
Evaluation of Shoulder Risk Factors in the Repetitive Task of Slaughterhouse


 and
and 
Abstract
:1. Introduction
1.1. Assessment in the Slaughterhouse Industry
1.2. Causes of Musculoskeletal Disorders in Manufacturing Industries
1.3. Shoulder Illnesses
1.4. Evaluation of Slaughterhouse Task
2. Materials and Methods
2.1. Subjects
2.2. Data Collection Procedures
2.3. Data Collection Instruments
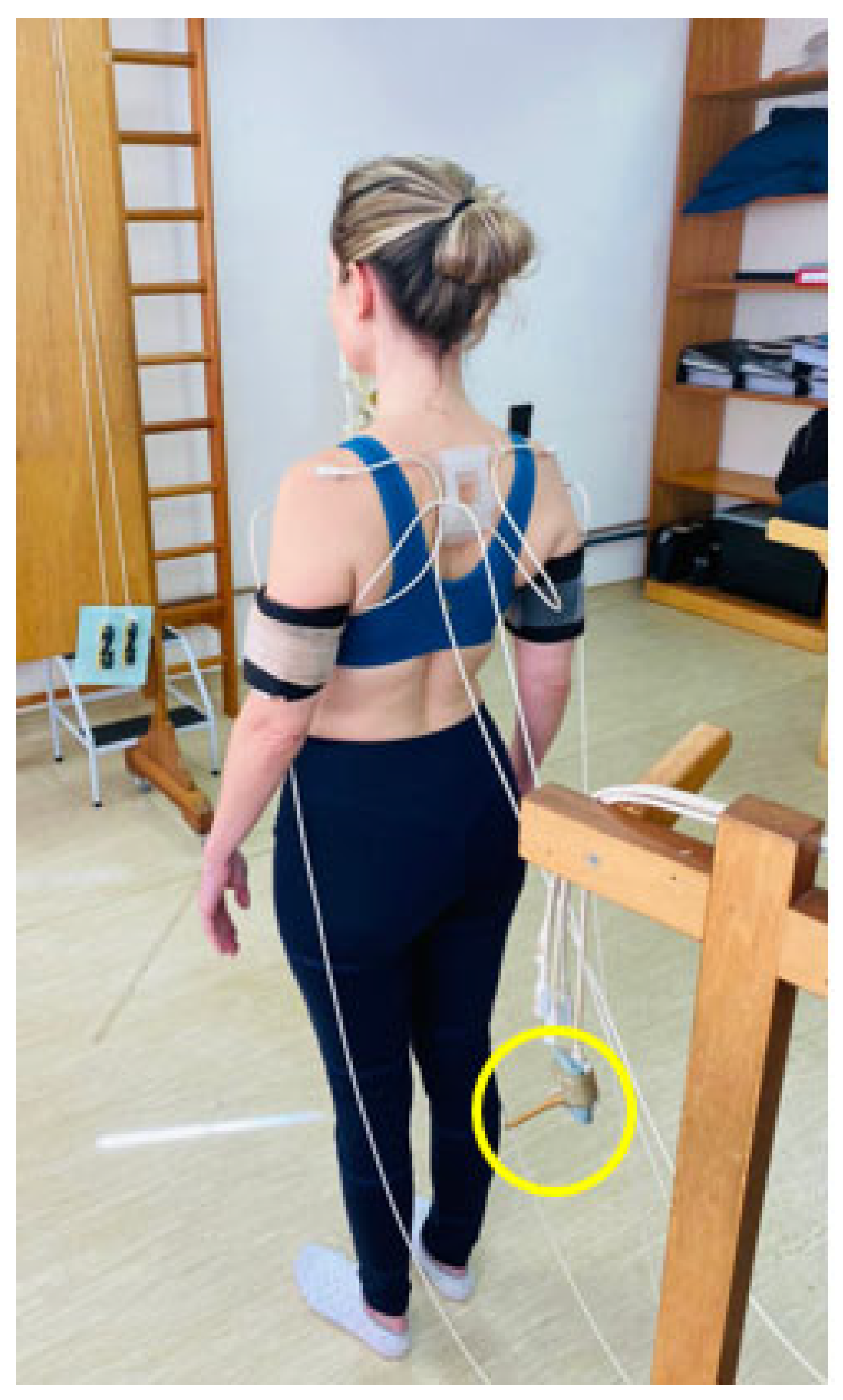
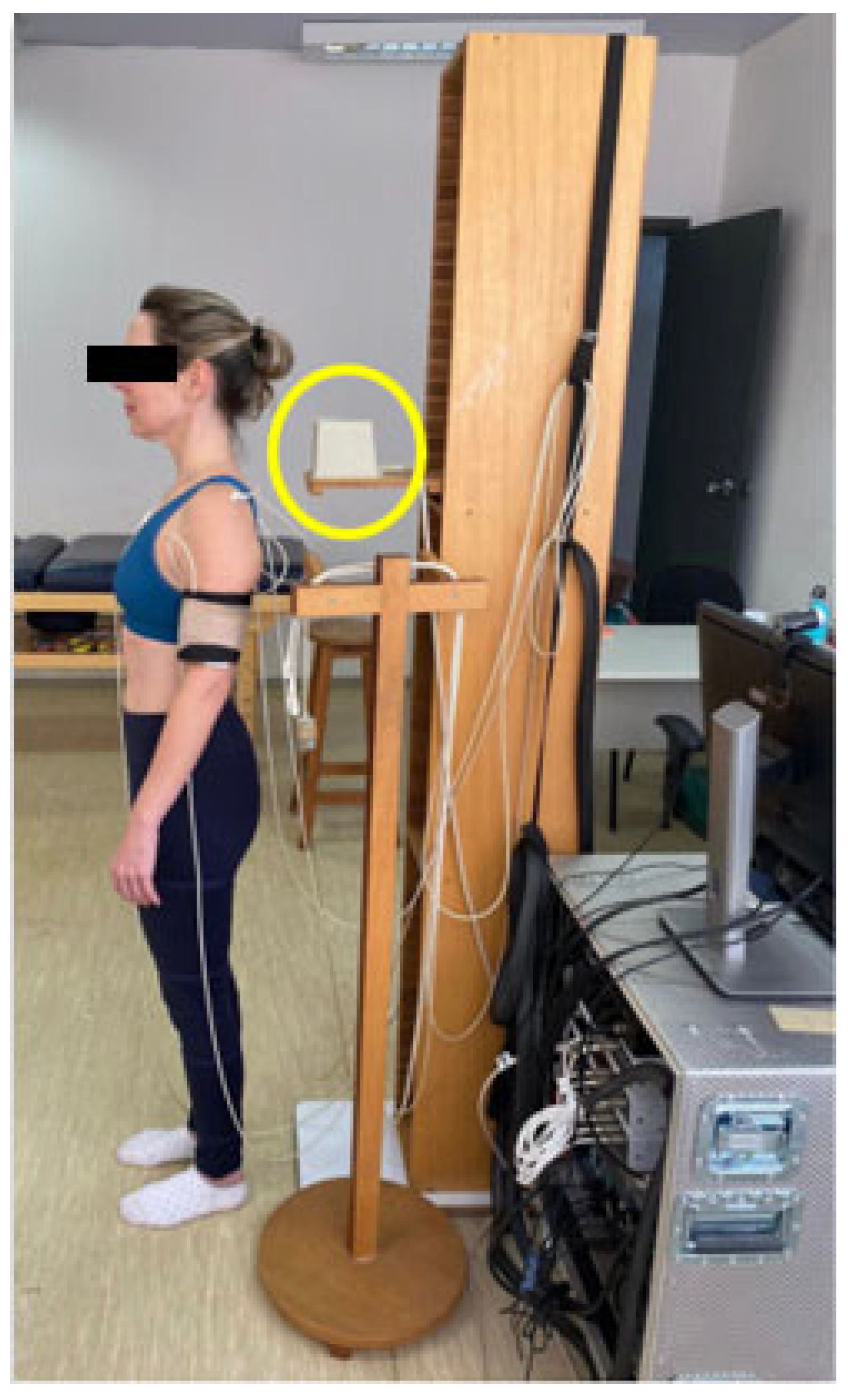
2.3.1. Setup Subject Sensors
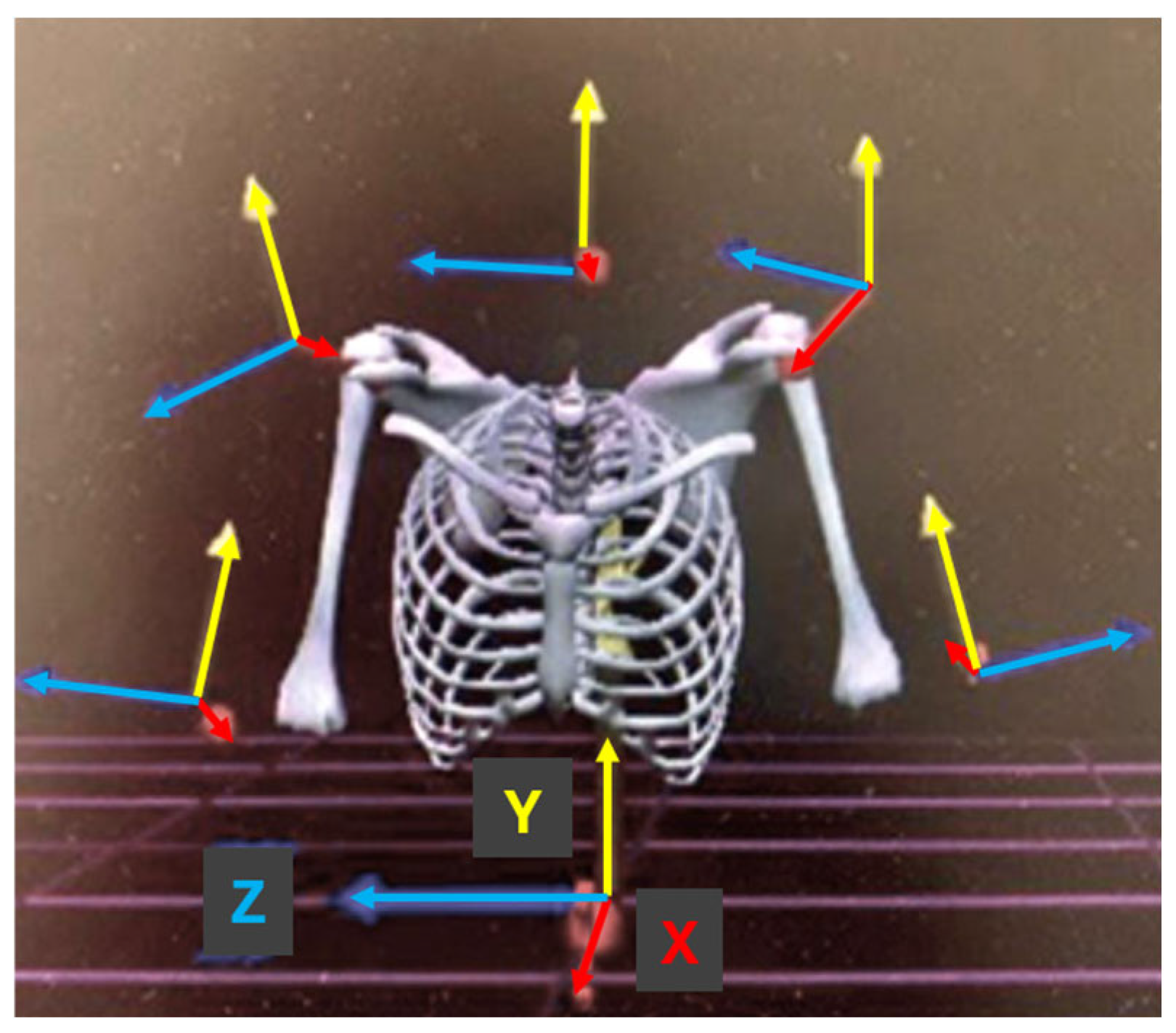
2.3.2. Kinematic Evaluation and Intersegmental Coordination
2.3.3. Recognition of the Sensors in the Body
2.4. Procedure
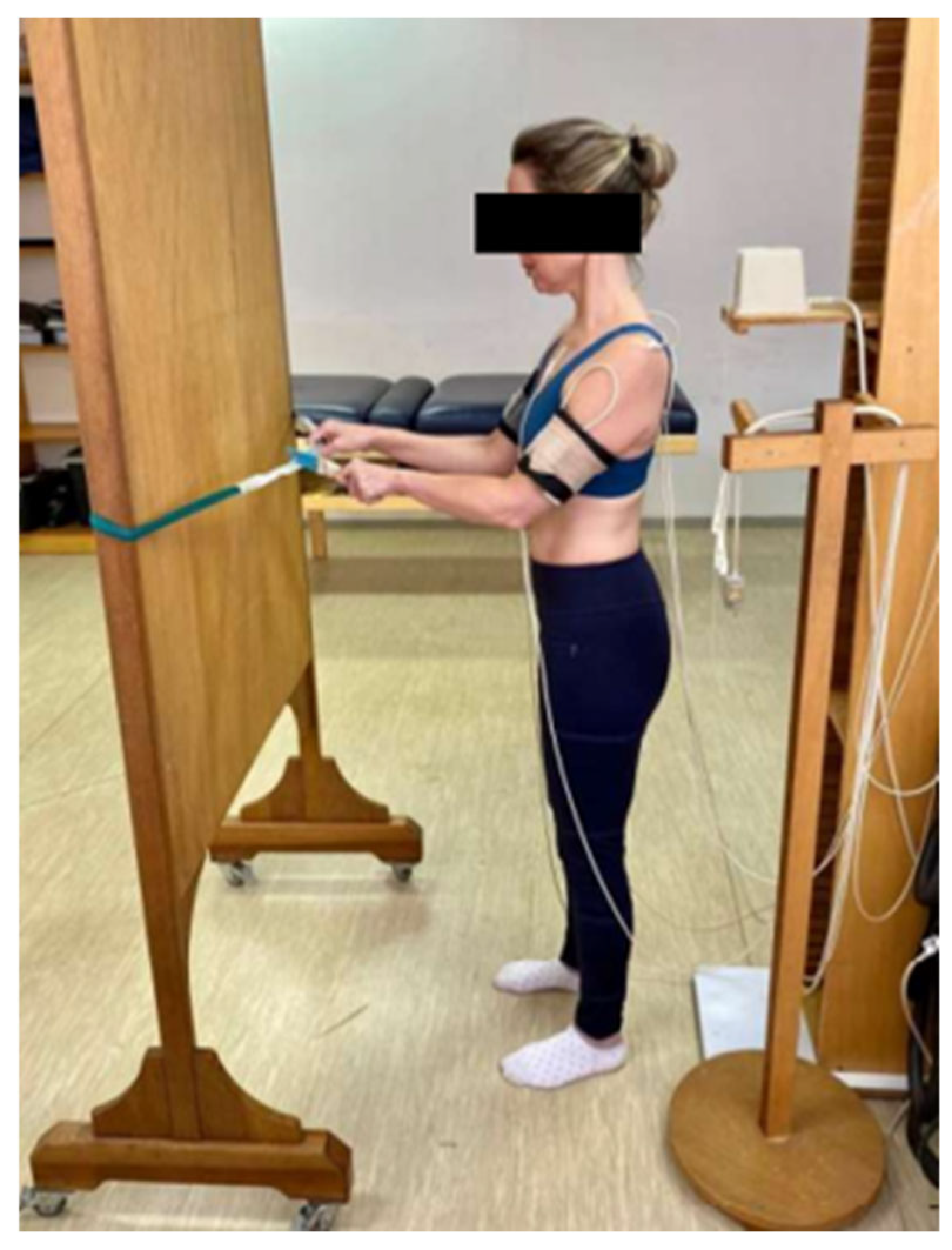
2.5. Laboratory Simulation
2.6. Cutting Wing Sector
2.7. Electromagnetic System
2.8. Data Analysis and Statistics
2.9. OCRA Method
3. Results
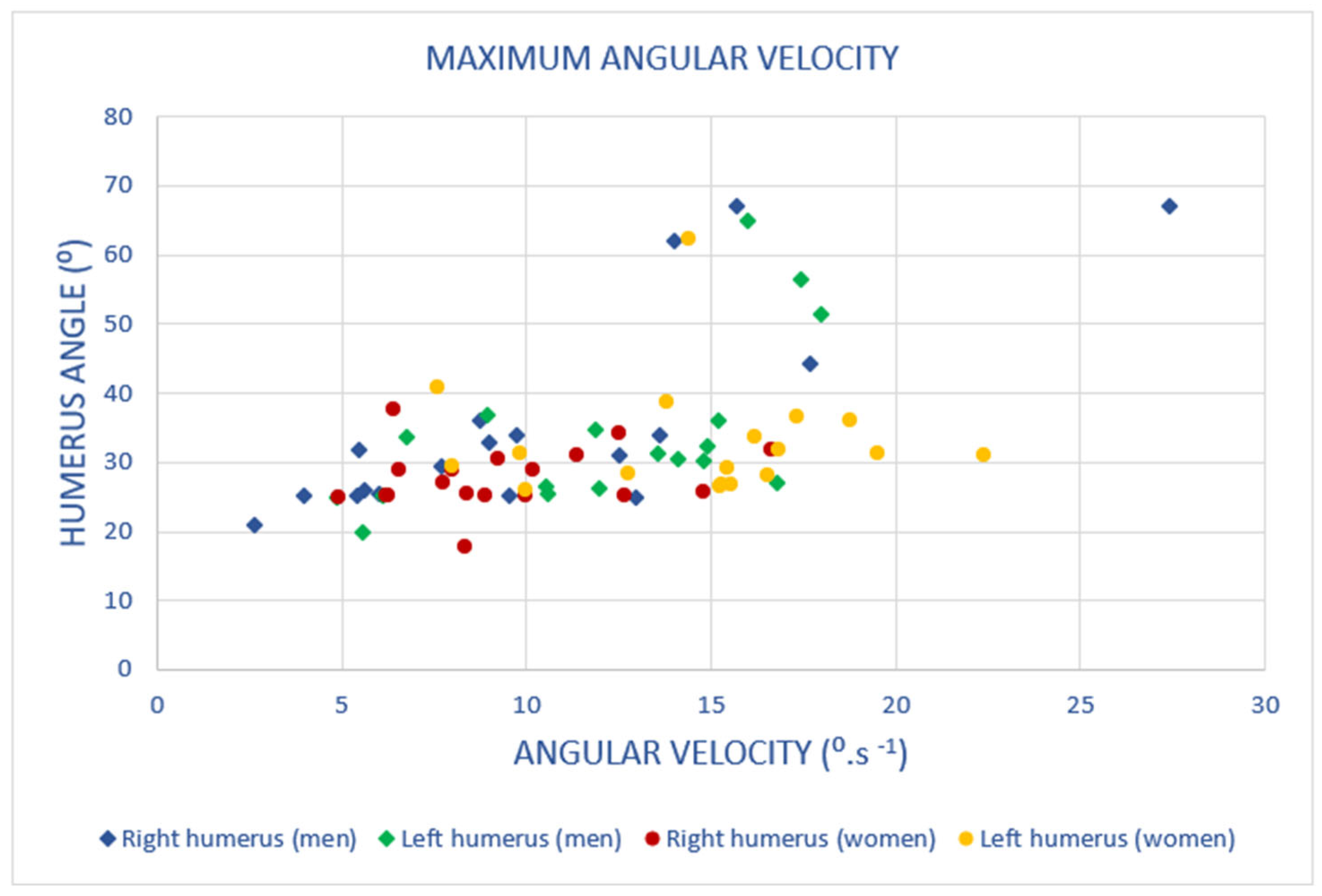
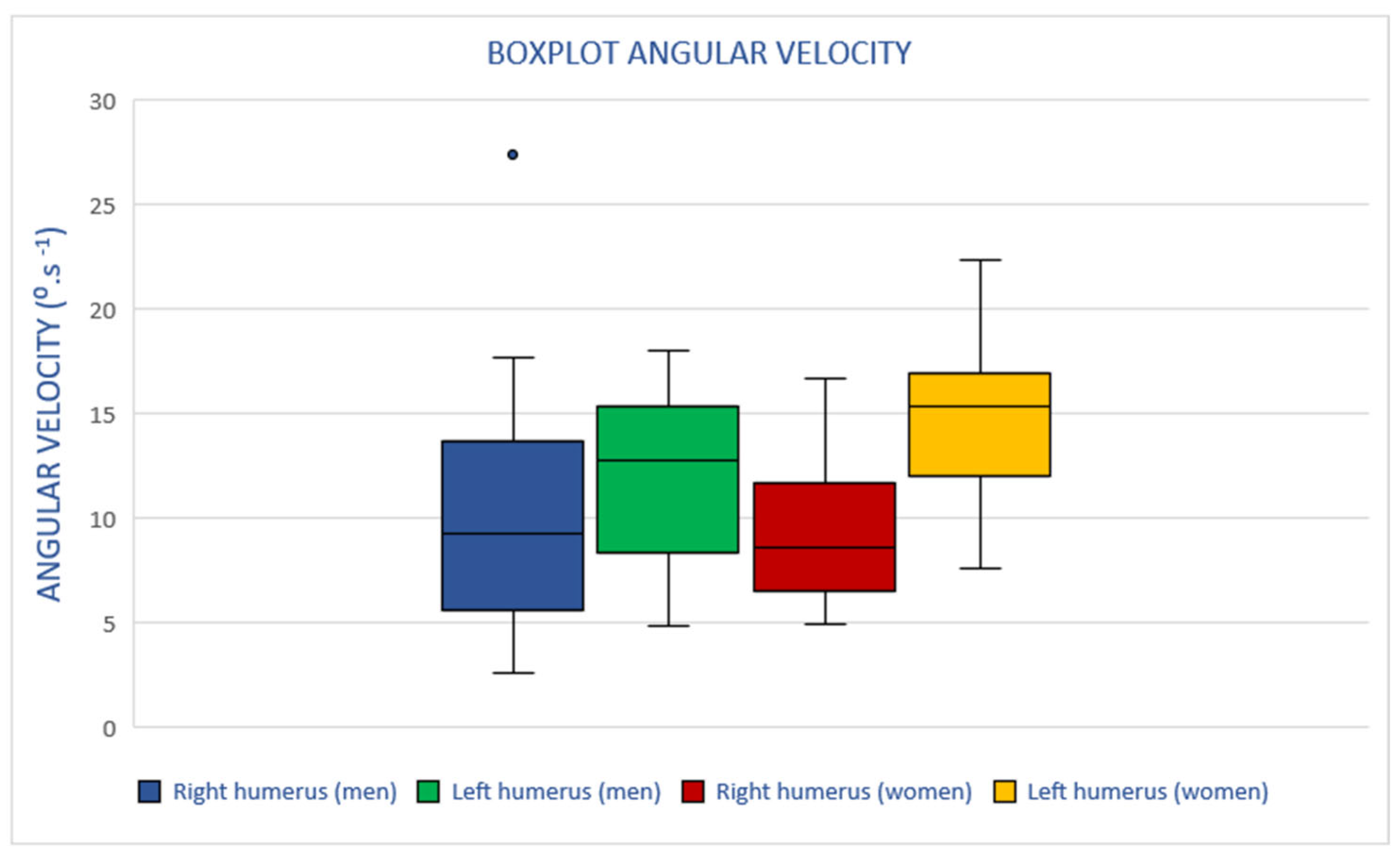
3.1. Angular Velocity
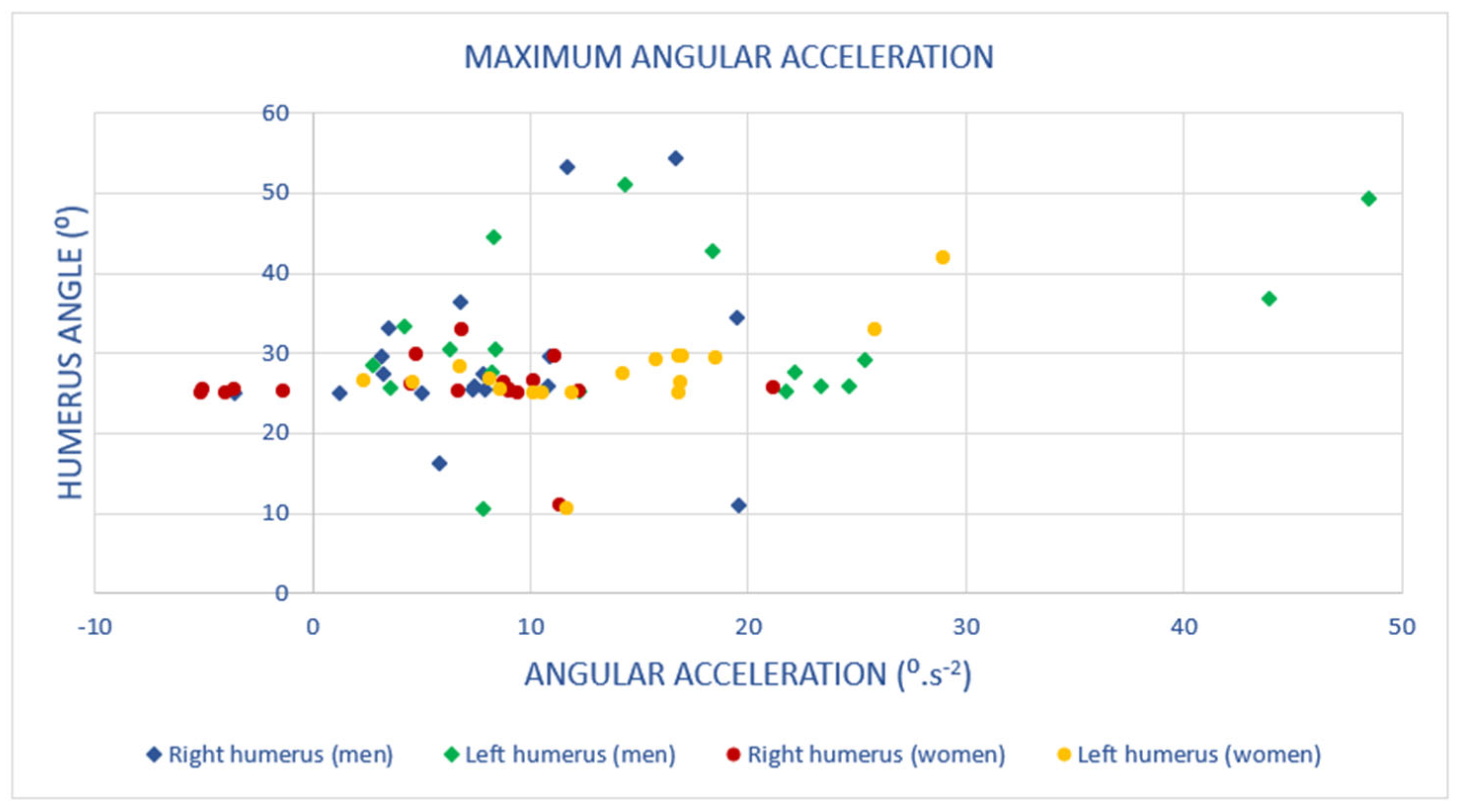
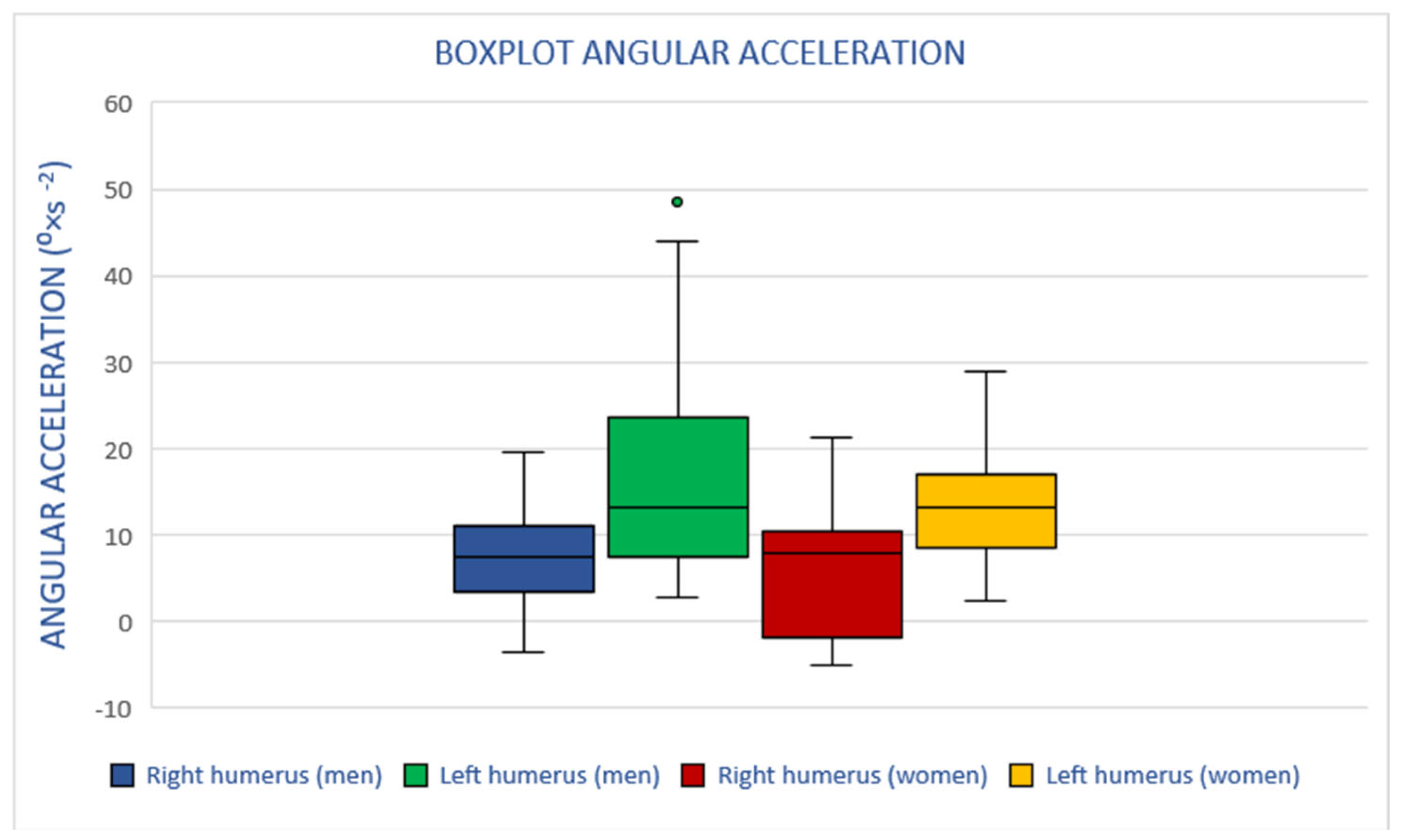
3.2. Angular Acceleration
3.3. ISO 11228-3
3.4. Statistical Differences According to the Mann–Whitney U Test
3.5. Medical Record and Incidence of Shoulder MSD
4. Discussion
4.1. Humerus Elevation
4.2. Angular Velocity
4.3. Angular Acceleration
4.4. Repetitive Movements
4.5. Shoulder Disorders in a Real Environment
4.6. Implications for Practice
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harari, Y.; Bechar, A.; Riemer, R. Workers’ biomechanical loads and kinematics during multiple-task manual material handling. Appl. Ergon. 2020, 83, 102985. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.; Assila, N.; Goubault, E.; Begon, M. Sex differences in upper limb musculoskeletal biomechanics during a lifting task. Appl. Ergon. 2020, 86, 103106. [Google Scholar] [CrossRef]
- Kranz, C.; Lee, K.; Jadhav, P.; Vestlin, L.; Barker, M.; Jacques, A.; Netto, K. Kinematic and perceptual responses in heavy lifting and pulling: Are there differences between males and females? Appl. Ergon. 2021, 90, 103274. [Google Scholar] [CrossRef]
- Lv, X.; Ji, Y.; Que, X.; Qing, T.; Yang, Y. Dual-squeeze effect: How job demands fuel overwork and its consequences in the context of hospitality. Curr. Issues Tour. 2023, 26, 2265–2283. [Google Scholar] [CrossRef]
- Fan, X.; Lind, C.M.; Rhen, I.-M.; Forsman, M. Effects of sensor types and angular velocity computational methods in field measurements of occupational upper arm and trunk postures and movements. Sensors 2021, 21, 5527. [Google Scholar] [CrossRef]
- European Agency for Safety and Health (EU-OSHA). Work-Related Musculoskeletal Disorders: Prevalence, Costs and Demographics in the EU; EU-OSHA: Bilbao, Spain; Publications Office of the European Union: Luxembourg, 2019. [Google Scholar]
- Thigpen, C.A.; Padua, D.A.; Michener, L.A.; Guskiewicz, K.; Giuliani, C.; Keener, J.D.; Stergiou, N. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. J. Electromyogr. Kinesiol. 2010, 20, 701–709. [Google Scholar] [CrossRef]
- Fong, A.R.; Pipher, Z.R.; Cudlip, A.C.; Holmes, M.W.R. Examining kinematics and muscle activity of the upper extremity while performing cleaning tasks: A pre-post shift evaluation. Int. J. Ind. Ergon. 2023, 93, 103405. [Google Scholar] [CrossRef]
- Antwi-Afari, M.F.; Anwer, S.; Umer, W.; Mi, H.Y.; Yu, Y.; Moon, S.; Hossain, M.U. Machine learning-based identification and classification of physical fatigue levels: A novel method based on a wearable insole device. Int. J. Ind. Ergon. 2023, 93, 103404. [Google Scholar] [CrossRef]
- Moussavi, S.E.; Zare, M.; Mahdjoub, M.; Grunder, O. Balancing high operator’s workload through a new job rotation approach: Application to an automotive assembly line. Int. J. Ind. Ergon. 2019, 71, 136–144. [Google Scholar] [CrossRef]
- Santos, M.R.D.; Mendes, C. Manual therapy and its role in occupational health: Reducing absenteeism and presenteeism by treating chronic pain with spinal manipulation and mobilization in the workplace. Eur. J. Integr. Med. 2020, 35, 101078. [Google Scholar] [CrossRef]
- Crawford, J.O.; Berkovic, D.; Erwin, J.; Copsey, S.M.; Davis, A.; Giagloglou, E.; Woolf, A. Best Practice & Research Clinical Rheumatology Musculoskeletal health in the workplace. Best Pract. Res. Clin. Rheumatol. 2020, 34, 101558. [Google Scholar] [PubMed]
- Arciniega-Rocha, R.P.; Erazo-Chamorro, V.C.; Szabo, G. The Prevention of Industrial Manual Tool Accidents Considering Occupational Health and Safety. Safety 2023, 9, 51. [Google Scholar] [CrossRef]
- Fleck, S.J.; Kraemer, W.J. Fundamentos do Treinamento de Força Muscular, 4th ed.; Human Kinetics: Porto Alegre, Brazil, 2017. [Google Scholar]
- Caldwell, J.A.; Caldwell, J.L.; Thompson, L.A.; Lieberman, H.R. Fatigue and its management in the workplace. Neurosci. Biobehav. Rev. 2019, 96, 272–289. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.C.; Calvin, T.F.; Keir, P.J. Adaptations to isolated shoulder fatigue during simulated repetitive work. Part II: Recovery. J. Electromyogr. Kinesiol. 2016, 29, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Maciukiewicz, J.M.; Lang, A.E.; Vidt, M.E.; Grenier, S.G.; Dickerson, C.R. Characterization of cashier shoulder and low back muscle demands. Int. J. Ind. Ergon. 2017, 59, 80–91. [Google Scholar] [CrossRef]
- McDonald, A.C.; Mulla, D.M.; Keir, P.J. Using EMG Amplitude and Frequency to Calculate a Multimuscle Fatigue Score and Evaluate Global Shoulder Fatigue. Hum. Factors 2018, 61, 526–536. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, V.S.; Devalkar, R.V. Postural analysis of building construction workers using ergonomics. Int. J. Constr. Manag. 2019, 19, 464–471. [Google Scholar] [CrossRef]
- Acaröz, S.; Sahin, U.K.; Akoglu, S. The investigation of work-related musculoskeletal disorders among female workers in a hazelnut factory: Prevalence, working posture, work-related and psychosocial factors. Int. J. Ind. Ergon. 2019, 74, 102838. [Google Scholar] [CrossRef]
- Lucas, J.; van Doorn, P.; Hegedus, E.; Lewis, J.; van der Windt, D. A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet. Disord. 2022, 23, 1073. [Google Scholar] [CrossRef]
- Prado, W.; Azevedo, V.; de Lucca, S.R.; Bandini, M. Shoulder arthralgia: Case study of the Occupational Medicine clinic of Universidade Estadual de Campinas (Unicamp). Revista Brasileira de Medicina do Trabalho 2022, 20, 555–562. [Google Scholar] [CrossRef]
- Bodin, J.; Ha, C.; Sérazin, C.; Descatha, A.; Leclerc, A.; Goldberg, M.; Roquelaure, Y. Effects of individual and work-related factors on incidence of shoulder pain in a large working population. J. Occup. Health 2012, 54, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Fayão, J.G.; Libardoni, T.d.C.; Martins, J.; Souza, C.d.S.; de Oliveira, A.S. Queixas musculoesqueléticas no ombro: Características dos usuários e dos atendimentos na atenção primária. Fisioter. Pesqui. 2019, 26, 78–84. [Google Scholar] [CrossRef]
- EU-OSHA. Lesões musculosqueléticas. In Agencia Nacional para a Segurança e Saúde no Trabalho; EU-OSHA: Bilbao, Spain, 2019; Available online: https://osha.europa.eu/pt/themes/musculoskeletal-disorders (accessed on 12 June 2024).
- Macpherson, R.A.; Lane, T.J.; Collie, A.; McLeod, C.B. Age, sex, and the changing disability burden of compensated work-related musculoskeletal disorders in Canada and Australia. BMC Public Health 2018, 18, 758. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.R.; Serra, M.V.G.B.; de Almeida, L.B.; Villela, W.V.; Scalon, J.D.; Quemelo, P.R.V. Symptoms and risks for musculoskeletal disorders among male and female footwear industry workers. Int. J. Ind. Ergon. 2015, 48, 110–116. [Google Scholar] [CrossRef]
- Troelstra, A.S.; Straker, L.; Harris, M.; Brown, S.; der Beek, A.J.V.; Coenen, P. Multimorbidity is common among young workers and related to increased work absenteeism and presenteeism: Results from the population–based Raine Study cohort. Scand. J. Work. Environ. Health 2020, 46, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Pensola, T.; Haukka, E.; Kaila-kangas, L.; Neupane, S.; Leino-Arjas, P. Good work ability despite multisite musculoskeletal pain? A study among occupationally active Finns. Scand. J. Public Health 2016, 44, 300–310. [Google Scholar] [CrossRef] [PubMed]
- De Kok, J.; Vroonhof, P.; Snijders, J.; Roullis, G.; Clarke, M.; Peereboom, K.; Isusi, I. Work-related musculoskeletal disorders: Prevalence, costs and demographics in the EU; 2019. Available online: https://osha.europa.eu/es/publications/ (accessed on 12 June 2024).
- Halliday, B.; Van der Laan, L.; Raineri, A. Prioritizing Work Health, Safety, and Wellbeing in Corporate Strategy: An Indicative Framework. Safety 2023, 10, 18. [Google Scholar] [CrossRef]
- Meskers, C.G.; Fraterman, H.; van der Helm, F.C.; Vermeulen, H.M.; Rozing, P.M. Calibration of the ‘Flock of Birds’ electromagnetic tracking device and its application in shoulder motion studies. J. Biomech. 1999, 32, 629–633. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an upper extremity outcome measure: The DASH (disabilities of the arm, shoulder and hand). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Ludewig, P.M.; Cook, T.M. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys. Ther. 2000, 80, 276–291. [Google Scholar] [CrossRef]
- An, K.N.; Korinek, S.L.; Kilpela, T.; Edis, S. Kinematic and kinetic analysis of push-up exercise. Biomed. Sci. Instrum. 1990, 26, 53–57. [Google Scholar]
- Wu, G.; Van der Helm, F.C.; Veeger, H.D.; Makhsous, M.; Van Roy, P.; Anglin, C.; Buchholz, B. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: Shoulder, elbow, wrist and hand. J. Biomech. 2005, 38, 981–992. [Google Scholar] [CrossRef]
- Hannah, D.C.; Scibek, J.S. Collecting shoulder kinematics with electromagnetic tracking systems and digital inclinometers: A review. World J. Orthop. 2015, 6, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.H.; Moriya, É.T.U.; Maciel, C.D.; Serrão, F.V. Test-retest reliability of three-dimensional kinematics using an electromagnetic tracking system during single-leg squat and stepping maneuver. Gait Posture 2014, 39, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Biazotto, C.C.; Camarini, P.M.F.; Tucci, H.T.; McQuade, K.J.; de Oliveira, A.S. Reliability of electromagnetic tracking of scapular orientation and position in healthy sendentary individuals. Rev. Bras. Cineantropometria Desempenho Hum. 2014, 16, 689–697. [Google Scholar] [CrossRef]
- Araki, D.; Matsushita, T.; Hoshino, Y.; Nagai, K.; Nishida, K.; Koga, H.; Kuroda, R. The Anterolateral Structure of the Knee Does Not Affect Anterior and Dynamic Rotatory Stability in Anterior Cruciate Ligament Injury- Quantitative Evaluation With the Electromagnetic. Am. J. Sports Med. 2019, 47, 3381–3388. [Google Scholar] [CrossRef] [PubMed]
- Cerrito, A.; Milburn, P.; Adams, R.; Evans, K. Cervical spine kinematics measured during rugby union scrums: Reliability of optoelectronic and electromagnetic tracking systems. Cogent Med. 2018, 5, 1526758. [Google Scholar] [CrossRef]
- ISO 11228-3:2007; Ergonomics—Manual Handling—Part 3: Handling of Low Loads at High Frequency. International Standard Organization: Geneva, Switzerland, 2007.
- Nordander, C.; Hansson, G.Å.; Ohlsson, K.; Arvidsson, I.; Balogh, I.; Strömberg, U.; Skerfving, S. Exposure-response relationships for work-related neck and shoulder musculoskeletal disorders—Analyses of pooled uniform data sets. Appl. Ergon. 2016, 55, 70–84. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Schall, M.C.; Fethke, N.B. Gyroscope vector magnitude: A proposed method for measuring angular velocities. Appl. Ergon. 2023, 109, 103981. [Google Scholar] [CrossRef]
- Balogh, I.; Arvidsson, I.; Björk, J.; Hansson, G.Å.; Ohlsson, K.; Skerfving, S.; Nordander, C. Work-related neck and upper limb disorders—Quantitative exposure-response relationships adjusted for personal characteristics and psychosocial conditions. BMC Musculoskelet. Disord. 2019, 20, 139. [Google Scholar] [CrossRef]
- Arvidsson, I.; Dahlqvist, C.; Enquist, H.; Nordander, C. Action Levels for the Prevention of Work-Related Musculoskeletal Disorders in the Neck and Upper Extremities: A Proposal. Ann. Work Expo. Health 2021, 65, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Dalbøge, A.; Frost, P.; Andersen, J.H.; Svendsen, S.W. Surgery for subacromial impingement syndrome in relation to intensities of occupational mechanical exposures across 10-year exposure time windows. Occup. Environ. Med. 2017, 75, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Jee, H.; Park, J. Comparative Analyses of the Dominant and Non-Dominant Upper Limbs during the Abduction and Adduction Motions. Iran. J. Public Health 2019, 48, 1768–1776. [Google Scholar] [CrossRef]
- Sande, L.P.; Coury, H.J.C.G.; Oishi, J.; Kumar, S. Effect of musculoskeletal disorders on prehension strength. Appl. Ergon. 2001, 32, 609–616. [Google Scholar] [CrossRef]
- Agtuahene, M.A.; Quartey, J.; Kwakye, S. Influence of hand dominance, gender, and body mass index on hand grip strength. S. Afr. J. Physiother. 2023, 79, 1923. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Wing Cut Sector | |||
|---|---|---|---|
| Force Factor (FMJ) | |||
| Multiplier | % MCV | BORG | |
| Right Hand | 0.65 | 20 | 2 |
| Left Hand | 0.35 | 30 | 2 |
| Postural Factor (PM) | |||
| Upper Limb | Score | Multiplier | |
| Right Hand | Supination (60%) | 1/3 time | 0.7 |
| Left Hand | Flexion and Pronation (60%) | 2/3 time | 0.7 |
| Repetitiveness Factor (ReM) | |||
| Factor | Multiplier | ||
| Right Hand | Cadence 1–7 s | 0.7 | |
| Left Hand | Cadence 1–7 s | 0.7 | |
| Additional Factor (AM) | |||
| Condition | Multiplier | ||
| Right Hand | Cold, gloves, pace by machine | 0.8 | |
| Left Hand | Cold, gloves, pace by machine | 0.8 | |
| Recorevy Periods Factor (Fr) | |||
| Hours with no restore | Multiplier | ||
| Right Hand | 2 | 0.8 | |
| Left Hand | 2 | 0.8 | |
| Duration Factor (Fd) | |||
| Period | Multiplier | ||
| Right Hand | 7:30 h (450 min) | 1 | |
| Left Hand | 7:30 h (450 min) | 1 | |
| Result Right Hand: 7.644 | |||
| Result Left Hand: 4.116 | |||
| Technical actions recommended right hand: 3 | |||
| Technical actions recommended left hand: 6 | |||
| Right side | Variable | Angular Velocity | Angular Acceleration |
| U-Mann–Whitney | 158.000 | 147.000 | |
| Z | −0.127 | −0.475 | |
| Significance | 0.913 | 0.650 | |
| Left side | U-Mann–Whitney | 104.000 | 154.000 |
| Z | −1.835 | −0.253 | |
| Significance | 0.068 | 0.815 |
| Gender |
Previous Overload or Repetitive Work | Period Working in The Slaughterhouse | ||
|---|---|---|---|---|
| 0–2 Years | 2–5 Years | >5 Years | ||
| Male | Yes | 0% | 8% | 8% |
| No | 8% | 0% | 6% | |
| Female | Yes | 0% | 0% | 0% |
| No | 8% | 25% | 8% | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rosado, A.S.; Cabrini, I.; Duarte, N.; Baptista, J.S.; Guedes, J.C. Evaluation of Shoulder Risk Factors in the Repetitive Task of Slaughterhouse. Safety 2024, 10, 63. https://doi.org/10.3390/safety10030063
Rosado AS, Cabrini I, Duarte N, Baptista JS, Guedes JC. Evaluation of Shoulder Risk Factors in the Repetitive Task of Slaughterhouse. Safety. 2024; 10(3):63. https://doi.org/10.3390/safety10030063
Chicago/Turabian StyleRosado, Ana Sophia, Isabella Cabrini, Natalia Duarte, João Santos Baptista, and Joana C. Guedes. 2024. "Evaluation of Shoulder Risk Factors in the Repetitive Task of Slaughterhouse" Safety 10, no. 3: 63. https://doi.org/10.3390/safety10030063
APA StyleRosado, A. S., Cabrini, I., Duarte, N., Baptista, J. S., & Guedes, J. C. (2024). Evaluation of Shoulder Risk Factors in the Repetitive Task of Slaughterhouse. Safety, 10(3), 63. https://doi.org/10.3390/safety10030063