcopenia. Nutrients 2019, 11, 1991. [Google Scholar] [CrossRef]
- Breen, L.; Phillips, S.M. Skeletal muscle protein metabolism in the elderly: Interventions to counteract the’anabolic resistance’of ageing. Nutr. Metab. 2011, 8, 68. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Sloan, L.A.; Araujo, A.C.; Laurindo, L.F.; Sloan, K.P. Vitamin D and Its Role on Inflammation, Oxidative Stress and Cardiovascular Disease. In Lipophilic Vitamins in Health and Disease; Springer: Berlin/Heidelberg, Germany, 2024; pp. 291–311. [Google Scholar]
- Lalia, A. Omega-3 Fatty Acids to Combat Sarcopenia; College of Medicine—Mayo Clinic: Rochester, MN, USA, 2016. [Google Scholar]
- Bruyère, O.; Reginster, J.-Y.; Beaudart, C. Lifestyle approaches to prevent and retard sarcopenia: A narrative review. Maturitas 2022, 161, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Barazzoni, R.; Bischoff, S.; Boirie, Y.; Busetto, L.; Cederholm, T.; Dicker, D.; Toplak, H.; Van Gossum, A.; Yumuk, V.; Vettor, R. Sarcopenic obesity: Time to meet the challenge. Obes. Facts 2018, 11, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Picca, A.; Fanelli, F.; Calvani, R.; Mulè, G.; Pesce, V.; Sisto, A.; Pantanelli, C.; Bernabei, R.; Landi, F.; Marzetti, E. Gut dysbiosis and muscle aging: Searching for novel targets against sarcopenia. Mediat. Inflamm. 2018, 2018, 7026198. [Google Scholar] [CrossRef]
- Liu, C.; Cheung, W.H.; Li, J.; Chow, S.K.H.; Yu, J.; Wong, S.H.; Ip, M.; Sung, J.J.Y.; Wong, R.M.Y. Understanding the gut microbiota and sarcopenia: A systematic review. J. Cachexia Sarcopenia Muscle 2021, 12, 1393–1407. [Google Scholar] [CrossRef]
- Sakuma, K.; Hamada, K.; Yamaguchi, A.; Aoi, W. Current nutritional and pharmacological approaches for attenuating sarcopenia. Cells 2023, 12, 2422. [Google Scholar] [CrossRef]
- Huang, L.-T.; Wang, J.-H. The therapeutic intervention of sex steroid hormones for sarcopenia. Front. Med. 2021, 8, 739251. [Google Scholar] [CrossRef]
- Nielsen, B.R.; Andersen, H.E.; Hovind, P.; Jørgensen, N.R.; Schwarz, P.; Kristensen, S.H.; Suetta, C. Sarcopenia and self-reported markers of physical frailty in patients with osteoporosis. Arch. Osteoporos. 2024, 19, 77. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Barbalho, S.M.; Marquess, A.R.; Grecco, A.I.d.S.; Goulart, R.d.A.; Tofano, R.J.; Bishayee, A. Pomegranate (Punica granatum L.) and metabolic syndrome risk factors and outcomes: A systematic review of clinical studies. Nutrients 2022, 14, 1665. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.; Park, S.-M.; Kim, N.S.; Lee, H. Ginsenoside Rc, an Active Component of Panax ginseng, Alleviates Oxidative Stress-Induced Muscle Atrophy via Improvement of Mitochondrial Biogenesis. Antioxidants 2023, 12, 1576. [Google Scholar] [CrossRef]
- Rondanelli, M.; Miccono, A.; Peroni, G.; Guerriero, F.; Morazzoni, P.; Riva, A.; Guido, D.; Perna, S. A systematic review on the effects of botanicals on skeletal muscle health in order to prevent sarcopenia. Evid.-Based Complement. Altern. Med. 2016, 2016, 5970367. [Google Scholar] [CrossRef]
- Oliynyk, S.; Oh, S. Actoprotective effect of ginseng: Improving mental and physical performance. J. Ginseng Res. 2013, 37, 144. [Google Scholar] [CrossRef] [PubMed]
- Lopresti, A.L.; Smith, S.J. Ashwagandha (Withania somnifera) for the treatment and enhancement of mental and physical conditions: A systematic review of human trials. J. Herb. Med. 2021, 28, 100434. [Google Scholar] [CrossRef]
- Laurindo, L.F.; de Carvalho, G.M.; de Oliveira Zanuso, B.; Figueira, M.E.; Direito, R.; de Alvares Goulart, R.; Buglio, D.S.; Barbalho, S.M. Curcumin-based nanomedicines in the treatment of inflammatory and immunomodulated diseases: An evidence-based comprehensive review. Pharmaceutics 2023, 15, 229. [Google Scholar] [CrossRef] [PubMed]
- Silva, I.F.d.; Bragante, W.R.; Junior, R.C.M.; Laurindo, L.F.; Guiguer, E.L.; Araújo, A.C.; Fiorini, A.M.; Nicolau, C.C.; Oshiiwa, M.; Lima, E.P.d. Effects of Smallanthus sonchifolius Flour on Metabolic Parameters: A Systematic Review. Pharmaceuticals 2024, 17, 658. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Rodrigues, V.D.; Minniti, G.; de Carvalho, A.C.A.; Zutin, T.L.M.; DeLiberto, L.K.; Bishayee, A.; Barbalho, S.M. Pomegranate (Punica granatum L.) phytochemicals target the components of metabolic syndrome. J. Nutr. Biochem. 2024, 131, 109670. [Google Scholar] [CrossRef]
- German, I.J.S.; Pomini, K.T.; Andreo, J.C.; Shindo, J.V.T.C.; Castro, M.V.M.d.; Detregiachi, C.R.P.; Araújo, A.C.; Guiguer, E.L.; Fornari Laurindo, L.; Bueno, P.C.d.S. New Trends to Treat Muscular Atrophy: A Systematic Review of Epicatechin. Nutrients 2024, 16, 326. [Google Scholar] [CrossRef]
- Zhang, W.; Xiao, D.; Mao, Q.; Xia, H. Role of neuroinflammation in neurodegeneration development. Signal Transduct. Target. Ther. 2023, 8, 267. [Google Scholar] [CrossRef]
- Ciurea, A.V.; Mohan, A.G.; Covache-Busuioc, R.-A.; Costin, H.-P.; Glavan, L.-A.; Corlatescu, A.-D.; Saceleanu, V.M. Unraveling molecular and genetic insights into neurodegenerative diseases: Advances in understanding Alzheimer’s, Parkinson’s, and Huntington’s diseases and amyotrophic lateral sclerosis. Int. J. Mol. Sci. 2023, 24, 10809. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Tuka, B.; Vécsei, L. Navigating the Neurobiology of Migraine: From Pathways to Potential Therapies. Cells 2024, 13, 1098. [Google Scholar] [CrossRef]
- Pluvinage, J.V.; Wyss-Coray, T. Systemic factors as mediators of brain homeostasis, ageing and neurodegeneration. Nat. Rev. Neurosci. 2020, 21, 93–102. [Google Scholar] [CrossRef]
- Sheikh, A.M.; Yano, S.; Tabassum, S.; Nagai, A. The Role of the Vascular System in Degenerative Diseases: Mechanisms and Implications. Int. J. Mol. Sci. 2024, 25, 2169. [Google Scholar] [CrossRef] [PubMed]
- Drakes, N.; Kondrikova, G.; Pytel, D.; Hamlett, E.D. Unveiling the Intricate Link Between Anaerobe Niche and Alzheimer Disease Pathogenesis. J. Infect. Dis. 2024, 230, S117–S127. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wang, L.; Cheng, W.; Lv, J.; Guan, X.; Guo, T.; Wu, J.; Zhang, W.; Gao, T.; Liu, X. Two distinct trajectories of clinical and neurodegeneration events in Parkinson’s disease. Park. Dis. 2023, 9, 111. [Google Scholar] [CrossRef] [PubMed]
- Bartl, M.; Dakna, M.; Schade, S.; Otte, B.; Wicke, T.; Lang, E.; Starke, M.; Ebentheuer, J.; Weber, S.; Toischer, K. Blood markers of inflammation, neurodegeneration, and cardiovascular risk in early Parkinson’s disease. Mov. Disord. 2023, 38, 68–81. [Google Scholar] [CrossRef]
- Nim, S.; O’Hara, D.M.; Corbi-Verge, C.; Perez-Riba, A.; Fujisawa, K.; Kapadia, M.; Chau, H.; Albanese, F.; Pawar, G.; De Snoo, M.L. Disrupting the α-synuclein-ESCRT interaction with a peptide inhibitor mitigates neurodegeneration in preclinical models of Parkinson’s disease. Nat. Commun. 2023, 14, 2150. [Google Scholar] [CrossRef]
- Gupta, D.; Kuruvilla, A. Vascular parkinsonism: What makes it different? Postgrad. Med. J. 2011, 87, 829–836. [Google Scholar] [CrossRef]
- Jacob, M.A.; Cai, M.; Bergkamp, M.; Darweesh, S.K.; Gelissen, L.M.; Marques, J.; Norris, D.G.; Duering, M.; Esselink, R.A.; Tuladhar, A.M. Cerebral small vessel disease progression increases risk of incident parkinsonism. Ann. Neurol. 2023, 93, 1130–1141. [Google Scholar] [CrossRef]
- Li, Y.; Zhang, C.; Xu, W.; Chen, J.; Tuo, J.; Wen, Y.; Huang, Z.; Zeng, R. Serum Sirtuin1 level decreases in Parkinson’s disease and vascular parkinsonism: A prospective observational study. Clin. Neurol. Neurosurg. 2023, 225, 107595. [Google Scholar] [CrossRef] [PubMed]
- Oveisgharan, S.; Yu, L.; Poole, V.N.; Evia, A.M.; Barnes, L.L.; Schneider, J.A.; Arfanakis, K.; Bennett, D.A.; Buchman, A.S. Association of white matter hyperintensities with pathology and progression of parkinsonism in aging. JAMA Neurol. 2021, 78, 1494–1502. [Google Scholar] [CrossRef]
- Visser, A.E.; de Vries, N.M.; Richard, E.; Bloem, B.R. Tackling vascular risk factors as a possible disease modifying intervention in Parkinson’s disease. npj Park. Dis. 2024, 10, 50. [Google Scholar] [CrossRef]
- Camerino, I.; Ferreira, J.; Vonk, J.M.; Kessels, R.P.; de Leeuw, F.-E.; Roelofs, A.; Copland, D.; Piai, V. Systematic review and meta-analyses of word production abilities in dysfunction of the basal ganglia: Stroke, small vessel disease, Parkinson’s disease, and Huntington’s disease. Neuropsychol. Rev. 2024, 34, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Al-Bachari, S.; Naish, J.H.; Parker, G.J.; Emsley, H.C.; Parkes, L.M. Blood–brain barrier leakage is increased in Parkinson’s disease. Front. Physiol. 2020, 11, 593026. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, I.; Asanuma, M. Neuron-astrocyte interactions in Parkinson’s disease. Cells 2020, 9, 2623. [Google Scholar] [CrossRef]
- Paolini Paoletti, F.; Simoni, S.; Parnetti, L.; Gaetani, L. The contribution of small vessel disease to neurodegeneration: Focus on Alzheimer’s disease, Parkinson’s disease and multiple sclerosis. Int. J. Mol. Sci. 2021, 22, 4958. [Google Scholar] [CrossRef]
- Choi, H.L.; Ahn, J.H.; Chang, W.H.; Jung, W.; Kim, B.S.; Han, K.; Youn, J.; Shin, D.W. Risk of Parkinson disease in stroke patients: A nationwide cohort study in South Korea. Eur. J. Neurol. 2024, 31, e16194. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Jabir, M.S.; Al-Gareeb, A.I.; Albuhadily, A.K. New insight on the possible role of statins in Vascular Parkinsonism: A need for presumptive therapy. Ageing Res. Rev. 2024, 95, 102209. [Google Scholar] [CrossRef]
- Eisenmenger, L.B.; Peret, A.; Famakin, B.M.; Spahic, A.; Roberts, G.S.; Bockholt, J.H.; Johnson, K.M.; Paulsen, J.S. Vascular contributions to Alzheimer’s disease. Transl. Res. 2023, 254, 41–53. [Google Scholar] [CrossRef] [PubMed]
- Twait, E.L.; Gerritsen, L.; Moonen, J.E.; Verberk, I.M.; Teunissen, C.E.; Visser, P.J.; van der Flier, W.M.; Geerlings, M.I.; UCC SMART Study Group, the NCDC. Plasma Markers of Alzheimer’s Disease Pathology, Neuronal Injury, and Astrocytic Activation and MRI Load of Vascular Pathology and Neurodegeneration: The SMART-MR Study. J. Am. Heart Assoc. 2024, 13, e032134. [Google Scholar] [CrossRef]
- Lei, T.; Yang, Z.; Li, H.; Qin, M.; Gao, H. Interactions between nanoparticles and pathological changes of vascular in Alzheimer’s disease. Adv. Drug Deliv. Rev. 2024, 207, 115219. [Google Scholar] [CrossRef]
- Toribio-Fernandez, R.; Ceron, C.; Tristão-Pereira, C.; Fernandez-Nueda, I.; Perez-Castillo, A.; Fernandez-Ferro, J.; Moro, M.A.; Ibañez, B.; Fuster, V.; Cortes-Canteli, M. Oral anticoagulants: A plausible new treatment for Alzheimer’s disease? Br. J. Pharmacol. 2024, 181, 760–776. [Google Scholar] [CrossRef]
- Tu, M.-C.; Huang, S.-M.; Hsu, Y.-H.; Yang, J.-J.; Lin, C.-Y.; Kuo, L.-W. Joint diffusional kurtosis magnetic resonance imaging analysis of white matter and the thalamus to identify subcortical ischemic vascular disease. Sci. Rep. 2024, 14, 2570. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Xing, H.; Zhang, Z. Microvascular Perfusion Imaging in Alzheimer’s Disease. J. Integr. Neurosci. 2024, 23, 70. [Google Scholar] [CrossRef] [PubMed]
- Nazzi, C.; Avenanti, A.; Battaglia, S. The Involvement of Antioxidants in Cognitive Decline and Neurodegeneration: Mens Sana in Corpore Sano. Antioxidants 2024, 13, 701. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neural Correlates and Molecular Mechanisms of Memory and Learning. Int. J. Mol. Sci. 2024, 25, 2724. [Google Scholar] [CrossRef] [PubMed]
- Liloia, D.; Zamfira, D.A.; Tanaka, M.; Manuello, J.; Crocetta, A.; Keller, R.; Cozzolino, M.; Duca, S.; Cauda, F.; Costa, T. Disentangling the role of gray matter volume and concentration in autism spectrum disorder: A meta-analytic investigation of 25 years of voxel-based morphometry research. Neurosci. Biobehav. Rev. 2024, 164, 105791. [Google Scholar] [CrossRef]
- Martos, D.; Lőrinczi, B.; Szatmári, I.; Vécsei, L.; Tanaka, M. The Impact of C-3 Side Chain Modifications on Kynurenic Acid: A Behavioral Analysis of Its Analogs in the Motor Domain. Int. J. Mol. Sci. 2024, 25, 3394. [Google Scholar] [CrossRef]
- Tanaka, M.; Szabó, Á.; Körtési, T.; Szok, D.; Tajti, J.; Vécsei, L. From CGRP to PACAP, VIP, and beyond: Unraveling the next chapters in migraine treatment. Cells 2023, 12, 2649. [Google Scholar] [CrossRef]
- Tajti, J.; Szok, D.; Csáti, A.; Szabó, Á.; Tanaka, M.; Vécsei, L. Exploring Novel Therapeutic Targets in the Common Pathogenic Factors in Migraine and Neuropathic Pain. Int. J. Mol. Sci. 2023, 24, 4114. [Google Scholar] [CrossRef]
- Fornari Laurindo, L.; Aparecido Dias, J.; Cressoni Araujo, A.; Torres Pomini, K.; Machado Galhardi, C.; Rucco Penteado Detregiachi, C.; Santos de Argollo Haber, L.; Donizeti Roque, D.; Dib Bechara, M.; Vialogo Marques de Castro, M. Immunological dimensions of neuroinflammation and microglial activation: Exploring innovative immunomodulatory approaches to mitigate neuroinflammatory progression. Front. Immunol. 2024, 14, 1305933. [Google Scholar] [CrossRef]
- Valotto Neto, L.J.; Reverete de Araujo, M.; Moretti Junior, R.C.; Mendes Machado, N.; Joshi, R.K.; dos Santos Buglio, D.; Barbalho Lamas, C.; Direito, R.; Fornari Laurindo, L.; Tanaka, M. Investigating the Neuroprotective and Cognitive-Enhancing Effects of Bacopa monnieri: A Systematic Review Focused on Inflammation, Oxidative Stress, Mitochondrial Dysfunction, and Apoptosis. Antioxidants 2024, 13, 393. [Google Scholar] [CrossRef]
- Kalick, L.S.; Khan, H.A.; Maung, E.; Baez, Y.; Atkinson, A.N.; Wallace, C.E.; Day, F.; Delgadillo, B.E.; Mondal, A.; Watanapokasin, R.; et al. Mangosteen for malignancy prevention and intervention: Current evidence, molecular mechanisms, and future perspectives. Pharmacol. Res. 2023, 188, 106630. [Google Scholar] [CrossRef] [PubMed]
- Bosso, H.; Barbalho, S.M.; de Alvares Goulart, R.; Otoboni, A. Green coffee: Economic relevance and a systematic review of the effects on human health. Crit. Rev. Food Sci. Nutr. 2023, 63, 394–410. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Araújo, A.C.; Penteado Detregiachi, C.R.; Buchaim, D.V.; Guiguer, É.L. The Potential Role of Medicinal Plants in Bone Regeneration. Altern. Ther. Health Med. 2019, 25, 32–39. [Google Scholar] [PubMed]
- Barbalho, S.M.; Bosso, H.; Salzedas-Pescinini, L.M.; de Alvares Goulart, R. Green tea: A possibility in the therapeutic approach of inflammatory bowel diseases?: Green tea and inflammatory bowel diseases. Complement. Ther. Med. 2019, 43, 148–153. [Google Scholar] [CrossRef]
- Bássoli, R.; Audi, D.; Ramalho, B.; Audi, M.; Quesada, K.; Barbalho, S. The Effects of Curcumin on Neurodegenerative Diseases: A Systematic Review. J. Herb. Med. 2023, 42, 100771. [Google Scholar] [CrossRef]
- Marton, L.T.; Barbalho, S.M.; Sloan, K.P.; Sloan, L.A.; Goulart, R.d.A.; Araújo, A.C.; Bechara, M.D. Curcumin, autoimmune and inflammatory diseases: Going beyond conventional therapy–a systematic review. Crit. Rev. Food Sci. Nutr. 2022, 62, 2140–2157. [Google Scholar] [CrossRef]
- Nunes, Y.C.; Mendes, N.M.; Pereira de Lima, E.; Chehadi, A.C.; Lamas, C.B.; Haber, J.F.S.; dos Santos Bueno, M.; Araújo, A.C.; Catharin, V.C.S.; Detregiachi, C.R.P.; et al. Curcumin: A Golden Approach to Healthy Aging: A Systematic Review of the Evidence. Nutrients 2024, 16, 2721. [Google Scholar] [CrossRef] [PubMed]
- Buglio, D.S.; Marton, L.T.; Laurindo, L.F.; Guiguer, E.L.; Araújo, A.C.; Buchaim, R.L.; Goulart, R.d.A.; Rubira, C.J.; Barbalho, S.M. The role of resveratrol in mild cognitive impairment and Alzheimer’s disease: A systematic review. J. Med. Food 2022, 25, 797–806. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Direito, R.; Bueno Otoboni, A.M.; Goulart, R.A.; Quesada, K.; Barbalho, S.M. Grape processing waste: Effects on inflammatory bowel disease and colorectal cancer. Food Rev. Int. 2024, 40, 336–369. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Bueno Ottoboni, A.M.M.; Fiorini, A.M.R.; Guiguer, E.L.; Nicolau, C.C.T.; Goulart, R.d.A.; Flato, U.A.P. Grape juice or wine: Which is the best option? Crit. Rev. Food Sci. Nutr. 2020, 60, 3876–3889. [Google Scholar] [CrossRef]
- Barbalho, S.; Direito, R.; Laurindo, L.; Marton, L.; Guiguer, E.; Goulart, R.d.A.; Tofano, R.J.; Carvalho, A.; Flato, U.; Capelluppi Tofano, V. Ginkgo biloba in the aging process: A narrative review. Antioxidants 2022, 11, 525. [Google Scholar] [CrossRef] [PubMed]
- Jászberényi, M.; Thurzó, B.; Bagosi, Z.; Vécsei, L.; Tanaka, M. The Orexin/Hypocretin System, the Peptidergic Regulator of Vigilance, Orchestrates Adaptation to Stress. Biomedicines 2024, 12, 448. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. A Decade of Dedication: Pioneering Perspectives on Neurological Diseases and Mental Illnesses. Biomedicines 2024, 12, 1083. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Battaglia, S.; Giménez-Llort, L.; Chen, C.; Hepsomali, P.; Avenanti, A.; Vécsei, L. Innovation at the Intersection: Emerging Translational Research in Neurology and Psychiatry. Cells 2024, 13, 790. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. From Lab to Life: Exploring Cutting-Edge Models for Neurological and Psychiatric Disorders. Biomedicines 2024, 12, 613. [Google Scholar] [CrossRef]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neurodegeneration in Cognitive Impairment and Mood Disorders for Experimental, Clinical and Translational Neuropsychiatry. Biomedicines 2024, 12, 574. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Schmidt, A.; Hassel, S.; Tanaka, M. Case reports in neuroimaging and stimulation. Front. Media SA 2023, 14, 1264669. [Google Scholar]
- Tanaka, M.; Diano, M.; Battaglia, S. Editorial: Insights into structural and functional organization of the brain: Evidence from neuroimaging and non-invasive brain stimulation techniques. Front. Psychiatry 2023, 14, 1225755. [Google Scholar] [CrossRef]
- Tanaka, M.; Szabó, Á.; Vécsei, L. Preclinical modeling in depression and anxiety: Current challenges and future research directions. Adv. Clin. Exp. Med. 2023, 32, 505–509. [Google Scholar] [CrossRef]
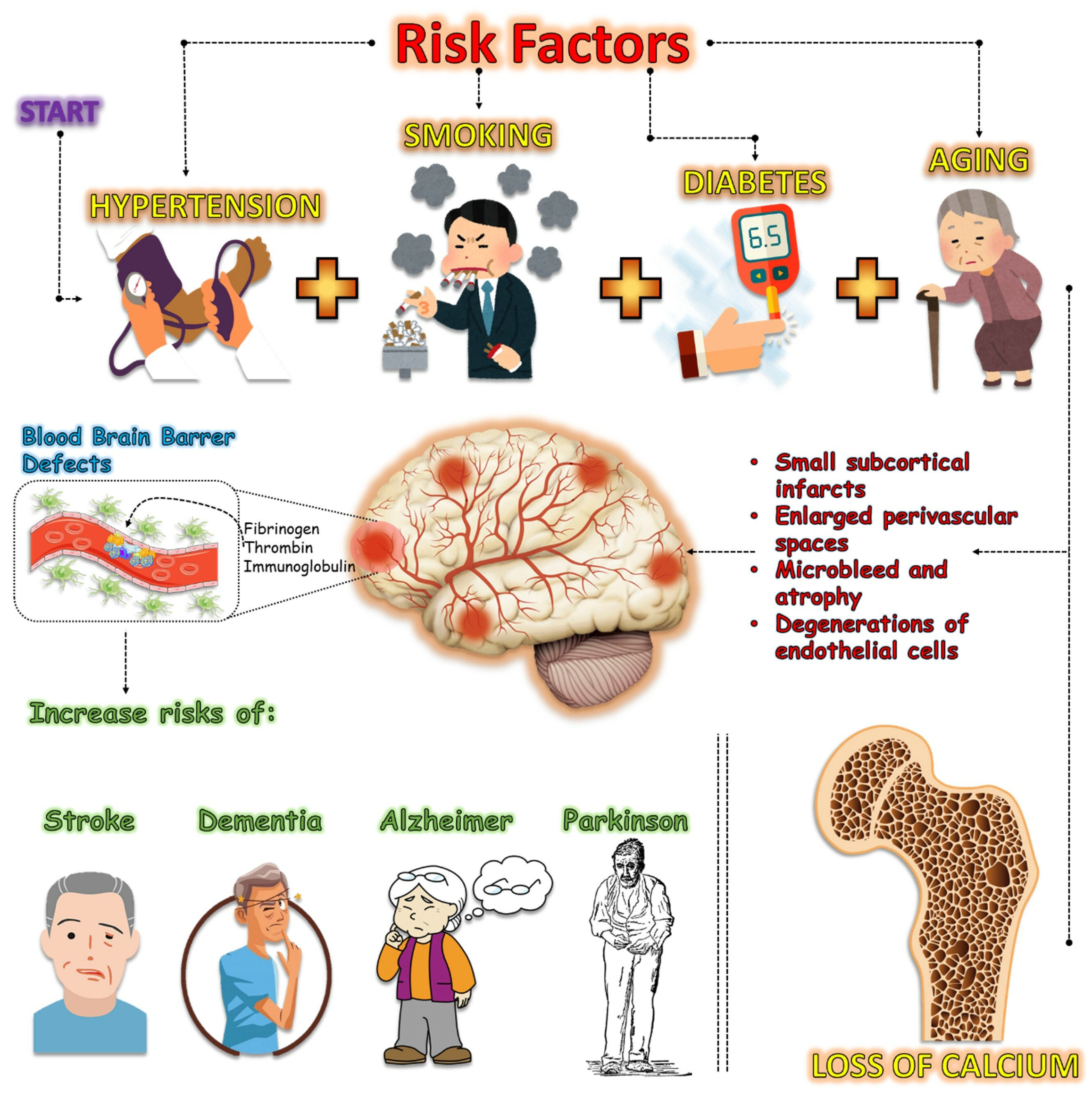

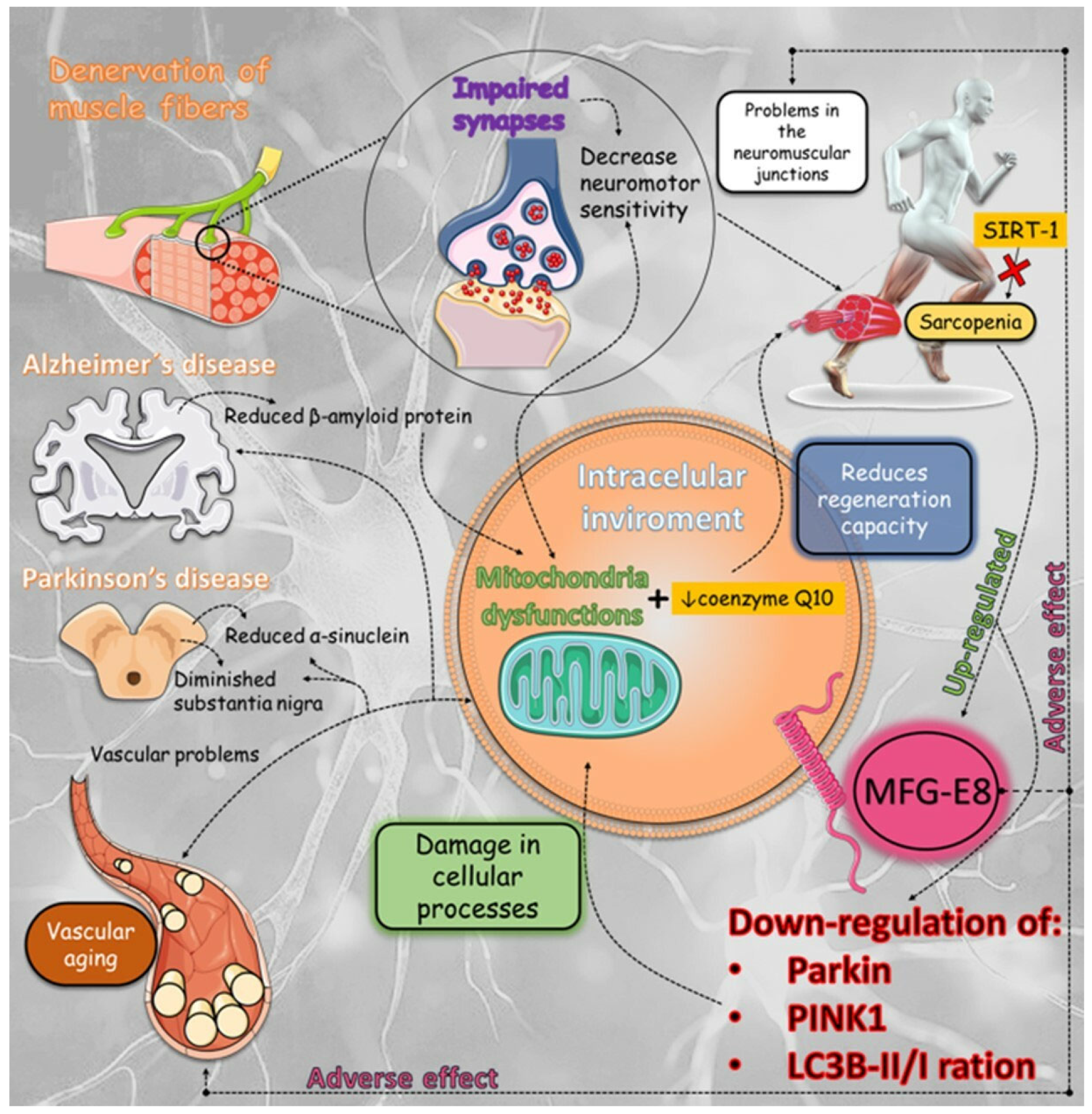

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Lima, E.P.; Tanaka, M.; Lamas, C.B.; Quesada, K.; Detregiachi, C.R.P.; Araújo, A.C.; Guiguer, E.L.; Catharin, V.M.C.S.; de Castro, M.V.M.; Junior, E.B.; et al. Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions. Biomedicines 2024, 12, 2096. https://doi.org/10.3390/biomedicines12092096
de Lima EP, Tanaka M, Lamas CB, Quesada K, Detregiachi CRP, Araújo AC, Guiguer EL, Catharin VMCS, de Castro MVM, Junior EB, et al. Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions. Biomedicines. 2024; 12(9):2096. https://doi.org/10.3390/biomedicines12092096
Chicago/Turabian Stylede Lima, Enzo Pereira, Masaru Tanaka, Caroline Barbalho Lamas, Karina Quesada, Claudia Rucco P. Detregiachi, Adriano Cressoni Araújo, Elen Landgraf Guiguer, Virgínia Maria Cavallari Strozze Catharin, Marcela Vialogo Marques de Castro, Edgar Baldi Junior, and et al. 2024. "Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions" Biomedicines 12, no. 9: 2096. https://doi.org/10.3390/biomedicines12092096
APA Stylede Lima, E. P., Tanaka, M., Lamas, C. B., Quesada, K., Detregiachi, C. R. P., Araújo, A. C., Guiguer, E. L., Catharin, V. M. C. S., de Castro, M. V. M., Junior, E. B., Bechara, M. D., Ferraz, B. F. R., Catharin, V. C. S., Laurindo, L. F., & Barbalho, S. M. (2024). Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions. Biomedicines, 12(9), 2096. https://doi.org/10.3390/biomedicines12092096