
A Novel Diagnostic and Treatment Approach to an Unusual Case of Dens Invaginatus in a Mandibular Lateral Incisor Using CBCT and 3D Printing Technology


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Pretreatment Planning
2.2. Nonsurgical Treatment
2.3. Surgical Treatment
3. Results
4. Discussion
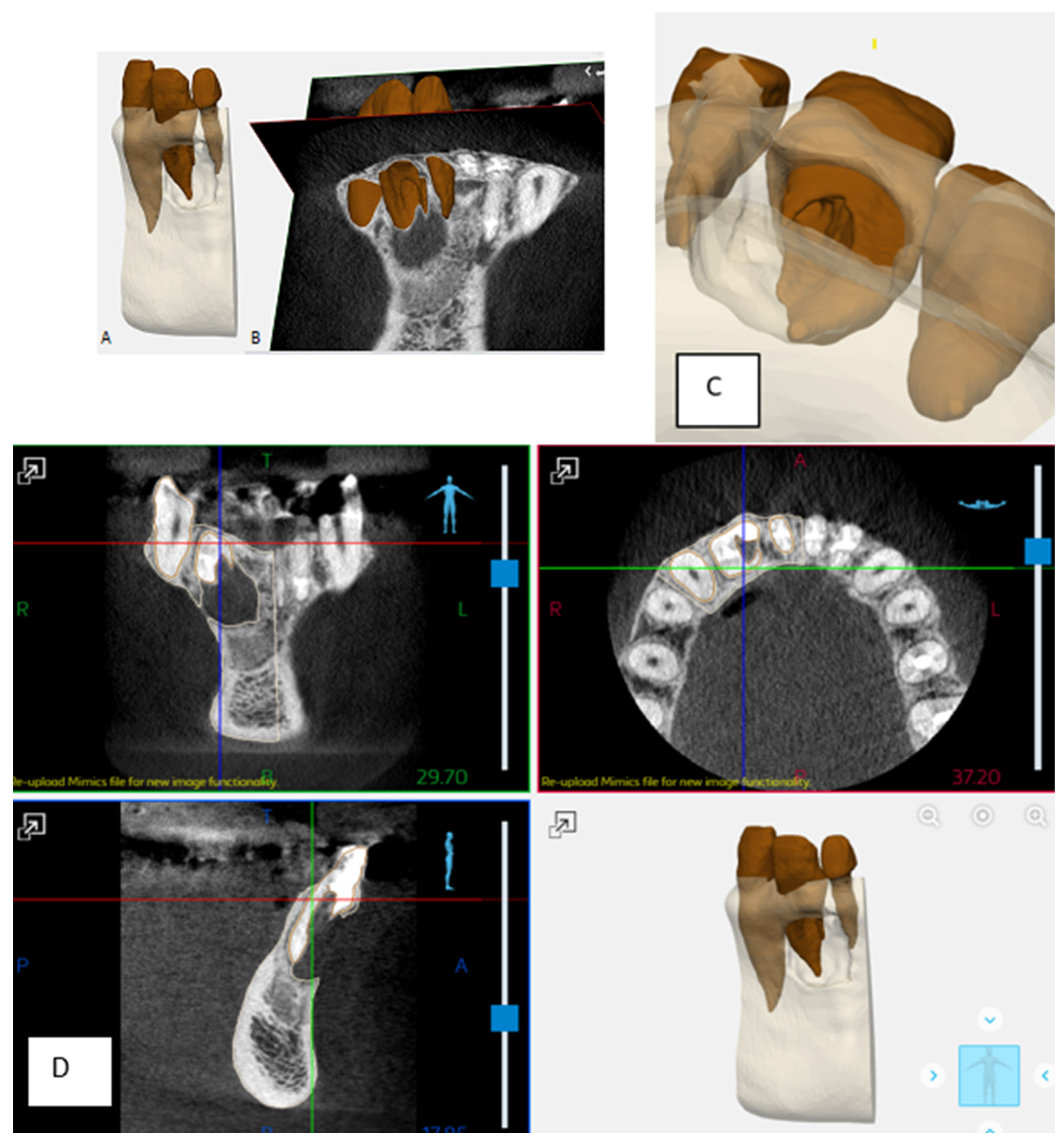
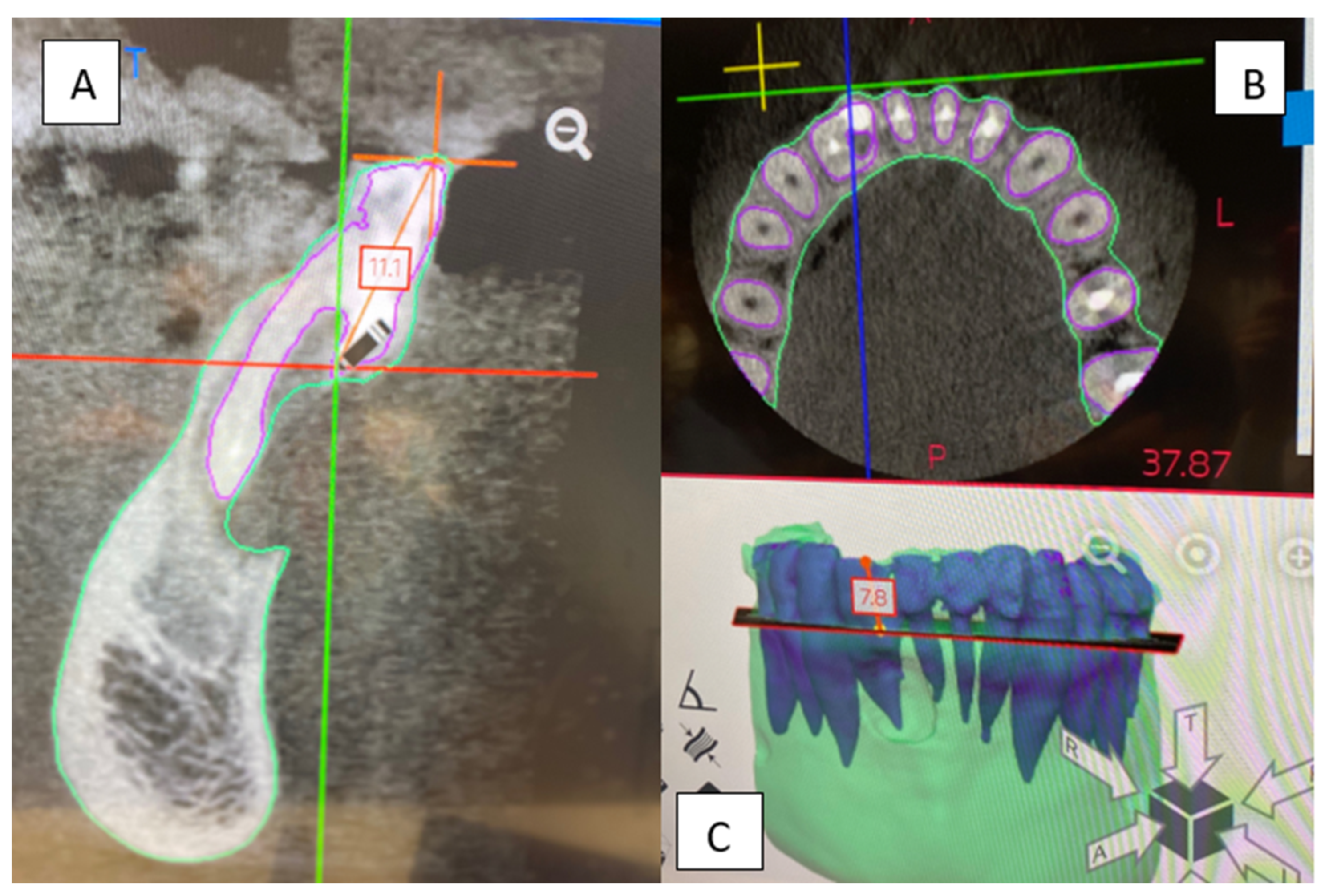
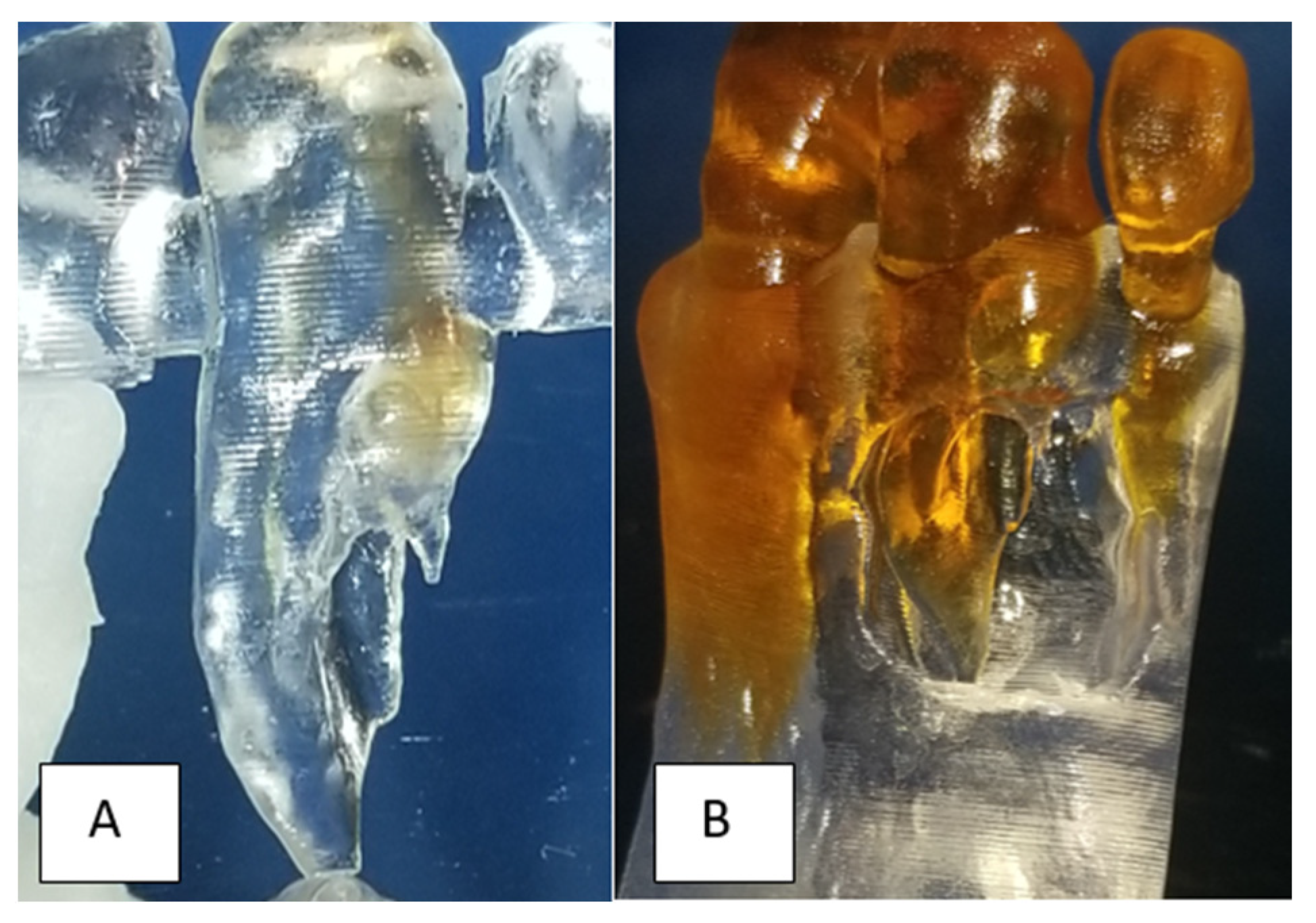
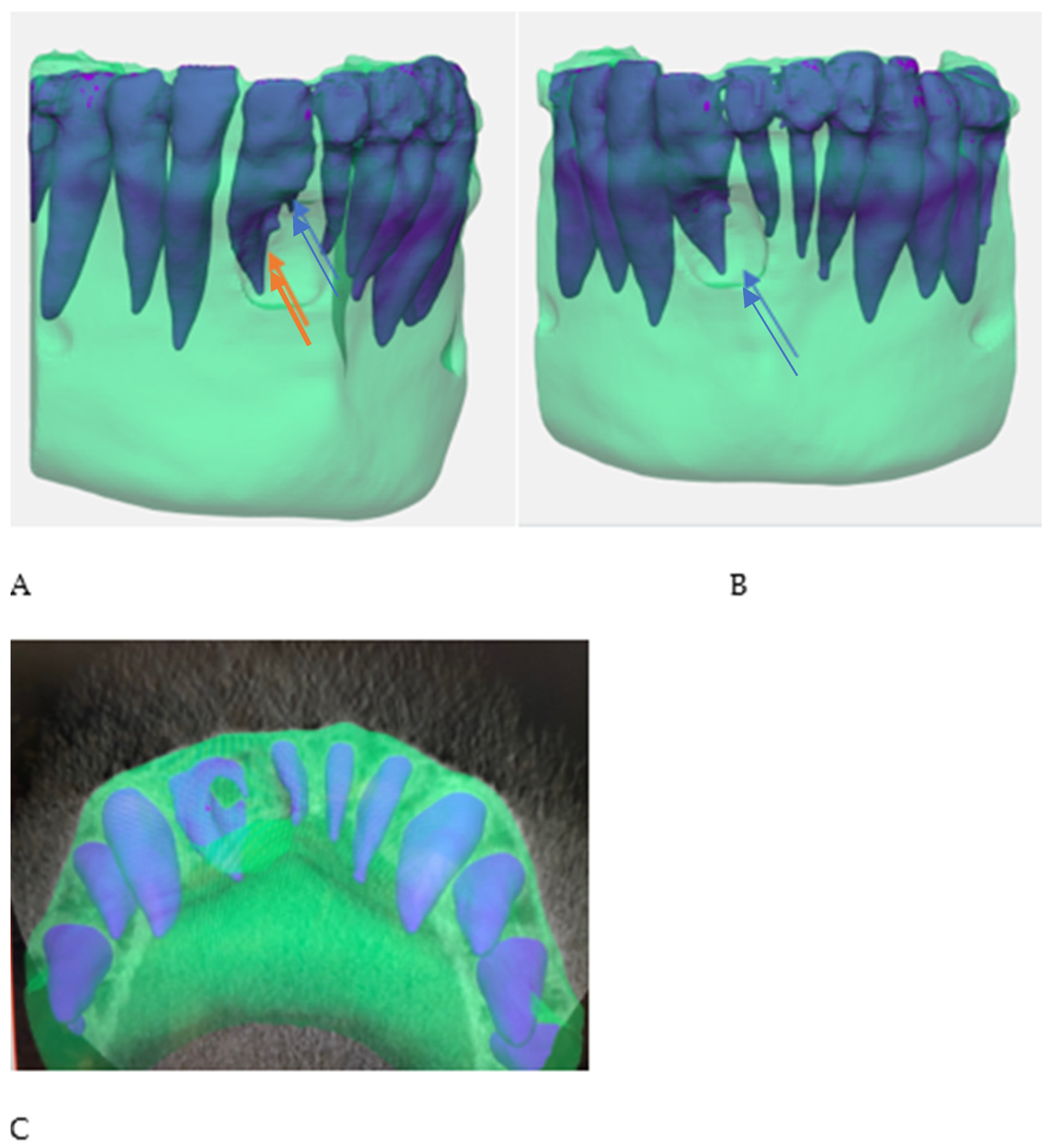
- The comparison between the use of 3D printing and milling with the use of Materialise software, as used in the current study, was profiled in a study by Kachhara et al. They concluded that an exact tooth replica can be created to assist in treatment planning [26]. The ability of the clinician to view a 3D model versus manipulating a CBCT image in the axial, sagittal, and coronal views, is beneficial to appreciating the fine detail of the unique root anatomy. The exact replica is produced to a high level of detail that can be directly viewed. Being able to handle the physical model provides an opportunity to manipulate and observe the model and appreciate the unique characteristics of the tooth and root anatomy when conceptualizing the proposed nonsurgical and surgical endodontic treatment.
- Potential challenges to using 3D printing technology for treatment planning include access to technology, knowledge of appropriate software, cost, and patient acceptance of complex treatment plans. When using advanced technologies, patients should be informed of potential complications. When considering the use of advanced technology, the benefit to the patient should be of primary concern. Materials used in this case have been extensively researched, such as MTA and advanced platelet rich fibrin (A-PRF). The unique aspect of this case is the use of combined therapies with advanced 3D printing technology to ensure a more predictable, inclusive treatment. Longer term follow-up, as seen in this case, is encouraged to continue to evaluate the successful outcome of treatment in rare, unusual cases.
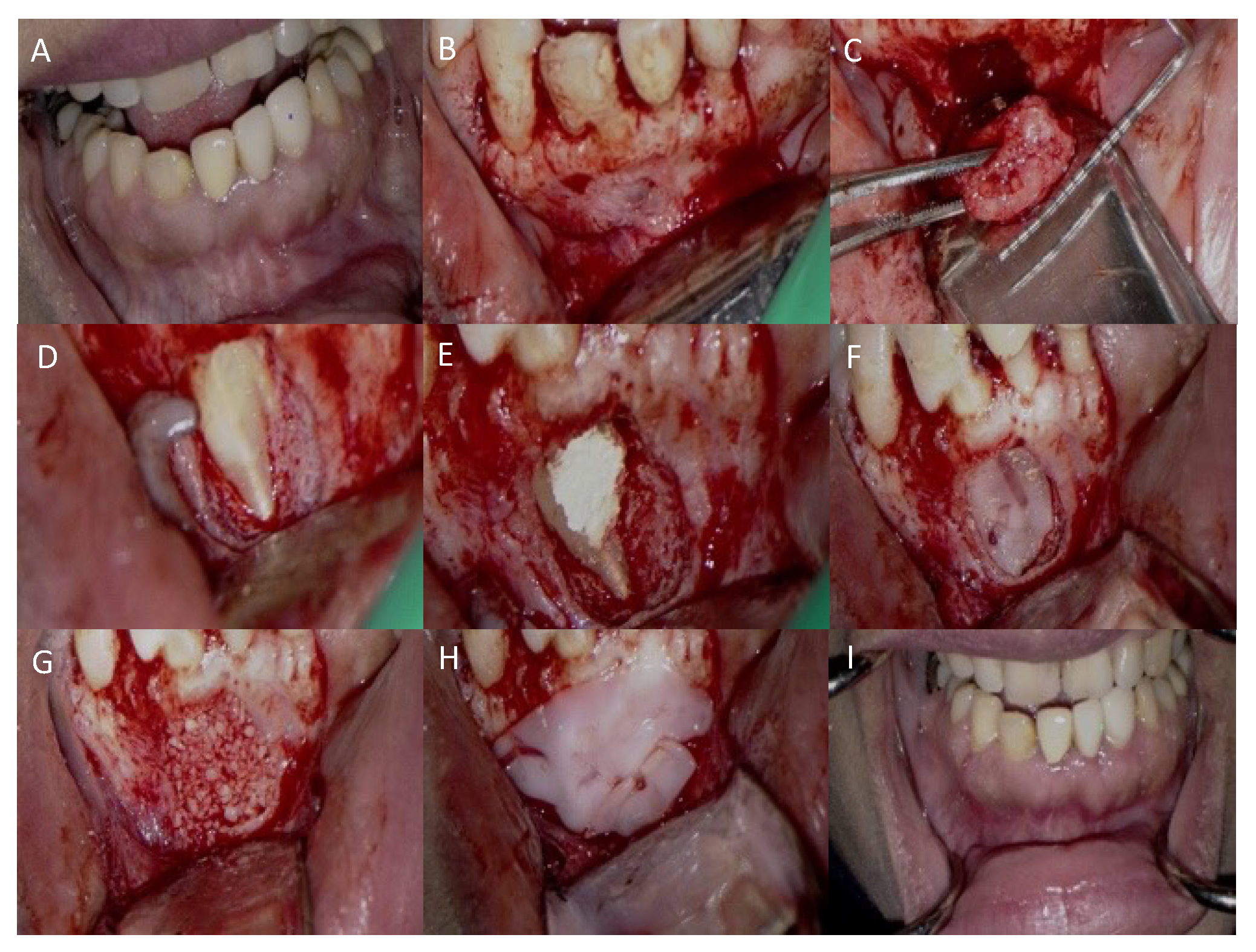
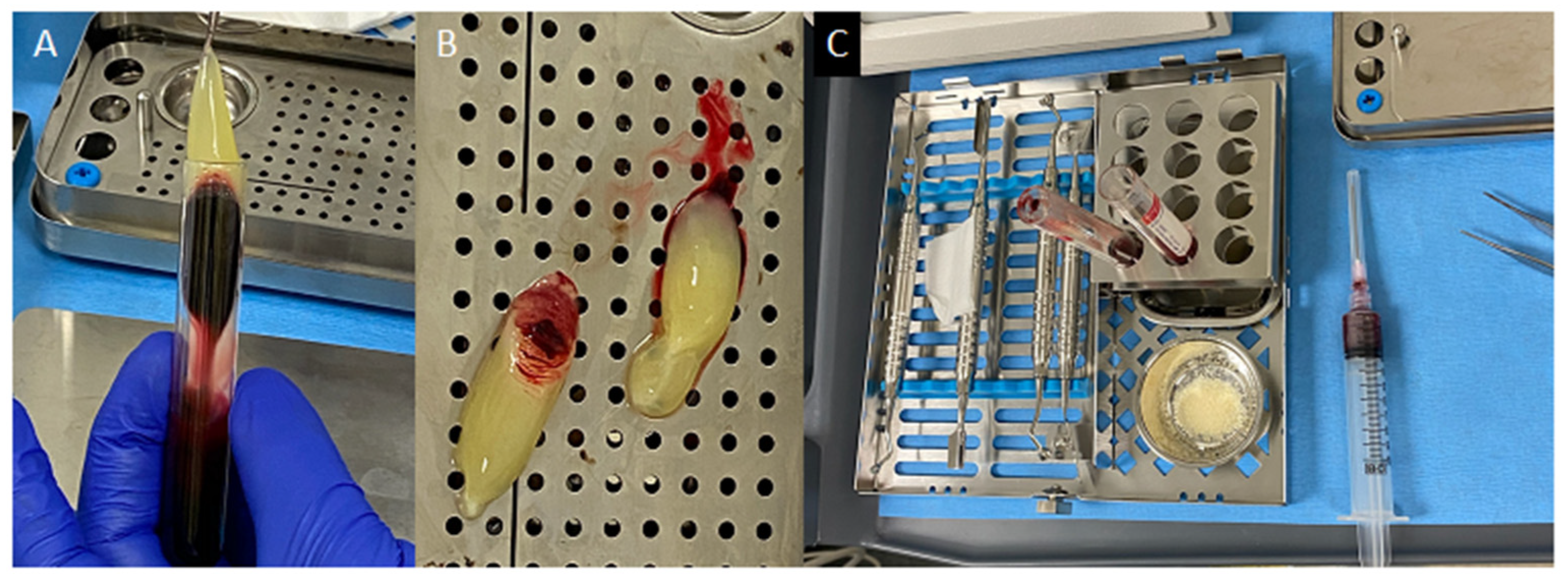
- The use of two PRF membranes made several significant contributions to treatment execution. The soft, flexible nature of PRF is ideal for layering over MTA without adversely affecting the surface texture. The first membrane delicately smoothed and contained the material within the confines of the DI during the setting period. The second PRF membrane was used to protect the entire defect and to retain the grafting particulate and maintain its osteoconductive properties, enabling the ingrowth of vascular and cellular connective tissues. The PRF in grafting gives the advantage of using the patient’s blood products to maximize available growth factors and to dramatically improve the speed of osseous healing [8,27,28]. For DIs with a wide, oblique foramen, PRF is critical to retaining and protecting the MTA filling while providing the above-mentioned healing benefits. The present case report demonstrated that using 3D models led to improved pretreatment planning and provided a more accurate protocol for the surgical intervention.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Oehlers, F. Dens invaginatus (dilated composite odontome): I. Variations of the invagination process and associated anterior crown forms. Oral Surg. Oral Med. Oral Pathol. 1957, 10, 1204–1218. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Wang, X.; Fang, Y.; Von den Hoff, J.W.; Meng, L. An update on the diagnosis and treatment of dens invaginatus. Aust. Dent. J. 2017, 62, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Gallacher, A.; Ali, R.; Bhakta, S. Dens invaginatus: Diagnosis and management strategies. Br. Dent. J. 2016, 221, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Alani, A.; Bishop, K. Dens Invaginatus: Part 1: Classification, prevalence and aetiology. Int. Endod. J. 2008, 41, 1123–1136. [Google Scholar] [CrossRef]
- Nallapati, S. Clinical Management of a Maxillary Lateral Incisor with Vital Pulp and Type 3 Dens Invaginatus: A Case Report. J. Endod. 2004, 30, 726–731. [Google Scholar] [CrossRef]
- Pitt-Ford, H.E. Peri-radicular inflammation related to Dens invaginatus treated without damaging the dental pulp: A case report. Int. J. Paediatr. Dent. 1998, 8, 283±286. [Google Scholar] [CrossRef]
- Chaniotis, A.; Tzanetakis, G.; Kontakiotis, E.; Tosios, K.I. Combined Endodontic and Surgical Management of a Mandibular Lateral Incisor with a Rare Type of Dens Invaginatus. J. Endod. 2008, 34, 1255–1260. [Google Scholar] [CrossRef]
- Agrawal, P.; Wankhade, J.; Warhadpande, M. A Rare Case of Type III Dens Invaginatus in a Mandibular Second Premolar and Its Nonsurgical Endodontic Management by Using Cone-beam Computed Tomography: A Case Report. J. Endod. 2016, 42, 669–672. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Saraf, P.; Patil, J. Endodontic management of type IIIB dens invaginatus: An unusual case report. Saudi Endo. J. 2018, 8, 144–148. [Google Scholar] [CrossRef]
- Goel, S.; Nawal, R.; Talwar, S. Management of Dent Invaginatus Type II Associated with Immature Apex and Large Periradicular Lesion Using Platelet-rich Fibrin and Biodentine. J. Endod. 2017, 43, 1750–1755. [Google Scholar] [CrossRef]
- Mohan, A.; Krishnan, U.; Akber, M.; Nair, M.G.; Balan, A. Successful management of a case of true radicular dens invaginatus using platelet-rich fibrin and guided tissue regeneration. Aust. Endod. J. 2020, 46, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Zoya, A.; Ali, S.; Alam, S.; Tewari, R.K.; Mishra, S.K.; Kumar, A.; Andrabi, S.M.U.N. Double Dens Invaginatus with Multiple Canals in a Maxillary Central Incisor: Retreatment and Managing Complications. J. Endod. 2015, 41, 1927–1932. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.; Wei, X. Combined Therapy for a Rare Case of Type III Dens Invaginatus in a Mandibular Central Incisor with a Periapical Lesion: A Case Report. J. Endod. 2017, 43, 1378–1382. [Google Scholar] [CrossRef] [PubMed]
- Silberman, A.; Cohenca, N.; Simon, J. Anatomical redesign for the treatment of dens invaginatus type III with open apexes: A literature review and case presentation. J. Am. Dent. Assoc. 2006, 137, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Kfir, A.; Telishevsky-Strauss, Y.; Leitner, A.; Metzger, Z. The diagnosis and conservative treatment of a complex type 3 dens invaginatus using cone beam computed tomography (CBCT) and 3D plastic models. Int. Endod. J. 2013, 46, 275–288. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Hwang, J.; Kim, H. Treatment of peri-invagination lesion and vitality preservation in an immature type III dens invaginatus: A case report. BMC Oral Health 2020, 20, 29. [Google Scholar] [CrossRef] [PubMed]
- Ricucci, D.; Milovidova, I.; Siquiera, J. Unusual location of dens invaginatus causing a difficult-to-diagnose pulpal involvement. J. Endod. 2020, 46, 1522–1529. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.; Brito-Junior, M.; de Souza, F.; Von Zastrow, E.; da Cunha, C.O.; Silveira, F.F.; Nunes, E.; César, C.A.S.; Glória, J.C.R.; Soares, J.A. Management of Cyst-like Periapical Lesion by Orthograde Decompression and Long-term Calcium Hydroxide/Chlorhexidine Intracanal Dressing: A Case Series. J. Endod. 2016, 42, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Mohammadi, Z.; Dummer, P. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int. Endod. J. 2011, 44, 697–730. [Google Scholar] [CrossRef]
- Best, S.; Ammons, C.; Karunanayake, G.; Saemundsson, S.R.; Tawil, P.Z. Outcome Assessment of Teeth with Necrotic Pulps and Apical Periodontitis Treated with Long-term Calcium Hydroxide. J. Endod. 2021, 47, 11–18. [Google Scholar] [CrossRef]
- Ng, Y.-L.; Mann, V.; Rahbaran, S.; Lewsey, J.; Gulabivala, K. Outcome of primary root canal treatment: Systematic review of the literature—Part 2. Influence of clinical factors. Int. Endod. J. 2008, 41, 6–31. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Giménez, M.; Sánchez-Torres, A.; Gay-Escoda, C. Prognostic factors on periapical surgery: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2015, 20, e715–e722. [Google Scholar] [CrossRef] [PubMed]
- Reis, T.; Barbosa, C.; Franco, M.; Baptista, C.; Alves, N.; Castelo-Baz, P.; Martin-Cruces, J.; Martin-Biedma, B. 3D-Printed Teeth in Endodontics: Why, How, Problems and Future-A Narrative Review. Int. J. Environ. Res. Public. Health 2022, 19, 7966. [Google Scholar] [CrossRef] [PubMed]
- Byun, C.; Kim, C.; Cho, S.; Baek, S.H.; Kim, G.; Kim, S.G.; Kim, S.Y. Endodontic Treatment of an Anomalous Anterior Tooth with the Aid of a 3-dimensional Printed Physical Tooth Model. J. Endod. 2015, 41, 961–965. [Google Scholar] [CrossRef] [PubMed]
- Jha, S.; Balachandran, R.; Sharma, S.; Kumar, V.; Chawla, A.; Logani, A. A Novel Approach to Repositioning and Stabilization of a Luxated Tooth with Displacement Using a 3D Printed Guide. J. Endod. 2022, 48, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Kachhara, S.; Nallaswamy, D.; Ganapathy, D.; Ariga, P. Comparison of the CBCT, CT, 3D Printing, and CAD-CAM Milling Options for the Most Accurate Root Form Duplication Required for the Root Analogue Implant (RAI) Protocol. J. Indian Acad. Oral Med. Radiol. 2021, 33, 141–145. [Google Scholar] [CrossRef]
- Kobayashi, E.; Fluckiger, L.; Fujioka-Kobayashi, M.; Sawada, K.; Sculean, A.; Schaller, B.; Miron, R.J. Comparative release of growth factors from PRP, PRF, and advanced-PRF. Clin. Oral Investig. 2016, 20, 2353–2360. [Google Scholar] [CrossRef]
- Dohan, D.; Choukroun, J.; Diss, A.; Dohan, S.L.; Dohan, A.J.; Mouhyi, J.; Gogly, B. Platelet-rich fibrin (PRF): A second-generation platelet concentrate. Part III: Leucocyte activation: A new feature for platelet concentrates? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2006, 101, e51–e55. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
LaLonde, L.; Askar, M.; Paurazas, S. A Novel Diagnostic and Treatment Approach to an Unusual Case of Dens Invaginatus in a Mandibular Lateral Incisor Using CBCT and 3D Printing Technology. Dent. J. 2024, 12, 107. https://doi.org/10.3390/dj12040107
LaLonde L, Askar M, Paurazas S. A Novel Diagnostic and Treatment Approach to an Unusual Case of Dens Invaginatus in a Mandibular Lateral Incisor Using CBCT and 3D Printing Technology. Dentistry Journal. 2024; 12(4):107. https://doi.org/10.3390/dj12040107
Chicago/Turabian StyleLaLonde, Lindsey, Mazin Askar, and Susan Paurazas. 2024. "A Novel Diagnostic and Treatment Approach to an Unusual Case of Dens Invaginatus in a Mandibular Lateral Incisor Using CBCT and 3D Printing Technology" Dentistry Journal 12, no. 4: 107. https://doi.org/10.3390/dj12040107
APA StyleLaLonde, L., Askar, M., & Paurazas, S. (2024). A Novel Diagnostic and Treatment Approach to an Unusual Case of Dens Invaginatus in a Mandibular Lateral Incisor Using CBCT and 3D Printing Technology. Dentistry Journal, 12(4), 107. https://doi.org/10.3390/dj12040107