
Observance of the Atlantic Diet in a Healthy Population from Galicia (NW Spain): A Comparative Study Using a New Scale-Based Procedure to Assess Adherence

 ,
,  ,
,  , and
, and 
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population and Ethical Statement
2.2. Questionnaire on Dietary Habits
2.3. Data Matrix
2.4. Statistical Analysis
2.5. Proposed Procedure for Assessment of Adherence to the AD: The Atlantic Diet Scale (ADS)
2.6. Other Procedures for Assessing Adherence to the Atlantic Diet
3. Results and Discussion
3.1. Galician Consuming Pattern-2022 (GCP-2022)
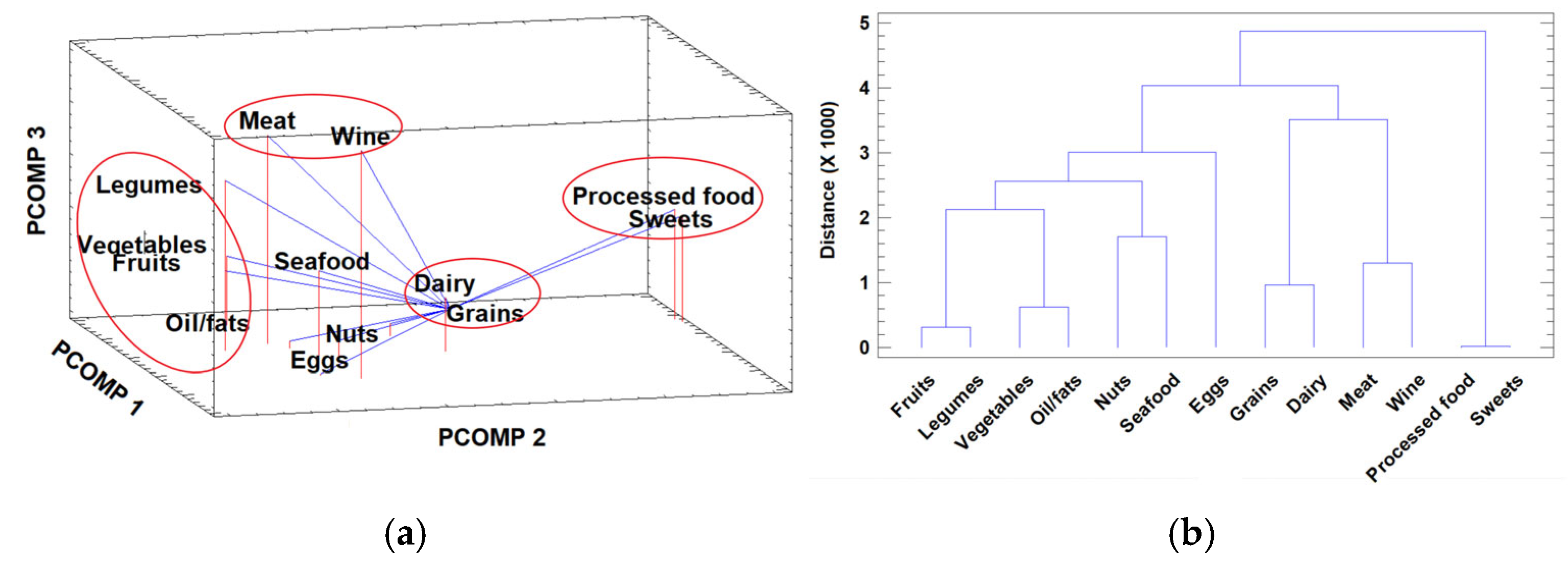
3.1.1. Multivariate Data Visualization
3.1.2. Intake Patterns: Influence of Gender, Age and Geographic Origin
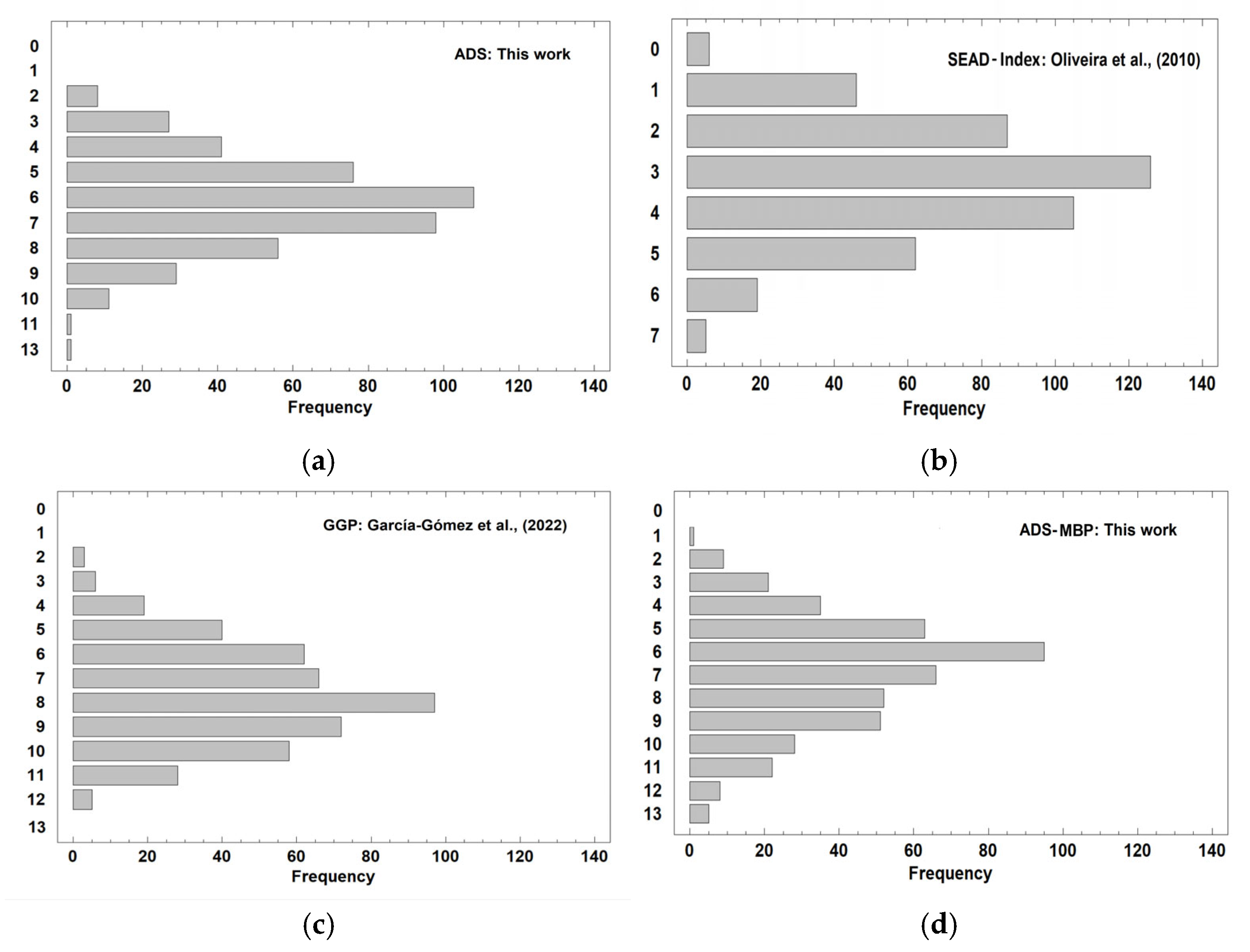
3.2. Adherence to the Atlantic Diet
3.3. Study Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sales, N.M.R.; Pelegrini, P.B.; Goersch, M.C. Nutrigenomics: Definitions and advances of this new science. J. Nutr. Metab. 2014, 2014, 202759. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Lopes, C.; Rodríguez-Artalejo, F. Adherence to the Southern European Atlantic Diet and occurrence of nonfatal acute myocardial infarction. Am. J. Clin. Nutr. 2010, 92, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Velho, M.V.; Pinheiro, R.; Rodrigues, A.S. The Atlantic diet–Origin and features. Int. J. Food Stud. 2016, 5, 106–119. [Google Scholar] [CrossRef]
- Leis Trabazo, R.; de Lamas Pérez, C.; Castro Pérez, X.; Solla, P. Atlantic diet. Nutrition and gastronomy in Galicia. Nutr. Hosp. 2019, 36, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Agricultura pesca y Alimentación. Protected Designations of Origin (D.O.P.) Protected Geographical Indication (I.G.P.). Available online: https://www.mapa.gob.es/en/alimentacion/temas/calidad-diferenciada/dop-igp/ (accessed on 30 June 2025).
- López-Iglesias, E. The agricultural and agri-food sector in Galicia; assessment of changes since European integration, 1986–2016. RGE/GJE 2019, 28, 1–20. [Google Scholar] [CrossRef]
- Casanueva Freijó, F. Bases Científicas de la Dieta Atlántica; Servicio de Publicaciones e Intercambio Científico, Universidad de Santiago de Compostela: Santiago de Compostela, Spain, 2020. [Google Scholar]
- García-Gómez, B.; Rivas-Casais, A.; Lorences-Touzón, R.; Piedrafita-Páez, N.; Muñoz-Ferreiro, N.; Vázquez-Odériz, L.; Romero-Rodríguez, Á. Adherence to and knowledge about the Atlantic Diet pattern in the senior population of the Galician region (NW-Spain). J. Funct. Foods 2022, 91, 105015. [Google Scholar] [CrossRef]
- Tojo, R.; Leis, R. El papel de la Dieta Atlántica como contrapunto saludable a la Dieta Occidental actual. In La Dieta Atlántica, el Pescado y las Algas—Su Importancia en el Neurodesarrollo y la Función Cerebral; Fundación Dieta Atlántica, Universidade de Santiago de Compostela: Santiago de Compostela, Spain, 2009; pp. 23–28. [Google Scholar]
- Schwingshackl, L.; Hoffmann, G. Monounsaturated fatty acids and risk of cardiovascular disease: Synopsis of the evidence available from systematic reviews and meta-analyses. Nutrients 2012, 4, 1989–2007. [Google Scholar] [CrossRef] [PubMed]
- Olas, B. The cardioprotective properties of selected nuts: Their functional ingredients and molecular mechanisms. Foods 2024, 13, 242. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.; Bergamaschi, M.; Magro, L.; Petrini, A.; Bittante, G. Relationships of a detailed mineral profile of meat with animal performance and beef quality. Animals 2019, 9, 1073. [Google Scholar] [CrossRef] [PubMed]
- Bakaloudi, D.R.; Halloran, A.; Rippin, H.L.; Oikonomidou, A.C.; Dardavesis, T.I.; Williams, J.; Wickramasinghe, K.; Breda, J.; Chourdakis, M. Intake and adequacy of the vegan diet. A systematic review of the evidence. Clin. Nutr. 2021, 40, 3503–3521. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, C.; Fente, C.; Barreiro, R.; López-Racamonde, O.; Cepeda, A.; Regal, P. Association between breast milk mineral content and maternal adherence to healthy dietary patterns in Spain: A Transversal study. Foods 2020, 9, 659. [Google Scholar] [CrossRef] [PubMed]
- Tunick, M.H.; Van Hekken, D.L. Dairy products and health: Recent insights. J. Agric. Food Chem. 2015, 63, 9381–9388. [Google Scholar] [CrossRef] [PubMed]
- Vivanco, P.G.; Taboada, P.; Coelho, A. The Southern European Atlantic diet and Its supplements: The chemical bases of its anticancer properties. Nutrients 2023, 15, 4274. [Google Scholar] [CrossRef] [PubMed]
- Instituto Galego de Estatística. Esperanza de Vida sen Limitación: Resumo de Resultados; IGE: Santiago de Compostela, Spain, 2022; Available online: https://www.ige.gal/estatico/html/gl/OperacionsEstruturais/PDF/Resumo_resultados_Esperanza_sen_limitacion_2019.pdf (accessed on 28 June 2025).
- Lorenzo, P.M.; Izquierdo, A.G.; Rodríguez-Carnero, G.; Fernández-Pombo, A.; Iglesias, A.; Carreira, M.C.; Tejera, C.; Bellido, D.; Martínez-Olmos, M.A.; Leis, R.; et al. Epigenetic effects of healthy foods and lifestyle habits from the Southern European Atlantic diet pattern: A Narrative review. Adv. Nutr. 2022, 13, 1725–1747. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Malvar, M.; Leis, R.; Benítez-Estévez, A.J.; Sánchez-Castro, J.; Gude, F. A randomised, family-focused dietary intervention to evaluate the Atlantic diet: The GALIAT study protocol. BMC Public Health 2016, 16, 820. [Google Scholar] [CrossRef] [PubMed]
- Porto-Arias, J.J.; Lorenzo, T.; Lamas, A.; Regal, P.; Cardelle-Cobas, A.; Cepeda, A. Food patterns and nutritional assessment in Galician university students. J. Physiol. Biochem. 2018, 74, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Carballo-Casla, A.; Stefler, D.; Ortolá, R.; Chen, Y.; Knuppel, A.; Kubinova, R.; Pajak, A.; Rodríguez-Artalejo, F.; Brunner, E.J.; Bobak, M. The Southern European Atlantic diet and all-cause and cause-specific mortality: A European multicohort study. Eur. J. Prev. Cardiol. 2024, 31, 358–367. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Llorens, X.; Moreira, M.T.; Feijoo, G.; González-García, S. Linking environmental sustainability and nutritional quality of the Atlantic diet recommendations and real consumption habits in Galicia (NW Spain). Sci. Total Environ. 2019, 683, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Esteve-Llorens, X.; Darriba, C.; Moreira, M.T.; Feijoo, G.; González-García, S. Towards an environmentally sustainable and healthy Atlantic dietary pattern: Life cycle carbon footprint and nutritional quality. Sci. Total Environ. 2019, 646, 704–715. [Google Scholar] [CrossRef] [PubMed]
- da Costa, G.G.; da Conceição Nepomuceno, G.; da Silva Pereira, A.; Teixeira Simões, B.F. Worldwide dietary patterns and their association with socioeconomic data: An ecological exploratory study. Glob. Health 2022, 18, 31. [Google Scholar] [CrossRef] [PubMed]
- DGSP-Dirección General de Salud Pública. Encuesta Sobre los Hábitos Alimentarios de la Población Adulta Gallega; Consellería de Sanidad, Xunta de Galicia: Santiago de Compostela, Spain, 2007; Available online: https://www.sergas.es/cas/Publicaciones/Docs/SaludPublica/PDF-2153-es.pdf (accessed on 12 February 2025).
- Carbajal, Á. Manual de Nutrición y Dietética; Departamento de Nutrición, Facultad de Farmacia, Universidad Complutense de Madrid: Madrid, Spain, 2013. Available online: https://www.ucm.es/nutricioncarbajal/manual-de-nutricion (accessed on 12 February 2025).
- Jolliffe, I.T. Principal Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Massart, D.L.; Kaufman, L. (Eds.) Hierarchical clustering methods. In The Interpretation of Analytical Chemical Data by the Use of Cluster Analysis; Wiley: New York, NY, USA, 1983; pp. 75–101. [Google Scholar]
- Deming, S.N.; Michotte, Y.; Massart, D.L.; Kaufman, L.; Vandeginste, B.G.M. Chemometrics: A Textbook; Elsevier: Amsterdam, The Netherlands, 1988. [Google Scholar]
- Fay, M.P.; Proschan, M.A. Wilcoxon–Mann–Whitney or t-test? On assumptions for hypothesis tests and multiple interpretations of decision rules. Stat. Surv. 2010, 4, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Dodge, Y. Kruskal-Wallis Test. In The Concise Encyclopedia of Statistics; Springer: New York, NY, USA, 2008. [Google Scholar] [CrossRef]
- Abdi, H.; Williams, L.J. Tukey’s Honestly Significant Difference (HSD) Test. In Encyclopedia of Research Design; Salkind, N.J., Ed.; SAGE Publications: Thousand Oaks, CA, USA, 2010. [Google Scholar]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Barrea, L.; Verde, L.; Suárez, R.; Frias-Toral, E.; Vásquez, C.A.; Colao, A.; Savastano, S.; Muscogiuri, G. Sex-differences in Mediterranean diet: A key piece to explain sex-related cardiovascular risk in obesity? A cross-sectional study. J. Transl. Med. 2024, 22, 44. [Google Scholar] [CrossRef] [PubMed]
- Chambers, S.; Lobb, A.; Butler, L.T.; Traill, W.B. The influence of age and gender on food choice: A focus group exploration. Int. J. Consum. Stud. 2008, 32, 356–365. [Google Scholar] [CrossRef]
- Morrison, K.T.; Nelson, T.A.; Ostry, A.S. Mapping spatial variation in food consumption. Appl. Geogr. 2011, 31, 1262–1267. [Google Scholar] [CrossRef]
- Prättälä, R.; Paalanen, L.; Grinberga, D.; Helasoja, V.; Kasmel, A.; Petkeviciene, J. Gender differences in the consumption of meat, fruit and vegetables are similar in Finland and the Baltic countries. Eur. J. Public Health 2007, 17, 520–525. [Google Scholar] [CrossRef] [PubMed]
- Wardle, J.; Haase, A.M.; Steptoe, A.; Nillapun, M.; Jonwutiwes, K.; Bellisie, F. Gender differences in food choice: The contribution of health beliefs and dieting. Ann. Behav. Med. 2004, 27, 107–116. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Sánchez-Villegas, A.; De la Fuente, C.; De Irala, J.; Martínez, J.; Martínez-González, M.A. Olive oil consumption and weight change: The SUN prospective cohort study. Lipids 2006, 41, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Parekh, N.; Martinez-Steele, E.; Monteiro, C.A.; Chang, V.W. Ultra-processed food consumption among US adults from 2001 to 2018. Am. J. Clin. Nutr. 2022, 115, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Dicken, S.; Qamar, S.; Batterham, R.L. Who consumes ultra-processed food? A systematic review of sociodemographic determinants of ultra-processed food consumption from nationally representative samples. Nutr. Res. Rev. 2024, 37, 416–445. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Status Report on Alcohol Consumption, Harm and Policy Responses in 30 European Countries 2019; WHO Regional Office for Europe: Copenhagen, Denmark, 2019; Available online: https://iris.who.int/bitstream/handle/10665/346060/WHO-EURO-2019-3544-43303-60695-eng.pdf?sequence=3 (accessed on 5 July 2025).
- Kritz-Silverstein, D.; Bettencourt, R. Egg consumption: Trends over 48 years, patterns across the lifespan, and predictors of intake. Nutrients 2025, 17, 533. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.D.; Miller, P.E.; Vargas, A.J.; Weed, D.L.; Cohen, S.S. Meta-analysis of egg consumption and risk of coronary heart disease and stroke. J. Am. Coll. Nutr. 2016, 35, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Partearroyo, T.; Samaniego-Vaesken, M.D.L.; Ruiz, E.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Current food consumption amongst the Spanish ANIBES study population. Nutrients 2019, 11, 2663. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.L. Rising consumption of meat and milk in developing countries has created a new food revolution. J. Nutr. 2003, 133 (Suppl. S2), 3907S–3910S. [Google Scholar] [CrossRef] [PubMed]
- Cantillo, J.; Martín, J.C.; Román, C. Analysis of the main determinants of away-from-home consumption of fishery and aquaculture products in the EU28. Appetite 2021, 163, 105216. [Google Scholar] [CrossRef] [PubMed]
- Bergen, N.; Labonté, R. “Everything is perfect, and we have no problems”: Detecting and limiting social desirability bias in qualitative research. Qual. Health Res. 2020, 30, 783–792. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Category | OADCV g/Person/Day [25] | GCP-2022 g/Person/Day This Work | p |
|---|---|---|---|
| Fruit | 1024 | 372.94 ± 347.67 | *** |
| Vegetables | 633 | 538.64 ± 356.33 | *** |
| Legumes | 29.3 | 28.63 ± 38.87 | ns |
| Grains | 291 | 126.94 ± 76.32 | *** |
| Nuts | 33 | 20.78 ± 28.86 | *** |
| Dairy | 419 | 368.94 ± 227.20 | *** |
| Eggs | 23.7 | 30.76 ± 32.94 | *** |
| Meat | 91.9 | 107.52 ± 107.20 | ** |
| Seafood | 195.7 | 82.98 ± 85.82 | *** |
| Processed food | 0.00 | 66.03 ± 85.58 | *** |
| Sweets | 11.7 | 47.48 ± 81.51 | *** |
| Oil/fats | 29.9 | 15.41 ± 14.48 | *** |
| No | Item | Yes | No |
|---|---|---|---|
| 1 | More than 3 servings/week of fish and/or seafood | 1 | 0 |
| 2 | More than or equal to 2 servings/day of vegetables and greens | 1 | 0 |
| 3 | Daily or almost daily potatoes | 1 | 0 |
| 4 | More than or equal to 3 servings/day of fruit | 1 | 0 |
| 5 | More than or equal to 2 servings/week of pulses | 1 | 0 |
| 6 | Daily fresh bread | 1 | 0 |
| 7 | More than or equal to 4 servings/week of nuts | 1 | 0 |
| 8 | Daily milk and dairy products | 1 | 0 |
| 9 | More than 4 servings/week of meat | 1 | 0 |
| 10 | Olive oil used as the main cooking fat | 1 | 0 |
| 11 | 1 (woman) or 2 (man) glasses of wine/day | 1 | 0 |
| 12 | Use of simple culinary techniques (boiling, stewing and/or grilling) | 1 | 0 |
| 13 | Fresh local and seasonal products | 1 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rivas-Fernández, I.; Roade-Pérez, P.; López-Alonso, M.; Pereira-Lestayo, V.; Monte-Secades, R.; Argüeso-Armesto, R.; Herrero-Latorre, C. Observance of the Atlantic Diet in a Healthy Population from Galicia (NW Spain): A Comparative Study Using a New Scale-Based Procedure to Assess Adherence. Foods 2025, 14, 2614. https://doi.org/10.3390/foods14152614
Rivas-Fernández I, Roade-Pérez P, López-Alonso M, Pereira-Lestayo V, Monte-Secades R, Argüeso-Armesto R, Herrero-Latorre C. Observance of the Atlantic Diet in a Healthy Population from Galicia (NW Spain): A Comparative Study Using a New Scale-Based Procedure to Assess Adherence. Foods. 2025; 14(15):2614. https://doi.org/10.3390/foods14152614
Chicago/Turabian StyleRivas-Fernández, Inés, Paula Roade-Pérez, Marta López-Alonso, Víctor Pereira-Lestayo, Rafael Monte-Secades, Rosa Argüeso-Armesto, and Carlos Herrero-Latorre. 2025. "Observance of the Atlantic Diet in a Healthy Population from Galicia (NW Spain): A Comparative Study Using a New Scale-Based Procedure to Assess Adherence" Foods 14, no. 15: 2614. https://doi.org/10.3390/foods14152614
APA StyleRivas-Fernández, I., Roade-Pérez, P., López-Alonso, M., Pereira-Lestayo, V., Monte-Secades, R., Argüeso-Armesto, R., & Herrero-Latorre, C. (2025). Observance of the Atlantic Diet in a Healthy Population from Galicia (NW Spain): A Comparative Study Using a New Scale-Based Procedure to Assess Adherence. Foods, 14(15), 2614. https://doi.org/10.3390/foods14152614