
The Impact of Vitamin Deficiencies on Oral Manifestations in Children

 ,
, 
Abstract
1. Introduction
Purpose of the Study
2. Materials and Methods
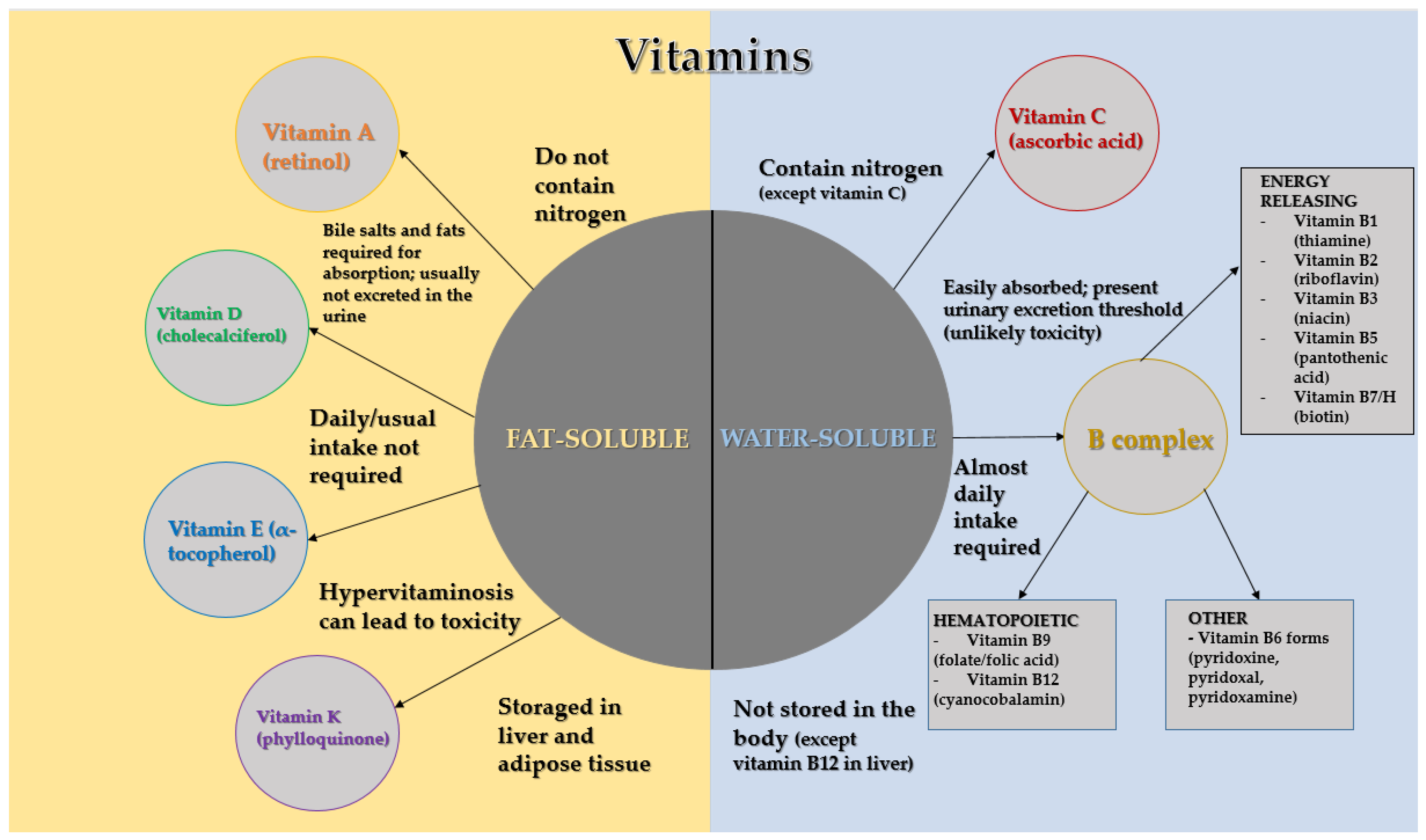
3. Fat-Soluble Vitamins
3.1. Vitamin A
Oral Manifestations of Vitamin A Deficiency
3.2. Vitamin D
Oral Manifestations of Vitamin D Deficiency
3.3. Vitamin E
Oral Manifestations of Vitamin E Deficiency
3.4. Vitamin K
Oral Manifestations of Vitamin K Deficiency
4. Water-Soluble Vitamins
4.1. B-Complex Vitamins
Oral Manifestations of B-Complex Vitamin Deficiency
4.2. Vitamin C
Oral Manifestations of Vitamin C Deficiency
5. The Importance of Recognizing Vitamin Deficiencies in the Oral Cavity
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hugar, S.M.; Dhariwal, N.S.; Majeed, A.; Badakar, C.; Gokhale, N.; Mistry, L. Assessment of Vitamin B12 and Its Correlation with Dental Caries and Gingival Diseases in 10- to 14-year-old Children: A Cross-sectional Study. Int. J. Clin. Pediatr. Dent. 2017, 10, 142–146. [Google Scholar]
- Mataix, J. Nutrición para Educadores, 2nd ed.; Diez de Santos: Madrid, Spain, 2013; pp. 117–126. [Google Scholar]
- O’Brien, S.K.; Malacova, E.; Sherriff, J.L.; Black, L.J. The Prevalence and Predictors of Dietary Supplement Use in the Australian Population. Nutrients 2017, 9, E1154. [Google Scholar] [CrossRef] [PubMed]
- Youness, R.A.; Dawoud, A.; ElTahtawy, O.; Farag, M.A. Fat-soluble Vitamins: Updated Review of Their Role and Orchestration in Human Nutrition Throughout Life Cycle with Sex Differences. Nutr. Metab. 2022, 19, 60. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.L. Fat-Soluble Vitamins. Nurs. Clin. N. Am. 2021, 56, 33–45. [Google Scholar] [CrossRef]
- Rodwell, V.W.; Bender, D.A.; Botham, K.M.; Kennelly, P.J.; Weil, A.P. Harper’s Illustrated Biochemistry, 31st ed.; Mc Graw Hill: New Delhi, India, 2018; pp. 535–549. [Google Scholar]
- Said, H.M.; Nexo, E. Gastrointestinal Handling of Water-Soluble Vitamins. Compr. Physiol. 2018, 8, 1291–1311. [Google Scholar]
- Madhusudhan, K.S.; Pallavi, M.R. Malnutrition-a Risk for Oral Health. Int. J. Sci. Res. 2019, 8, 74–77. [Google Scholar]
- Shaik, P.S.; Pachava, S. The Role of Vitamins and Trace Elements on Oral Health: A Systematic Review. Int. J. Med. Rev. 2017, 4, 22–31. [Google Scholar] [CrossRef]
- Tolkachjov, S.N.; Bruce, A.J. Oral Manifestations of Nutritional Disorders. Clin. Dermatol. 2017, 35, 441–452. [Google Scholar] [CrossRef]
- Radochová, V.; Slezák, R.; Radocha, J. Oral Manifestations of Nutritional Deficiencies: Single Centre Analysis. Acta Medica (Hradec Kral.) 2020, 63, 95–100. [Google Scholar] [CrossRef]
- Croatian Pediatric Society. Available online: https://pedijatrija.hlz.hr/ (accessed on 1 February 2024).
- World Health Organization. Available online: https://www.who.int/health-topics/nutrition (accessed on 23 March 2024).
- Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/nutrition/micronutrient-malnutrition/index.html (accessed on 23 March 2024).
- Mardešić, D.; Barić, I. Pedijatrija, 8th ed.; Školska knjiga: Zagreb, Croatia, 2013; pp. 83–93. [Google Scholar]
- Office of Dietary Supplements—National Institutes of Health. Available online: https://ods.od.nih.gov/factsheets/list-VitaminsMinerals/ (accessed on 1 February 2024).
- Reddy, P.; Jialal, I. Biochemistry, Fat Soluble Vitamins; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK534869/ (accessed on 1 February 2024).
- Ross, A.C.; Caballero, B.; Cousins, R.J.; Tucker, K.; Ziegler, T. Modern Nutrition in Health and Disease, 11th ed.; Wolters Kluwer Health/Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014; pp. 260–398. [Google Scholar]
- Zinder, R.; Cooley, R.; Vlad, L.G.; Molnar, J.A. Vitamin A and Wound Healing. Nutr. Clin. Pract. 2019, 34, 839–849. [Google Scholar] [CrossRef]
- Elmadfa, I.; Meyer, A.L. The Role of the Status of Selected Micronutrients in Shaping the Immune Function. Endocr. Metab. Immune Disord. Drug Targets 2019, 19, 1100–1115. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez Gossweiler, A.; Martinez-Mier, E.A. Chapter 6: Vitamins and Oral Health. Monogr. Oral Sci. 2020, 28, 59–67. [Google Scholar] [PubMed]
- Álvarez, R.; Vaz, B.; Gronemeyer, H.; de Lera, Á.R. Functions, Therapeutic Applications, and Synthesis of Retinoids and Carotenoids. Chem. Rev. 2014, 114, 1–125. [Google Scholar] [CrossRef] [PubMed]
- Meléndez-Martínez, A.J. An Overview of Carotenoids, Apocarotenoids, and Vitamin A in Agro-Food, Nutrition, Health, and Disease. Mol. Nutr. Food Res. 2019, 63, e1801045. [Google Scholar] [CrossRef] [PubMed]
- Park, J.A.; Lee, J.H.; Lee, H.J. Association of Some Vitamins and Minerals with Periodontitis in a Nationally Representative Sample of Korean Young Adults. Biol. Trace Elem. Res. 2017, 178, 171–179. [Google Scholar] [CrossRef]
- Chaitanya, N.C.; Muthukrishnan, A.; Babu, D.B.G. Role of Vitamin E and Vitamin A in Oral Mucositis Induced by Cancer Chemo/Radiotherapy—A Meta-Analysis. J. Clin. Diagn. Res. 2017, 11, ZE06–ZE09. [Google Scholar] [CrossRef]
- Lacruz, R.S.; Habelitz, S.; Wright, J.T.; Paine, M.L. Dental Enamel Formation and Implications for Oral Health and Disease. Physiol. Rev. 2017, 97, 939–993. [Google Scholar] [CrossRef] [PubMed]
- Warren, N.G.; Body, B.A. Candidiasis. In Sexually Transmitted Diseases: Epidemiology, Pathology, Diagnosis, and Treatment; Routledge: London, UK, 2023; pp. 149–163. [Google Scholar]
- Grgurić, J.; Jovančević, M. Preventivna i Socijalna Pedijatrija; Medicinska Naklada: Zagreb, Croatia, 2018; pp. 279–285. [Google Scholar]
- Janoušek, J.; Pilařová, V.; Macáková, K.; Nomura, A.; Veiga-Matos, J.; Silva, D.D.D.; Remião, F.; Saso, L.; Malá-Ládová, K.; Malý, J.; et al. Vitamin D: Sources, Physiological Role, Biokinetics, Deficiency, Therapeutic Use, Toxicity, and Overview of Analytical Methods for Detection of Vitamin D and Its Metabolites. Crit. Rev. Clin. Lab. Sci. 2022, 59, 517–554. [Google Scholar] [CrossRef]
- Grossman, Z.; Hadjipanayis, A.; Stiris, T.; Del Torso, S.; Mercier, J.C.; Valiulis, A.; Shamir, R. Vitamin D in European Children-Statement from the European Academy of Paediatrics (EAP). Eur. J. Pediatr. 2017, 176, 829–831. [Google Scholar] [CrossRef]
- Sassi, F.; Tamone, C.; D’Amelio, P. Vitamin D: Nutrient, Hormone, and Immunomodulator. Nutrients 2018, 10, 1656. [Google Scholar] [CrossRef]
- Patseadou, M.; Haller, D.M. Vitamin D in Adolescents: A Systematic Review and Narrative Synthesis of Available Recommendations. J. Adolesc. Health 2020, 66, 388–407. [Google Scholar] [CrossRef]
- Khammissa, R.A.G.; Fourie, J.; Motswaledi, M.H.; Ballyram, R.; Lemmer, J.; Feller, L. The Biological Activities of Vitamin D and Its Receptor in Relation to Calcium and Bone Homeostasis, Cancer, Immune and Cardiovascular Systems, Skin Biology, and Oral Health. Biomed. Res. Int. 2018, 2018, 9276380. [Google Scholar] [CrossRef] [PubMed]
- Bishop, L.E.; Ismailova, A.; Dimeloe, S.; Hewison, M.; White, J.H. Vitamin D and Immune Regulation: Antibacterial, Antiviral, Anti-Inflammatory. JBMR Plus 2020, 5, e10405. [Google Scholar] [CrossRef] [PubMed]
- Uwitonze, A.M.; Rahman, S.; Ojeh, N.; Grant, W.B.; Kaur, H.; Haq, A.; Razzaque, M.S. Oral Manifestations of Magnesium and Vitamin D Inadequacy. J. Steroid Biochem. Mol. Biol. 2020, 200, 105636. [Google Scholar] [CrossRef] [PubMed]
- Combs, G.F. The Vitamins: Fundamental Aspects in Nutrition and Health, 3rd ed.; Elsevier Academic Press: Amsterdam, The Netherlands, 2008; pp. 3–177, 345–354. [Google Scholar]
- Swapna, L.A.; Abdulsalam, R. Vitamin D Deficiency and Its Effects on Tooth Structure and Pulpal Changes. Open Access Maced. J. Med. Sci. 2021, 9, 81–87. [Google Scholar] [CrossRef]
- Aguiar, M.; Andronis, L.; Pallan, M.; Högler, W.; Frew, E. The Economic Case for Prevention of Population Vitamin D Deficiency: A Modelling Study Using Data from England and Wales. Eur. J. Clin. Nutr. 2020, 74, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Toupenay, S.; Fournier, B.P.; Manière, M.C.; Naulin, C.I.; Berdal, A.; Molla, M.L.D. Amelogenesis Imperfecta: Therapeutic Strategy from Primary to Permanent Dentition Across Case Reports. BMC Oral Health. 2018, 18, 108. [Google Scholar] [CrossRef]
- Wright, J.T.; Grange, D.K.; Fete, M. Hypohidrotic Ectodermal Dysplasia. GeneReviews®; University of Washington: Seattle, WA, USA, 1993. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1112/ (accessed on 1 February 2024).
- Mortensen, N.B.; Haubek, D.; Dalgård, C.; Nørgaard, S.M.; Christoffersen, L.; Cantio, E.; Rasmussen, A.; Möller, S.; Christesen, H.T. Vitamin D Status and Tooth Enamel Hypomineralization Are Not Associated in 4-y-old Children: An Odense Child Cohort Study. J. Steroid Biochem. Mol. Biol. 2022, 221, 106130. [Google Scholar] [CrossRef]
- Dudding, T.; Thomas, S.J.; Duncan, K.; Lawlor, D.A.; Timpson, N.J. Re-examining the Association Between Vitamin D and Childhood Caries. PLoS ONE 2015, 10, e0143769. [Google Scholar] [CrossRef][Green Version]
- Herzog, K.; Scott, J.M.; Hujoel, P.; Seminario, A.L. Association of Vitamin D and Dental Caries in Children: Findings from the National Health and Nutrition Examination Survey, 2005–2006. J. Am. Dent. Assoc. 2016, 147, 413–420. [Google Scholar] [CrossRef]
- Hujoel, P.P. Vitamin D and Dental Caries in Controlled Clinical Trials: Systematic Review and Meta-Analysis. Nutr. Rev. 2013, 71, 88–97. [Google Scholar] [CrossRef]
- Nørrisgaard, P.E.; Haubek, D.; Kühnisch, J.; Chawes, B.L.; Stokholm, J.; Bønnelykke, K.; Bisgaard, H. Association of High-Dose Vitamin D Supplementation During Pregnancy with the Risk of Enamel Defects in Offspring: A 6-Year Follow-Up of a Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Rosier, B.T.; Marsh, P.D.; Mira, A. Resilience of the Oral Microbiota in Health: Mechanisms That Prevent Dysbiosis. J. Dent. Res. 2018, 97, 371–380. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Zhou, Y.; Shi, J. The Association Between Serum 25-Hydroxyvitamin D Levels and Dental Caries in US Adults. Oral Dis. 2020, 26, 1537–1547. [Google Scholar] [CrossRef] [PubMed]
- Wójcik, D.; Krzewska, A.; Szalewski, L.; Pietryka-Michałowska, E.; Szalewska, M.; Krzewski, S.; Pels, E.; Beń-Skowronek, I. Dental Caries and Vitamin D3 in Children with Growth Hormone Deficiency. Medicine 2018, 97, e9811. [Google Scholar] [CrossRef] [PubMed]
- Gyll, J.; Ridell, K.; Öhlund, I.; Karlsland Åkeson, P.; Johansson, I.; Lif Holgerson, P. Vitamin D Status and Dental Caries in Healthy Swedish Children. Nutr. J. 2018, 17, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhang, W.; Li, H.; Aprecio, R.; Wu, W.; Lin, Y.; Li, Y. Effects of 25-Hydroxyvitamin D3 on Cathelicidin Production and Antibacterial Function of Human Oral Keratinocytes. Cell. Immunol. 2013, 283, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Davidopoulou, S.; Diza, E.; Sakellari, D.; Menexes, G.; Kalfas, S. Salivary Concentration of Free LL-37 in Edentulism, Chronic Periodontitis, and Healthy Periodontium. Arch. Oral Biol. 2013, 58, 930–934. [Google Scholar] [CrossRef] [PubMed]
- Hans, M.; Madaan Hans, V. Epithelial Antimicrobial Peptides: Guardian of the Oral Cavity. Int. J. Pept. 2014, 2014, 370297. [Google Scholar] [CrossRef]
- Khurshid, Z.; Naseem, M.; Yahya, I.A.F.; Mali, M.; Sannam Khan, R.; Sahibzada, H.A.; Zafar, M.S.; Moin, S.F.; Khan, E. Significance and Diagnostic Role of Antimicrobial Cathelicidins (LL-37) Peptides in Oral Health. Biomolecules 2017, 7, 80. [Google Scholar] [CrossRef]
- Grant, M.; Kilsgard, O.; Akerman, S.; Klinge, B.; Demmer, R.T.; Malmstrom, J.; Jonsson, D. The Human Salivary Antimicrobial Peptide Profile According to the Oral Microbiota in Health, Periodontitis, and Smoking. J. Innate Immun. 2018, 11, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Singleton, R.; Day, G.; Thomas, T.; Schroth, R.; Klejka, J.; Lenaker, D.; Berner, J. Association of Maternal Vitamin D Deficiency with Early Childhood Caries. J. Dent. Res. 2019, 98, 549–555. [Google Scholar] [CrossRef]
- Tang, X.; Pan, Y.; Zhao, Y. Vitamin D Inhibits the Expression of Interleukin-8 in Human Periodontal Ligament Cells Stimulated with Porphyromonas gingivalis. Arch. Oral Biol. 2013, 58, 397–407. [Google Scholar] [CrossRef] [PubMed]
- Nebel, D.; Svensson, D.; Arosenius, K.; Larsson, E.; Jönsson, D.; Nilsson, B.O. 1α,25-Dihydroxyvitamin D3 Promotes Osteogenic Activity and Downregulates Proinflammatory Cytokine Expression in Human Periodontal Ligament Cells. J. Periodont. Res. 2015, 50, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Jagelavičiene, E.; Vaitkevičiene, I.; Šilingaite, D.; Šinknuaite, E.; Daugelaite, G. The Relationship Between Vitamin D and Periodontal Pathology. Medicina 2018, 54, 45. [Google Scholar] [CrossRef]
- Antonucci, R.; Locci, C.; Clemente, M.G.; Chicconi, E.; Antonucci, L. Vitamin D Deficiency in Childhood: Old Lessons and Current Challenges. J. Pediatr. Endocrinol. Metab. 2018, 31, 247–260. [Google Scholar] [CrossRef]
- Szewczyk, K.; Chojnacka, A.; Górnicka, M. Tocopherols and Tocotrienols-Bioactive Dietary Compounds; What Is Certain, What Is Doubt? Int. J. Mol. Sci. 2021, 22, 6222. [Google Scholar] [CrossRef]
- Meganathan, P.; Fu, J.Y. Biological Properties of Tocotrienols: Evidence in Human Studies. Int. J. Mol. Sci. 2016, 17, 1682. [Google Scholar] [CrossRef]
- Jiang, Q. Metabolism of Natural Forms of Vitamin E and Biological Actions of Vitamin E Metabolites. Free Radic. Biol. Med. 2022, 179, 375–387. [Google Scholar] [CrossRef]
- Kemnic, T.R.; Coleman, M. Vitamin E Deficiency. In Nutrition and the Eye: A Practical Approach; Butterworth-Heinemann: Oxford, UK, 2023; pp. 121–122. [Google Scholar]
- Jilani, T.; Iqbal, M.P. Vitamin E Deficiency in South Asian Population and the Therapeutic Use of Alpha-Tocopherol (Vitamin E) for Correction of Anemia. Pak. J. Med. Sci. 2018, 34, 1571–1575. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Almas, K. The Role of Nutrition in Periodontal Health: An Update. Nutrients 2016, 8, 530. [Google Scholar] [CrossRef] [PubMed]
- Shahidi, F.; Pinaffi-Langley, A.C.C.; Fuentes, J.; Speisky, H.; de Camargo, A.C. Vitamin E as an Essential Micronutrient for Human Health: Common, Novel, and Unexplored Dietary Sources. Free Radic. Biol. Med. 2021, 176, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Schwalfenberg, G.K. Vitamins K1 and K2: The Emerging Group of Vitamins Required for Human Health. J. Nutr. Metab. 2017, 2017, 6254836. [Google Scholar] [CrossRef]
- Riley, P.; Glenny, A.M.; Worthington, H.V.; Littlewood, A.; Fernandez Mauleffinch, L.M.; Clarkson, J.E.; McCabe, M.G. Interventions for Preventing Oral Mucositis in Patients with Cancer Receiving Treatment: Cytokines and Growth Factors. Cochrane Database Syst. Rev. 2017, 11, CD011990. [Google Scholar] [CrossRef] [PubMed]
- Halder, M.; Petsophonsakul, P.; Akbulut, A.C.; Pavlic, A.; Bohan, F.; Anderson, E.; Maresz, K.; Kramann, R.; Schurgers, L. Vitamin K: Double Bonds beyond Coagulation Insights into Differences between Vitamin K1 and K2 in Health and Disease. Int. J. Mol. Sci. 2019, 20, 896. [Google Scholar] [CrossRef]
- Akbulut, A.C.; Pavlic, A.; Petsophonsakul, P.; Halder, M.; Maresz, K.; Kramann, R.; Schurgers, L. Vitamin K2 Needs an RDI Separate from Vitamin K1. Nutrients 2020, 12, 1852. [Google Scholar] [CrossRef]
- Zurynski, Y.; Grover, C.J.; Jalaludin, B.; Elliott, E.J. Vitamin K Deficiency Bleeding in Australian Infants 1993-2017: An Australian Paediatric Surveillance Unit Study. Arch. Dis. Child. 2020, 105, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Magnusson, M.; Ignjatovic, V.; Hardikar, W.; Monagle, P. A Conceptual and Practical Approach to Haemostasis in Paediatric Liver Disease. Arch. Dis. Child. 2016, 101, 854–859. [Google Scholar] [CrossRef]
- Zeynelabidin, S.; Klouwer, F.C.C.; Meijers, J.C.M.; Suijker, M.H.; Engelen, M.; Poll-The, B.T.; van Ommen, C.H. Coagulopathy in Zellweger Spectrum Disorders: A Role for Vitamin K. J. Inherit. Metab. Dis. 2018, 41, 249–255. [Google Scholar] [CrossRef]
- Jagannath, V.A.; Thaker, V.; Chang, A.B.; Price, A.I. Vitamin K Supplementation for Cystic Fibrosis. Cochrane Database Syst. Rev. 2017, 8, CD008482. [Google Scholar] [CrossRef]
- Engelen, E.T.; Schutgens, R.E.; Mauser-Bunschoten, E.P.; van Es, R.J.; van Galen, K.P. Antifibrinolytic Therapy for Preventing Oral Bleeding in People on Anticoagulants Undergoing Minor Oral Surgery or Dental Extractions. Cochrane Database Syst. Rev. 2018, 7, CD012293. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, D.O. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients 2016, 8, 68. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.B.; Wang, Y.F.; Hou, W.; Wang, Y.P.; Xiao, S.Y.; Fu, Y.Y.; Wang, J.; Zheng, S.W.; Zheng, P.H. Effect of B-Complex Vitamins on the Antifatigue Activity and Bioavailability of Ginsenoside Re after Oral Administration. J. Ginseng Res. 2017, 41, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.L.; Zheng, J.B.; Chen, F.S. Relationships between Degree of Milling and Loss of Vitamin B, Minerals, and Change in Amino Acid Composition of Brown Rice. LWT-Food Sci. Technol. 2017, 82, 429–436. [Google Scholar] [CrossRef]
- Wiley, K.D.; Gupta, M. Vitamin B1 (Thiamine) Deficiency; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537204/ (accessed on 1 February 2024).
- Cavalcoli, F.; Zilli, A.; Conte, D.; Massironi, S. Micronutrient Deficiencies in Patients with Chronic Atrophic Autoimmune Gastritis: A Review. World J. Gastroenterol. 2017, 23, 563–572. [Google Scholar] [CrossRef]
- Edwards, K.A.; Tu-Maung, N.; Cheng, K. Thiamine Assays—Advances, Challenges, and Caveats. ChemistryOpen 2017, 6, 178–191. [Google Scholar] [CrossRef]
- Moskovitz, M.; Dotan, M.; Zilberman, U. The Influence of Infantile Thiamine Deficiency on Primary Dentition. Clin. Oral Investig. 2017, 21, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Al-Maweri, S.A.; Halboub, E.; Ashraf, S.; Alqutaibi, A.Y.; Qaid, N.M.; Yahya, K. Single Application of Topical Doxycycline in Management of Recurrent Aphthous Stomatitis: A Systematic Review and Meta-Analysis of the Available Evidence. BMC Oral Health 2020, 20, 231. [Google Scholar] [CrossRef]
- Plewa, M.C.; Chatterjee, K. Recurrent Aphthous Stomatitis. In European Handbook of Dermatological Treatments, 3rd ed.; Springer: Berlin/Heidelberg, Germany, 2023; pp. 67–71. [Google Scholar]
- Yılmaz, S.; Tuna Kırsaçlıoğlu, C.; Şaylı, T.R. Celiac Disease and Hematological Abnormalities in Children with Recurrent Aphthous Stomatitis. Pediatr. Int. 2020, 62, 705–710. [Google Scholar] [CrossRef]
- Sharabi, A.F.; Winters, R. Glossitis; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK560627/ (accessed on 1 February 2024).
- Li, R.; Yu, K.; Wang, Q.; Wang, L.; Mao, J.; Qian, J. Pellagra Secondary to Medication and Alcoholism: A Case Report and Review of the Literature. Nutr. Clin. Pract. 2016, 31, 785–789. [Google Scholar] [CrossRef]
- Redzic, S.; Hashmi, M.F.; Gupta, V. Niacin Deficiency. South Med. J. 2023, 45, 775. [Google Scholar]
- Palmer, C.A.; Boyd, L.D. Diet and Nutrition in Oral Health, 3rd ed.; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2016; pp. 187–230. [Google Scholar]
- Sanvictores, T.; Chauhan, S. Vitamin B5 (Pantothenic Acid). In Clinical Guide to Nutrition & Dietary Supplements in Disease Management; Churchill Livingstone: London, UK, 2023; pp. 699–701. [Google Scholar]
- Alibabić, V.; Mujić, I. Pravilna Prehrana i Zdravlje, 1st ed.; Veleučilište u Rijeci: Rijeka, Croatia, 2016. [Google Scholar]
- Brown, M.J.; Ameer, M.A.; Daley, S.F.; Beier, K. Vitamin B6 Deficiency; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470579/ (accessed on 1 February 2024).
- Bistas, K.G.; Tadi, P. Biotin; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK554493/ (accessed on 1 February 2024).
- Wolf, B. Biotinidase Deficiency. In GeneReviews®; University of Washington: Seattle, WA, USA, 1993. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1322/ (accessed on 1 February 2024).
- Hu, L.; Zhou, M.; Young, A.; Zhao, W.; Yan, Z. In Vivo Effectiveness and Safety of Probiotics on Prophylaxis and Treatment of Oral Candidiasis: A Systematic Review and Meta-Analysis. BMC Oral Health 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Anonymous. LiverTox: Clinical and Research Information on Drug—Induced Liver Injury. Folic Acid; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012. [Google Scholar]
- Rathee, M.; Jain, P. Gingivitis. Aust. J. Pharm. 2023, 96, 64–67. [Google Scholar]
- Green, R.; Miller, J.W. Vitamin B12 Deficiency. Vitam. Horm. 2022, 119, 405–439. [Google Scholar] [PubMed]
- Gramer, G.; Hoffmann, G.F. Vitamin B12 Deficiency in Newborns and Their Mothers-Novel Approaches to Early Detection, Treatment, and Prevention of a Global Health Issue. Curr. Med. Sci. 2020, 40, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Hawthorne, S.; Levy, H.L. Can Newborn Screening for Vitamin B12 Deficiency be Incorporated into All Newborn Screening Programs? J. Pediatr. 2020, 216, 9–11.e1. [Google Scholar] [CrossRef] [PubMed]
- Green, R. Vitamin B12 Deficiency from the Perspective of a Practicing Hematologist. Blood 2017, 129, 2603–2611. [Google Scholar] [CrossRef] [PubMed]
- Khan, N.F.; Saeed, M.; Chaudhary, S. Haematological Parameters and Recurrent Aphthous Stomatitis. J. Coll. Physicians Surg. Pak. 2013, 23, 124–127. [Google Scholar]
- Liu, H.L.; Chiu, S.C. The Effectiveness of Vitamin B12 for Relieving Pain in Aphthous Ulcers: A Randomized, Double-blind, Placebo-controlled Trial. Pain Manag. Nurs. 2015, 16, 182–187. [Google Scholar] [CrossRef]
- Lugović-Mihić, L.; Špiljak, B.; Blagec, T.; Delaš Aždajić, M.; Franceschi, N.; Gašić, A.; Parać, E. Factors Participating in the Occurrence of Inflammation of the Lips (Cheilitis) and Perioral Skin. Cosmetics 2023, 10, 9. [Google Scholar] [CrossRef]
- Blagec, T.; Glavina, A.; Špiljak, B.; Bešlić, I.; Bulat, V.; Lugović-Mihić, L. Cheilitis: A Cross-Sectional Study-Multiple Factors Involved in the Aetiology and Clinical Features. Oral Dis. 2023, 29, 3360–3371. [Google Scholar] [CrossRef]
- Abdullah, M.; Jamil, R.T.; Attia, F.N. Vitamin C (Ascorbic Acid). In Encyclopedia of Toxicology, 3rd ed.; Academic Press: Cambridge, MA, USA, 2023; pp. 962–963. [Google Scholar]
- DePhillipo, N.N.; Aman, Z.S.; Kennedy, M.I.; Begley, J.P.; Moatshe, G.; LaPrade, R.F. Efficacy of Vitamin C Supplementation on Collagen Synthesis and Oxidative Stress After Musculoskeletal Injuries: A Systematic Review. Orthop. J. Sports Med. 2018, 6, 2325967118804544. [Google Scholar] [CrossRef] [PubMed]
- Padayatty, S.J.; Levine, M. Vitamin C: The Known and the Unknown and Goldilocks. Oral Dis. 2016, 22, 463–493. [Google Scholar] [CrossRef] [PubMed]
- Pullar, J.M.; Carr, A.C.; Vissers, M.C.M. The Roles of Vitamin C in Skin Health. Nutrients 2017, 9, 866. [Google Scholar] [CrossRef] [PubMed]
- Corpe, C.P.; Eck, P.; Wang, J.; Al-Hasani, H.; Levine, M. Intestinal Dehydroascorbic Acid (DHA) Transport Mediated by the Facilitative Sugar Transporters, GLUT2 and GLUT8. J. Biol. Chem. 2013, 288, 9092–9101. [Google Scholar] [CrossRef] [PubMed]
- Alagl, A.S.; Bhat, S.G. Ascorbic Acid: New Role of an Age-Old Micronutrient in the Management of Periodontal Disease in Older Adults. Geriatr. Gerontol. Int. 2015, 15, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Gicchino, M.F.; Romano, A.; Cioffi, S.; Fiori, F.; Miraglia del Giudice, E.; Lucchese, A.; Olivieri, A.N.; Serpico, R. Oral Manifestations in Scurvy Pediatric Patients: A Systematic Review and a Case Report. Appl. Sci. 2021, 11, 8323. [Google Scholar] [CrossRef]
- Fujii, T.; Luethi, N.; Young, P.J.; Frei, D.R.; Eastwood, G.M.; French, C.J.; Deane, A.M.; Shehabi, Y.; Hajjar, L.A.; Oliveira, G.; et al. Effect of Vitamin C, Hydrocortisone, and Thiamine vs Hydrocortisone Alone on Time Alive and Free of Vasopressor Support among Patients with Septic Shock: The VITAMINS Randomized Clinical Trial. J. Am. Med. Assoc. 2020, 323, 423–431. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Qiao, Y.; Zhang, Z.; Wu, Z.; Liu, D.; Liao, Z.; Yin, D.; He, M. Dual Action of Vitamin C in Iron Supplement Therapeutics for Iron Deficiency Anemia: Prevention of Liver Damage Induced by Iron Overload. Food Funct. 2018, 9, 5390–5401. [Google Scholar] [CrossRef]
- Smirnoff, N. Ascorbic Acid Metabolism and Functions: A Comparison of Plants and Mammals. Free Radic. Biol. Med. 2018, 122, 116–129. [Google Scholar] [CrossRef]
- Perkins, A.; Sontheimer, C.; Otjen, J.P.; Shenoi, S. Scurvy Masquerading as Juvenile Idiopathic Arthritis or Vasculitis with Elevated Inflammatory Markers: A Case Series. J. Pediatr. 2020, 218, 234–237.e2. [Google Scholar] [CrossRef] [PubMed]
- Hahn, T.; Adams, W.; Williams, K. Is Vitamin C Enough? A Case Report of Scurvy in a Five-Year-Old Girl and Review of the Literature. BMC Pediatr. 2019, 19, 74. [Google Scholar]
- Sharp, W.G.; Berry, R.C.; Burrell, L.; Scahill, L.; McElhanon, B.O. Scurvy as a Sequela of Avoidant-Restrictive Food Intake Disorder in Autism: A Systematic Review. J. Dev. Behav. Pediatr. 2020, 41, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Mealey, B.L.; Van Dyke, T.E.; Bartold, P.M.; Dommisch, H.; Eickholz, P.; Geisinger, M.L.; Genco, R.J.; Glogauer, M.; Goldstein, M.; et al. Periodontal Health and Gingival Diseases and Conditions on an Intact and a Reduced Periodontium: Consensus Report of Workgroup 1 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S74–S84. [Google Scholar] [CrossRef] [PubMed]
- Fortenberry, M.; Rucker, H.; Gaines, K. Pediatric Scurvy: How an Old Disease Is Becoming a New Problem. J. Pediatr. Pharmacol. Ther. 2020, 25, 735–741. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Shaharyar, A.; Kumar, A.; Bhat, M.S.; Mishra, M. Scurvy in Pediatric Age Group—A Disease Often Forgotten? J. Clin. Orthop. Trauma 2015, 6, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Byard, R.W.; Maxwell-Stewart, H. Scurvy-Characteristic Features and Forensic Issues. Am. J. Forensic Med. Pathol. 2019, 40, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Robitaille, L.; Hoffer, L.J. A Simple Method for Plasma Total Vitamin C Analysis Suitable for Routine Clinical Laboratory Use. Nutr. J. 2016, 15, 40. [Google Scholar] [CrossRef]
- Vaezipour, N.; Leibundgut, K. Nonalimental Scurvy with Relapse Symptoms after Stopping Oral Vitamin C Supplementation. Pediatrics 2018, 142, e20172139. [Google Scholar] [CrossRef]
- Plevin, D.; Galletly, C. The Neuropsychiatric Effects of Vitamin C Deficiency: A Systematic Review. BMC Psychiatry 2020, 20, 315. [Google Scholar] [CrossRef]
- Cazzolla, A.P.; Cosola, M.D.; Ballini, A.; Santacroce, L.; Lovero, R.; Testa, N.F.; Lacarbonara, V.; De Franco, A.; Troiano, G.; Cantore, S.; et al. The Association between Nutritional Alterations and Oral Lesions in a Pediatric Population: An Epidemiological Study. Biomed. Res. Int. 2021, 2021, 9992451. [Google Scholar] [CrossRef] [PubMed]
- Niazi, F.C.; Pepper, T. Dental Fluorosis; StatPearls Publishing: Treasure Island, FL, USA, 2024. Available online: https://www.ncbi.nlm.nih.gov/books/NBK585039/ (accessed on 23 March 2024).
- Patel, P.P.; Patel, P.A.; Zulf, M.M.; Yagnik, B.; Kajale, N.; Mandlik, R.; Khadilkar, V.; Chiplonkar, S.A.; Phanse, S.; Patwardhan, V.; et al. Association of dental and skeletal fluorosis with calcium intake and serum vitamin D concentration in adolescents from a region endemic for fluorosis. Indian J. Endocrinol. Metab. 2017, 21, 190–195. [Google Scholar]
- Andrés, C.M.C.; Pérez de la Lastra, J.M.; Juan, C.A.; Plou, F.J.; Pérez-Lebeña, E. Antioxidant Metabolism Pathways in Vitamins, Polyphenols, and Selenium: Parallels and Divergences. Int. J. Mol. Sci. 2024, 25, 2600. [Google Scholar] [CrossRef]
- Fasano, A.; Catassi, C. Clinical practice. Celiac disease. N. Engl. J. Med. 2012, 367, 2419–2426. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, C.N.; Blanchard, J.F.; Rawsthorne, P.; Yu, N. The prevalence of extraintestinal diseases in inflammatory bowel disease: A population-based study. Am. J. Gastroenterol. 2001, 96, 1116–1122. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.M.; Darukhanavala, A.; Hicks, R.; Kelly, A. An update on methods for assessing bone quality and health in Cystic Fibrosis. J. Clin. Transl. Endocrinol. 2021, 27, 100281. [Google Scholar] [CrossRef]
- Freitas, L.G.; Cortés, M.A.P.; Stein, C.; Cousin, E.; Faustino-Silva, D.D.; Hilgert, J.B. Dietary Intake Quality and Associated Factors in One-Year-Old Children Seen by Primary Healthcare Services. Ciênc. Saúde Coletiva 2020, 25, 2561–2570. [Google Scholar] [CrossRef]
- Posa, F.; Colaianni, G.; Di Cosola, M.; Dicarlo, M.; Gaccione, F.; Colucci, S.; Grano, M.; Mori, G. The Myokine Irisin Promotes Osteogenic Differentiation of Dental Bud-Derived MSCs. Biology 2021, 10, 295. [Google Scholar] [CrossRef]
- Charitos, I.A.; Ballini, A.; Cantore, S.; Boccellino, M.; Di Domenico, M.; Borsani, E.; Nocini, R.; Di Cosola, M.; Santacroce, L.; Bottalico, L. Stem Cells: A Historical Review about Biological, Religious, and Ethical Issues. Stem Cells Int. 2021, 2021, 9978837. [Google Scholar] [CrossRef]
- Kresevic, D.M.; Denton, J.E.; Burant, C.J.; Pallaki, M. Racial Difference in Response to Vitamin D Supplementation. J. Natl. Med. Assoc. 2015, 107, 18–24. [Google Scholar] [CrossRef]
- Girish Babu, K.L.; Subramaniam, P.; Madhusudan, K.S. Association of Nutritional Status and Dental Health among 3–6 -year-old Children of a South Indian Population. Saudi J. Oral. Sci. 2019, 6, 31–36. [Google Scholar]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Vitamin | Life Stage | ||||||
|---|---|---|---|---|---|---|---|
| Birth–6 Months | 7–12 Months | 1–3 Years | 4–8 Years | 9–13 Years | Teen Males 14–18 Years | Teen Females 14–18 Years | |
| Vitamin A (mcg RAE) | 400 | 500 | 300 | 400 | 600 | 900 | 700 |
| Vitamin D (mcg/IU) | 10/400 | 10/400 | 15/600 | 15/600 | 15/600 | 15/600 | 15/600 |
| Vitamin E (mg) | 4 | 5 | 6 | 7 | 11 | 15 | 15 |
| Vitamin K (mcg) | 2 | 2.5 | 30 | 55 | 60 | 75 | 75 |
| Vitamin | Life Stage | ||||||
|---|---|---|---|---|---|---|---|
| Birth–6 Months | 7–12 Months | 1–3 Years | 4–8 Years | 9–13 Years | Teen Males 14–18 Years | Teen Females 14–18 Years | |
| Vitamin B1 (mg) | 0.2 | 0.3 | 0.5 | 0.6 | 0.9 | 1.2 | 1 |
| Vitamin B2 (mg) | 0.3 | 0.4 | 0.5 | 0.6 | 0.9 | 1.3 | 1 |
| Vitamin B3 (mg NE) | 2 ** | 4 | 6 | 8 | 12 | 16 | 14 |
| Vitamin B5 (mg) | 1.7 | 1.8 | 2 | 3 | 4 | 5 | 5 |
| Vitamin B6 (mg) | 0.1 | 0.3 | 0.5 | 0.6 | 1 | 1.3 | 1.2 |
| Vitamin B7/H (mcg) | 5 | 6 | 8 | 12 | 20 | 25 | 25 |
| Vitamin B9 (mcg DFE) | 65 | 80 | 150 | 200 | 300 | 400 | 400 |
| Vitamin B12 (mcg) | 0.4 | 0.5 | 0.9 | 1.2 | 1.8 | 2.4 | 2.4 |
| Vitamin C (mg) | 40 | 50 | 15 | 25 | 45 | 75 | 65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lešić, S.; Ivanišević, Z.; Špiljak, B.; Tomas, M.; Šoštarić, M.; Včev, A. The Impact of Vitamin Deficiencies on Oral Manifestations in Children. Dent. J. 2024, 12, 109. https://doi.org/10.3390/dj12040109
Lešić S, Ivanišević Z, Špiljak B, Tomas M, Šoštarić M, Včev A. The Impact of Vitamin Deficiencies on Oral Manifestations in Children. Dentistry Journal. 2024; 12(4):109. https://doi.org/10.3390/dj12040109
Chicago/Turabian StyleLešić, Stjepanka, Zrinka Ivanišević, Bruno Špiljak, Matej Tomas, Magdalena Šoštarić, and Aleksandar Včev. 2024. "The Impact of Vitamin Deficiencies on Oral Manifestations in Children" Dentistry Journal 12, no. 4: 109. https://doi.org/10.3390/dj12040109
APA StyleLešić, S., Ivanišević, Z., Špiljak, B., Tomas, M., Šoštarić, M., & Včev, A. (2024). The Impact of Vitamin Deficiencies on Oral Manifestations in Children. Dentistry Journal, 12(4), 109. https://doi.org/10.3390/dj12040109