1. Introduction
Myxomatous mitral valve disease (MMVD) is a chronic disease that affects between 30% and 70% of the canine population over 10 years of age, and is the most prevalent heart disease in the species [
1]. In the early stages, MMVD can behave as a benign disease throughout the life of the animal [
2]. However, progressive valvular degeneration leads to worsening volume overload that promotes sympathetic tone and activates the renin–angiotensin–aldosterone system over time [
3]. In addition, tissue fibrosis occurs, possibly promoting the formation of substrates for arrhythmia development [
4]. P wave dispersion is an electrocardiographic measurement of the duration of atrial depolarization (P wave) in multiple leads [
5]. This is an important marker of atrial remodeling and a predictor of atrial fibrillation, and it involves measuring the P wave at its longest and shortest duration. In humans, P wave dispersion reflects failures in the homogeneity of sinus impulse propagation in the atria, as well as prolonged interatrial and intra-atrial conduction; characteristics that are present in patients with supraventricular arrhythmias [
6].
While P wave dispersion refers to the electrophysiological properties of atrial tissue [
5], QT interval dispersion is a marker of homogeneity in ventricular repolarization [
7]. In humans, greater QT interval dispersion is associated with a greater predisposition to sudden death, the development of severe ventricular arrhythmias, hypertrophic cardiomyopathy, long QT syndrome, myocardial infarction, and congestive heart failure (CHF) [
7]. In turn, QT interval instability is a marker for predicting ventricular repolarization instability. It predicts long QT syndrome and Torsades de Pointes [
8]. To measure QT interval instability, a sequence of consecutive beats is chosen, and QT intervals are measured. Then, a center of gravity and a rotated center of gravity are calculated. The distance to the X coordinate represents the long-term instability (length of the plot), and the distance to the Y coordinate represents the short-term instability (width of the plot). Both short-term instability (STI) and long-term instability (LTI) medians are calculated. The median of the distances of all points to the center of gravity is the total instability [
8].
Heart rate variability (HRV) corresponds to differences between ventricular depolarization intervals and can be measured using an electrocardiogram [
9]. Increases in sympathetic tone increase the heart rate, whereas an increase in parasympathetic tone causes it to slow down. Thus, analyzing HRV in dogs allows us to assess the autonomic nervous system state, as described in human medicine [
10]; this factor is reduced in heart disease and heart failure as a reflection of the increased sympathetic tone and decreased parasympathetic tone [
11].
HRV assessment in dogs is possible through analysis in the time and frequency domains, as described in human medicine. Time domain analyses are measured using intervals derived from depolarizations that obtain normal-to-normal depolarization intervals (NNs), from which measurements are performed. Frequency domain analysis uses spectral analysis and Fourier transformation, transforming time domain information into the frequency domain [
12]. In time domains, the SDNN (standard deviation of RR intervals) is the most commonly used parameter for assessing HRV [
12] and represents the activity of the autonomic nervous system, reflecting sympathetic and parasympathetic modulation. Other parameters include rMSSD (square root of the mean square of differences between consecutive RRs) and pNN50 (the division of NN50, the number of differences in consecutive RR intervals longer than 50 milliseconds, by the number of RR intervals) reflecting parasympathetic activity [
12,
13].
In frequency domain components, high frequency (HF) is a marker of parasympathetic tone. In dogs, low frequency (LF) can be considered sympathetic activity and/or a set of sympathetic and vagal activities [
14], in addition to baroreflex sensitivity [
12], as described in humans. Therefore, the ratio between LF/HF represents the relationship between baroreflex sensitivity and parasympathetic modulation [
12].
Because changes in myocardial structure and HRV reduction in dogs with MMVD predispose them to arrhythmias, the present study aims to compare the associated markers of P-wave and QT interval dispersion, QT interval instability, and HRV analyses in asymptomatic MMVD dogs with and without cardiac remodeling that requires treatment (stages B2 and B1, respectively). We will thus assess whether structural cardiac alterations, in the absence of heart failure, predispose dogs to arrhythmias, conduction disturbances, and increased sympathetic stimulation, as previously documented by other authors in dogs with CHF [
11,
15].
Although some studies have already presented useful data about HRV analysis [
11] and QT instability [
15] in dogs with MMVD, to the best of our knowledge, ours is the first to include HRV analysis, P wave and QT wave dispersion, and QT instability in evaluating dogs with MMVD.
2. Materials and Methods
This study was conducted according to animal welfare standards after protocol approval from the Ethics Committee on the Use of Animals—CEUA (protocol 0165/2021).
This study was conducted retrospectively with data obtained from medical records. Dogs were classified according to the criteria described in guidelines published by the American College of Veterinary Internal Medicine (ACVIM) in 2019 [
16] (echocardiographic changes compatible with MMVD, systolic murmur in the mitral focus of grade ≥III/VI, a left atrium/aorta ratio of ≥1.6, and a normalized left ventricle diastolic diameter of ≥1.7) [
16]. Both groups included dogs submitted to anamnesis, clinical examination, echocardiographic, and electrocardiographic exams; the latter being reanalyzed by a single evaluator to maintain standardization. This evaluator is a veterinarian, a member of the postgraduate program in Veterinary Medicine in the Cardiology Department (a veterinary with a residency in Small Animall Medicine and two years of experience in electrocardiography). Regarding drug administration, none of the enrolled dogs underwent cardiovascular therapy for MMVD treatment during the electrocardiographic analysis. In the case of stage B1 dogs, this was because no medical therapy is recommended at this stage [
16]. In the case of stage B2 dogs, this was because electrocardiographic data were acquired at the first presentation, before pimobendan was prescribed [
16]. Exclusion criteria were as follows: dogs with MMVD in stages other than B1 and B2; dogs with cardiac diseases other than MMVD; dogs with clinically relevant systemic diseases (e.g., infectious diseases, presence of moderate-to-severe azotemia, i.e., a serum creatinine level of >2.8, according to International Renal Interest Society classification [
17]); and dogs receiving vasoactive drugs and/or sedatives at the time of data collection.
Computerized electrocardiographic exams were recorded in 3 min. The exam was performed in unsedated dogs positioned and restrained in right lateral recumbency, following the technique described by Tilley in 1992 [
18]. The electrodes were attached to the humerus–radius–ulna and femur–tibia–patella joints, and damped in alcohol 70% solution. The bipolar (DI, DII, and DIII) and unipolar (aVR, aVL, and aVF) leads were recorded and processed by TEB ECG-PC VET® software. Standard electrocardiography measurements (P wave duration and amplitude, PR interval duration, QRS duration and amplitude, QT interval duration, T wave amplitude and RR intervals) were measured in a single beat and analyzed according to Santilli et al. [
19].
Data collected via short-term electrocardiogram for HRV analysis were processed in the Kubios HRV Standard software (Kubios HRV 3.1, Kubios, Kuopio, Finland). After processing, analyses were performed in the time and frequency domains (SDNN, rMSSD, pNN50, LF, HF, LF/HF ratio), and the mean indices of the RR intervals (mean RR) and heart rate (mean HR) were obtained [
20]. For each animal, the P wave and QT interval durations were obtained in 6 leads (D1, D2, D3, aVR, aVL, and aVF) and then the maximum and minimum durations among these values were obtained. The dispersion was calculated using the formula d = max-min (Pd = Pmax-Pmin and QTd = QTmax − QTmin) [
21]. QT measurements were corrected (QTC) with TEB ECG-PC VET
® using Bazzet’s formula: QTC = QT/√RR. From the previous measurements, the centers of gravity and rotated centers of gravity were calculated, and in sequence, the QT mean (QTa), QT variance (QTv), total instability (TI), long-term instability (LTI), and short-term instability (STI) were determined according to the literature (2005) [
8].
HRV was measured by manually counting RR intervals (in milliseconds) in lead D2 in 3 min using a TEB ECG-PC VET® device. These measurements were later tabulated in Microsoft Excel and transferred to Kubios. The data were processed using this software, providing tachograms, scatter plots, and frequency graphics for analysis and SDNN, rMSSD, pNN50, LF, HF, and LF/HF indices.
The Shapiro–Wilk test evaluated the assumption of normality in the distribution of variables in the groups of dogs with stage B1 or stage B2 MMVD. The t-test for independent samples determined the variables in which the assumption of normality was met in the comparison between groups B1 and B2. The nonparametric Mann–Whitney test was used for variables in which the assumption of normality was not met. A p-value of less than 0.05 indicated a statistical difference between the groups.
Because this study aims to evaluate the arrhythmogenic profile of B-stage dogs, all of the arrhythmic events observed during the monitorization in both groups were described.
3. Results
The study population comprised 60 animals of both sexes (63.3% females and 36.7% males in group B1; and 43.3% females and 56.7% males in group B2). This comprised 26 mixed-breed dogs, 7 Poodles, 6 Dachshunds, 4 Lhasa Apsos, 4 Yorkshire Terriers, 3 Miniature Pinschers, 2 Maltese, 2 Shih Tzus, 2 Schnauzers, 1 Australian Cattle Dog, 1 Basset Hound, 1 Jack Russel Terrier, and 1 Labrador Retriever. Ages ranging from 1.8 to 17 were evaluated; and 30 dogs in stage B1, and 30 in stage B2 were selected. There was no statistically significant difference between the ages of the groups listed in
Table 1.
When we consider standard electrocardiography measurements from a single beat [
20] and the HR measured on the TEB ECG-PC VET® device, only the QRS amplitude in mV showed a statistical significance between groups (
Table 2 and
Table 3), showing higher values in group B2.
The base rhythm was sinus arrhythmia in most patients (25 dogs in group B1 and 24 dogs in group B2), with sinus rhythm occurring in 5 dogs from group B1 and 6 from group B2. Six dogs from group B1 and seven dogs from group B2 had sinus arrests; two dogs from group B1 had ventricular premature complexes; one dog from group B1 and five from group B2 had supraventricular premature complexes; and one dog from group B1 had a right bundle branch block and two dogs from group B2 had interatrial and/or intra-atrial blocks [
19].
The means of the maximum and minimum P wave duration (Pmax and Pmin) and P wave dispersion (Pd) measurements were higher in group B2 than B1; however, a statistically significant difference (
p < 0.05) was observed only in the parameters of minimum and maximum P wave duration (Pmin and Pmax). No significant differences were found between QT interval dispersion parameters. Regarding QT dispersion measurements, although group B2 presented higher QTmax and QTmin means, statistically, there was no significant difference between the groups in
Table 4.
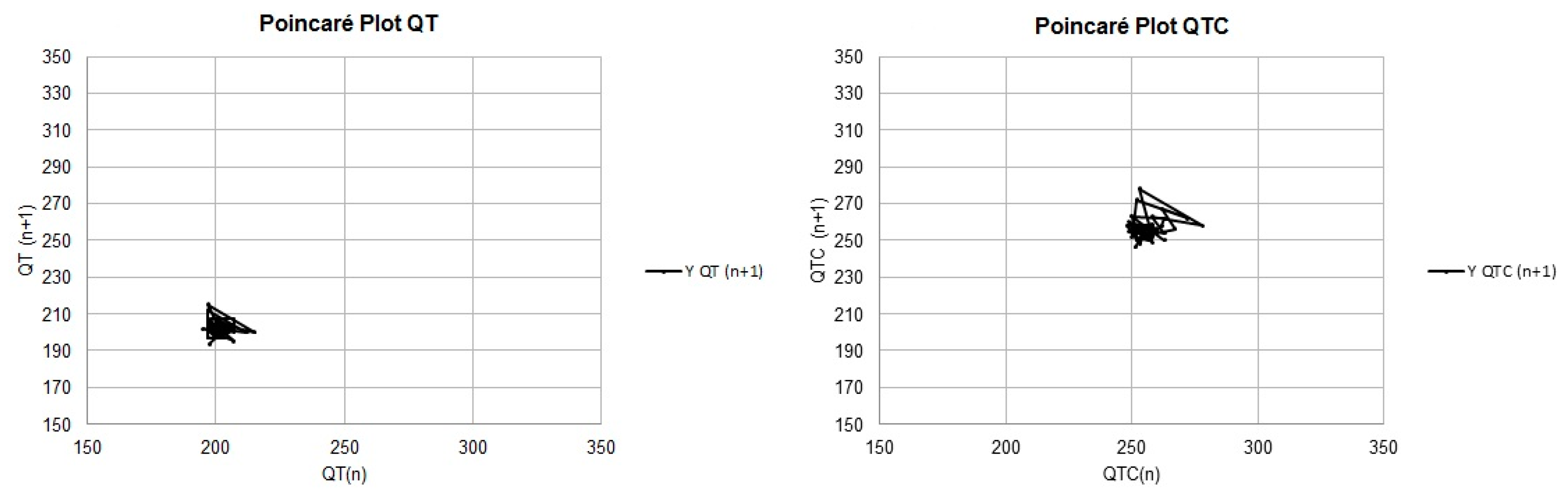
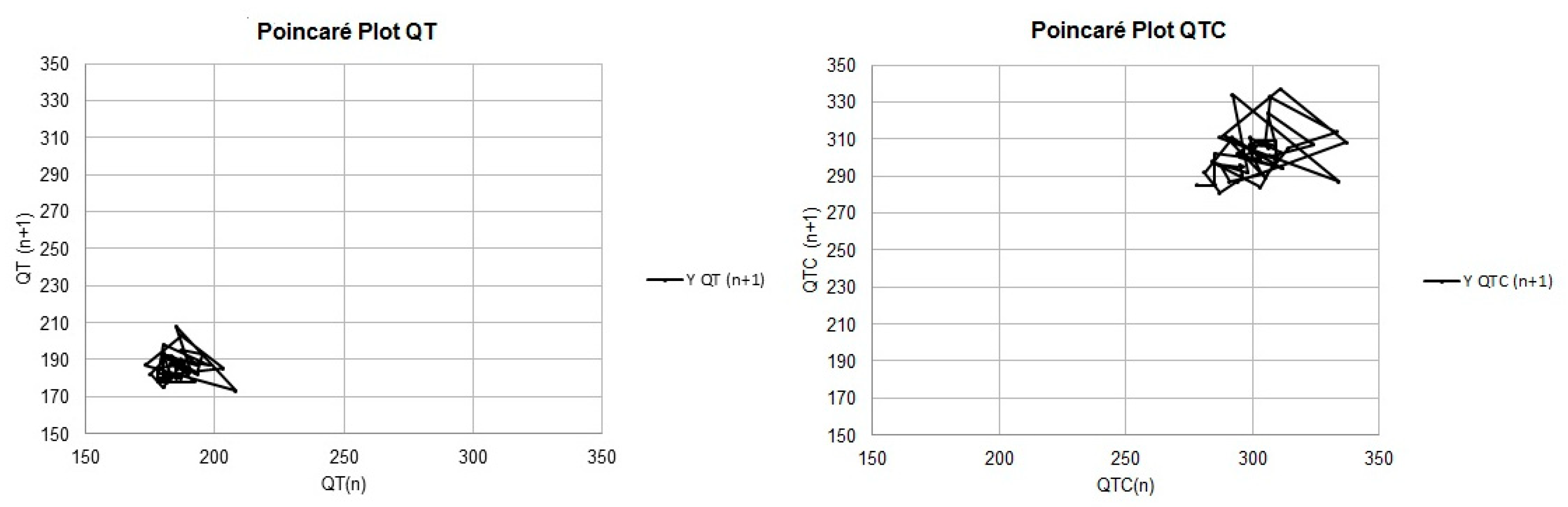
Except for the mean and median of the LTI values calculated with the uncorrected QT values, all the means and medians of the measurements related to the QT instability parameters were higher in group B2 than in group B1. However, a statistically significant difference (
p < 0.05) was observed only in the STI parameters performed with uncorrected QT measurements, as depicted in
Figure 1 and
Figure 2, and
Table 5.
Regarding HRV parameters, the RR interval means and medians were higher in group B1 than in group B2. As the intervals between beats increase, the heart rate (HR) value decreases; thus, group B1 had a lower HR than group B2. Despite some mild discrepancies in the means and medians, it was not possible to observe any statistically significant difference related to HRV parameters (
p < 0.05) (
Table 6).
4. Discussion
Although the electrocardiographic P wave duration values evaluated in lead D2 showed no significant difference between the groups, the Pmax and Pmin values used to calculate the P wave dispersion were higher in group B2 than B1 (
p = 0.0140 and 0.0256, respectively), possibly because of the greater left atrial overload faced by group B2. However, in isolation, P wave duration is a limited parameter for evaluating atrial enlargement [
22].
Regarding the QT interval, there was no significant difference between the dispersion indices; however, in the instability parameters, it was possible to observe an increase in STI in B2 patients compared with B1 patients (
p = 0.0473). In the Poincaré plot for instability analysis, the STI is demonstrated by width measurements, the LTI is demonstrated by length measurements, and the TI is related to both measurements. The QT interval instability index is a mathematical model that measures variation in this interval with each heartbeat; this is related to aspects of Poincaré graphs, which dynamically depict the behavior of intervals at each beat. In this type of chart, width is a measure of short-term instability (STI), length is a measure of long-term instability (LTI), and a measure called total instability (TI) depends on both [
23].
Therefore, the increase in STI shows that cardiac remodeling interferes, albeit subtly, with ventricular electrical activity, providing us with information about the onset of instability changes in all parameters, in stage C of this disease. These findings corroborate the literature when compared with a recent study (2018) that evaluated QT interval instability in MMVD patients, showing a progressive increase in the indices as the disease progressed [
15]. Therefore, the QT interval instability index can quantify variation in the cardiac repolarization time, which predisposes dogs to ventricular arrhythmias [
23].
Regarding the HRV parameters in the present study, it was not possible to prove a significant difference between the groups, although the averages of the SDNN, rMSSD, and pNN50 parameters were slightly higher in group B1, and there was a higher HF average and lower LF/HF ratio in the same group. The HRV analysis values for both groups were similar to those observed by Martinello et al. (2022) in healthy animals of similar ages [
20]. This allows us to infer that, alone, cardiac remodeling in MMVD cannot change the sympathetic–parasympathetic balance in dogs without CHF. The same can be observed in analyses of dogs with CHF secondary to MMVD, such as in the study by Oliveira et al. (2012), which observed a reduction in SDANN and pNN50 parameters in a group of animals in stage C [
11].
These findings suggest that the changes in sympathetic tone detected in patients with CHF are not present in the initial stages of cardiac remodeling. In another recent study, a reduction in HRV parameters was observed in the time domains, in relation to stages C and B but without differences between two animals labeled B1 and B2. However, in the same study, the frequency domain analysis showed a difference between animals B1 and B2, showing a reduction in the HF vagal component and an increase in the LF/HF ratio in B2 in relation to B1 [
24].
Some of the limitations of this study included the difficulty of standardizing information previously obtained about the animals, as the animals were not clinically evaluated or examined by the same veterinarians. Additionally, considering that some of the animals first presented at the Cardiology Service, it was difficult to obtain a complete medical history of comorbidities from the veterinarian’s reports. Because the present study used information previously obtained from patients without sedation, some exams presented many artifacts, making it difficult to measure a series of consecutive parameters. Additionally, most of the animals were not familiar with the hospital environment, a factor that can generate stress and, therefore, changes in physiological parameters.
Another limitation regarding the retrospective nature of this study is that only a few patients had fully cardiologic standardized evaluations that were sufficient to fulfill the inclusion criteria; for that reason, only a few were included. This is also why creating a control group and an analysis of larger ECG tracings (i.e., 24-h Holter monitorization) were not possible, as healthy patients usually do not undergo a complete cardiologic standardized evaluation.
Another limitation is that the electrocardiographic tracings were reviewed by one examiner, leading to a lack of inter-observer analysis. The lack of statistics for the echocardiographic exams is also a limitation.
Due to the fact that this study focused on more specific analysis, some standard ECG parameters were not statistically evaluated, such as the mean electrical axes of P wave, the ST segment amplitude, the T wave duration and mean electrical axes of the QRS complex.
Lastly, regarding stage B2 patients, it is possible to observe a wide range of phenotypes, ranging from dogs with signs of cardiac remodeling to dogs about to present congestive heart failure (the latter are patients evolving to stage C). The different sizes of cardiac chambers, as well as the different hemodynamic statuses, make B2 patients a group where electrophysiological changes may manifest in different ways as the disease progresses. Therefore, to precisely determine when alterations begin, further studies are needed to subclassify the B2 group and correlate electrophysiological changes to the severity of the disease.


 ,
, 

{kind=link}
{kind=link}