Abstract
Repetitive movements and the speed of upper limbs increase the risk of musculoskeletal disorders. This study aimed to analyse the risk of shoulder injuries in repetitive tasks by evaluating the humerus angle, angular velocity, and angular acceleration during simulated chicken wing cutting. The study was conducted in a laboratory simulating a real environment. Thirty-six healthy right-handed volunteers were assessed using an electromagnetic tracking device, TrakSTAR, integrated with MotionMonitor™ (Innovative Sports Training, Inc. Chicago, IL) and software to collect 3-D kinematic data developed in the research centre. The equipment measured the angles performed by the upper limbs during the entire movement. The humerus angles were automatically transformed into angular velocity (°·s−1) and angular acceleration (°·s−2). Maximum angular velocities were 27.39°·s−1 (men, right humerus) and 22.39°·s−1 (women, left humerus), both below the safe limit. Maximum accelerations were 25.32°·s−2 (men, left side) and 28.94°·s−2 (women, left side); safety values for these accelerations are not established. Monotony is a risk factor, especially for the dominant side. Future studies should evaluate risk factors simultaneously in repetitive tasks. Repetitiveness exceeds the safe limit according to the OCRA method.
1. Introduction
1.1. Assessment in the Slaughterhouse Industry
Work-related musculoskeletal disorders (WRMSD) represent about 40% of work diseases [1], and the upper limbs are the most affected body parts [2]. Manual material handling (MMH), usually in industries [1], increases the risk of WRMSD [3] due to exhaustion at work [4]. Activities in the slaughterhouse industry demand repetitive upper limb movements throughout the workday. Monotony, inappropriate postures, and environmental conditions increase the risk of upper-limb WRMSD [2].
Arm movements involve the angular velocity and acceleration of the shoulder joint. Increased velocity of upper arms during tasks is associated with shoulder illnesses [1]. Variations in acceleration affect velocity, which directly influences kinetic energy and applied force [2], potentially increasing the risk of musculoskeletal disorders (MSD).
1.2. Causes of Musculoskeletal Disorders in Manufacturing Industries
Awkward postures, repetitive movements [5] with more than 25 lifts per day [3], and heavy manual handling [5] are significant physical stressors. Also, heavy physical work [6], with loads greater than 25 kg [3], elevated arms for an extended period [5], shoulder elevation above 60° [7], and high velocities of upper limbs increase the incidence of shoulder disorders [5]. Repeated muscle activation may also cause microtrauma, impairing movement control [8]. Physically demanding tasks are known to be associated with occupational injuries [9]. Manual material handling increases the incidence of MSD, and its associated costs [1] represent up to 40% of occupational costs [10,11,12]. Repetitiveness and force applied at work should be evaluated to minimise eventual worker illnesses [13].
Excessive tiredness is usually felt at the end of the working day, and adequate rest is vital to restore energy for another entire workday [3]. A healthy and rested musculoskeletal system can perform maximal voluntary muscular actions, which produce the strength needed for the tasks. A partially fatigued muscle has a reduced capacity [14], affecting cognitive performance [15]. The postural compensation modifies the articular angles [16] and requires the employee to adopt inappropriate and awkward postures. The adoption of this posture is a reality in static and repetitive work, increasing the risk of WRMSD [5] due to repetitive strain injuries or cumulative trauma disorders [17,18,19,20].
1.3. Shoulder Illnesses
Shoulder pain is the third most common WRMSD [21,22], affecting 21% of the population [7]. This syndrome is originated mainly due to repetitive and risen movements (>60°) [7,23]. Individuals affected by shoulder pain are mostly ageing, married, and working women [24]. It is noticeable that employees in the slaughterhouse industry are greatly affected by shoulder illnesses, mainly women. According to the European Agency for Safety and Health [25], obesity increases the risk by 20%. Rotator cuff syndrome (RCS) is the most common illness of the joint, treated with conservative treatment, with no surgery, in 88% of cases. It is ineffective for 58% of workers, requiring surgery [22]. Concerning gender, females are the most affected by upper limb WRMSD [2]. Incidence of WRMSD was evaluated in 14.8% and 12.6% in Australia, 42% and 35.9% in Canada [26], 75% and 57% [27], 39% and 21% [28], 42% and 30% [29] in women and men, respectively. The European Agency for Safety and Health at Work stated that female workers’ complaints are significantly higher than male, mainly chronic WRMSD disorders [30]. Female muscle activity is higher, while males have greater muscle strength [3]. Biological features like muscle composition may elucidate the higher male force [2]. Kranz [3] stated that strength influences lifting tasks more than gender. Loads adjusted to the individual’s strength end the difference in lifting strategy and may benefit the employee. Hazard control in the company is vital in reducing potential illnesses [31].
1.4. Evaluation of Slaughterhouse Task
The research assessed the slaughterhouse industry’s upper limb movements due to the high incidence of shoulder injury. Potential risk factors were measured in the laboratory, simulating real conditions. Employees manipulate over ten chickens per minute, stressing identical muscle groups. The main factors contemplated were repetitiveness, humerus elevation, angular velocity, and angular acceleration. The real motives of upper limb disorders must be known to minimise the risk. The research assessed the movements of the upper limb while simulating cutting the wing of a chicken, which is a real task in a slaughterhouse. Results are given in angles and frames (time) and converted into angular velocities and angular accelerations through an algorithm developed specifically for this purpose. The experimental work and data collection took place in a laboratory. This allowed for greater control over the entire trial, namely the minimisation of data variability and easier instrumentation of the subjects while performing the tasks. In addition, biases arising from using accelerometers and inertial centres in an environment full of metal were avoided.
The study’s main goal is to assess the maximum humeral elevation, angular velocity, and angular acceleration of the humerus while performing the task, comparing the results with established safe values from biomechanics and ergonomics perspectives.
2. Materials and Methods
The evaluation was made in the Universidade Federal de São Carlos (UFSCar)—Physiotherapy Department—Shoulder Laboratory, located in São Carlos, Estate of São Paulo, Brazil.
2.1. Subjects
Thirty-six volunteers (18 female and 18 male), healthy and right handed, aged between 20 and 35 years (average age 25.4 years, standard deviation 3.5), were selected. For inclusion criteria, individuals should be sedentary, with a maximum 25 Body Mass Index (BMI) (average BMI 23.1, standard deviation 3.1), without a history of shoulder disorder or surgery, and without shoulder pain. Participants with upper limb abnormality or amputation were excluded. Each volunteer was informed about the research objectives and, upon agreeing to participate, signed an informed consent by resolution 466/2012 of the National Health Council (CNS). The project was submitted and approved by the Research Ethics Committee of UFSCar nº 63256222.3.0000.5504, approved on 5 November 2022.
2.2. Data Collection Procedures
Subjects were submitted to the kinematic evaluation process of the shoulder joint complex. Electromagnetics sensors were used for the assessment. At the beginning of the evaluation, volunteers were aware of the simulated tasks and could have water, rest, and quit the research anytime.
2.3. Data Collection Instruments
2.3.1. Setup Subject Sensors
The program is oriented to digitise each point using a centroid related to segment endpoints’ location and axes. Regarding the location of spine joint centres, the motion monitor assumes that sensors are close to joint centres. Each subject’s body mass and height are manually inserted into the program (computer) to better recognise the body structure.
2.3.2. Kinematic Evaluation and Intersegmental Coordination
A six-degree-of-freedom electromagnetic tracking device, the TrakSTAR (Ascension Technology Corporation, Burlington, ON, Canada), integrated with MotionMonitor® software (Innovative Sports Training, Inc., Chicago, IL, USA), was used to collect 3-D kinematic data [32]. The transmitter produces an electromagnetic field that induces current in the sensors with three orthogonal coils. Each sensor’s position and 3-D orientation were tracked simultaneously, with a sampling frequency of 100 Hz. System root means square accuracy is 0.5° for orientation and 0.18 cm for position in a metal-free environment at 76 cm away from the transmitter. The sensors measure 1.8 × 0.8 × 0.8 cm, one of which is connected to a tip (stylus) for digitising anatomical points and building the joint coordinate system.
The subjects were positioned in an orthostatic position, with arms relaxed at the side of the body (Figure 1). The transmitter was placed directly behind the shoulders, at the level of the scapular spine (Figure 2).
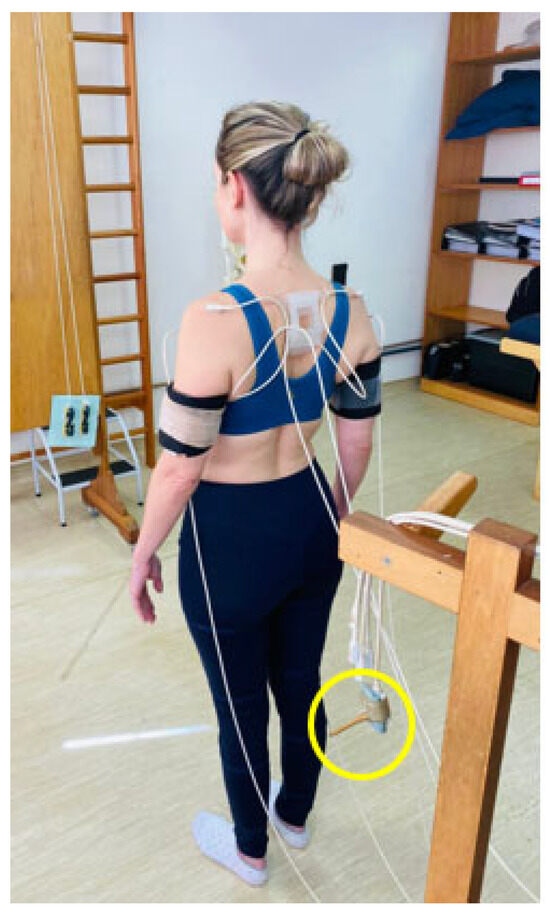
Figure 1.
Sensors placed on the body of a subject.
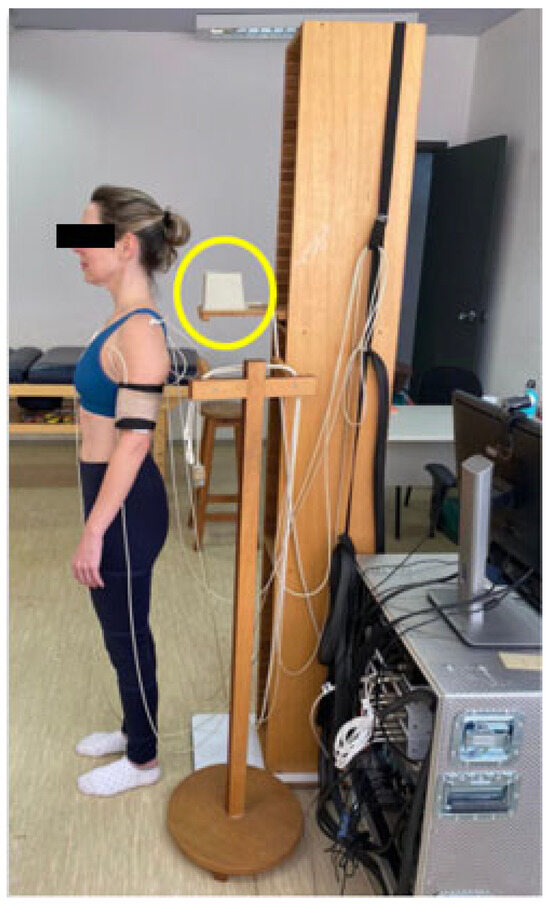
Figure 2.
Transmitter behind the subject.
Sensor #1 is connected to a wooden tip (yellow circle in Figure 1) with known displacements to digitise the anatomical landmarks needed to build the joint coordinate systems. Three electromagnetic sensors were attached with double-sided adhesive tape to the sternum, to the acromion of the scapula, and to a thermoplastic cuff attached to the distal humerus to track humeral movement, as in previous studies [33]. A difference of more than 5° in more than one scapular movement in the relaxed position was attributed to sensor movement, as a 5° change would be greater than any expected measurement error based on a previous study [34]. Digitising involves bringing the tip to the location of the palpated reference point and digitally recording the 3-D coordinate locations relative to the respective segment sensor. Chest landmarks included the sternal notch, C7 spinous process, T8 spinous process, and xiphoid process. Scapular landmarks included the root of the vertebral column, the posterolateral acromion, and the inferior angle of the scapula. Humeral landmarks included the lateral and medial epicondyles. The centre of the humeral head was estimated by passively moving the arm through short arcs (less than 45°) to define the pivot point [35]. Local coordinate systems were established for the trunk, scapula, and humerus using the digitised reference points, following the protocol recommended by the International Society of Biomechanics [36].
The z-axis was pointed laterally, the x-axis anteriorly, and the y-axis superiorly for data analysis on the right side. The orientation of the axes to the left has changed. The z-axis will be pointed laterally, the x-axis posteriorly, and the y-axis superiorly. These three axes define the cardinal planes of the trunk. The y-axis was formed by the vector joining the midpoints between the spinous process of C7 and the manubrium of the sternum and between the spinous process of T8 and the xiphoid process. The z-axis was directed perpendicularly to the sagittal plane, and the x-axis was perpendicular to the z and y axes.
The z-axis was defined in the plane of the scapula at the root of the scapular spine at the acromial angle to state the scapular axes. The x-axis was directed perpendicular to the plane of the scapula, and the y-axis was perpendicular to the x and z axes. The YXZ sequence was used to describe scapular movements about the trunk. The position of the humerus relative to the trunk was determined using the sequence YX’Y”, according to the protocol setup. The first rotation defined the elevation plane, the second the humeral elevation angle, and the third defined the internal/external rotations. The kinematic analysis was based on scapula orientation data at rest and those measured at angles of 30°, 60°, 90°, and 120° during maximal elevation activity in the sagittal plane.
2.3.3. Recognition of the Sensors in the Body
Based on individual dimensions, the program recognises each marked joint (sternum, acromion, and distal humerus). After placing sensors on the skin, a calibration protocol minimises analysis errors, allowing the program to accurately recognise each volunteer’s body dimensions. During the calibration, Sensor #1 indicates each joint. The protocol calibrates the trunk along the X, Y, and Z axes. After trunk recognition, humeral movements (flexion, extension, adduction, abduction) are performed for both right and left upper limbs. T12/L1 vertebrae and medial and lateral epicondyles are identified for accuracy. Subsequently, the sternum is recognised, marking the T8 and C7 vertebrae and the jugular notch. The right and left scapulae are identified by recognising the scapular spine, acromion angle, inferior angle, and anterior clavicle. Finally, the humeri are identified by recognising the medial and lateral epicondyles.
The program displays the angles of each joint, which can be assessed on the computer display. These angles are analysed according to biomechanical standards. If values are incorrect, a new calibration is performed. If correct, a protocol of movements (neutral position and raised upper limbs) is evaluated to verify the feasibility of these angles. The assessment begins after the complete procedure.
Each volunteer has its joint recognition. Figure 3 shows the body structure of an assessed volunteer. The program permitted the identification of individual characteristics.
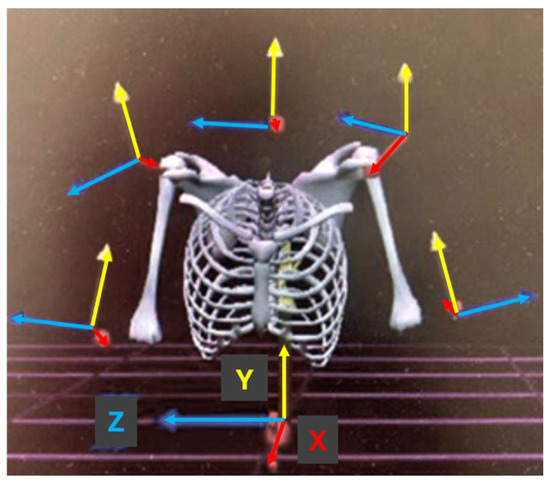
Figure 3.
Recognition of joints.
2.4. Procedure
Repetitive movement of the upper limb simulating the cutting of a chicken wing in a slaughterhouse was assessed. The activity performs humerus elevation with internal/external rotation of the scapula.
Wing cutting section: The employee uses a small knife that is slightly weighted. There is no need to bend or rotate the trunk. Number of raw materials manipulated per minute: 12.5 chickens. Execution: to complete the task, the worker realises two actions (grabbing the wing with the left hand and cutting the wing with the right hand). It results in two actions per chicken: 25 actions per minute.
2.5. Laboratory Simulation
Work settings were verified in a real environment (cadence, furniture dimensions, temperature, humidity, force) to be replicated in the laboratory. The research was conducted as close as possible to reality in a laboratory. The evaluation was not accomplished in a real environment because it is not possible to transport the TrakSTAR equipment (Burlington, ON, Canada), and electromagnetic interferences compromise the results. Some conditions could not be replicated. The laboratory temperature was not controlled. In the workplace, weather conditions are controlled. The environment is cold (temperature around 10 °C) and humid (around 80% humidity), so the product does not perish. In the laboratory, the air conditioner was turned on at the beginning of the setup and was turned off for the research because signal interference occurred. Male volunteers remained shirtless, and women wore a top to connect the sensors to the skin. In the industry, workers wear specific safety clothes. However, the development of the activity, as dimensions on the desktop, applied force to cut the wing, cadence, were similar to the reality.
2.6. Cutting Wing Sector
Simulating the cutting of a wing used a theraband green—professional resistance bands—heavy resistance. Values: Increase from preceding colour at 100% at elongation (25%); Resistance in pounds at 100% elongation (4.6 lbs); Resistance in kilograms at 100% elongation (2.1 kg or 25% of increasing resistance). The resistance of the elastic band is based on the amount it can be stretched, which is measured in pounds or kilograms of force. Two strips were tied on the wooden board, given a resistance of (1300/1400 kg), which was the resistance the volunteers should overcome to displace the wing and cut the wing. The force was measured with a handheld dynamometer (KA—B111, Shenzhen PLS Electronics Co., Ltd., Shenzhen, China). The strips were placed in the subject’s centre of gravity, pulling the strips with the left hand and “cutting” the strips with the dominant hand, using a small knife with slight weight. The knife had a protective cover, avoiding cutting the strips and accidents with the volunteer. The resistance of the strips was close to the value of the displacement of the wing. Real chickens (dead chickens) were hanged by rope on their feet to achieve their values. The displacement and cutting of the wing’s resistance were measured using the same dynamometer.
Figure 4 illustrates the measurement of the simulating chicken wing, which was realised in every evaluation. Figure 5 illustrates the simulation of the chicken wing. In the figure, the volunteer displaces the chicken with the right hand and cuts it with the left hand (the model is the left hand).

Figure 4.
Measuring the pressure of theraband.
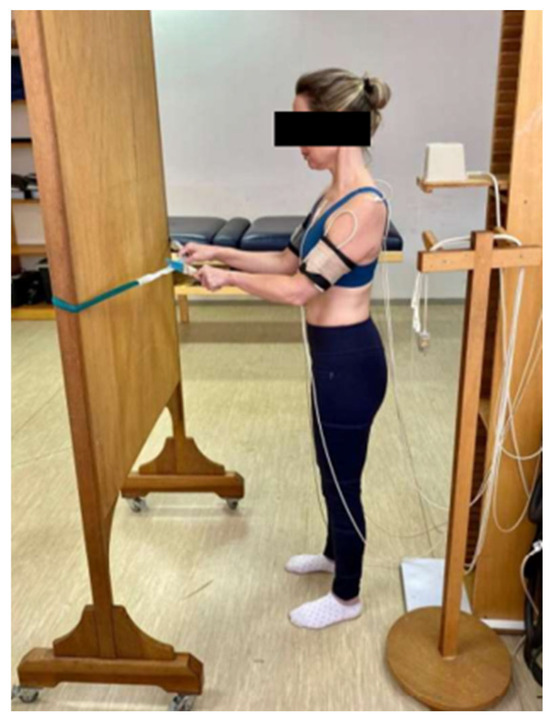
Figure 5.
Simulating cutting the wing.
2.7. Electromagnetic System
Positions are chased by an electromagnetic transmitter that detects the position and orientation of the sensors attached to the skin [37]. It is a six-degrees-of-freedom measuring device to track the three-dimensional (3D) orientation [38]. Electromagnetic data of the scapula, in defining the position and orientation, are consistent [39], even though the joint realises great movements as the scapula slides and rotates under layers of soft tissue [37].
The equipment has high accuracy [40] but also limitations. It is vulnerable to magnetic interference [38,39], and reliability reduces as the distance between the electromagnetic field and the sensors increases [41].
2.8. Data Analysis and Statistics
Biomechanics analysis was performed to measure shoulder kinematics. The movement was recorded during the entire cycle, allowing the detection of the humerus elevation at each frame. The program extracts raw data of the angles (degrees) performed by the shoulder joint and frames (time). To evaluate the data, an algorithm was developed to convert the angles and frames into maximum humerus angles (°), angular velocities (°·s−1), and angular accelerations (°·s−2). A window size of ten frames was used to calculate it, five behind and five ahead, characterising 1 s. The program averaged these ten frames (1 s) for all calculations to achieve the greatest effort.
Data processing was done using Python language and Pandas library, an open-source data analysis and manipulation tool. An API developed using Falcon Framework, a minimalist framework for building mission-critical REST APIs and microservices, was also built to integrate the data processing components into a visualisation tool. The visualisation tool was built using React, a library for web and native user interfaces, with JavaScript language.
The data processing components found all peak values of humerus angles (°) within a recording. The angular velocity (°·s−1) was calculated by dividing the difference between two subsequent angle measurements, in degrees, by the fixed measurement rate between frames, in seconds. The angular acceleration (°·s−2) was calculated by dividing the difference between two subsequent angular velocities calculations, in degrees per second, by the fixed measurement rate, in seconds.
Statistics are achieved by measuring joint centre positions and joint trajectories quantified by degrees (°), angular velocity (°·s−1), and angular acceleration (°·s−2). The moment in which arms have maximum effort was selected considering both the maximum elevation angle of the humerus combined with the maximum angular velocity and the maximum elevation angle of the humerus and maximum angular acceleration. It must be highlighted that the peak of the humerus angle was not considered, as it reflects the moment the arm changes the trajectory. Angular acceleration and velocity are zero on the peak of the angle.
The assessment considered the higher values achieved individually by the volunteers compared with safe pattern values. It also assessed the moment of the movement at which the maximum velocity and acceleration were achieved. The analysis was made according to the dominant and non-dominant sides, and genders were evaluated separately. For the statistical analysis, the Mann–Whitney test, IC 95% (p < 0.05) was used. It is a non-parametric statistical test that compares the two independent groups and non-normal data. The statistic provides an analysis of differences between the assessed groups and permits reliable outcomes with a small sample. It used the program named Jamovi 2.3.28, especially to compare dominant and non-dominant sides and genders.
2.9. OCRA Method
The OCRA Checklist method allows the evaluation of the risk factors of upper limb musculoskeletal disorders [4]. According to Colombini and Ochipinti [4], the method contemplates assessing risk factors. The method may be used for all sample sizes.
The assessed factors are (a) Force Factor (FMJ). Technical actions involve force measured by the Borg scale (0–10), corresponding to workers’ perceptions. The period of each action (%) was verified to calculate the force. (b) Postural Factor (PM). Shoulders, elbows, wrists, hands, and fingers are individually evaluated based on the cycle of the repetitive task. Both sides were analysed independently. (c) Repetitiveness Factor (ReM). A metronome in iPhone X measured the cadence for two minutes, five times. Confirming the period of each task, workers were filmed for 2 min. The frequency was determined by the number of technical actions performed per minute. (d) Additional Factor (AM), divided into physical-mechanical and organisational conditions. Conditions that may increase the risk of the task. The score was defined as determined by the method. (e) Recovery Periods Factor (Fr). Task duration and distribution of breaks during the working day were collected. The workers performed three breaks of 20 min, distributed after 01:40 h of work, and one hour for lunch/dinner during the journey. (f) Duration Factor (Fd). The total period of the shifts is 450 min (Table 1).

Table 1.
OCRA method (ISO 11228-3).
3. Results
The results of individual performance is illustrated in Figure 6 regarding angular velocity. Each point represents the subjects in the graphs below. Figure 7 shows the overall results of angular velocity and its variations. The maximum angular acceleration of the volunteers is clarified in Figure 8. Figure 9 show the overall evaluation of volunteers concerning angular acceleration. To investigate eventual differences, gender, as well as dominant and non-dominant sides, was evaluated separately.
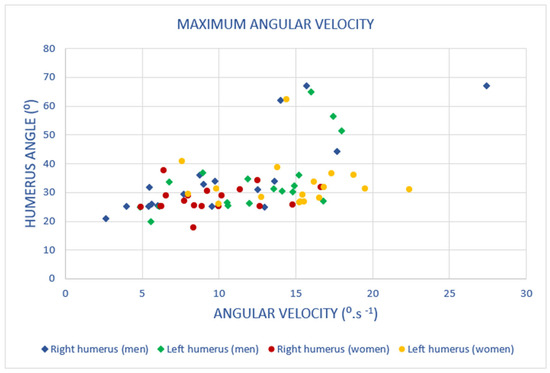
Figure 6.
Scatter plot, maximum angular velocity.
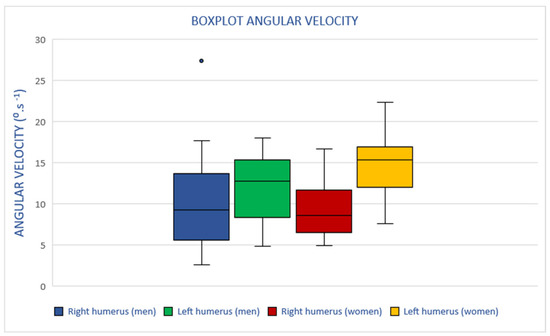
Figure 7.
Boxplot, the maximum angular velocity of humerus.
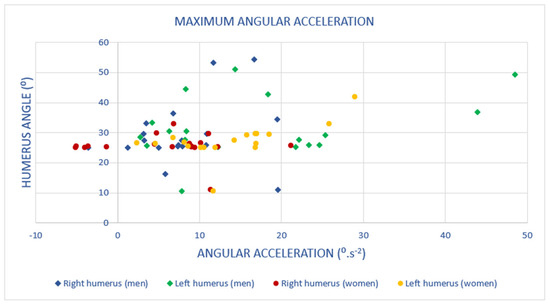
Figure 8.
Scatter plot, maximum angular acceleration.
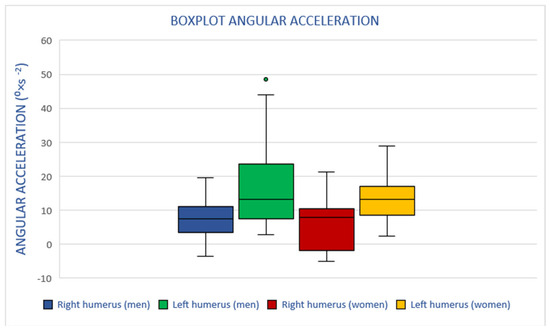
Figure 9.
Boxplot, angular acceleration of humerus.
3.1. Angular Velocity
Humerus elevation and speed are related to MSD. To verify eventual risk, it was assessed the maximum angular velocity and maximum angular acceleration performed by each volunteer and in which humerus elevation the maximum values were achieved.
The higher velocities were mostly performed around 30° arm elevation by men and women on both sides. Figure 6 illustrates the maximum angular velocity of each volunteer and in which humerus elevation was performed.
The maximum angular velocity is mostly performed by the left arm, exhibiting more varied movement patterns.
Some volunteers adopt discrepant patterns. The motivation for the inconsistency of movements was not investigated. Possibly, the task does not demand high arm elevation (<90°), permitting a great range of freedom to execute it.
Figure 7 shows the performance of the sample when analysing differences in velocity among genders.
Men performed the movement with greater variability of humerus velocity than women. The female’s left side achieved greater velocity.
3.2. Angular Acceleration
Figure 8 demonstrates the maximum angular acceleration performed by the volunteers and the corresponding humerus elevation.
The maximum angular acceleration is diverse among volunteers of both genders. It is not possible to establish standard behaviour. However, the dominant side has shown a higher movement pattern and lower angular acceleration.
Also, the maximum angular acceleration is performed close to 30°, demonstrating a correlation with maximum angular velocity.
The performed maximum acceleration is illustrated in Figure 9.
It is not possible to establish an ordinary pattern, but it is clear that discrepancies are greater on the male left side. Both genders realised higher angular accelerations on the non-dominant side.
3.3. ISO 11228-3
During the working day, workers realise monotonous activity. ISO 11228-3 [42] establishes the OCRA method to evaluate the eventual risk of repetitive tasks. Table 1 illustrates the result according to the method. The factors were evaluated according to a real environment.
In the real environment, employees manipulate around 12 chickens per minute, displacing the wing with the non-dominant hand and cutting the same wing with the dominant side. According to the result of the OCRA method, repetitiveness is a risk factor. The safe limit is three wing cuts and six displacements per minute.
3.4. Statistical Differences According to the Mann–Whitney U Test
The Mann–Whitney U test is a statistical tool used to compare two independent non-parametric samples that do not follow a normal distribution. If the p-value is less than the significance level predetermined by the method (0.06), the null hypothesis can be rejected, concluding that there is a significant difference between the samples. Otherwise, there is not enough evidence to reject the null hypothesis.
Statistical divergences between genders, left and right, were made using the Mann–Whitney test. It analysed differences in angles, velocity, accelerations, and force.
Table 2 demonstrates that there is no difference between men and women.
Table 2.
U-Mann–Whitney results concerning the differences between men and women.
3.5. Medical Record and Incidence of Shoulder MSD
Medical records of employees working in the industry in 2017 were analysed. The company has a privacy policy that does not allow obtaining recent medical records. However, the documents of all the employees working in 2017 were evaluated. For statistical analysis, it was separated by sector, gender, and period working in industry (<2 years, 2–5 years, >5 years). The percentage reflects the incidence of shoulder illnesses in workers who previously have or have not worked with demanding or repetitive tasks.
The wing cut sector had around 66% female and 33% male in 2017. The analysis was made using sex analysis of male and female gender, considering the total sample of workers in the sector.
Workers affected by musculoskeletal disorders while working in the cut wing sector (Table 3):
Table 3.
Percentage of men affected by shoulder illnesses.
The incidence of shoulder MSD in the slaughterhouse industry is high. Females are more prone to shoulder injury, although the repetitiveness is still the same for men and women. Also, the movement pattern is not greatly discrepant among genders.
4. Discussion
The equipment used to evaluate was an electromagnetic system (EMS). The acquisition of electromagnetic data has demonstrated that the 3D kinematics of the scapula are reliable in defining joint position and orientation [39]. The method has limitations, as the measurement quality reduces as the distance between the electromagnetic field and the sensors increases [41] and vulnerability to magnetic interference [38,39]. These subjects were carefully avoided.
4.1. Humerus Elevation
The significant differences in humerus angles during the wing cut permit us to conclude that tasks performed close to the centre of gravity and with no weight to lift or carry increase the possibility of a range of movements. Females have shown similar movements on the right side while cutting the wing.
The maximum angular accelerations and maximum angular velocities are greatly performed around 30° of humerus elevation, which is not considered harmful to the body structure.
4.2. Angular Velocity
High velocities of the upper limb predict the risk of injury [5,43,44]. It is associated with almost all shoulder diagnoses [45], increasing tension neck disorder, rotator cuff, and acromioclavicular syndrome, especially in women [45,46]. Establishing limits is important, but there needs to be an agreement regarding maximum velocity and acceleration. Balogh et al. [45] and Dalbøge et al. [47] settled that median upper arm velocity underneath 45°·s−1 is inoffensive for employees. Balogh et al. [45] and Arvidson et al. [46] recommend 60°·s−1 as a healthy limit for upper limb velocity, being repetitive tasks or not [5].
Assessing the angular velocity results, none of the volunteers achieved the standard maximum value (45°·s−1). The maximum velocities were 27.39°·s−1, performed by men in the right humerus and 22.39°·s−1, executed by women in the left humerus (Figure 6). These were the maximum values obtained in simulations. According to Balogh et al. [45] and Dalbøge et al. [47], all the values are harmless and do not justify the incidence of shoulder WRMSD in the slaughterhouse industry. Figure 7 also makes it clear that the highest values achieved by the volunteers were lower than the maximum patterns established by the literature.
Concerning gender, it is impossible to establish who performed higher angular velocity, but the non-dominant side practised higher angular velocities on average.
4.3. Angular Acceleration
Angular acceleration has yet to be broadly studied. There are no established standard safe values, and it is impossible to define whether they are damaging. Angular accelerations are greater for non-dominant hands. It may be justified because the dominant side revealed greater movement control and stability [48]. Maximum accelerations were 25.32°·s−2 (43.95°·s−2 and 48.47°·s−2, outliers) on men’s left arm and 28.94°·s−2 on women’s left side (Figure 8). On average, men executed higher angular acceleration than women (Figure 9).
To cut the chicken wing, the task is performed close to the centre of gravity. Arms have remained relatively high. The maximum angular acceleration is mostly performed close to 30° of humerus elevation and angular velocity. It permits the establishment of a parallel between maximum velocity and acceleration.
If the investigated factors are analysed distinctly, it cannot be said that the task is prone to developing WRMSD. It does not demand high humerus elevation; angular velocity is not considered harmful, and angular acceleration values are not known if it is risky. However, if analysed, maximum angular velocities/accelerations are simultaneous with the maximum humerus angle, eventually increasing the effort and giving rise to WRMSD.
4.4. Repetitive Movements
Repetitive handling is unavoidable in the slaughterhouse industry. The ISO 11228-3 [42] establishes the OCRA method to estimate the risk in repetitive tasks. The method evaluates the factors settled in Table 1 to assess the risk. The work is considered safe if the result is lower than 2.2, low risk if the result is between 2.3 and 3.5, and significant risk if the result is higher than 3.6. The analysis of the OCRA method permitted us to conclude that the results are different for the right and left arms as the movement varies. Using the left arm, the worker displaces wing joints and cuts the same wing with the right hand (all the volunteers are right hand). However, the risk is high for both sides; the right hand shows greater risk than the left arm (7.6, and 4.1, respectively). The period spent performing each action and arm movements vary. The method also recommends three technical (movements) actions for the right hand and six technical actions for the left hand. Knowing that in a real environment, the workers practice over 12 technical actions by each hand per minute, overwork is undeniable. Repetition of movements is a characteristic of the job. Dynamic movements are related to WRMD, affecting muscles, tendons, and nerves [49], intensifying the risk of illnesses. Repetitiveness is a factor of risk, especially for the dominant side. The cadence should be carefully reorganised.
An important factor is that the assembly lines are fixed, and the machine paces cadence. Shoulder movements to complete the tasks cannot be changed. Consequently, solutions to avoid musculoskeletal injuries are challenging.
Regarding gender, both presented variations in movements. Humerus angles of maximum angular accelerations and maximum angular velocities are closer to the maximum humerus elevation for both men and women, which may be a risk factor.
4.5. Shoulder Disorders in a Real Environment
According to the literature, the humerus elevation and the angular velocity are not considered risk factors because the measured values are not harmful. However, the incidence of shoulder musculoskeletal disorders in the slaughterhouse industry is high. The analysed medical records showed a high incidence of shoulder disorders among workers. Table 2 and Table 3 demonstrate that females suffered greatly from shoulder MSD, especially women without previous experience. The statistical analysis did not evaluate differences between genders that justify the higher incidence of shoulder MSD in women.
The force is related to the height. Thus, hand grip strength is higher for males [50]. It may justify a lower incidence of MSD in men.
Potential risk factors for shoulder musculoskeletal disorders in the slaughterhouse industry were assessed due to the high incidence of illnesses. The primary cause is repetitiveness, which overuses the same muscle groups.
4.6. Implications for Practice
The shoulder is a complex structure that needs to be studied, mainly due to the great range of movements. The slaughterhouse industry demands repetitive movements of upper limbs that overwhelm the shoulder complex. The research assessed the humerus elevation, maximum angular velocity and acceleration, and repetitiveness to evaluate the risk factors of shoulder musculoskeletal disorders. It was possible to conclude that the repetition of movements is harmful to the structure. The humerus elevation and the angular velocity are performed below the safe patterns. It was not possible to conclude regarding angular accelerations because there is a lack of standard safe values. However, the incidence of shoulder disorders in the sector is high, which allows us to consider that angular velocity results can be detrimental in repetitive tasks.
The performed angular velocity and angular acceleration, combined with excessive repetitiveness, can be a risk factor for shoulder structure. Joint overuse tends to reduce strength throughout the workday, making it highly sensitive to fluctuations in velocities and accelerations.
The results achieved in this study can be used as a standard for assessments in manufacturing industries. Further studies should estimate maximum safe values of angular velocities and accelerations for repetitive tasks, which are lower than those for occasional movements.
4.7. Limitations
The laboratory allowed simulation of the task but not the environmental conditions. Also, modifications in physical conditions may alter the movements, and the effort while realising the task was not assessed. The human body is sensitive to external and internal factors, which may intensify force or weakness.
It is impossible to conclude whether the angular acceleration is high or low due to the lack of research on standard safe values. Future research should evaluate the maximum angular acceleration for the shoulder joint. Future studies should also evaluate the risk factors simultaneously, i.e., maximum angular velocity/acceleration in arm elevation and repetitive tasks. Individual factors such as physical fitness or the cumulative effects of these factors with the demands of the job also need further study by researchers
Finally, the assessment should be conducted with real workers to confirm the results, even if this requires changing the type of equipment used for data collection.
5. Conclusions
The task demands repetitive movements of the shoulder complex during the workday. The method established by ISO 11228-3 allowed us to conclude that repetition is a risk factor for musculoskeletal disorders. Shoulder angular velocity is lower than the established safe limit, and angular acceleration is not known if it is safe or not due to the lack of pattern values. Humerus elevation is not considered harmful to the body’s structure. Although the lower standardised values of angular velocity and humerus elevation are performed repetitively, they may become harmful if assessed simultaneously. Monotony and overuse of identical muscle groups may be affected by external factors.
The repetitiveness is high and damaging to the shoulder structure. The study is aware of the most significant cause of illnesses, allowing effective interventions to reduce the risk of repetitive movements.
Additionally, the identification of maximum angular acceleration close to the maximum humerus angle emphasises the requirement of ergonomic considerations in task design and worker training. Concerning angular acceleration values, further research is needed to determine the threshold that eventually damages worker safety.
Author Contributions
Conceptualization, A.S.R., I.C. and N.D.; methodology, A.S.R., I.C. and N.D.; formal analysis, N.D., J.S.B. and J.C.G.; investigation A.S.R., I.C., N.D., J.S.B. and J.C.G.; data curation, A.S.R. and I.C.; writing—original draft preparation, A.S.R.; writing—review and editing, J.S.B. and J.C.G.; supervision, N.D., J.S.B. and J.C.G.; project administration, A.S.R., J.S.B. and J.C.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Doctoral Program in Occupational Safety and Health of the University of Porto, grant number demsso.asgmr.PD9986.
Institutional Review Board Statement
The project was submitted and approved by the Research Ethics Committee of UFSCar nº 63256222.3.0000.5504, approved on 5 November 2022.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data will be available, on justified request to the authors.
Acknowledgments
Paula Camargo, https://orcid.org/0000-0002-8961-4353, prcamargo@ufscar.br; permitted the use of the laboratory and participated in the setup of the machine. Melina Haik, https://orcid.org/0000-0002-8703-8356, participated with knowledge of the shoulder complex. Vinicius de Oliveira Peixoto, Computer Engineer, http://lattes.cnpq.br/2491537202160741, accessed on 12 June 2024; vinicius.oliveira.peixoto@gmail.com, that developed the software used for the analysis of data.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Harari, Y.; Bechar, A.; Riemer, R. Workers’ biomechanical loads and kinematics during multiple-task manual material handling. Appl. Ergon. 2020, 83, 102985. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.; Assila, N.; Goubault, E.; Begon, M. Sex differences in upper limb musculoskeletal biomechanics during a lifting task. Appl. Ergon. 2020, 86, 103106. [Google Scholar] [CrossRef]
- Kranz, C.; Lee, K.; Jadhav, P.; Vestlin, L.; Barker, M.; Jacques, A.; Netto, K. Kinematic and perceptual responses in heavy lifting and pulling: Are there differences between males and females? Appl. Ergon. 2021, 90, 103274. [Google Scholar] [CrossRef]
- Lv, X.; Ji, Y.; Que, X.; Qing, T.; Yang, Y. Dual-squeeze effect: How job demands fuel overwork and its consequences in the context of hospitality. Curr. Issues Tour. 2023, 26, 2265–2283. [Google Scholar] [CrossRef]
- Fan, X.; Lind, C.M.; Rhen, I.-M.; Forsman, M. Effects of sensor types and angular velocity computational methods in field measurements of occupational upper arm and trunk postures and movements. Sensors 2021, 21, 5527. [Google Scholar] [CrossRef]
- European Agency for Safety and Health (EU-OSHA). Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU; EU-OSHA: Bilbao, Spain; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Thigpen, C.A.; Padua, D.A.; Michener, L.A.; Guskiewicz, K.; Giuliani, C.; Keener, J.D.; Stergiou, N. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J. Electromyogr. Kinesiol. 2010, 20, 701–709. [Google Scholar] [CrossRef]
- Fong, A.R.; Pipher, Z.R.; Cudlip, A.C.; Holmes, M.W.R. Examining kinematics and muscle activity of the upper extremity while performing cleaning tasks: A pre-post shift evaluation. Int. J. Ind. Ergon. 2023, 93, 103405. [Google Scholar] [CrossRef]
- Antwi-Afari, M.F.; Anwer, S.; Umer, W.; Mi, H.Y.; Yu, Y.; Moon, S.; Hossain, M.U. Machine learning-based identification and classification of physical fatigue levels: A novel method based on a wearable insole device. Int. J. Ind. Ergon. 2023, 93, 103404. [Google Scholar] [CrossRef]
- Moussavi, S.E.; Zare, M.; Mahdjoub, M.; Grunder, O. Balancing high operator’s workload through a new job rotation approach: Application to an automotive assembly line. Int. J. Ind. Ergon. 2019, 71, 136–144. [Google Scholar] [CrossRef]
- Santos, M.R.D.; Mendes, C. Manual therapy and its role in occupational health: Reducing absenteeism and presenteeism by treating chronic pain with spinal manipulation and mobilization in the workplace. Eur. J. Integr. Med. 2020, 35, 101078. [Google Scholar] [CrossRef]
- Crawford, J.O.; Berkovic, D.; Erwin, J.; Copsey, S.M.; Davis, A.; Giagloglou, E.; Woolf, A. Best Practice & Research Clinical Rheumatology Musculoskeletal health in the workplace. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101558. [Google Scholar] [PubMed]
- Arciniega-Rocha, R.P.; Erazo-Chamorro, V.C.; Szabo, G. The Prevention of Industrial Manual Tool Accidents Considering Occupational Health and Safety. Safety 2023, 9, 51. [Google Scholar] [CrossRef]
- Fleck, S.J.; Kraemer, W.J. Fundamentos do Treinamento de Força Muscular, 4th ed.; Human Kinetics: Porto Alegre, Brazil, 2017. [Google Scholar]
- Caldwell, J.A.; Caldwell, J.L.; Thompson, L.A.; Lieberman, H.R. Fatigue and its management in the workplace. Neurosci. Biobehav. Rev. 2019, 96, 272–289. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.C.; Calvin, T.F.; Keir, P.J. Adaptations to isolated shoulder fatigue during simulated repetitive work. Part II: Recovery. J. Electromyogr. Kinesiol. 2016, 29, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Maciukiewicz, J.M.; Lang, A.E.; Vidt, M.E.; Grenier, S.G.; Dickerson, C.R. Characterization of cashier shoulder and low back muscle demands. Int. J. Ind. Ergon. 2017, 59, 80–91. [Google Scholar] [CrossRef]
- McDonald, A.C.; Mulla, D.M.; Keir, P.J. Using EMG Amplitude and Frequency to Calculate a Multimuscle Fatigue Score and Evaluate Global Shoulder Fatigue. Hum. Factors 2018, 61, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, V.S.; Devalkar, R.V. Postural analysis of building construction workers using ergonomics. Int. J. Constr. Manag. 2019, 19, 464–471. [Google Scholar] [CrossRef]
- Acaröz, S.; Sahin, U.K.; Akoglu, S. The investigation of work-related musculoskeletal disorders among female workers in a hazelnut factory: Prevalence, working posture, work-related and psychosocial factors. Int. J. Ind. Ergon. 2019, 74, 102838. [Google Scholar] [CrossRef]
- Lucas, J.; van Doorn, P.; Hegedus, E.; Lewis, J.; van der Windt, D. A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet. Disord. 2022, 23, 1073. [Google Scholar] [CrossRef]
- Prado, W.; Azevedo, V.; de Lucca, S.R.; Bandini, M. Shoulder arthralgia: Case study of the Occupational Medicine clinic of Universidade Estadual de Campinas (Unicamp). Revista Brasileira de Medicina do Trabalho 2022, 20, 555–562. [Google Scholar] [CrossRef]
- Bodin, J.; Ha, C.; Sérazin, C.; Descatha, A.; Leclerc, A.; Goldberg, M.; Roquelaure, Y. Effects of individual and work-related factors on incidence of shoulder pain in a large working population. J. Occup. Health 2012, 54, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Fayão, J.G.; Libardoni, T.d.C.; Martins, J.; Souza, C.d.S.; de Oliveira, A.S. Queixas musculoesqueléticas no ombro: Características dos usuários e dos atendimentos na atenção primária. Fisioter. Pesqui. 2019, 26, 78–84. [Google Scholar] [CrossRef]
- EU-OSHA. Lesões musculosqueléticas. In Agencia Nacional para a Segurança e Saúde no Trabalho; EU-OSHA: Bilbao, Spain, 2019; Available online: https://osha.europa.eu/pt/themes/musculoskeletal-disorders (accessed on 12 June 2024).
- Macpherson, R.A.; Lane, T.J.; Collie, A.; McLeod, C.B. Age, sex, and the changing disability burden of compensated work-related musculoskeletal disorders in Canada and Australia. BMC Public Health 2018, 18, 758. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.R.; Serra, M.V.G.B.; de Almeida, L.B.; Villela, W.V.; Scalon, J.D.; Quemelo, P.R.V. Symptoms and risks for musculoskeletal disorders among male and female footwear industry workers. Int. J. Ind. Ergon. 2015, 48, 110–116. [Google Scholar] [CrossRef]
- Troelstra, A.S.; Straker, L.; Harris, M.; Brown, S.; der Beek, A.J.V.; Coenen, P. Multimorbidity is common among young workers and related to increased work absenteeism and presenteeism: Results from the population–based Raine Study cohort. Scand. J. Work. Environ. Health 2020, 46, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Pensola, T.; Haukka, E.; Kaila-kangas, L.; Neupane, S.; Leino-Arjas, P. Good work ability despite multisite musculoskeletal pain? A study among occupationally active Finns. Scand. J. Public Health 2016, 44, 300–310. [Google Scholar] [CrossRef] [PubMed]
- De Kok, J.; Vroonhof, P.; Snijders, J.; Roullis, G.; Clarke, M.; Peereboom, K.; Isusi, I. Work-related musculoskeletal disorders: Prevalence, costs and demographics in the EU; 2019. Available online: https://osha.europa.eu/es/publications/ (accessed on 12 June 2024).
- Halliday, B.; Van der Laan, L.; Raineri, A. Prioritizing Work Health, Safety, and Wellbeing in Corporate Strategy: An Indicative Framework. Safety 2023, 10, 18. [Google Scholar] [CrossRef]
- Meskers, C.G.; Fraterman, H.; van der Helm, F.C.; Vermeulen, H.M.; Rozing, P.M. Calibration of the ‘Flock of Birds’ electromagnetic tracking device and its application in shoulder motion studies. J. Biomech. 1999, 32, 629–633. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Cook, T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys. Ther. 2000, 80, 276–291. [Google Scholar] [CrossRef]
- An, K.N.; Korinek, S.L.; Kilpela, T.; Edis, S. Kinematic and kinetic analysis of push-up exercise. Biomed. Sci. Instrum. 1990, 26, 53–57. [Google Scholar]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Buchholz, B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Hannah, D.C.; Scibek, J.S. Collecting shoulder kinematics with electromagnetic tracking systems and digital inclinometers: A review. World J. Orthop. 2015, 6, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.H.; Moriya, É.T.U.; Maciel, C.D.; Serrão, F.V. Test-retest reliability of three-dimensional kinematics using an electromagnetic tracking system during single-leg squat and stepping maneuver. Gait Posture 2014, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Biazotto, C.C.; Camarini, P.M.F.; Tucci, H.T.; McQuade, K.J.; de Oliveira, A.S. Reliability of electromagnetic tracking of scapular orientation and position in healthy sendentary individuals. Rev. Bras. Cineantropometria Desempenho Hum. 2014, 16, 689–697. [Google Scholar] [CrossRef][Green Version]
- Araki, D.; Matsushita, T.; Hoshino, Y.; Nagai, K.; Nishida, K.; Koga, H.; Kuroda, R. The Anterolateral Structure of the Knee Does Not Affect Anterior and Dynamic Rotatory Stability in Anterior Cruciate Ligament Injury- Quantitative Evaluation With the Electromagnetic. Am. J. Sports Med. 2019, 47, 3381–3388. [Google Scholar] [CrossRef] [PubMed]
- Cerrito, A.; Milburn, P.; Adams, R.; Evans, K. Cervical spine kinematics measured during rugby union scrums: Reliability of optoelectronic and electromagnetic tracking systems. Cogent Med. 2018, 5, 1526758. [Google Scholar] [CrossRef]
- ISO 11228-3:2007; Ergonomics—Manual Handling—Part 3: Handling of Low Loads at High Frequency. International Standard Organization: Geneva, Switzerland, 2007.
- Nordander, C.; Hansson, G.Å.; Ohlsson, K.; Arvidsson, I.; Balogh, I.; Strömberg, U.; Skerfving, S. Exposure-response relationships for work-related neck and shoulder musculoskeletal disorders—Analyses of pooled uniform data sets. Appl. Ergon. 2016, 55, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Schall, M.C.; Fethke, N.B. Gyroscope vector magnitude: A proposed method for measuring angular velocities. Appl. Ergon. 2023, 109, 103981. [Google Scholar] [CrossRef]
- Balogh, I.; Arvidsson, I.; Björk, J.; Hansson, G.Å.; Ohlsson, K.; Skerfving, S.; Nordander, C. Work-related neck and upper limb disorders—Quantitative exposure-response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet. Disord. 2019, 20, 139. [Google Scholar] [CrossRef]
- Arvidsson, I.; Dahlqvist, C.; Enquist, H.; Nordander, C. Action Levels for the Prevention of Work-Related Musculoskeletal Disorders in the Neck and Upper Extremities: A Proposal. Ann. Work Expo. Health 2021, 65, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Surgery for subacromial impingement syndrome in relation to intensities of occupational mechanical exposures across 10-year exposure time windows. Occup. Environ. Med. 2017, 75, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Jee, H.; Park, J. Comparative Analyses of the Dominant and Non-Dominant Upper Limbs during the Abduction and Adduction Motions. Iran. J. Public Health 2019, 48, 1768–1776. [Google Scholar] [CrossRef]
- Sande, L.P.; Coury, H.J.C.G.; Oishi, J.; Kumar, S. Effect of musculoskeletal disorders on prehension strength. Appl. Ergon. 2001, 32, 609–616. [Google Scholar] [CrossRef]
- Agtuahene, M.A.; Quartey, J.; Kwakye, S. Influence of hand dominance, gender, and body mass index on hand grip strength. S. Afr. J. Physiother. 2023, 79, 1923. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).