Abstract
Emergomycosis is an endemic mycosis caused by the Emergomyces species. Infections due to this agent have been reported globally. Hence, the present systematic review on Emergomyces infections was conducted to study the disease epidemiology, underlying diseases and risk factors, causative agents, and treatment and outcome. The MEDLINE, Scopus, Embase, and Web of Science databases were searched systematically with appropriate keywords from January 1990 to October 2022. A total of 77 cases of emergomycosis were included in the analysis. Emergomycosis was most commonly seen in patients with human immunodeficiency virus (HIV) infection (n = 61, 79.2%) and HIV-uninfected patients with or without other comorbidities (n = 16, 20.8%). The underlying disease and risk factors significantly associated with emergomycosis in the HIV-infected patients were CD4+ T-cell counts less than 100 cells/mm3 (n = 55, 90.2%), anaemia (n = 30, 49.2%), and thrombocytopenia (n = 17, 27.9%), whereas in the HIV-uninfected patients, treatment with immunosuppressive drugs (n = 10, 62.5%), renal disease (n = 8, 50%), transplant recipients (n = 6, 37.5%), and diabetes mellitus (n = 4, 25%) were the significant risk factors associated with emergomycosis. Emergomyces africanus (n = 55, 71.4%) is the most common causative agent, followed by E. pasteurianus (n = 9, 11.7%) and E. canadensis (n = 5, 6.5%). E. africanus was most often isolated from HIV-infected patients (n = 54, 98.2%), whereas E. pasteurianus was most common in HIV-uninfected patients (n = 5, 55.6%). The all-cause mortality rate of the total cohort is 42.9%. No significant variation in the mortality rate is observed between the HIV-infected patients (n = 28, 36.4%) and the HIV-uninfected patients (n = 5, 6.5%). In conclusion, with an increase in the immunosuppressed population across the globe in addition to HIV infection, the case burden of emergomycosis may increase in the future. Hence, clinicians and mycologists should be vigilant and clinically suspicious of emergomycosis, which helps in early diagnosis and initiation of antifungal treatment to prevent disease mortality.
1. Introduction
Emergomycosis is an emerging thermally dimorphic fungal infection caused by the genus Emergomyces (formerly placed under the genus Emmonsia), belonging to the order Onygenales and family Ajellomycetaceae [1,2]. The taxonomy of fungal species in the family Ajellomycetaceae is rapidly evolving using a phylogenetic or phylogenomic approach, and multiple new species and genera have been described [1,2]. Multi-gene phylogenetic analyses on Emmonsia and Emmonsia-like fungal species revealed that the genus is polyphyletic [1,2]. Further, phylogenetic studies showed that Emmonsia species were clustered closely with the genus Emergomyces and Blastomyces [1,2,3]. Hence, the species described previously under Emmonsia were taxonomically repositioned, either in the genus Emergomyces or Blastomyces [1,2,3]. These recent phylogenetic changes may render the genus Emmonsia obsolete. Based on molecular phylogenetic analyses, seven species are currently placed in the genus Emergomyces, namely E. africanus, E. canadensis, E. crescens, E. europaeus, E. orientalis, E. pasteurianus, and E. sola [1,2,3]. Except for E. sola (non-pathogenic soil saprobe, not associated with human infections), the other pathogenic Emergomyces species are known to cause invasive human diseases [4].
The Emergomyces species is a soil saprobe, and humans may acquire the infection by inhaling the contaminated spores from the environment. Infections due to Emergomyces species are rising globally, and the cases are being reported from Africa, Asia, Europe, North America, and South America [4,5]. However, a high case burden has been seen in Africa, specifically in South Africa [6,7]. Further, soil samples analysed using molecular techniques from South Africa reported a 30% positivity rate for E. africanus, a primary causative agent of human-disseminated emergomycosis in Africa [8]. Similarly, E. crescens, causing granulomatous pulmonary adiaspiromycosis in humans and rodents, has been isolated from soils and rodent tissue samples [9]. The ecological niche of other pathogenic Emergomyces species is largely unknown. The significant risk factors associated with emergomycosis were human immunodeficiency virus (HIV) infection, transplant recipients, and malignancies [4,5]. However, occasionally, infections are reported in apparently healthy immunocompetent hosts [4]. The disease manifests as skin lesions, pulmonary infection, fungemia, or severe disseminated disease. Most patients with Emergomyces infections are immunocompromised; early diagnosis is essential to initiate appropriate antifungal therapy. The mortality rate in emergomycosis patients ranges from 48 to 51% [6,10]. With this background, the present systematic review was conducted to understand the disease epidemiology, underlying disease and risk factors, and treatment and outcome associated with emergomycosis.
2. Methods
2.1. Study Design, Selection, and Data Extraction
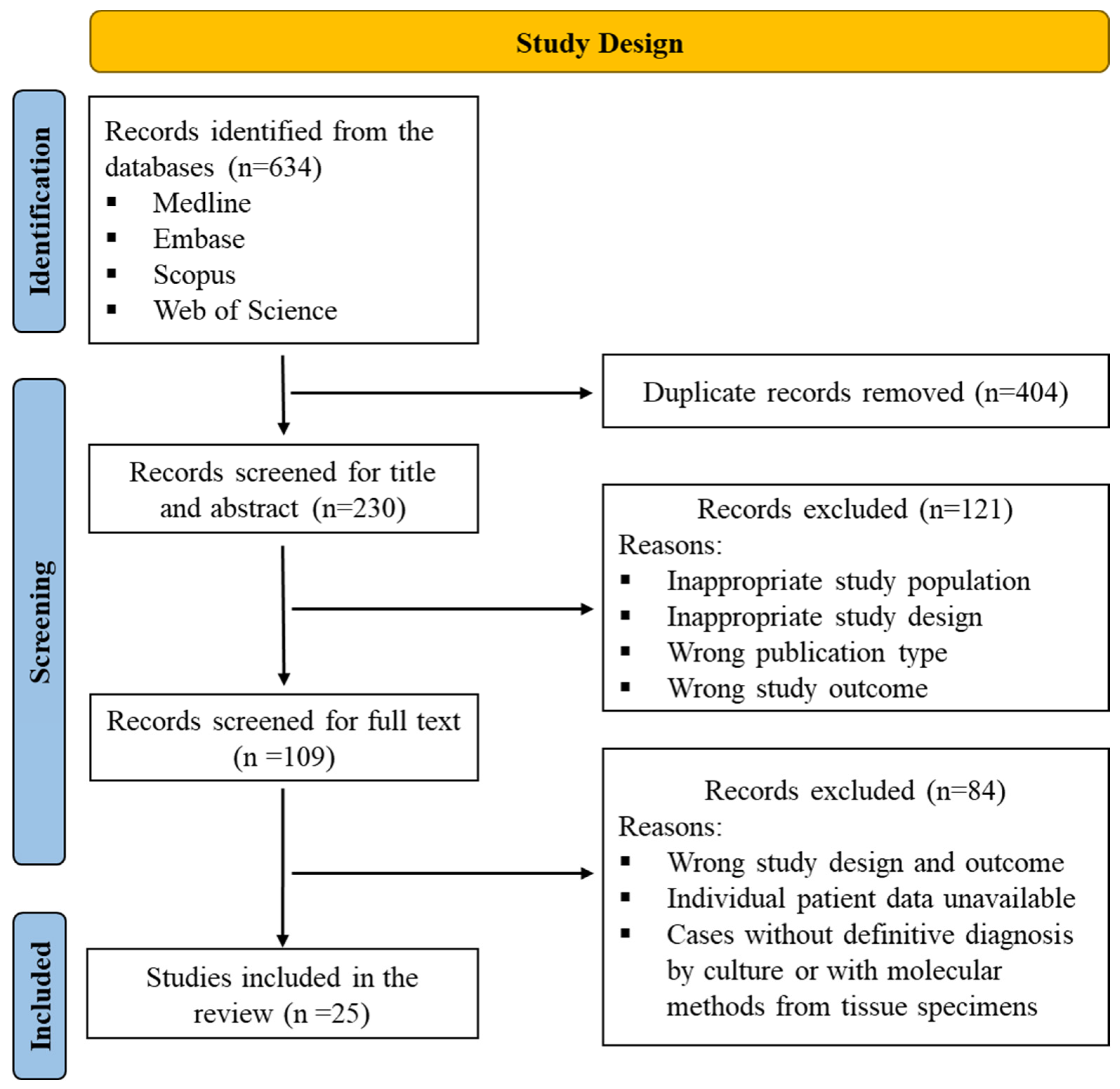
The systematic review was conducted per PRISMA guidelines and has been registered with PROSPERO (registration number: CRD42023375274). Studies on Emergomyces infections published between January 1990 and October 2022 were searched from the following databases: Medline, Embase, Scopus, and Web of Science, along with back-references of the published literature. The citations of the studies that matched the search strategy were retrieved from these databases and uploaded to the Rayyan QCRI software [11]. Duplicates were removed, then the title and abstract of the articles were screened for inclusion by two independent reviewers (K.S.V and H.P.P), and discrepancies were fixed via discussion and consensus with the third reviewer (A.S.). Further, full texts were screened for inclusion of the studies in the review (K.S.V and H.P.P), and the studies that failed to fulfil the inclusion criteria were excluded from the analysis. A detailed study description is given in Figure 1.
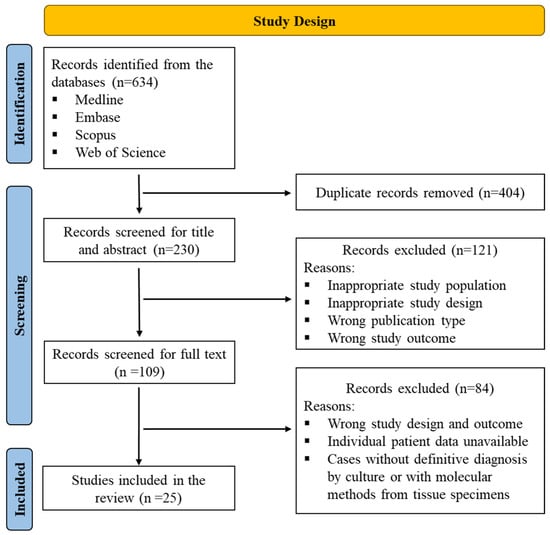
Figure 1.
PRISMA flowchart depicting the study design and process.
Only proven cases of Emergomyces infections, either with culture or with molecular methods from tissue specimens (definitive diagnosis of emergomycosis), were included in the analysis. Studies with proven Emergomyces infections published in English texts, such as case series, case reports, prospective and retrospective studies, and conference papers with complete case details, were included in the review. The data from the included studies, such as country of the study, number of Emergomyces cases reported, patient’s age, sex, underlying diseases and risk factors, mode of diagnosis, causative agents, antifungal treatment, and outcome of the disease (i.e., mortality) were extracted (K.S.V and D.R.G). Further, the taxonomy of Emergomyces was revised recently; hence, we contacted the authors to confirm the species identification (only when the speciation of the isolates was not clearly defined). Further, this review excluded narrative and mini reviews, systematic and meta-analysis studies, editorials, and non-English literature.
2.2. Risk of Bias Assessment
The included articles were assessed for risk of bias using a modification of the Joanna Briggs Institute (JBI) tool for the case series [12,13]. The articles were categorised as having a low, high, or unclear risk of bias under the following domains: clear inclusion criteria, a valid identification method, clear reporting of the demographic information, clinical parameters, outcomes, and the presenting site(s)/clinic(s) of demographic information.
2.3. Statistical Analysis
The clinical details extracted from emergomycosis cases, such as underlying diseases and risk factors, mode of diagnosis, causative agents, treatment, and the disease outcome between the groups (HIV-infected and HIV-uninfected patients), were compared. We performed the χ2 test (Fisher’s exact test) using SPSS version 22 to draw the statistical inference. A two-sided p-value < 0.05 was considered significant.
3. Results
A total of 25 studies that fulfilled the inclusion criteria were analysed, and the risk of bias was evaluated [10,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38]. Three studies had a high risk of bias in one of the domains assessed (in two studies, clinical findings were not described [30,38]); and one study had an unclear risk of bias, failing to document the disease outcome properly [33]). Of these studies, a total of 77 proven cases of emergomycosis either with culture (n = 72, 93.5%) or with molecular diagnosis from tissue specimens (n = 5, 6.5%) were included in the study. By geographic distribution, most cases were from Africa (n = 57, 74%), Asia (n = 7, 9.1%), North America (n = 7, 9.1%), Europe (n = 5, 6.5%), and South America (n = 1, 1.3%). Adults were most commonly affected (n = 75, 98.7%) with one paediatric case. The age group of the patients ranged between 03 and 80 years. The mean age of the patients was 39.25 years (standard deviation ± 13.28). Males were more commonly affected (n = 47, 61%). The male and female ratio is 1.57:1. The clinical details, such as clinical manifestations, underlying diseases, and risk factors, are summarised in Table 1 and Table S1.

Table 1.
Clinical details of emergomycosis patients.
For comparative analysis based on the underlying disease and risk factors, we categorised the patients into two groups: (a) HIV-infected and (b) HIV-uninfected patients with or without other comorbidities. Of the 77 cases analysed, most were seen in patients with HIV infection (n = 61, 79.2%). Emergomycosis was more commonly seen in HIV-infected patients with CD4+ T-cell counts less than 100 cells/mm3 (n = 55, 90.2%, p < 0.0001). Further, anaemia (n = 30, 49.2%, p = 0.010) and thrombocytopenia (n = 17, 27.9%, p = 0.016) were the significant risk factors in the HIV group. Whereas in the HIV-uninfected patients (n = 16, 20.8%), the significant risk factors associated with emergomycosis were patients on immunosuppressive drugs (n = 10, 62.5%, p < 0.0001), renal disease (n = 8, 50%, p < 0.0001), transplant recipients (n = 6, 37.5%, p < 0.0001), and diabetes mellitus (n = 4, 25%, p = 0.006). Further, in the HIV-uninfected patients, four were apparently healthy, and no risk factors were ascertained (n = 4, 25%, p = 0.001). The other risk factors such as opportunistic infections were most common in the HIV-infected (n = 26, 33.8%), compared to the HIV-uninfected patients (n = 3, 3.9%, p = 0.092). Table S2 summarises the opportunistic infections in the emergomycosis patients.
The disease manifested as skin lesions in most of the HIV patients (n = 58, 95.1%), compared to the HIV-uninfected patients (n = 7, 43.8%, p < 0.0001) (Table S3). A subset analysis of HIV-infected patients did not identify any other significant risk factors, such as patients not receiving anti-retroviral therapy (ART) or ART-defaulted patients before the appearance of skin lesions. The lesions primarily appeared as papules (n = 32, 41.6%), nodules (n = 17, 22.1%), crust (n = 15, 19.5%), and plaques (n = 11, 14.3%) in both groups (Table S3), and the appearances/clinical descriptions of the skin lesions were not statistically significant between HIV-infected and HIV-uninfected patients (Table S3). Other than skin lesions, the disease manifested as pulmonary disease in HIV-uninfected patients (n = 12, 75%, p = 0.000l). Table S4 describes the chest and abdominal radiological findings in the emergomycosis patients. Abnormal chest radiological findings such as lung opacities and lung infiltrates were more common in the HIV-uninfected patients (n = 14, 87.5%) compared to the HIV-infected patients (n = 32, 52.5%, p = 0.011). Contrastingly, in the HIV-infected patients, the dissemination of the disease is seen, and the causative agents are isolated from blood (n = 23, 37.7%, p = 0.074) and bone marrow specimens (n = 14, 23%, p = 0.034) more frequently (Table 2).
Table 2.
Diagnostic methods and causative agents of emergomycosis.
The specimens and diagnostic methods used in the emergomycosis detection are described in Table 2. Most of the cases were diagnosed with histology and culture (n = 50, 64.9%), culture alone (n = 22, 28.6%), and histology and molecular detection from tissue specimens (n = 5, 6.5%). Bone marrow specimens in HIV patients (n = 14, 23%, p = 0.034) and the respiratory specimens (n = 12, 75%, p = 0.0001) in the HIV-uninfected patients showed higher isolation rate for Emergomyces species. For the culture-proven cases, due to the taxonomy reclassification of Emergomyces species, we contacted the authors of the study (only when proper speciation is not mentioned in the article) to confirm the species identification. The majority of the cases in this review were due to E. africanus (n = 55, 71.4%), followed by E. pasteurianus (n = 9, 11.7%), E. canadensis (n = 5, 6.5%), E. crescens (n = 2, 2.6%), E. orientalis (n = 2, 2.6%), and E. europaeus (n = 1, 1.3%). However, in three cases, the species identification of Emergomyces was not available. Emergomyces africanus was significantly isolated from the HIV-infected patients (n = 54, 98.2%, p = 0.0001). In comparison, E. pasteurianus (n = 5, 55.6%, p = 0.016) was more commonly isolated from the HIV-uninfected patients.
Treatment and outcome of an Emergomyces infection are summarised in Table 1 and Table S5. The all-cause mortality of the total cohort was 42.9% (n = 33). Antifungal therapy was initiated in 64 (83.1%) patients, and 9 (11.7%) patients did not receive any antifungal drugs; the mortality rates in these groups were 34.4% and 88.9%, respectively (p = 0.003). Most patients received combination therapy of amphotericin B and azoles (n = 34, 44.2%), and in this group, the mortality rate was 23.5% (n = 8, p = 0.003). Further, the subset analysis showed that amphotericin B and itraconazole were given to 24 patients, and in these patients, the mortality rate decreased to 20.8% (n = 5, p = 0.012). Further, we assessed the mortality rate between the HIV-infected (n = 28, 45.9%) and the HIV-uninfected patients (n = 5, 31.3%, p = 0.397), where no significant difference was observed.
4. Discussion
The present systematic review discusses the underlying diseases and risk factors, causative agents, treatment, and disease outcome in emergomycosis cases. This review identified 77 proven emergomycosis cases either with culture or with direct detection using molecular methods from tissue specimens that were analysed from January 1990 to October 2022. The causative agents of emergomycosis infections were E. africanus (n = 55, 71.4%), E. pasteurianus (n = 9, 11.7%), and E. canadensis (n = 5, 6.5%). Most emergomycosis cases were seen in HIV-infected patients (n = 61, 79.2%). The underlying diseases and risk factors for emergomycosis in the HIV-infected patients were CD4+ T-cell counts (<100 cells/mm3), anaemia, and thrombocytopenia (Table 1). HIV-uninfected patients on immunosuppressive drug therapy, transplant recipients, renal diseases, and diabetes mellitus were at significant risk for emergomycosis. Further, few cases of emergomycosis have been reported in apparently healthy immunocompetent hosts (Table 1).
Most of the emergomycosis cases described in this review are reported from Africa (n = 57, 74%), specifically high burden is seen in South Africa (n = 56, 98.2%). E. africanus is the most common agent causing emergomycosis in South Africa (n = 55, 96.5%). The reason for the highest case burden in South Africa is unknown. The possible reason for the increased case burden of emergomycosis in South Africa may be attributed to the high prevalence of the HIV-infected population and non-adherence to anti-retroviral therapy, high clinical awareness, or high spore burden of Emergomyces species in South African soils [4,5,7]. An environmental study from South Africa showed that 30% of the analysed soil samples contained E. africanus [8]. It is presumed that patients acquire the infection via inhalation of the spores from the environment. A study from South Africa analysed the air propagules using quantitative PCR, and the study reported that 10% of the samples analysed contained E. africanus [39]. These findings showed that, possibly, the high spore burden due to Emergomyces spores in the environment and the host factors (immunocompromised conditions such as HIV, malignancies, and solid organ transplant recipients) may be the prime factors contributing to the disease burden. Further, other than E. africanus, infections due to newly described Emergomyces species are reported across continents. However, the ecological niche of those Emergomyces species has yet to be known. In contrast to E. africanus, the second most common agent of emergomycosis, E. pasteurianus causes infection more often in HIV-uninfected patients (n = 5, 31.3%), compared to HIV-infected patients (n = 4, 6.6%, p = 0.016).
In the present review, patients with emergomycosis often presented with skin lesions (n = 65, 84.4%); however, the skin lesions were most common in the HIV patients (75.3%) compared to the HIV-uninfected patients (9.1%) (Table S3). Contrastingly, in the HIV-uninfected patients, emergomycosis presented as respiratory disease; the respiratory specimens yielded a higher isolation rate of Emergomyces species in the HIV-uninfected patients (75%) compared to 5% in the HIV-infected patients (p = 0.0001). Further, blood (37.7%) and bone marrow (23%, p = 0.034) specimens had higher positive culture rates in HIV-infected patients, showing the disseminated nature of the disease in the HIV-infected patients. The risk factors for emergomycosis in HIV-infected patients were CD4+ T-cell counts (<100 cells/mm3), anaemia, and thrombocytopenia. In HIV-uninfected patients, treatment with immunosuppressive drugs and transplant recipients were at significant risk for emergomycosis (Table 1). These findings show that the lack of a cell-mediated immune response is the most significant risk factor for emergomycosis.
In the present review, the all-cause mortality rate of emergomycosis was 42.9%. At the same time, the difference in the mortality rate was not statistically significant between the HIV-infected patients (36.4%) compared to 6.5% in the HIV-uninfected patients. Similarly, the other studies documented a mortality rate of 48–51% [6,10]. There are no standard treatment guidelines for the management of emergomycosis. The treatment guidelines devised by the Infectious Diseases Society of America (IDSA) for managing other endemic mycoses, such as histoplasmosis, are currently followed in treating emergomycosis infections [40,41,42]. The treatment and outcome of the disease are described in Table 1 and Table S5. Patients on antifungal therapy had a lesser mortality rate, 34.4%, than those without antifungal treatment (89%, p = 0.003). Amphotericin B and triazole combination therapy had a better survival rate at 76.5% (p = 0.003). Amphotericin B and itraconazole therapy effectively reduced the mortality rate in patients with emergomycosis (20.8%, p = 0.012). Further, triazole alone was used as therapy in 19 (24.7%) patients, and the mortality rate was 36.8% (p = 0.602). These findings showed that the combination therapy of amphotericin B and azole specifically itraconazole, may help in the improved clinical outcome of the disease. These findings correlate with the in vitro antifungal susceptibility testing results, as amphotericin B was the most effective drug against the Emergomyces species [43,44]. Similarly, itraconazole has low minimum inhibitory concentrations, making it the ideal candidate for step-down therapy following amphotericin B [43,44].
5. Conclusions
This review highlights the emergence of new thermal dimorphic fungi, the Emergomyces species, and their importance in clinical settings as this agent is associated with high mortality. The disease prevalence of emergomycosis is not known; population-based studies are necessary to estimate the true prevalence/incidence. Patients with HIV, malignancy, and transplant recipients are at increased risk for emergomycosis. In the future, an increase in emergomycosis infections may be seen in patients with defective cell-mediated immunity or with immunosuppressive therapy. Further, emergomycosis is an endemic disease, and a high index of clinical suspicion is needed for early diagnosis and treatment. However, the disease has recently been seen in non-endemic areas, and many new species have been described. Hence, a molecular phylogenetic approach and genomic studies are essential to understanding disease epidemiology. Emergomycosis is associated with high mortality; further, there are no standard treatment guidelines available. Based on the available data, combination therapy with amphotericin B and step-down therapy with itraconazole may help achieve better survival rates. In future, clinical trials or in vivo animal model studies are essential to understand the efficacy of different antifungal agents against the Emergomyces species and to design treatment guidelines.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jof9101039/s1, Table S1: Clinical manifestations in emergomycosis patients; Table S2: Opportunistic infections in emergomycosis patients; Table S3: Descriptions of skin lesions in emergomycosis patients; Table S4: Radiological findings in emergomycosis patients; Table S5: Antifungal treatment in the emergomycosis patients.
Author Contributions
H.P. and A.S. developed the concept proposal of the study. K.V. and H.P. designed the search terms and protocols of the study. K.V. and D.R.G. extracted the data generated in the study. H.P. and K.V. performed the statistical analysis. H.P. and A.S. wrote the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Institutional Human Ethics Committee, PES Institute of Medical Sciences & Research, Kuppam-517425, Andhra Pradesh, India. The certificate of approval number is PESIMSR/IHEC/C-143/2023 dated 04-09-2023.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in the article or in Supplementary Materials.
Acknowledgments
We acknowledge the following authors for sharing the species identification and the genes used for identification of Emergomyces species. We thank Nelesh P. Govender, Centre for Healthcare-associated infections, Antimicrobial Resistance and Mycoses, National Institute for Communicable disease, Division of the National Health Laboratory Services, School of Pathology, Faculty of Health Sciences, University of the Witwatersrand, Johannesburg, South Africa. We thank Ilan S. Schwartz, Department of Medicine, Duke University School of Medicine, Durham, North Carolina, The United States of America. We thank Brian Eley, Department of Paediatrics and Child Health, University of Cape Town, Cape Town, South Africa.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Jiang, Y.; Dukik, K.; Muñoz, J.F.; Sigler, L.; Schwartz, I.S.; Govender, N.P.; Kenyon, C.; Feng, P.; van den Ende, B.G.; Stielow, J.B.; et al. Phylogeny, ecology and taxonomy of systemic pathogens and their relatives in Ajellomycetaceae (Onygenales): Blastomyces, Emergomyces, Emmonsia, Emmonsiellopsis. Fungal Divers. 2018, 90, 245–291. [Google Scholar] [CrossRef]
- Dukik, K.; Muñoz, J.F.; Jiang, Y.; Feng, P.; Sigler, L.; Stielow, J.B.; Freeke, J.; Jamalian, A.; Gerrits van den Ende, B.; McEwen, J.G.; et al. Novel taxa of thermally dimorphic systemic pathogens in the Ajellomycetaceae (Onygenales). Mycoses 2017, 60, 296–309. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Tsui, C.K.M.; Ahmed, S.A.; Hagen, F.; Shang, Z.; Gerrits van den Ende, A.H.G.; Verweij, P.E.; Lu, H.; de Hoog, G.S. Intraspecific Diversity and Taxonomy of Emmonsia crescens. Mycopathologia 2020, 185, 613–627. [Google Scholar] [CrossRef]
- Samaddar, A.; Sharma, A. Emergomycosis, an Emerging Systemic Mycosis in Immunocompromised Patients: Current Trends and Future Prospects. Front. Med. 2021, 8, 670731. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, I.S.; Govender, N.P.; Sigler, L.; Jiang, Y.; Maphanga, T.G.; Toplis, B.; Botha, A.; Dukik, K.; Hoving, J.C.; Muñoz, J.F.; et al. Emergomyces: The global rise of new dimorphic fungal pathogens. PLoS Pathog. 2019, 15, e1007977. [Google Scholar] [CrossRef]
- Mapengo, R.E.; Maphanga, T.G.; Grayson, W.; Govender, N.P. Endemic mycoses in South Africa, 2010-2020: A decade-long description of laboratory-diagnosed cases and prospects for the future. PLoS Negl. Trop. Dis. 2022, 16, e0010737. [Google Scholar] [CrossRef]
- Ibe, C.; Mnyambwa, N.P.; Mfinanga, S.G. Emergomycosis in Africa: Time to Pay Attention to This Emerging Deadly Fungal Infection. Int. J. Gen. Med. 2023, 16, 2313–2322. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Lerm, B.; Hoving, J.C.; Kenyon, C.; Horsnell, W.G.; Basson, W.J.; Otieno-Odhiambo, P.; Govender, N.P.; Colebunders, R.; Botha, A. Emergomyces africanus in Soil, South Africa. Emerg. Infect. Dis. 2018, 24, 377–380. [Google Scholar] [CrossRef]
- Peterson, S.W.; Sigler, L. Molecular genetic variation in Emmonsia crescens and Emmonsia parva, etiologic agents of adiaspiromycosis, and their phylogenetic relationship to Blastomyces dermatitidis (Ajellomyces dermatitidis) and other systemic fungal pathogens. J. Clin. Microbiol. 1998, 36, 2918–2925. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Govender, N.P.; Corcoran, C.; Dlamini, S.; Prozesky, H.; Burton, R.; Mendelson, M.; Taljaard, J.; Lehloenya, R.; Calligaro, G.; et al. Clinical Characteristics, Diagnosis, Management, and Outcomes of Disseminated Emmonsiosis: A Retrospective Case Series. Clin. Infect. Dis. 2015, 61, 1004–1012. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.; Rutjes, A.W.S.; Reitsma, J.B.; Bossuyt, P.M.M.; Kleijnen, J. The development of QUADAS: A tool for the quality assessment of studies of diagnostic accuracy included in systematic reviews. BMC Med. Res. Methodol. 2003, 3, 25. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Barker, T.H.; Moola, S.; Tufanaru, C.; Stern, C.; McArthur, A.; Stephenson, M.; Aromataris, E. Methodological quality of case series studies: An introduction to the JBI critical appraisal tool. JBI Evid. Synth. 2020, 18, 2127–2133. [Google Scholar] [CrossRef] [PubMed]
- Wellinghausen, N.; Kern, W.V.; Haase, G.; Rozdzinski, E.; Kern, P.; Marre, R.; Essig, A.; Hetzel, J.; Hetzel, M. Chronic granulomatous lung infection caused by the dimorphic fungus Emmonsia sp. Int. J. Med. Microbiol. 2003, 293, 441–445. [Google Scholar] [CrossRef]
- Dot, J.-M.; Debourgogne, A.; Champigneulle, J.; Salles, Y.; Brizion, M.; Puyhardy, J.M.; Collomb, J.; Plénat, F.; Machouart, M. Molecular diagnosis of disseminated adiaspiromycosis due to Emmonsia crescens. J. Clin. Microbiol. 2009, 47, 1269–1273. [Google Scholar] [CrossRef]
- Pelegrín, I.; Ayats, J.; Xiol, X.; Cuenca-Estrella, M.; Jucglà, A.; Boluda, S.; Fernàndez-Sabé, N.; Rafecas, A.; Gudiol, F.; Cabellos, C. Disseminated adiaspiromycosis: Case report of a liver transplant patient with human immunodeficiency infection, and literature review. Transpl. Infect. Dis. 2011, 13, 507–514. [Google Scholar] [CrossRef]
- Pelegrín, I.; Alastruey-Izquierdo, A.; Ayats, J.; Cuenca-Estrella, M.; Cabellos, C. A second look at Emmonsia infection can make the difference. Transpl. Infect. Dis. 2014, 16, 519–520. [Google Scholar] [CrossRef]
- Kenyon, C.; Bonorchis, K.; Corcoran, C.; Meintjes, G.; Locketz, M.; Lehloenya, R.; Vismer, H.F.; Naicker, P.; Prozesky, H.; van Wyk, M.; et al. A Dimorphic Fungus Causing Disseminated Infection in South Africa. N. Engl. J. Med. 2013, 369, 1416–1424. [Google Scholar] [CrossRef]
- Fielli, M.; Ceccato, A.; Capece, P.; Posse, G.; Monteverde, A.; Gonzalez, A. Human Adiaspiromycosis: A Case from Argentina. Chest 2013, 144, 220A. [Google Scholar] [CrossRef]
- van Hougenhouck-Tulleken, W.G.; Papavarnavas, N.S.; Nel, J.S.; Blackburn, L.Y.; Govender, N.P.; Spencer, D.C.; Lippincott, C.K. HIV-associated disseminated emmonsiosis, Johannesburg, South Africa. Emerg. Infect. Dis. 2014, 20, 2164–2166. [Google Scholar] [CrossRef]
- Heys, I.; Taljaard, J.; Orth, H. An Emmonsia species causing disseminated infection in South Africa. N. Engl. J. Med. 2014, 370, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Feng, P.; Yin, S.; Zhu, G.; Li, M.; Wu, B.; Xie, Y.; Ma, H.; Zhang, J.; Cheng, C.; de Hoog, G.S.; et al. Disseminated infection caused by Emmonsia pasteuriana in a renal transplant recipient. J. Dermatol. 2015, 42, 1179–1182. [Google Scholar] [CrossRef] [PubMed]
- Lochan, H.; Naicker, P.; Maphanga, T.; Ryan, A.; Pillay, K.; Govender, N.P.; Eley, B. A case of emmonsiosis in an HIV-infected child. South. Afr. J. HIV Med. 2015, 16, 2–5. [Google Scholar] [CrossRef] [PubMed]
- Mutyaba, A.; Sonderup, M.W.; Locketz, M.; Okpechi, I.; Spearman, C.W.; Tooke, A. Disseminated Emmonsia in an HIV-HBV co-infected man. IDCases 2015, 2, 35–36. [Google Scholar] [CrossRef]
- Tang, X.H.; Zhou, H.; Zhang, X.Q.; De Han, J.; Gao, Q. Cutaneous Disseminated Emmonsiosis Due to Emmonsia pasteuriana in a Patient with Cytomegalovirus Enteritis. JAMA Dermatol. 2015, 151, 1263–1264. [Google Scholar] [CrossRef]
- Malik, R.; Capoor, M.R.; Vanidassane, I.; Gogna, A.; Singh, A.; Sen, B.; Rudramurthy, S.M.; Honnavar, P.; Gupta, S.; Chakrabarti, A. Disseminated Emmonsia pasteuriana infection in India: A case report and a review. Mycoses 2016, 59, 127–132. [Google Scholar] [CrossRef]
- Wang, P.; Kenyon, C.; de Hoog, S.; Guo, L.; Fan, H.; Liu, H.; Li, Z.; Sheng, R.; Yang, Y.; Jiang, Y.; et al. A novel dimorphic pathogen, Emergomyces orientalis (Onygenales), agent of disseminated infection. Mycoses 2017, 60, 310–319. [Google Scholar] [CrossRef]
- Koneru, H.; Penupolu, S. Pulmonary Adiaspiromycosis: An Emerging Fungal Infection. Chest 2017, 152, A162. [Google Scholar] [CrossRef]
- Crombie, K.; Spengane, Z.; Locketz, M.; Dlamini, S.; Lehloenya, R.; Wasserman, S.; Maphanga, T.G.; Govender, N.P.; Kenyon, C.; Schwartz, I.S. Paradoxical worsening of Emergomyces africanus infection in an HIV-infected male on itraconazole and antiretroviral therapy. PLoS Negl. Trop. Dis. 2018, 12, e0006173. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Sanche, S.; Wiederhold, N.P.; Patterson, T.F.; Sigler, L. Emergomyces canadensis, a Dimorphic Fungus Causing Fatal Systemic Human Disease in North America. Emerg. Infect. Dis. 2018, 24, 758–761. [Google Scholar] [CrossRef]
- Gast, K.B.; van der Hoeven, A.; de Boer, M.G.J.; van Esser, J.W.J.; Kuijper, E.J.; Verweij, J.J.; van Keulen, P.H.J.; van der Beek, M.T. Two cases of Emergomyces pasteurianus infection in immunocompromised patients in the Netherlands. Med. Mycol. Case Rep. 2019, 24, 5–8. [Google Scholar] [CrossRef] [PubMed]
- Moodley, A.; Mosam, A.; Govender, N.P.; Mahabeer, Y.; Chateau, A.V. Emergomyces africanus: The Mimicking Fungus. Dermatopathology 2019, 6, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Rooms, I.; Mugisha, P.; Gambichler, T.; Hadaschik, E.; Esser, S.; Rath, P.-M.; Haase, G.; Wilmes, D.; McCormick-Smith, I.; Rickerts, V. Disseminated Emergomycosis in a Person with HIV Infection, Uganda. Emerg. Infect. Dis. 2019, 25, 1750–1751. [Google Scholar] [CrossRef] [PubMed]
- Capoor, M.R.; Mishra, N.; Kolte, S.; Singla, G.; Gogna, A.; Rudramurthy, S.; Prakash, H.; Chakrabarti, A. Disseminated Emergomyces pasteurianus Infection in India: A Case Report and a Review. Mycopathologia 2020, 185, 193–200. [Google Scholar] [CrossRef]
- Chik, K.K.; To, W.K. Autochthonous Emergomyces pasteurianus pneumonia in an immunocompromised patient in Hong Kong: A case report. Hong Kong Med. J./Xianggang Yi Xue Za Zhi 2020, 26, 446–448. [Google Scholar] [CrossRef]
- He, D.; Quan, M.; Zhong, H.; Chen, Z.; Wang, X.; He, F.; Qu, J.; Zhou, T.; Lv, X.; Zong, Z. Emergomyces orientalis Emergomycosis Diagnosed by Metagenomic Next-Generation Sequencing. Emerg. Infect. Dis. 2021, 27, 2740–2742. [Google Scholar] [CrossRef]
- Kuzyk, A.C.; Burbidge, T.; Mydlarski, P.R. Cutaneous Emmonsia infection in a renal transplant recipient. JAAD Case Reports 2021, 11, 44–46. [Google Scholar] [CrossRef]
- Mah, J.; Bakker, A.; Tseng, C.; Lafay-Cousin, L.; Kuhn, S.; Brundler, M.-A.; Lisboa, L.F. Isolated Pulmonary Emergomycosis in an Immunocompetent Patient in Alberta, Canada. Open Forum Infect. Dis. 2022, 9, ofac021. [Google Scholar] [CrossRef]
- Schwartz, I.S.; McLoud, J.D.; Berman, D.; Botha, A.; Lerm, B.; Colebunders, R.; Levetin, E.; Kenyon, C. Molecular detection of airborne Emergomyces africanus, a thermally dimorphic fungal pathogen, in Cape Town, South Africa. PLoS Negl. Trop. Dis. 2018, 12, e0006174. [Google Scholar] [CrossRef]
- Wheat, L.J.; Freifeld, A.G.; Kleiman, M.B.; Baddley, J.W.; McKinsey, D.S.; Loyd, J.E.; Kauffman, C.A. Infectious Diseases Society of America Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 807–825. [Google Scholar] [CrossRef]
- Chapman, S.W.; Dismukes, W.E.; Proia, L.A.; Bradsher, R.W.; Pappas, P.G.; Threlkeld, M.G.; Kauffman, C.A. Infectious Diseases Society of America Clinical practice guidelines for the management of blastomycosis: 2008 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2008, 46, 1801–1812. [Google Scholar] [CrossRef]
- Kauffman, C.A.; Bustamante, B.; Chapman, S.W.; Pappas, P.G. Infectious Diseases Society of America Clinical practice guidelines for the management of sporotrichosis: 2007 update by the Infectious Diseases Society of America. Clin. Infect. Dis. 2007, 45, 1255–1265. [Google Scholar] [CrossRef]
- Dukik, K.; Al-Hatmi, A.M.S.; Curfs-Breuker, I.; Faro, D.; de Hoog, S.; Meis, J.F. Antifungal Susceptibility of Emerging Dimorphic Pathogens in the Family Ajellomycetaceae. Antimicrob. Agents Chemother. 2018, 62, 1–6. [Google Scholar] [CrossRef]
- Maphanga, T.G.; Britz, E.; Zulu, T.G.; Mpembe, R.S.; Naicker, S.D.; Schwartz, I.S.; Govender, N.P. In Vitro Antifungal Susceptibility of Yeast and Mold Phases of Isolates of Dimorphic Fungal Pathogen Emergomyces africanus (Formerly Emmonsia sp.) from HIV-Infected South African Patients. J. Clin. Microbiol. 2017, 55, 1812–1820. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).