
Clinical and Radiological Features of Pneumocystis jirovecii Pneumonia in Children: A Case Series
 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Inclusion Criteria
2.3. Diagnosis of PJP
2.4. Data Collection
2.5. Imaging Review
2.6. Statistical Analysis
3. Results
3.1. Clinical and Epidemiological Characteristics of Study Population
3.2. Study Population
3.3. Clinical Presentation
3.4. PJP Diagnostic Criteria
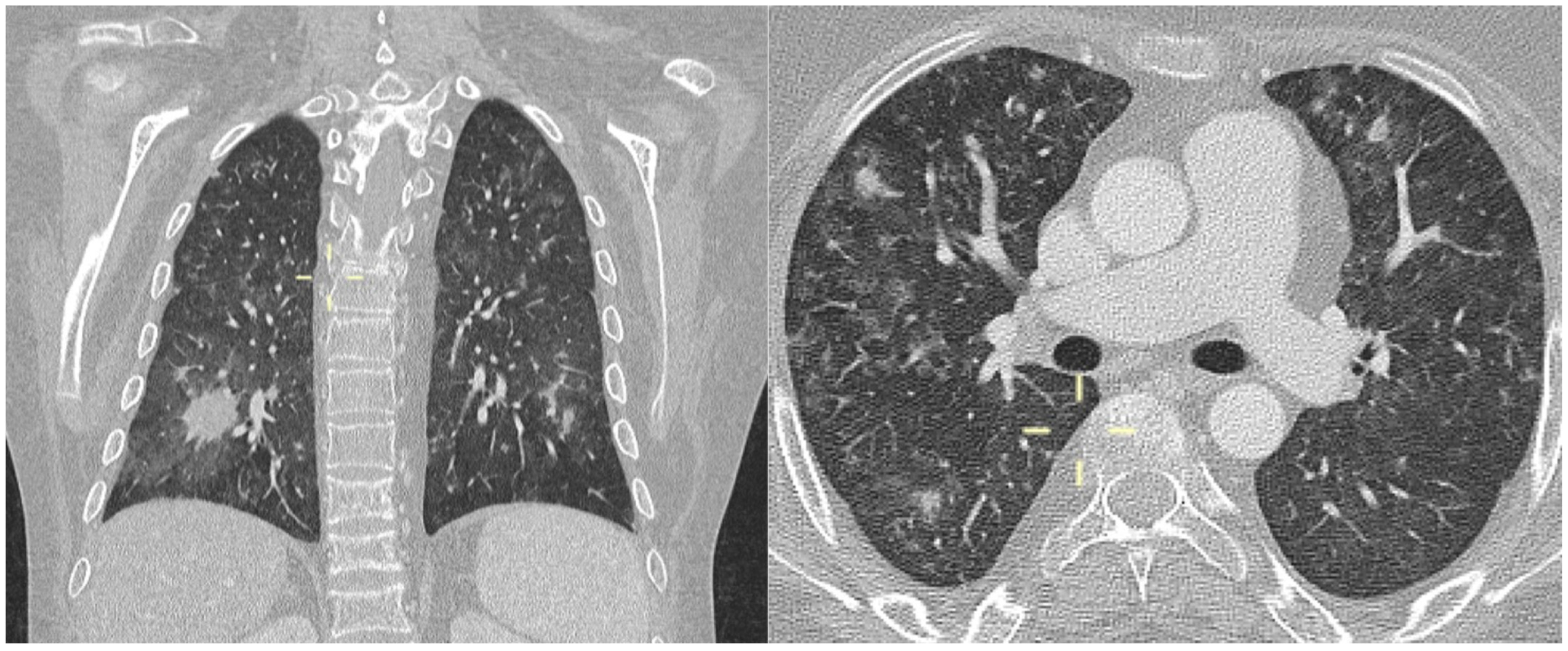
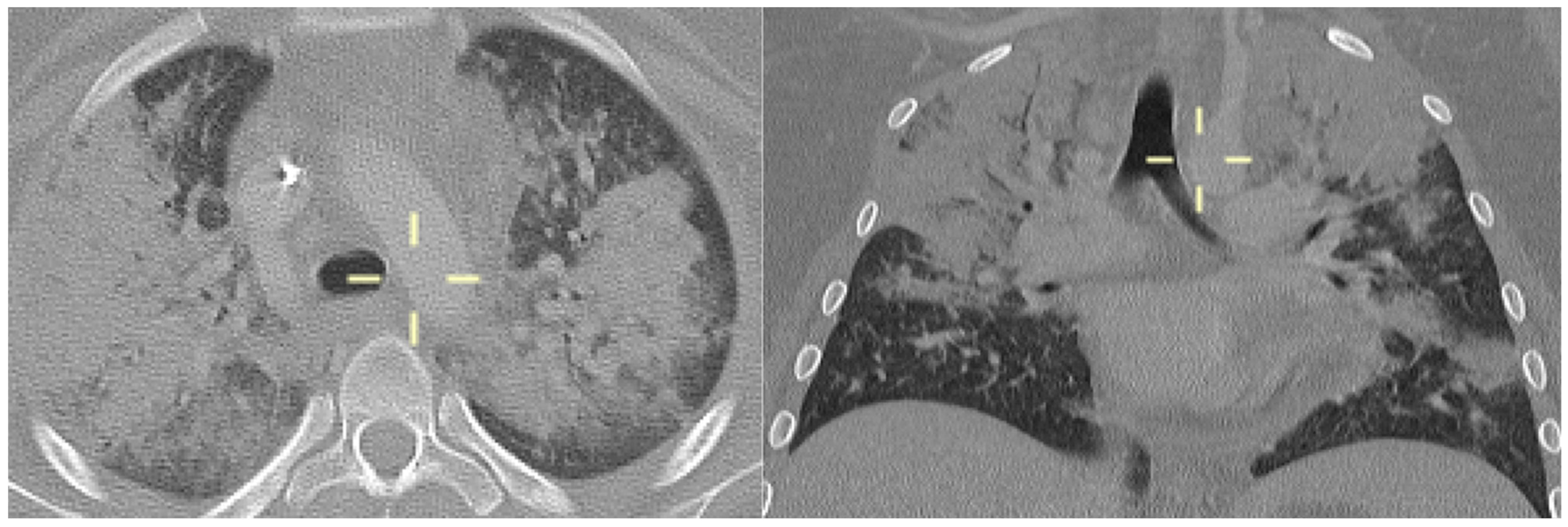
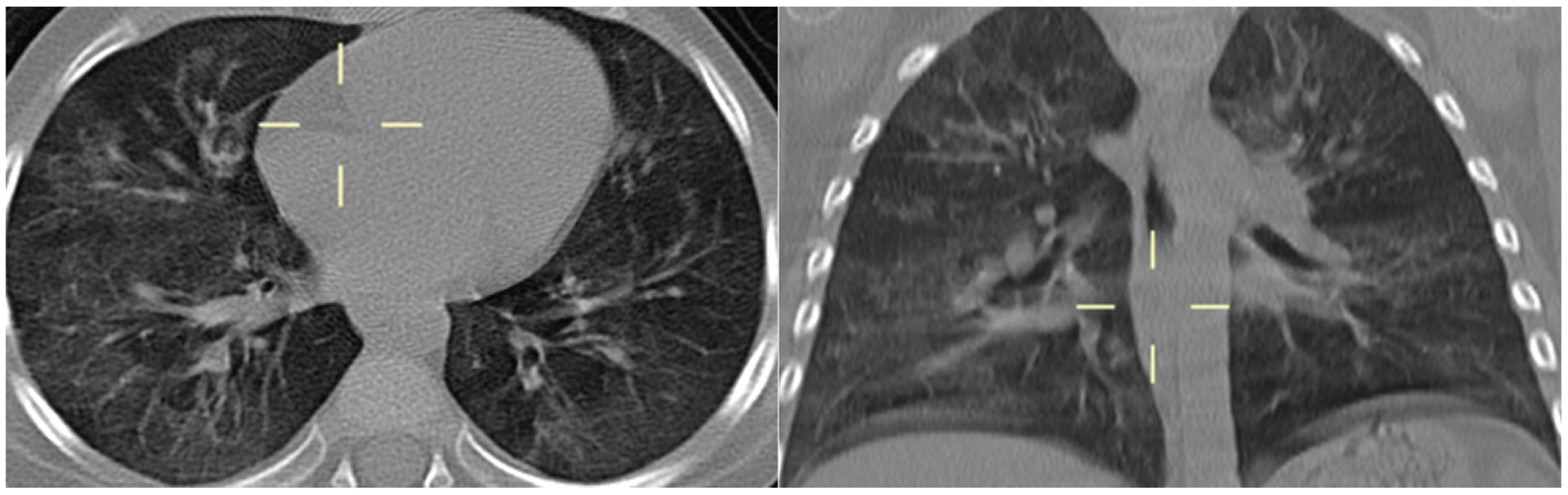
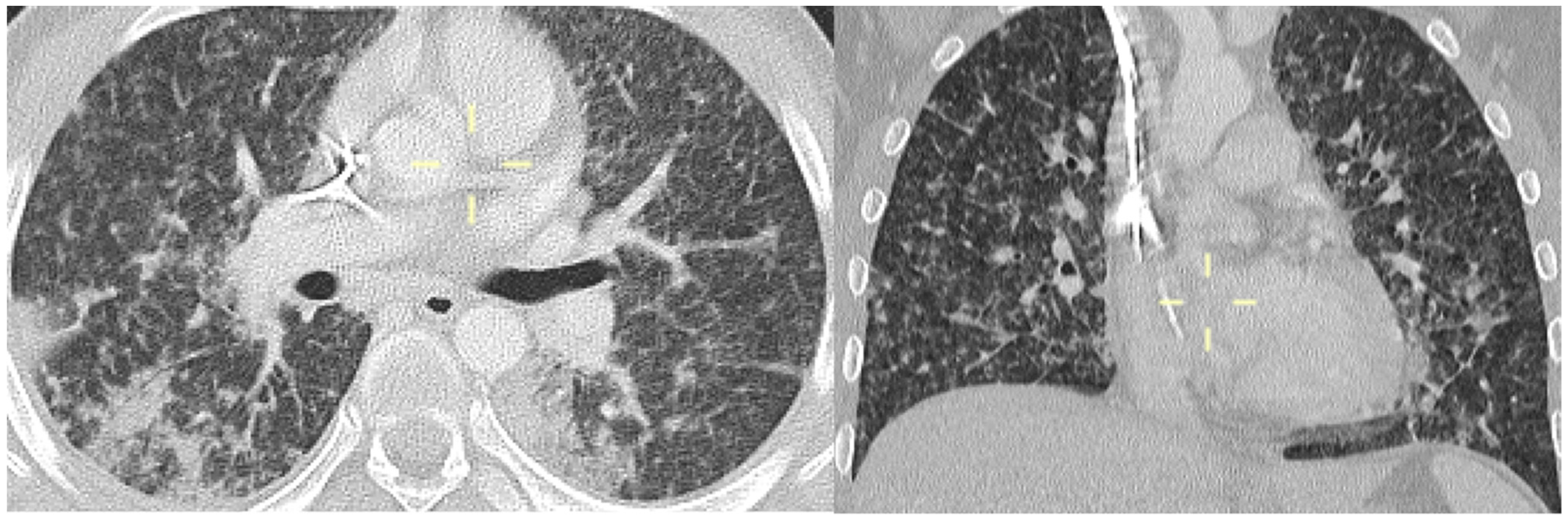
3.5. Radiological Features of PJP in the Study Population
3.6. Treatment and Outcomes
3.7. Secondary Prophylaxis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gona, P.; Van Dyke, R.B.; Williams, P.L.; Dankner, W.M.; Chernoff, M.C.; Nachman, S.A.; Seage, G.R. Incidence of Opportunistic and Other Infections in HIV-Infected Children in the HAART Era. J. Am. Med. Assoc. 2006, 296, 292. [Google Scholar] [CrossRef] [PubMed]
- Morris, A.; Lundgren, J.D.; Masur, H.; Walzer, P.D.; Hanson, D.L.; Frederick, T.; Huang, L.; Beard, C.B.; Kaplan, J.E. Current Epidemiology of Pneumocystis Pneumonia. Emerg. Infect. Dis. 2004, 10, 1713–1720. [Google Scholar] [CrossRef] [PubMed]
- Sepkowitz, K.A. Opportunistic Infections in Patients with and Patients without Acquired Immunodeficiency Syndrome. Clin. Infect. Dis. 2002, 34, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Yale, S.H.; Limper, A.H. Pneumocystis carinii Pneumonia in Patients without Acquired Immunodeficiency Syndrome: Associated Illnesses and Prior Corticosteroid Therapy. Mayo Clin. Proc. 1996, 71, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Roblot, F.; Godet, C.; Le Moal, G.; Garo, B.; Faouzi Souala, M.; Dary, M.; De Gentile, L.; Gandji, J.A.; Guimard, Y.; Lacroix, C.; et al. Analysis of underlying diseases and prognosis factors associated with Pneumocystis carinii pneumonia in immunocompromised HIV-negative patients. Eur. J. Clin. Microbiol. Infect. Dis. 2002, 21, 523–531. [Google Scholar] [PubMed]
- Ling, C.; Qian, S.; Wang, Q.; Zeng, J.; Jia, X.; Liu, J.; Li, Z. Pneumocystis pneumonia in non-HIV children: A 10-year retrospective study. Clin. Respir. J. 2018, 12, 16–22. [Google Scholar] [CrossRef]
- Basiaga, M.L.; Ross, M.E.; Gerber, J.S.; Ogdie, A. Incidence of Pneumocystis jirovecii and Adverse Events Associated with Pneumocystis Prophylaxis in Children Receiving Glucocorticoids. J. Pediatr. Infect. Dis. Soc. 2017, 7, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Thomas, C.F.; Limper, A.H. Pneumocystis Pneumonia. N. Engl. J. Med. 2004, 350, 2487–2498. [Google Scholar] [CrossRef]
- Pyrgos, V.; Shoham, S.; Roilides, E.; Walsh, T.J. Pneumocystis pneumonia in children. Paediatr. Respir. Rev. 2009, 10, 192–198. [Google Scholar] [CrossRef]
- Saltzman, R.W.; Albin, S.; Russo, P.; Sullivan, K.E. Clinical conditions associated with PCP in children. Pediatr. Pulmonol. 2012, 47, 510–516. [Google Scholar] [CrossRef]
- Russian, D.A.; Levine, S.J. Pneumocystis carinii Pneumonia in Patients without HIV Infection. Am. J. Med. Sci. 2001, 321, 56–65. [Google Scholar] [CrossRef] [PubMed]
- Lagrou, K.; Chen, S.; Masur, H.; Viscoli, C.; Decker, C.F.; Pagano, L.; Groll, A.H. Pneumocystis jirovecii Disease: Basis for the Revised EORTC/MSGERC Invasive Fungal Disease Definitions in Individuals without Human Immunodeficiency Virus. Clin. Infect. Dis. 2021, 72 (Suppl. S2), S114–S120. [Google Scholar] [CrossRef] [PubMed]
- Stern, A.; Green, H.; Paul, M.; Vidal, L.; Leibovici, L. Prophylaxis for Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients. Cochrane Database Syst. Rev. 2014, 2016. [Google Scholar] [CrossRef] [PubMed]
- Maertens, J.; Cesaro, S.; Maschmeyer, G.; Einsele, H.; Donnelly, J.P.; Alanio, A.; Hauser, P.M.; Lagrou, K.; Melchers, W.J.G.; Helweg-Larsen, J.; et al. ECIL guidelines for preventing Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J. Antimicrob. Chemother. 2016, 71, 2397–2404. [Google Scholar] [CrossRef] [PubMed]
- Sepkowitz, K.A. Pneumocystis carinii Pneumonia in Patients without AIDS. Clin. Infect. Dis. 1993, 17 (Suppl. S2), S416–S422. [Google Scholar] [CrossRef] [PubMed]
- Bakeera-Kitaka, S.; Musoke, P.; Downing, R.; Tumwine, J.K. Pneumocystis carinii in children with severe pneumonia at Mulago Hospital, Uganda. Ann. Trop. Paediatr. 2004, 24, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Kovacs, J.A. Pneumocystis carinii Pneumonia: A Comparison between Patients with the Acquired Immunodeficiency Syndrome and Patients with Other Immunodeficiencies. Ann. Intern. Med. 1984, 100, 663. [Google Scholar] [CrossRef] [PubMed]
- Monnet, X.; Vidal-Petiot, E.; Osman, D.; Hamzaoui, O.; Durrbach, A.; Goujard, C.; Miceli, C.; Bourée, P.; Richard, C. Critical care management and outcome of severe Pneumocystis pneumonia in patients with and without HIV infection. Crit. Care 2008, 12, R28. [Google Scholar] [CrossRef] [PubMed]
- Yun, K.S.; Anh, B.; Choi, S.H.; Hong, K.T.; Choi, J.Y.; Yun, K.W.; Kang, H.J.; Choi, E.H. Clinical Characteristics and Prognosis of the Modified Probable Pneumocystis jirovecii Pneumonia in Korean Children, 2001–2021. Children 2022, 9, 1596. [Google Scholar] [CrossRef]
- Katragkou, A.; Fisher, B.T.; Groll, A.H.; Roilides, E.; Walsh, T.J. Diagnostic Imaging and Invasive Fungal Diseases in Children. J. Pediatr. Infect. Dis. Soc. 2017, 6 (Suppl. S1), S22–S31. [Google Scholar] [CrossRef]
- Orlowski, H.L.P.; McWilliams, S.; Mellnick, V.M.; Bhalla, S.; Lubner, M.G.; Pickhardt, P.J.; Menias, C.O. Imaging Spectrum of Invasive Fungal and Fungal-Like Infections. RadioGraphics 2017, 37, 1119–1134. [Google Scholar] [CrossRef]
- Vogel, M.N.; Vatlach, M.; Weissgerber, P.; Goeppert, B.; Claussen, C.D.; Hetzel, J.; Horger, M. HRCT-features of Pneumocystis jiroveci pneumonia and their evolution before and after treatment in non-HIV immunocompromised patients. Eur. J. Radiol. 2012, 81, 1315–1320. [Google Scholar] [CrossRef]
- Toma, P.; Bertaina, A.; Castagnola, E.; Colafati, G.S.; D’Andrea, M.L.; Finocchi, A.; Lucidi, V.; Mastronuzzi, A.; Granata, C. Fungal infections of the lung in children. Pediatr. Radiol. 2016, 46, 1856–1865. [Google Scholar] [CrossRef]
- Cereser, L.; Dallorto, A.; Candoni, A.; Volpetti, S.; Righi, E.; Zuiani, C.; Girometti, R. Pneumocystis jirovecii pneumonia at chest High-resolution Computed Tomography (HRCT) in non-HIV immunocompromised patients: Spectrum of findings and mimickers. Eur. J. Radiol. 2019, 116, 116–127. [Google Scholar] [CrossRef]
- Hardak, E.; Brook, O.; Yigla, M. Radiological Features of Pneumocystis jirovecii Pneumonia in Immunocompromised Patients with and without AIDS. Lung 2010, 188, 159–163. [Google Scholar] [CrossRef]
- Selwyn, P.A.; Pumerantz, A.S.; Durante, A.; Alcabes, P.G.; Gourevitch, M.N.; Boiselle, P.G.; Elmore, J.G. Clinical predictors of Pneumocystis carinii pneumonia, bacterial pneumonia and tuberculosis in HIV-infected patients. AIDS 1998, 12, 885–893. [Google Scholar] [CrossRef]
- Kanne, J.P.; Yandow, D.R.; Meyer, C.A. Pneumocystis jiroveci Pneumonia: High-Resolution CT Findings in Patients with and without HIV Infection. Am. J. Roentgenol. 2012, 198, W555–W561. [Google Scholar] [CrossRef]
- Mantadakis, E. Pneumocystis jirovecii Pneumonia in Children with Hematological Malignancies: Diagnosis and Approaches to Management. J. Fungi 2020, 6, 331. [Google Scholar] [CrossRef]
- Castagnola, E.; Fioredda, F.; Moroni, C.; Loy, A.; Viscoli, C. Pneumothorax and Pneumocystis Pneumonia in an Infant with Acquired Immunodeficiency Syndrome. Pediatr. Infect. Dis. J. 1992, 11, 504. [Google Scholar] [CrossRef]
- Gruden, J.F.; Huang, L.; Turner, J.; Webb, W.R.; Merrifield, C.; Stansell, J.D.; Gamsu, G.; Hopewell, P.C. High-resolution CT in the evaluation of clinically suspected Pneumocystis carinii pneumonia in AIDS patients with normal, equivocal, or nonspecific radiographic findings. Am. J. Roentgenol. 1997, 169, 967–975. [Google Scholar] [CrossRef]
- Hsu, J.M.; Hass, A.; Gingras, M.-A.; Chong, J.; Costiniuk, C.; Ezer, N.; Fraser, R.S.; McDonald, E.G.; Lee, T.C. Radiographic features in investigated for Pneumocystis jirovecii pneumonia: A nested case-control study. BMC Infect. Dis. 2020, 20, 492. [Google Scholar] [CrossRef]
- Alanio, A.; Hauser, P.M.; Lagrou, K.; Melchers, W.J.G.; Helweg-Larsen, J.; Matos, O.; Cesaro, S.; Maschmeyer, G.; Einsele, H.; Donnelly, J.P.; et al. ECIL guidelines for the diagnosis of Pneumocystis jirovecii pneumonia in patients with haematological malignancies and stem cell transplant recipients. J. Antimicrob. Chemother. 2016, 71, 2386–2396. [Google Scholar] [CrossRef]
- Guegan, H.; Robert-Gangneux, F. Molecular diagnosis of Pneumocystis pneumonia in immunocompromised patients. Curr. Opin. Infect. Dis. 2019, 32, 314–321. [Google Scholar] [CrossRef]
- Summah, H.; Zhu, Y.G.; Falagas, M.E.; Vouloumanou, E.K.; Qu, J.M. Use of real-time polymerase chain reaction for the diagnosis of Pneumocystis pneumonia in immunocompromised patients: A meta-analysis. Chin. Med. J. 2013, 126, 1965–1973. [Google Scholar] [CrossRef]
- Fan, L.-C.; Lu, H.-W.; Cheng, K.-B.; Li, H.-P.; Xu, J.-F. Evaluation of PCR in Bronchoalveolar Lavage Fluid for Diagnosis of Pneumocystis jirovecii Pneumonia: A Bivariate Meta-Analysis and Systematic Review. PLoS ONE 2013, 8, e73099. [Google Scholar] [CrossRef]
- Desoubeaux, G.; Chesnay, A.; Mercier, V.; Bras-Cachinho, J.; Moshiri, P.; Eymieux, S.; De Kyvon, M.A.; Lemaignen, A.; Goudeau, A.; Bailly, É. Combination of β-(1,3)-D-glucan testing in serum and qPCR in nasopharyngeal aspirate for facilitated diagnosis of Pneumocystis jirovecii pneumonia. Mycoses 2019, 62, 1015–1022. [Google Scholar] [CrossRef]
- Morjaria, S.; Frame, J.; Franco-Garcia, A.; Geyer, A.; Kamboj, M.; Babady, N.E. Clinical Performance of (1,3) Beta-D Glucan for the Diagnosis of Pneumocystis Pneumonia (PCP) in Cancer Patients Tested with PCP Polymerase Chain Reaction. Clin. Infect. Dis. 2019, 69, 1303–1309. [Google Scholar] [CrossRef]
- Senécal, J.; Smyth, E.; Del Corpo, O.; Hsu, J.M.; Amar-Zifkin, A.; Bergeron, A.; Cheng, M.P.; Butler-Laporte, G.; McDonald, E.G.; Lee, T.C. Non-invasive diagnosis of Pneumocystis jirovecii pneumonia: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2022, 28, 23–30. [Google Scholar] [CrossRef]
- White, P.L.; Backx, M.; Barnes, R.A. Diagnosis and management of Pneumocystis jirovecii infection. Expert Rev. Anti-Infect. Ther. 2017, 15, 435–447. [Google Scholar] [CrossRef]
- Schmiegelow, K.; Attarbaschi, A.; Barzilai, S.; Escherich, G.; Frandsen, T.L.; Halsey, C.; Hough, R.; Jeha, S.; Kato, M.; Liang, D.-C.; et al. Consensus definitions of 14 severe acute toxic effects for childhood lymphoblastic leukaemia treatment: A Delphi consensus. Lancet Oncol. 2016, 17, e231–e239. [Google Scholar] [CrossRef]
- Caselli, D.; Petris, M.G.; Rondelli, R.; Carraro, F.; Colombini, A.; Muggeo, P.; Ziino, O.; Melchionda, F.; Russo, G.; Pierani, P.; et al. Single-Day Trimethoprim/Sulfamethoxazole Prophylaxis for Pneumocystis Pneumonia in Children with Cancer. J. Pediatr. 2014, 164, 389–392.e1. [Google Scholar] [CrossRef]
- Castagnola, E.; Mesini, A.; Saffioti, C.; Moscatelli, A.; Pierri, F.; Giardino, S.; Faraci, M. Failures of once-a-week trimethoprim-sulfamethoxazole prophylaxis in children undergoing allogeneic hematopoietic stem cell transplant. Transpl. Infect. Dis. 2020, 22, e13231. [Google Scholar] [CrossRef]
- Williams, K.M.; Ahn, K.W.; Chen, M.; Aljurf, M.D.; Agwu, A.L.; Chen, A.R.; Walsh, T.J.; Szabolcs, P.; Boeckh, M.J.; Auletta, J.J.; et al. The incidence, mortality and timing of Pneumocystis jiroveci pneumonia after hematopoietic cell transplantation: A CIBMTR analysis. Bone Marrow Transplant. 2016, 51, 573–580. [Google Scholar] [CrossRef]
- Taddeo, D.; Egedy, M.; Frappier, J.-Y. Adherence to treatment in adolescents. Paediatr. Child Health 2008, 13, 19–24. [Google Scholar] [CrossRef]
- Metzner, G.; von der Warth, R.; Glattacker, M. The concept of treatment beliefs in children and adolescents with chronic health conditions: A scoping review. Health Psychol. Rev. 2023, 1–35. [Google Scholar] [CrossRef]
- Castagnola, E.; Zarri, D.; Caprino, D.; Losurdo, G.; Micalizzi, C. Cotrimoxazole prophylaxis of Pneumocystis carinii infection during the treatment of childhood acute lymphoblastic leukemia—Beware non compliance in older children and adolescents. Support. Care Cancer 2001, 9, 552–553. [Google Scholar] [CrossRef]
- Giacobbe, D.R.; Dettori, S.; Di Pilato, V.; Asperges, E.; Ball, L.; Berti, E.; Blennow, O.; Bruzzone, B.; Calvet, L.; Capra Marzani, F.; et al. Pneumocystis jirovecii pneumonia in intensive care units: A multicenter study by ESGCIP and EFISG. Crit. Care 2023, 27, 323. [Google Scholar] [CrossRef]
- Lehrnbecher, T.; Robinson, P.D.; Fisher, B.T.; Castagnola, E.; Groll, A.H.; Steinbach, W.J.; Zaoutis, T.E.; Negeri, Z.F.; Beyene, J.; Phillips, B.; et al. Galactomannan, β-D-Glucan, and Polymerase Chain Reaction–Based Assays for the Diagnosis of Invasive Fungal Disease in Pediatric Cancer and Hematopoietic Stem Cell Transplantation: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2016, 63, 1340–1348. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient ID | Age (Years)/Sex | Underlining Condition | HCT Type | Time from HCT to PJP (Days) | Ongoing GvHD | Comorbidities at Diagnosis | CS at Diagnosis | Immunosuppressive Drugs at Diagnosis | Ongoing Lympho-penia | Ongoing PJP Prophylaxis Regimen | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|
| #1 | 19/M | JIA | No | NA | NA | SARS-CoV-2 pneumonia | Yes | CsA, canakinumab, MAS 825, anakinra, eculizumab | Yes | No | Full recovery |
| #2 | 8/F | ALL | No | NA | NA | No | No | MTX, mercaptopurine | No | TMP/SMX 1/w | Full recovery |
| #3 | 13/F | ALL | haplo | 26 | Yes (grade 2) | No | Yes | CT, rituximab | Yes | TMP/SMX 3/w | Full recovery |
| #4 | 2/F | MDS | MUD | 120 | Yes (grade 4) | No | Yes | CsA, ruxolitinib | No | TMP/SMX 1/w | Full recovery |
| #5 | 17/M | MPAL | MUD | 27 | No | BSI E. faecium | Yes | CT, dasatinib | Yes | TMP/SMX 1/w | Full recovery |
| #6 | 1/F | PI | No | NA | NA | No | Yes | anakinra, sirolimus | Yes | TMP/SMX 1/w | Full recovery |
| #7 | 3/M | PI | No | NA | NA | BSI C. koseri, esophageal candidiasis | No | No | Yes | TMP/SMX 1/w | Full recovery |
| #8 | 14/F | ependymoma | No | NA | NA | No | Yes | CT, RT | No | No | Full recovery |
| #9 | 4/F | CD | No | NA | NA | No | Yes | No | No | No | Full recovery |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricci, E.; Bartalucci, C.; Russo, C.; Mariani, M.; Saffioti, C.; Massaccesi, E.; Pierri, F.; Brisca, G.; Moscatelli, A.; Caorsi, R.; et al. Clinical and Radiological Features of Pneumocystis jirovecii Pneumonia in Children: A Case Series. J. Fungi 2024, 10, 276. https://doi.org/10.3390/jof10040276
Ricci E, Bartalucci C, Russo C, Mariani M, Saffioti C, Massaccesi E, Pierri F, Brisca G, Moscatelli A, Caorsi R, et al. Clinical and Radiological Features of Pneumocystis jirovecii Pneumonia in Children: A Case Series. Journal of Fungi. 2024; 10(4):276. https://doi.org/10.3390/jof10040276
Chicago/Turabian StyleRicci, Erica, Claudia Bartalucci, Chiara Russo, Marcello Mariani, Carolina Saffioti, Erika Massaccesi, Filomena Pierri, Giacomo Brisca, Andrea Moscatelli, Roberta Caorsi, and et al. 2024. "Clinical and Radiological Features of Pneumocystis jirovecii Pneumonia in Children: A Case Series" Journal of Fungi 10, no. 4: 276. https://doi.org/10.3390/jof10040276
APA StyleRicci, E., Bartalucci, C., Russo, C., Mariani, M., Saffioti, C., Massaccesi, E., Pierri, F., Brisca, G., Moscatelli, A., Caorsi, R., Bruzzone, B., Damasio, M. B., Marchese, A., Mesini, A., & Castagnola, E. (2024). Clinical and Radiological Features of Pneumocystis jirovecii Pneumonia in Children: A Case Series. Journal of Fungi, 10(4), 276. https://doi.org/10.3390/jof10040276