Multiple Undifferentiated Pleomorphic Sarcoma (Malignant Fibrous Histiocytoma) with Extradural Involvement in a 7-Year-Old Labrador Retriever

 , , ,
, , ,  and
and
Abstract
:1. Introduction
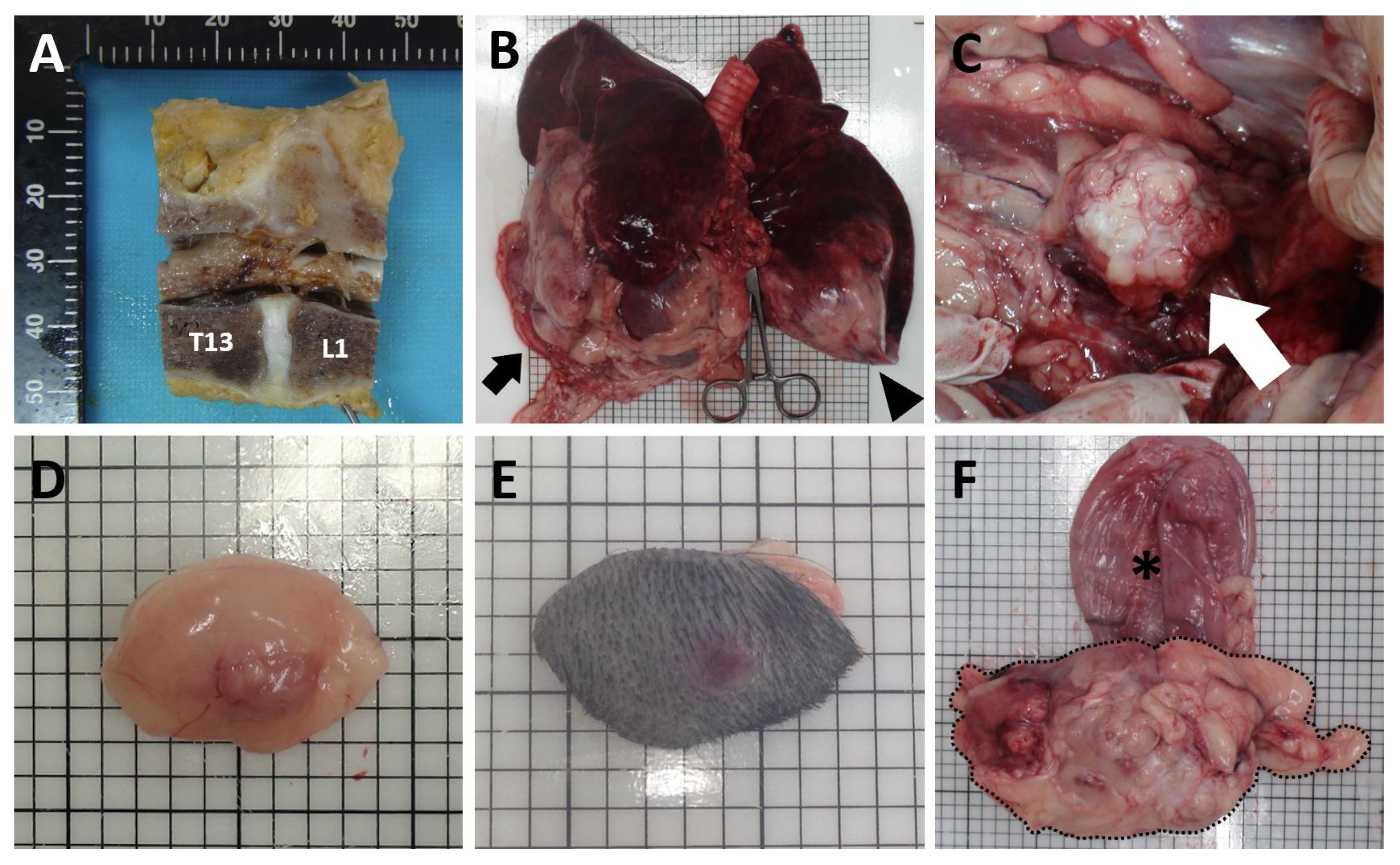
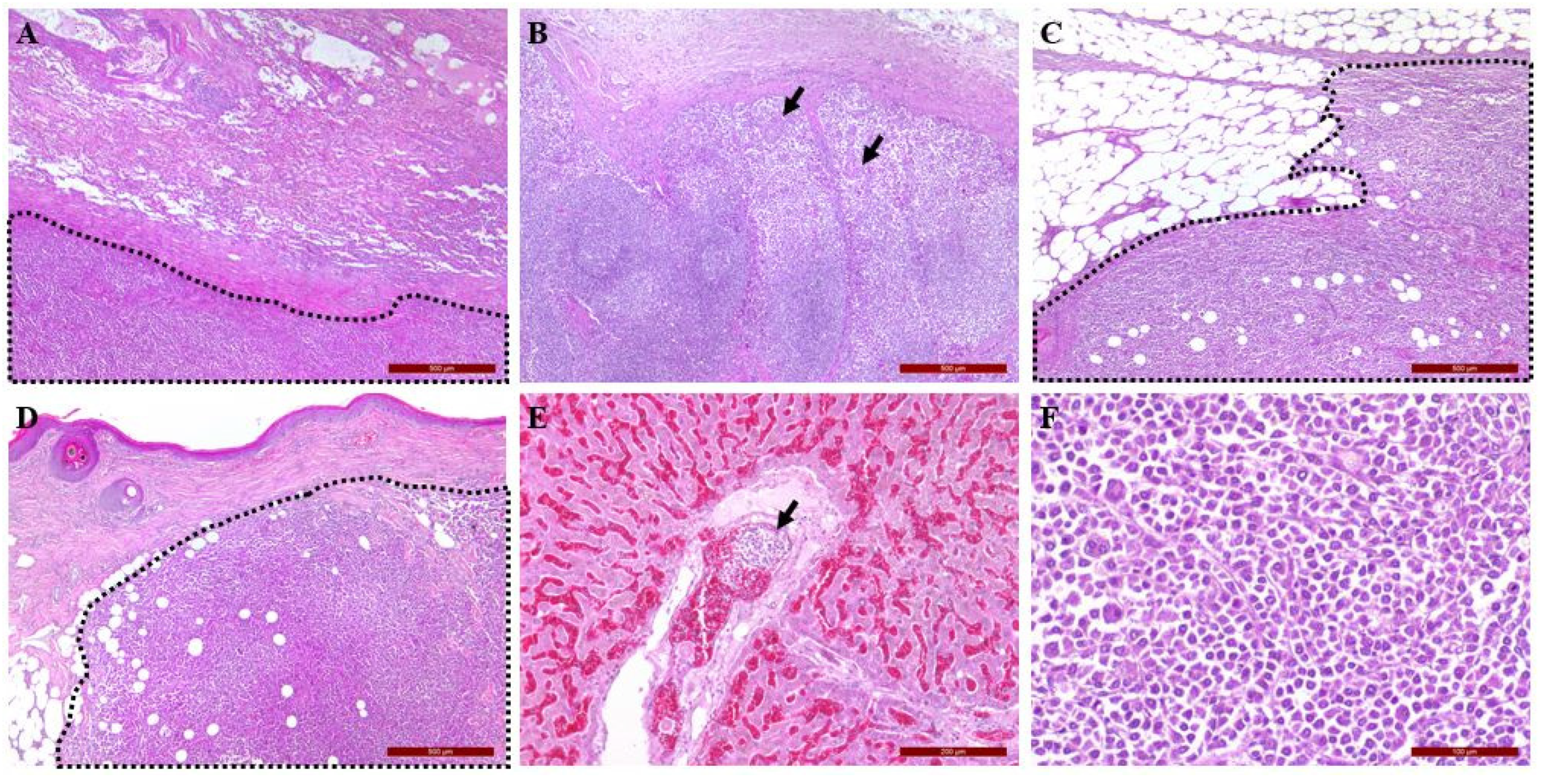
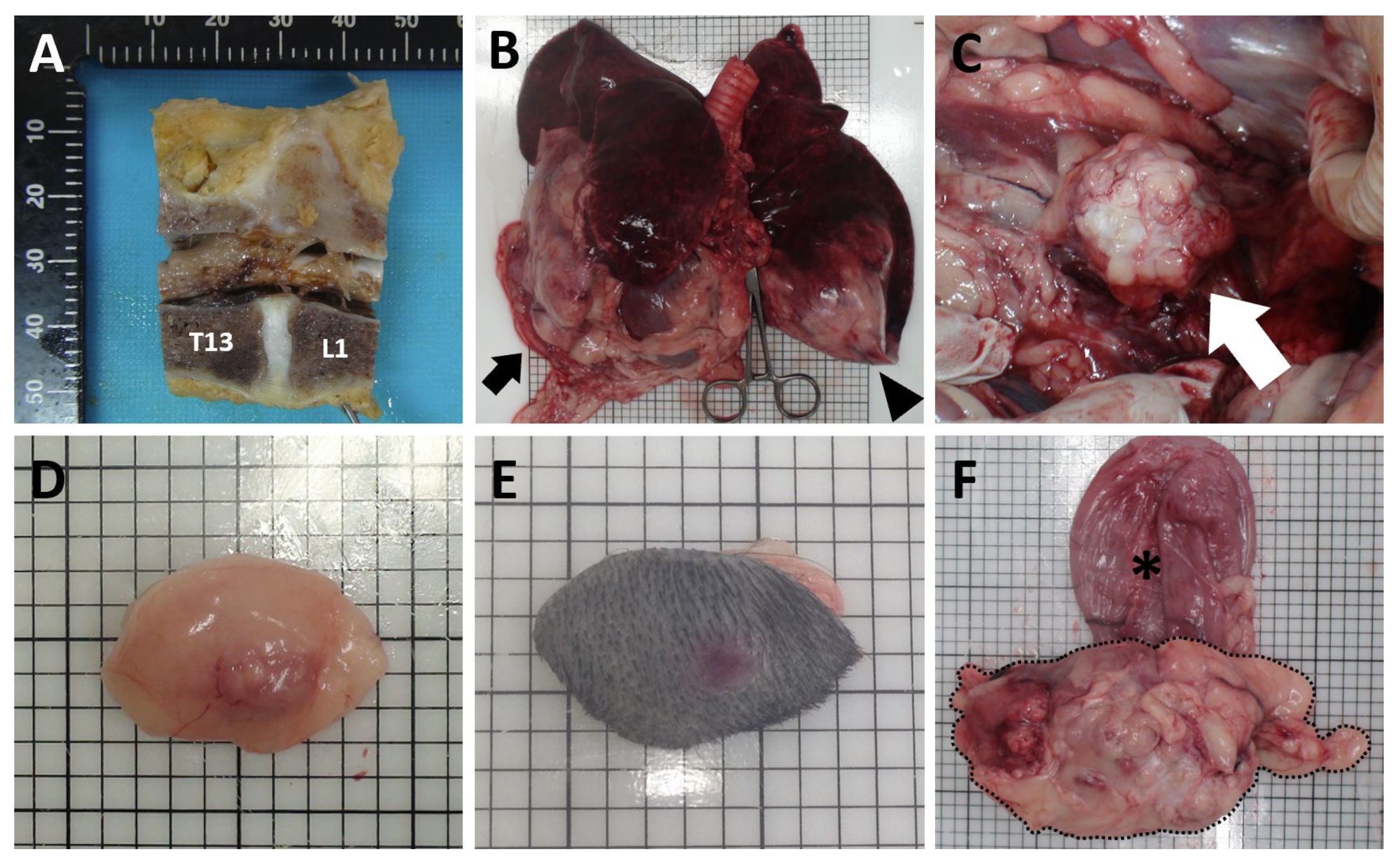
2. Clinical Description
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Agha, O.M.; Igbokwe, A.A. Malignant fibrous histiocytoma: Between the past and the present. Arch. Patho. Lab. Med. 2008, 132, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Kwon, Y.; Chang, J.; Jeong, S.; Lee, H.; Kim, J.; Jung, J.; Lee, Y. Undifferentiated pleomorphic sarcoma (Malignant Fibrous Histiocytoma) of Head in a Dog. J. Vet. Med. Sci. 2011, 73, 235–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huyghe, S.; Combes, A.; Vercauteren, G.; De Rooster, H. Undifferentiated pleomorphic sarcoma in a six-month-old Cocker Spaniel: A case report. Wien. Tierarztl. Monatsschr. 2014, 101, 3–10. [Google Scholar]
- Withrow, S.J.; Vail, D.M.; Page, R.L. Small Animal Clinical Oncology, 5th ed.; WB Saunders: Philadelphia, PA, USA, 2013; pp. 356–380. [Google Scholar]
- Hendrick, M.J.; Brooks, J.J.; Bruce, E.H. Six cases of malignant fibrous histiocytoma of the canine spleen. Vet. Pathol. 1992, 29, 351–354. [Google Scholar] [CrossRef]
- Schmidt, M.L.; Rutteman, G.R.; van Niel, M.H.; Wolvekamp, P.T. Clinical and radiographic manifestations of canine malignant histiocytosis. Vet. Q. 1993, 15, 117–120. [Google Scholar] [CrossRef]
- Fulmer, A.; Mauldin, G. Canine histiocytic neoplasia: An overview. Can. Vet. J. 2007, 48, 1041–1050. [Google Scholar]
- Liegl-Atzwanger, B.; Hofmann, G.; Leithner, A.; Beham, A. Undifferentiated high-grade pleomorphic sarcoma (UHPS): Diagnostic criteria, differential diagnosis, and treatment. An attempt to erasure the misnomer “MFH”. Eur. Surg. 2009, 41, 143–149. [Google Scholar] [CrossRef]
- Matushansky, I.; Siddiqi, S.; Hricik, T. MFH classification: Differentiating undifferentiated pleomorphic sarcoma in the 21st Century. Expert Rev. Anticancer Ther. 2009, 9, 1135–1144. [Google Scholar] [CrossRef] [Green Version]
- Gleiser, C.A.; Raulston, G.L.; Jardine, J.H.; Gray, K.N. Malignant fibrous histiocytoma in dogs and cats. Vet. Pathol. 1979, 16, 199–208. [Google Scholar] [CrossRef]
- Seiler, R.J.; Wilkinson, G.T. Malignant fibrous histiocytoma involving the ileum in a cat. Vet. Pathol. 1980, 17, 513–517. [Google Scholar] [CrossRef]
- Renlund, R.; Pritzker, K. Malignant fibrous histiocytoma involving the digit in a cat. Vet. Pathol. 1984, 21, 442–444. [Google Scholar] [CrossRef] [Green Version]
- Tanimoto, T.; Ohtsuki, Y.; Sonobe, H.; Takahashi, R.; Nomura, Y. Malignant fibrous histiocytoma in the spleen of a pig. Vet. Pathol. 1988, 25, 330–332. [Google Scholar] [CrossRef] [Green Version]
- Waters, C.B.; Morrison, W.B.; DeNicola, D.B.; Widmer, W.R.; White, M.R. Giant cell variant of malignant fibrous histiocytoma in dogs: 10 cases (1986–1993). J. Am. Vet. Med. Assoc. 1994, 205, 1420–1424. [Google Scholar]
- Sartin, E.A.; Hudson, J.A.; Herrera, G.A.; Dickson, A.M.; Wolfe, D.E. Invasive malignant fibrous histiocytoma in a cow. J. Am. Vet. Med. Assoc. 1996, 208, 1709–1710. [Google Scholar] [PubMed]
- Kiran, M.M.; Karaman, M.; Hatipoglu, F.; Koc, Y. Malignant fibrous histiocytoma in a dog: A case report. Vet. Med. 2005, 50, 553–557. [Google Scholar] [CrossRef] [Green Version]
- Ko, J.S.; Kim, H.J.; Choi, Y.M.; Kim, J.W.; Park, C.; Do, S.H. Diagnostic approach to malignant fibrous histiocytomas of soft tissue in dogs: A case report. Vet. Med. 2013, 58, 621–627. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.H.; Kim, H.J.; Lee, S.J.; Yoon, H.Y. Splenic malignant fibrous histiocytoma with concurrent hypertension and epistaxis in an Alaskan malamute dog. BMC Vet. Res. 2018, 14, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Teddy, P.J.; Esiri, M.M. Malignant fibrous histiocytoma producing spinal cord compression. J. Neurol. Neurosurg. Psychiatry 1979, 42, 838–842. [Google Scholar] [CrossRef]
- Bidwell, J.K.; Young, J.W.R.; Saylor, L. Malignant fibrous histiocytoma of the spine: Computed tomography appearance and review of the literature. J. Comput. Tomogr. 1987, 11, 355–358. [Google Scholar] [CrossRef]
- Van Biervliet, J.; Alcaraz, A.; Jackson, C.A.; Njaa, B.; De Lahunta, A.; Divers, T.J. Extradural undifferentiated sarcoma causing spinal cord compression in 2 horses. J. Vet. Intern. Med. 2004, 18, 248–251. [Google Scholar] [CrossRef]
- Morris, J.S.; McInnes, E.F.; Bostock, D.E.; Hoather, T.M.; Dobson, J.M. Immunohistochemical and histopathologic features of 14 malignant fibrous histiocytomas from Flat-Coated Retrievers. Vet. Pathol. 2002, 39, 473–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loblaw, D.A.; Mitera, G.; Ford, M.; Laperriere, N.J. A 2011 updated systematic review and clinical practice guideline for the management of malignant extradural spinal cord compression. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 312–317. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Postural Reaction | |||
|---|---|---|---|
| Left | Right | ||
| Paw position | Front | 2 | 2 |
| Rear | 1 | 1 | |
| Hopping | Front | 2 | 2 |
| Rear | 1 | 1 | |
| Hemistanding and Hemiwalking | Front | 2 | 2 |
| Rear | 1 | 1 | |
| Wheelbarrowing | 2 | 2 | |
| Extensor postural thrust | 1 | 1 | |
| Spinal Reflex | |||
|---|---|---|---|
| Left | Right | ||
| Patella (femoral) | 2 | 2 | |
| Cranial tibial | 1 | 1 | |
| Withdrawal | Front | 2 | 2 |
| Rear | 1 | 2 | |
| Perineal | 2 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, K.; Shin, J.; Kim, H.; Kim, H.; Kim, J.; Do, S.; Kim, H. Multiple Undifferentiated Pleomorphic Sarcoma (Malignant Fibrous Histiocytoma) with Extradural Involvement in a 7-Year-Old Labrador Retriever. Vet. Sci. 2022, 9, 3. https://doi.org/10.3390/vetsci9010003
Kim K, Shin J, Kim H, Kim H, Kim J, Do S, Kim H. Multiple Undifferentiated Pleomorphic Sarcoma (Malignant Fibrous Histiocytoma) with Extradural Involvement in a 7-Year-Old Labrador Retriever. Veterinary Sciences. 2022; 9(1):3. https://doi.org/10.3390/vetsci9010003
Chicago/Turabian StyleKim, Kihoon, Jaiho Shin, Hyosung Kim, Hanjun Kim, Jaehwan Kim, Sunhee Do, and Hwiyool Kim. 2022. "Multiple Undifferentiated Pleomorphic Sarcoma (Malignant Fibrous Histiocytoma) with Extradural Involvement in a 7-Year-Old Labrador Retriever" Veterinary Sciences 9, no. 1: 3. https://doi.org/10.3390/vetsci9010003
APA StyleKim, K., Shin, J., Kim, H., Kim, H., Kim, J., Do, S., & Kim, H. (2022). Multiple Undifferentiated Pleomorphic Sarcoma (Malignant Fibrous Histiocytoma) with Extradural Involvement in a 7-Year-Old Labrador Retriever. Veterinary Sciences, 9(1), 3. https://doi.org/10.3390/vetsci9010003