

Clinical Outcomes after Surgical Aortic Valve Replacement in 681 Octogenarians: A Single-Center Real-World Experience Comparing the Old Patients with the Very Old Patients



Abstract
1. Introduction
2. Materials and Methods
3. Results
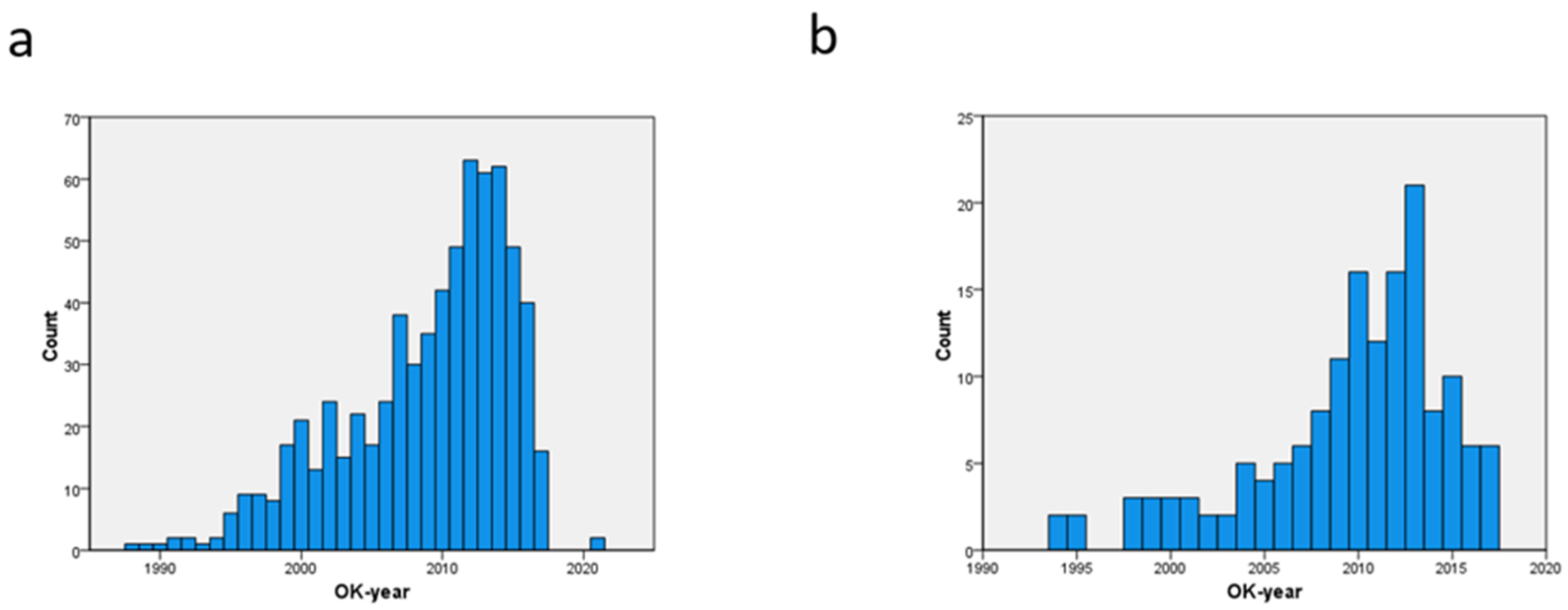
3.1. Temporal Reference Pattern, Preoperative Patient Profile, and Operative Data
3.2. Postoperative Adverse Events and Need for Resources
3.3. Independent Predictors for Short-Term Outcome
3.4. Long-Term Outcome
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Takagi, K.; Arinaga, K.; Takaseya, T.; Otsuka, H.; Shojima, T.; Shintani, Y.; Zaima, Y.; Saku, K.; Oryoji, A.; Hiromatsu, S. Aortic valve replacement with or without concomitant coronary artery bypass grafting in very elderly patients aged 85 years and older. Heart Vessel. 2020, 35, 1409–1418. [Google Scholar] [CrossRef] [PubMed]
- Stewart, S.; Afoakwah, C.; Chan, Y.K.; Strom, J.B.; Playford, D.; Strange, G.A. Counting the cost of premature mortality with progressively worse aortic stenosis in Australia: A clinical cohort study. Lancet Healthy Longev. 2022, 3, e599–e606. [Google Scholar] [CrossRef] [PubMed]
- Ennker, J.; Mortasawi, A.; Gehle, S.; Yaghmaie, M.; Schröder, T.; Rosendahl, U.; Ennker, I.C. Aortic valve replacement with or without concomitant coronary artery bypass grafting in the ninth decade of life. Langenbecks Arch. Surg. 2001, 386, 272–277. [Google Scholar] [CrossRef] [PubMed]
- Iung, B.; Cachier, A.; Baron, G.; Messika-Zeitoun, D.; Delahaye, F.; Tornos, P.; Gohlke-Bärwolf, C.; Boersma, E.; Ravaud, P.; Vahanian, A. Decision-making in elderly patients with severe aortic stenosis: Why are so many denied surgery? Eur. Heart J. 2005, 26, 2714–2720. [Google Scholar] [CrossRef] [PubMed]
- Mistiaen, W.; Van Cauwelaert, P.; Muylaert, P.; Wuyts, F.; Harrisson, F.; Bortier, H. Risk Factors and Survival after Aortic Valve Replacement in Octogenarians. J. Heart Valve Dis. 2004, 13, 538–544. [Google Scholar] [PubMed]
- Dimagli, A.; Sinha, S.; Caputo, M.; Angelini, G.D.; Benedetto, U. Trend in morbidity and mortality in surgical aortic valve replacement: A retrospective, observational, single-centre study. Interact. Cardiovasc. Thorac. Surg. 2020, 31, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Hamm, C.W.; Beyersdorf, F. GARY—The Largest Registry of Aortic Stenosis Treatment Worldwide: The German Aortic Valve Registry [GARY] established in 2010 has been accumulating data for a decade now. Eur. Heart J. 2020, 41, 733–735. [Google Scholar] [CrossRef]
- Czarnecki, A.; Qiu, F.; Koh, M.; Alter, D.A.; Austin, P.C.; Fremes, S.E.; Tu, J.V.; Wijeysundera, H.C.; Yan, A.T.; Ko, D.T. Trends in the incidence and outcomes of patients with aortic stenosis hospitalization. Am. Heart J. 2018, 199, 144–149. [Google Scholar] [CrossRef]
- Neyt, M.; Van Brabandt, H.; Van De Sande, S.; Devriese, S. Transcatheter Aortakunstklep Implantatie (TAVI): Een Health Technology Assessment Actualisatie. Health Technology Assessment (HTA); KCE Reports; Federaal Kenniscentrum voor de Gezondheidszorg (KCE): Brussel, Belgium, 2013. [CrossRef]
- Mistiaen, W.; Van Cauwelaert, P.; Muylaert, P.; De Worm, E. One thousand Carpentier-Edwards pericardial valves in the aortic position: What has changed in the past 20 years, and what are the effects on hospital complications? J. Heart Valve Dis. 2007, 16, 417–422. [Google Scholar] [PubMed]
- Bezzeccheri, A.; Vermeersch, P.; Verheye, S.; Wilgenhof, A.; Willemen, Y.; Vescovo, G.M.; Scott, B.; Convens, C.; Zivelonghi, C.; Agostoni, P. Trends and outcomes in transcatheter aortic valve implantation in Belgium: A 13-year single centre experience. Acta Cardiol. 2020, 77, 960–969. [Google Scholar] [CrossRef] [PubMed]
- Mistiaen, W.; Van Cauwelaert, P.; Muylaert, P.; De Worm, E. A thousand pericardial valves in aortic position: Risk factors for postoperative acute renal function impairment in elderly. J. Cardiovasc. Surg. 2009, 50, 233–237. [Google Scholar]
- Krane, M.; Voss, B.; Hiebinger, A.; Deutsch, M.A.; Wottke, M.; Hapfelmeier, A.; Badiu, C.C.; Bauernschmitt, R.; Lange, R. Twenty years of cardiac surgery in patients aged 80 years and older: Risks and benefits. Ann. Thorac. Surg. 2011, 91, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, T.; Hiroshi, T.; Toda, K.; Sawa, Y. Osaka Cardiovascular Surgery Research Group (OSCAR). Surgical Aortic Valve Replacement in Octogenerians in the Era of Transcatheter Aortic Valve Replacement. Circ. J. 2018, 82, 1592–1597. [Google Scholar] [CrossRef] [PubMed]
- Likosky, D.S.; Sorensen, M.J.; Dacey, L.J.; Baribeau, Y.R.; Leavitt, B.J.; DiScipio, A.W.; Hernandez, F., Jr.; Cochran, R.P.; Quinn, R.; Helm, R.E.; et al. Northern New England Cardiovascular Disease Study Group. Long-term survival of the very elderly undergoing aortic valve surgery. Circulation 2009, 120 (Suppl. 11), S127–S133. [Google Scholar] [CrossRef] [PubMed]
- Caceres, M.; Cheng, W.; De Robertis, M.; Mirocha, J.M.; Czer, L.; Esmailian, F.; Khoynezhad, A.; Ramzy, D.; Kass, R.; Trento, A. Survival and quality of life for nonagenarians after cardiac surgery. Ann. Thor. Surg. 2013, 95, 1598–1602. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.P.; LaPar, D.J.; Crosby, I.K.; Kern, J.A.; Lau, C.L.; Kron, I.L.; Ailawadi, G. Nonagenarians undergoing cardiac surgery. J. Card Surg. 2014, 29, 600–604. [Google Scholar] [CrossRef] [PubMed]
- Elsisy, M.F.; Schaff, H.V.; Crestanell, J.A.; Ajkhouli, M.A.; Stulak, J.M.; Stephens, E.H. Outcomes of cardiac surgery in nonagenarians. J Cardiac. Surg. 2022, 7, 1664–1670. [Google Scholar] [CrossRef]
- Böning, A.; Lutter, G.; Mrowczynski, W.; Attmann, T.; Bödeker, R.H.; Scheibelhut, C.; Cremer, J. Octogenarians undergoing combined aortic valve replacement and myocardial revascularization: Perioperative mortality and medium-term survival. Thorac. Cardiovasc. Surg. 2010, 58, 159–163. [Google Scholar] [CrossRef]
- Kolh, P.; Kerzmann, A.; Honore, C.; Comte, L.; Limet, R. Aortic valve surgery in octogenarians: Predictive factors for operative and long-term results. Eur. J. Cardiothorac. Surg. 2007, 31, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Langanay, T.; Flécher, E.; Fouquet, O.; Ruggieri, V.G.; De La Tour, B.; Félix, C.; Lelong, B.; Verhoye, J.P.; Corbineau, H.; Leguerrier, A. Aortic valve replacement in the elderly: The real life. Ann. Thorac. Surg. 2012, 93, 70–77. [Google Scholar] [CrossRef]
- Malvindi, P.G.; Luthra, S.; Giritharan, S.; Kowalewski, M.; Ohri, S. Long-term survival after surgical aortic valve replacement in patients aged 80 years and over. Eur. J. Cardiothorac. Surg. 2021, 60, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Porterie, J.; Kalavrouziotis, D.; Dumont, E.; Paradis, J.M.; De Larochellière, R.; Rodés-Cabau, J.; Mohammadi, S. Clinical impact of the heart team on the outcomes of surgical aortic valve replacement among octogenarians. J. Thorac. Cardiovasc. Surg. 2021, 11, 1010–1019.E5. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Preop and Operative Factors | >85 y (%) | 80–84 y (%) | p |
|---|---|---|---|
| Preoperative factors | |||
| Congestive heart failure | 75/154 (48.7) | 148/527 (28.0) | 0.001 |
| Need for urgent SAVR | 45/150 (30.0) | 109/515 (21.2) | 0.024 |
| Euroscore II > 8% | 51/124 (41.1) | 113/371 (30.5) | 0.029 |
| Hematological malignancy | 7/131 (5.3) | 9/446 (2.0) | 0.042 |
| BMI > 30 kg/m2 | 17/122 (13.9) | 79/365 (21.6) | 0.064 |
| Conduction defect (all types) | 68/154 (44.2) | 195/526 (37.1) | 0.112 |
| Diabetes mellitus | 36/154 (23.4) | 94/527 (17.8) | 0.121 |
| Coronary artery disease | 98/154 (63.9) | 370/527 (70.2) | 0.122 |
| NYHA III/IV | 94/110 (85.5) | 313/396 (79.0) | 0.134 |
| Arterial hypertension | 108/154 (70.1) | 395/523 (75.5) | 0.178 |
| Prior CABG | 19/154 (12.3) | 46/527 (8.7) | 0.180 |
| Plasma creatinine > 1.3 mg% | 43/154 (27.9) | 130/527 (24.7) | 0.414 |
| Myocardial infarction | 30/154 (19.5) | 89/525 (17.0) | 0.468 |
| Male gender | 79/154 (51.3) | 278/528 (52.7) | 0.567 |
| Complex ventricular arrhythmia | 18/154 (11.7) | 55/527 (10.4) | 0.659 |
| Peripheral artery disease (all) | 57/146 (39.0) | 200/488 (41.9) | 0.675 |
| Atrial fibrillation (all types) | 47/154 (30.5) | 169/527 (32.1) | 0.920 |
| All neurologic ischemic events | 26/154 (16.9) | 83/527 (15.7) | 0.729 |
| Pulmonary artery hypertension | 45/124 (36.3) | 134/387 (34.6) | 0.735 |
| Left ventricular hypertrophy | 127/140 (90.7) | 427/586 (89.9) | 0.781 |
| Left ventricular ejection fraction < 50% | 23/112 (20.5) | 75/375 (20.0) | 0.901 |
| FEV1 < 80% predicted value | 42/146 (28.8) | 147/507 (29.0) | 0.958 |
| Operative factors | |||
| Partial sternotomy | 16/14 (10.8) | 31/511 (6.1) | 0.048 |
| Cross-clamp time > 60 min | 66/112 (54.1) | 248/397 (62.5) | 0.098 |
| Concomitant CABG | 91/154 (59.1) | 349/527 (66.1) | 0.110 |
| Procedure on the ascending aorta | 5/154 (3.2) | 31/527 (5.9) | 0.197 |
| Perceval valve prosthesis® | 10/154 (6.5) | 23/527 (4.4) | 0.277 |
| Incomplete revascularization | 22/149 (14.8) | 66/513 (12.9) | 0.548 |
| Smallest valve size | 5/153 (3.3) | 21/536 (4.0) | 0.681 |
| Mitral valve repair | 7/154 (4.5) | 22/527 (4.2) | 0.839 |
| Cardiopulmonary bypass time > 120 min | 59/123 (42.8) | 198/466 (42.5) | 0.956 |
| Postoperative Events and Resources | >85 y (%) | 80–84 y (%) | p |
|---|---|---|---|
| Need for resources | |||
| Plasma derivatives | 46/121 (38.0) | 100/369 (27.1) | 0.023 |
| Length of stay in intensive care unit > 1 day | 64/137 (46.7) | 163/430 (37.9) | 0.067 |
| Mechanical ventilation > 8 h | 62/124 (50.0) | 156/367 (42.5) | 0.147 |
| Renal replacement therapy | 13/154 (8.4) | 28/526 (5.3) | 0.153 |
| Thrombocyte concentrate | 20/121 (16.5) | 50/369 (13.6) | 0.416 |
| Postoperative length of stay > 8 days | 74/147 (50.3) | 230/494 (46.6) | 0.420 |
| Permanent pacemaker implant | 7/154 (4.5) | 18/527 (3.4) | 0.509 |
| >4 units packed cells | 35/121 (28.9) | 97/369 (26.3) | 0.570 |
| Reintervention | 5/154 (3.2) | 14/528 (2.6) | 0.693 |
| Adverse events | |||
| 30-day mortality | 24/154 (15.6) | 45/527 (8.5) | 0.011 |
| Pulmonary complications | 36/154 (23.4) | 83/527 (15.7) | 0.028 |
| Thromboembolic event | 10/154 (6.5) | 17/527 (3.2) | 0.068 |
| Bleeding event | 18/154 (11.7) | 40/527 (7.6) | 0.109 |
| Low thrombocytes | 16/123 (13.0) | 65/371 (17.5) | 0.371 |
| New or progressing conduction defect | 29/154 (18.8) | 115/627 (21.8) | 0.424 |
| Acute renal injury | 53/154 (34.4) | 164/527 (31.1) | 0.440 |
| Low cardiac output syndrome | 20/153 (13.1) | 60/527 (11.4) | 0.569 |
| Recurrent or new-onset atrial fibrillation | 65/154 (42.2) | 209/527 (39.7) | 0.570 |
| Pneumothorax, prolonged chest drain | 36/154 (23.4) | 114/527 (21.6) | 0.646 |
| Delirium with agitation | 23/143 (16.1) | 84/490 (17.1) | 0.766 |
| Ventricular arrhythmias | 7/154 (4.5) | 23/527 (4.4) | 0.923 |
| Length of stay in days | 4.2 ± 7.0 | 3.6 ± 7.6 | 0.402 |
| Plasma creatinine (mg%) | 1.61 ± 0.97 | 1.70 ± 1.03 | 0.420 |
| Left atrial pressure (cm H2O) | 18.8 ± 4.9 | 18.4 ± 4.8 | 0.553 |
| Mean transvalvular gradient (mm Hg) | 11.6 ± 5.0 | 11.0 ± 5.4 | 0.577 |
| Postoperative length of stay (days) | 11.6 ± 7.5 | 11.4 ± 10.1 | 0.753 |
| Increase in plasma creatinine (mg%) | 0.53 ± 0.80 | 0.51 ± 0.75 | 0.821 |
| Units of packed cells | 3.4 ± 3.5 | 3.3 ± 4.1 | 0.829 |
| Mechanical ventilation duration (hours) | 19.3 ± 46.3 | 18.5 ± 54.0 | 0.863 |
| Peak transvalvular gradient (mm Hg) | 19.1 ± 8.0 | 19.2 ± 9.4 | 0.940 |
| 80 to 84 y | >85 y | |||
|---|---|---|---|---|
| Predictor | OR (95% CI) | p | OR (95% CI) | p |
| Acute renal injury | 5.69 (2.62–12.33) | <0.001 | 6.65 (2.18–19.65) | <0.001 |
| Urgent SAVR | 3.12 (1.49–6.51) | 0.002 | 6.64 (2.27–19.34) | <0.001 |
| Reintervention | 8.01 (2.04–31.46) | 0.003 | - | - |
| Incomplete revasc. | 2.96 (1.25–7.03) | 0.014 | - | - |
| Predictor | Odds Ratio | 95% CI | p |
|---|---|---|---|
| Emergent SAVR | 3.87 | 1.74–8.64 | 0.001 |
| FEV1 > 80% predicted | 2.44 | 1.39–4.26 | 0.002 |
| Atrial fibrillation | 2.30 | 1.30–4.06 | 0.004 |
| Age > 85 y | 2.02 | 1.11–3.66 | 0.021 |
| Preoperative plasma creatinine > 1.3 mg% | 1.94 | 1.09–3.45 | 0.025 |
| Coronary artery disease | 1.99 | 1.01–3.89 | 0.046 |
| Time | 80–84 y | n | <85 y | n | All Patients | n |
|---|---|---|---|---|---|---|
| 1 year | 91.7 ± 1.3% | 444 | 93.1 ± 2.2% | 120 | 92.0 ± 1.1 | 564 |
| 5 years | 67.8 ± 2.1% | 329 | 60.0 ± 4.3% | 78 | 66.4 ± 1.9 | 409 |
| 10 years | 26.2 ± 2.2% | 86 | 13.2 ± 3.4% | 11 | 25.3 ± 2.0% | 97 |
| Predictor | Odds Ratio | 95% CI | p |
|---|---|---|---|
| Preoperative plasma creatinine < 1.3 mg% | 1.40 | 1.11–1.76 | 0.005 |
| Preoperative congestive heart failure | 1.37 | 1.09–1.71 | 0.006 |
| Postoperative low cardiac output syndrome | 1.82 | 1.18–2.83 | 0.007 |
| Postoperative delirium | 1.45 | 1.09–1.92 | 0.010 |
| Postoperative ventricular arrhythmia | 1.84 | 1.13–3.00 | 0.021 |
| Emergent SAVR (<24 h) | 1.69 | 1.08–2.65 | 0.021 |
| Diabetes mellitus | 1.30 | 1.02–1.66 | 0.032 |
| Preoperatively treated malignancy | 1.30 | 1.01–1.69 | 0.046 |
| Preoperative FEV1 < 80% predicted value | 1.26 | 1.00–1.57 | 0.047 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mistiaen, W.; Deblier, I.; Dossche, K.; Vanermen, A. Clinical Outcomes after Surgical Aortic Valve Replacement in 681 Octogenarians: A Single-Center Real-World Experience Comparing the Old Patients with the Very Old Patients. Geriatrics 2024, 9, 44. https://doi.org/10.3390/geriatrics9020044
Mistiaen W, Deblier I, Dossche K, Vanermen A. Clinical Outcomes after Surgical Aortic Valve Replacement in 681 Octogenarians: A Single-Center Real-World Experience Comparing the Old Patients with the Very Old Patients. Geriatrics. 2024; 9(2):44. https://doi.org/10.3390/geriatrics9020044
Chicago/Turabian StyleMistiaen, Wilhelm, Ivo Deblier, Karl Dossche, and Anthony Vanermen. 2024. "Clinical Outcomes after Surgical Aortic Valve Replacement in 681 Octogenarians: A Single-Center Real-World Experience Comparing the Old Patients with the Very Old Patients" Geriatrics 9, no. 2: 44. https://doi.org/10.3390/geriatrics9020044
APA StyleMistiaen, W., Deblier, I., Dossche, K., & Vanermen, A. (2024). Clinical Outcomes after Surgical Aortic Valve Replacement in 681 Octogenarians: A Single-Center Real-World Experience Comparing the Old Patients with the Very Old Patients. Geriatrics, 9(2), 44. https://doi.org/10.3390/geriatrics9020044