Abstract
A healthy lifestyle from early childhood is a crucial factor that influences bone-related factors in adulthood. In this context, physical education or psychomotricity from early childhood is an important opportunity to face this problem. The present article aims to systematically summarize school-based interventions, evaluated through randomized controlled trial design, that influence the bones of children from early childhood. A systematic review of relevant articles was carried out using four main databases (PubMed, ProQuest Central (including 26 databases), Scopus, and Web of Sciences) until 12 November 2023. From a total of 42 studies initially found, 12 were included in the qualitative synthesis. In brief terms, from early childhood and during puberty, children’s bones are particularly responsive to exercise, making this an ideal time for interventions to maximize bone health. Therefore, incorporating physical activity into school curriculums is a strategic approach for enhancing bone health in children. Mainly, plyometric exercises can significantly enhance bone density and geometry. Nevertheless, collaboration among educators, healthcare professionals, and parents is key for designing and implementing these effective interventions.
1. Introduction
Physical exercise is any bodily movement produced by skeletal muscles that expends energy, although different types of exercises may differ depending on the intensity, duration, and frequency of movements [1]. Examples are aerobic exercise (i.e., any activity that uses large muscle groups, can be maintained continuously, and is rhythmic in nature) [2] or force–velocity-based exercises (i.e., exercises where the maximal force is inversely related to the velocity of shortening) [3]. Further, the combination of different types of exercises may lead to different kinds of exercise such as weight-bearing aerobic exercises (i.e., impact activities or any other exercise in which the arms, feet, and legs are bearing the weight, such as walking, stair climbing, jogging, or dancing) or strength and/or resistance exercises (i.e., the joints are moved against some kind of resistance) [4].
For instance, the importance of physical exercise addressed by the United Nations Education, Scientific, and Cultural Organization (UNESCO) supports the importance of fueling an active lifestyle in all age ranges [5]. Unfortunately, current data highlight a sedentary lifestyle for 81% of children, forecasting a 15% relative reduction until 2030 [6]. This fact may lead to negative consequences for children’s health. An example to combat this is reducing the risk of suffering from non-communicable diseases in adulthood, such as high levels of obesity-related chronic diseases including diabetes, metabolic syndrome, or cardiovascular disease (e.g., hypertension, elevated cholesterol) [7,8,9,10]. Hence, different effects may be the reason for health risks and serious long-term consequences [11].
Among these long-term consequences are bone-related factors [12] such as bone mass, properties of constituent tissue, and bone geometry [13]. One of the most common diseases is osteoporosis, which is a musculoskeletal disease caused by a decrement in bone mass and destruction of the bone microstructure [14]. Osteoporosis affects 200 million people worldwide, resulting in 8.9 million fractures every year [15]. According to a recent systematic review and meta-analysis, the prevalence of osteoporosis is 18.3% globally (women = 23.1%; men = 11.7%) [16]. This disease is caused by changes in hormone secretion that lead to the breakdown of the original balance in the body and cause dysfunction in structures such as bones [17]. This disorder may be shown in the skeleton by a reduction in bone mineral density caused by fluctuations in osteoclast and osteoblast activity [14]. However, the problems that may affect bones may arise from early childhood. For example, some other diseases such as the metabolic bone disease of prematurity (characterized by skeletal demineralization or, in some cases, fragility fractures) arise from prenatal and postnatal factors, when an infant born preterm may be deprived of fetal mineral accumulation [18]. Fortunately, and considering the reduction in the quality of life and mobility that bone-related diseases provoke, many studies have highlighted non-pharmacological approaches for the prevention of osteoporosis regarding exercise [15], anthropometry, sleep disruptions (e.g., abnormal sleep duration, night shift work) [19], or nutrition (e.g., importance of calcium and vitamin D) [15], which may highlight the importance of caring for health-related habits from the first years of life.
In a study performed with participants from early childhood to 30 years of age [20], the authors highlighted that the peak bone mass occurs between the end of the second decade and early in the third decade of life, although it depends on the skeletal site. This idea supports the importance of the circumpubertal years for accruing bone minerals [20]. Thus, due to the importance of lifestyle in bone-related factors, the importance of practicing regular exercise from childhood for reducing the risk of osteoporosis and associated fractures has been highlighted. The convergence of this critical period of bone accrual and bone loading is considered a “window of opportunity” for the development of a healthy skeleton. This important period starts from early childhood, as a universal consensus highlights the effects of antecedents for reducing adult bone health problems [21]. This fact places education, in general, and physical education, in particular, as a crucial opportunity to face this problem.
To date, different systematic reviews have tried to analyze the effects of exercise on bone-related factors in children and adolescents. Examples are analyzing the influence of physical activity on bone strength in children and adolescents [21], the influence of sedentary behavior and bone health [12], and the comparison of the association between bone health and different intensities of accelerometer-derived habitual physical activity [20]. However, to the best of the authors’ knowledge, there is no systematic review that tried to analyze the effects of different school-based interventions, evaluated through randomized controlled trial design, on children’s bone-related factors from the early childhood period.
The present article aims to systematically summarize school-based interventions, evaluated through randomized controlled trial design, that influence the bones of children from early childhood.
2. Materials and Methods
2.1. Experimental Approach to the Problem
The present systematic review was carried out according to two guidelines: the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22] and the guidelines for performing systematic reviews in sport sciences [23].
2.2. Information Sources
Four main databases were selected to identify the articles published before 12 November 2023: (1) PubMed, (2) ProQuest Central (including 26 databases), (3) Scopus, and (4) Web of Sciences.
2.3. Search Strategy
Following the PICO design provided by PRISMA, the following search strategy was used to look for relevant articles, where the authors were not blinded to journal names or manuscripts’ authors:
(preschool OR kindergarten OR “primary education” OR “elementary education” OR school) AND (“physical education”) AND (bone*) AND (“randomized controlled trial*”).
2.4. Inclusion/Exclusion Criteria
Two authors independently completed the search and compared results to ensure that the same articles were identified. Then, identifying information from the papers (title, authors, date, and database) was downloaded and transferred into an Excel spreadsheet (Microsoft Corporation, Redmond, WA, USA), and duplicates were removed. The remaining articles were independently screened for meeting inclusion and exclusion criteria (Table 1). Moreover, relevant articles not previously identified were also screened identically, and further studies that complied with the inclusion/exclusion criteria were included and labeled as “included from external sources”.

Table 1.
Inclusion/exclusion criteria.
2.5. Data Extraction
Data extraction was prepared using an Excel spreadsheet in accordance with the Cochrane Consumers and Communication Review Group’s data extraction template (Group, 2016). The spreadsheet was used to assess inclusion and exclusion requirements for all selected studies. The process was independently conducted by the two authors. Any disagreement regarding study eligibility was resolved in a discussion. Full text articles that were excluded from the analysis were recorded with reasons for exclusion. All records were stored in the spreadsheet.
2.6. Assessment of Study Methodology
The Physiotherapy Evidence Database (PEDro) scale was used to assess the methodological quality of pre-test and post-test studies with experimental (EXP) and control (CON) groups randomly selected. The scale scores the internal study validity in a range of zero (low methodological quality) to 10 (high methodological quality). The score that each section receives can be from zero (“no”) to one (“yes”), depending on the quality obtained by each point. Ten items are measured in the scale. Studies that score from 9 to 10 on the PEDro scale are considered to be of excellent methodological quality. Studies with a score between six and eight have good methodological quality, between four and five, fair quality, and below four points, poor methodological quality [24].
3. Results
3.1. Identification and Selection of Studies
A total of 42 original articles were found, of which 16 were duplicates. Thus, a total of 26 unique articles were identified. After checking titles and abstracts, seven articles were excluded because they did not meet inclusion criterion number five. The full text of the remaining 19 articles was then analyzed; one article was excluded because it did not meet inclusion criterion number one, two articles were excluded because they did not meet inclusion criterion number two, and four articles were excluded because they did not meet exclusion criterion number three. Thus, a total of 12 articles met all of the inclusion criteria and were included in the final qualitative synthesis (Figure 1).
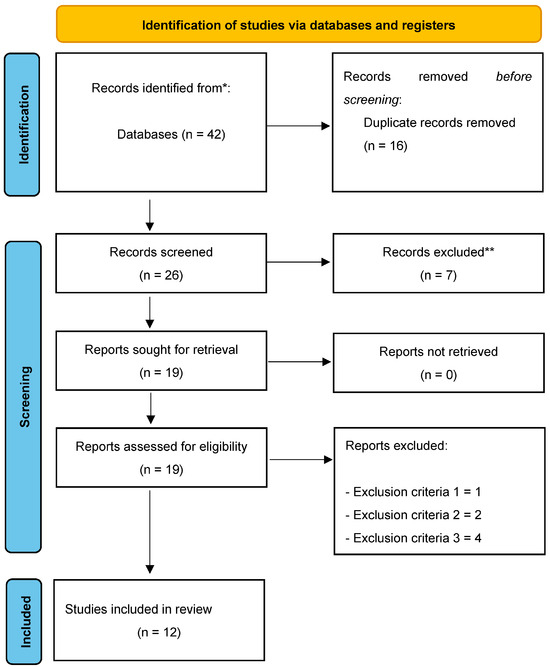
Figure 1.
Flow diagram of the study.
3.2. Quality Assessment
The quality assessment for this systematic review can be found in Table 2:
Table 2.
Methodological assessment of the included studies.
From the 12 included articles, eight obtained an excellent methodological quality score [25,26,28,30,32,35,36], while the remaining four studies obtained a good methodological quality score [27,29,33,34]. None of the included studies had fair or poor methodological quality.
3.3. Study Characteristics
A total of 12 articles were finally selected. From them, only two dealt with subjects about pubertal age (13–17 years) [35,36], while the remaining 10 articles analyzed subjects in both prepubertal and early pubertal stages (6–12 years) [25,30,31,32,33,34]. In addition, it is worth noting the wide variety of countries that integrated this type of study, such as the USA [27,29], Switzerland [25,33,34], Israel [28], Canada [31,32], Denmark [30], and Australia [35,36].
Assessment tools: Dual-energy X-ray absorptiometry (DXA) was used [25,26,27,29,30,32,33,34,35,36], followed by ultrasound densitometer [28,35,36] and peripheral quantitative computed tomography (pQCT) [26,31].
Intervention protocols: Six articles carried out intervention programs based on plyometric exercises (mainly high-intensity training that involves explosive movements based on the Stretch-Shortening Cycle (SSC)). This cycle enhances the power of the subsequent movement [25,27,30,32,35,36], while the rest of the studies purposed other methodologies: the implementation of varied high-intensity activities in 10-min time periods [28,31,33,34] and sports practices [26,29,30].
Duration of the interventions: The duration of the different intervention protocols was characterized by heterogeneity, with periods ranging from 7 months [27,32] to 4 years [26].
Outcomes: Regarding the results for bone parameters, 10 out of 12 studies detected significant improvements in the intervention groups compared to their respective control groups [26,27,28,29,30,31,32,33,34,35].
Sex and age: Significant improvements in both sexes were found, although both agents achieved different magnitudes in the variables analyzed [26,28,31,32,35].
Finally, only two articles examined the adherence and continuity of the improvements acquired from the intervention programs after a few years [33,36], while only one highlighted the importance of physical activity habits during the three years without intervention [33].
The characteristics of the studies were extracted and are clustered in Table 3:
Table 3.
Interventions for improving bone-related factors.
4. Discussion
The present article aimed to systematically summarize school-based interventions, evaluated through randomized controlled trial design, that influence the bones of children from early childhood.
In this review, there were only three programs developed during physical education classes. Therefore, since it is a strategic approach for enhancing bone health in children, taking advantage of the potential of this curricular subject and incorporating physical exercise programs in school curricula is necessary [37]. By targeting this intervention at an age where bones are most responsive to exercise, and ensuring that it is inclusive and adaptable to both genders, education from early childhood can play a pivotal role in establishing the foundation for lifelong bone health and overall well-being. Following MacKelvie et al. [32], early puberty may be a particularly suitable time for girls during growth for performing physical exercise interventions in order to have a positive effect on bone health. In this context, the onset of puberty brings an increment in girls’ estrogen levels, which significantly influence bone density. In fact, estrogen is vital for closing the growth plates and increasing the bone mineral density [38]. While the patterns of bone growth may vary between boys and girls, the benefits of physical activity for bone health are significant in both genders [39].
The regular plyometric exercises may also lead to an increment in bone mineral density in the lower extremities, which is a key factor in overall bone health [25,27,30,32,35,36]. Beyond density, the plyometric exercises can also improve bone geometry, making bones not just denser but also structurally sound [40]. Other types of exercise that can influence bones are weight-bearing physical activities such as running, jumping, and sports, which can stimulate bone growth through mechano-stimulation [41]. The stress placed on bones during these activities prompts bone-forming cells to increase bone mass and strength [42]. Following Larsen et al. [30], since peak bone mass is not yet achieved in this population group, this period is optimal for interventions like plyometric training to enhance bone properties. In addition, the plyometric exercises also contribute to improved muscular strength, coordination, and balance, which are important for overall physical development [43].
In this review, total body, femoral neck, and lumbar spine showed improvements in BMC and BMD during physical exercise programs in both sexes [27,32,33,34,35]. According to Lu et al. [44], the femoral neck, a critical region of the hip, benefits greatly from physical exercise. Given the femoral neck’s importance in weight-bearing and its vulnerability in later life (e.g., hip fractures), strengthening this area during childhood is particularly beneficial [37]. The lumbar spine is another key area that benefits from regular physical exercise. Exercises that involve bending, twisting, and lifting can increase the BMC and BMD in the vertebrae, which are vital for spinal health and posture [45]. Building strong bones during childhood can reduce the risk of osteoporosis and fractures later in life, especially in vulnerable areas like the hip and spine [46].
The impact of physical exercise programs on the distal radius and tibia properties in both boys and girls, with girls experiencing greater gains in the cortical area (CoA) and cortical thickness (CoTh) at the mid-tibia and radius [47], is an intriguing aspect of pediatric bone development and adaptation to exercise. These outcomes are highlighted in this systematic review in various studies [26,28]. The observation that girls show increments in CoA and CoTh in the mid-tibia and radius may be linked to hormonal differences and their response to mechanical loading during certain developmental stages [48]. Boys also benefit from exercise programs in terms of bone properties and the pattern of their bone development. Moreover, boys may respond differently to exercise due to factors like hormonal changes, growth rates, and the timing of growth spurts [49]. The cortical area and cortical thickness are key indicators of bone strength [50]. The cortical bone is the dense outer surface of bone that contributes significantly to bone strength and stability.
This review highlights the need to incorporate physical exercise programs into school curricula from early childhood for enhancing bone health in children, emphasizing that such interventions are particularly effective during early puberty in girls and beneficial for both genders, improving bone density, structure, and overall physical development. However, these findings should consider some limitations. One of them is the limited number of articles that were analyzed. It is important to raise awareness among educators, parents, or trainers of the importance of physical exercise in children to improve bone health. Another limitation would be the lack of studies carried out during the physical education classes during school hours.
5. Conclusions
Incorporating physical activity into school curriculums is a strategic approach to enhancing bone health in children. By targeting this intervention at an age where bones are most responsive to exercise, and ensuring it is inclusive and adaptable to both genders, schools can assume a pivotal role in establishing the foundation for lifelong bone health and overall well-being. The plyometric strength training offers a valuable method for improving lower extremity bone properties in prepubertal students. By capitalizing on the rapid bone development during this stage, the plyometric exercises can significantly enhance bone density and geometry. Collaboration among educators, healthcare professionals, and parents is a key for designing and implementing these effective interventions. For the aerobic and plyometric exercises, short rest periods are typical, especially if they are part of a game or play, while for structured strength training, 1–2 min of rest between sets is mainly recommended to prevent injuries. This consideration includes days with lighter or no scheduled exercise. Exercises should be suitable for the child’s age and physical development, knowing that younger children benefit more from play-like activities, while older children can engage in more structured exercises.
Author Contributions
Conceptualization, M.R.-G.; methodology, M.R.-G.; writing—original draft preparation, M.R.-G., R.M.-M. and A.M.-V.; writing—review and editing, M.R.-G., R.M.-M. and A.M.-V.; project administration, M.R.-G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical Activity, Exercise, and Physical Fitness: Definitions and Distinctions for Health-Related Research. Public Health Rep. 1985, 100, 126. [Google Scholar]
- Wahid, A.; Manek, N.; Nichols, M.; Kelly, P.; Foster, C.; Webster, P.; Kaur, A.; Friedemann Smith, C.; Wilkins, E.; Rayner, M.; et al. Quantifying the Association Between Physical Activity and Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. JAHA 2016, 5, e002495. [Google Scholar] [CrossRef]
- Bell, G.; Wenger, H. Physiological Adaptations to Velocity-Controlled Resistance Training. Sports Med. 1992, 13, 234–244. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Furlini, G.; Zati, A.; Letizia Mauro, G. The Effectiveness of Physical Exercise on Bone Density in Osteoporotic Patients. BioMed Res. Int. 2018, 2018, 4840531. [Google Scholar] [CrossRef]
- Luna, P.; Guerrero, J.; Cejudo, J. Improving Adolescents’ Subjective Well-Being, Trait Emotional Intelligence and Social Anxiety through a Programme Based on the Sport Education Model. Int. J. Environ. Res. Public Health 2019, 16, 1821. [Google Scholar] [CrossRef]
- Takehara, K.; Togoobaatar, G.; Kikuchi, A.; Lkhagvasuren, G.; Lkhagvasuren, A.; Aoki, A.; Fukuie, T.; Shagdar, B.-E.; Suwabe, K.; Mikami, M.; et al. Exercise Intervention for Academic Achievement Among Children: A Randomized Controlled Trial. Pediatrics 2021, 148, e2021052808. [Google Scholar] [CrossRef]
- Wright, K.; Giger, J.N.; Norris, K.; Suro, Z. Impact of a Nurse-Directed, Coordinated School Health Program to Enhance Physical Activity Behaviors and Reduce Body Mass Index among Minority Children: A Parallel-Group, Randomized Control Trial. Int. J. Nurs. Stud. 2013, 50, 727–737. [Google Scholar] [CrossRef]
- Xu, F.; Ware, R.S.; Tse, L.A.; Wang, Z.; Hong, X.; Song, A.; Li, J.; Wang, Y. A School-Based Comprehensive Lifestyle Intervention among Chinese Kids against Obesity (CLICK-Obesity): Rationale, Design and Methodology of a Randomized Controlled Trial in Nanjing City, China. BMC Public Health 2012, 12, 316. [Google Scholar] [CrossRef]
- Sahota, P.; Rudolf, M.C.J.; Dixey, R.; Hill, A.J.; Barth, J.H.; Cade, J. Randomised Controlled Trial of Primary School Based Intervention to Reduce Risk Factors for Obesity. BMJ 2001, 323, 5. [Google Scholar] [CrossRef]
- Vale, S.; Silva, P.; Santos, R.; Soares-Miranda, L.; Mota, J. Compliance with Physical Activity Guidelines in Preschool Children. J. Sports Sci. 2010, 28, 603–608. [Google Scholar] [CrossRef]
- Johnson, J.L.; Rudisill, M.E.; Hastie, P.; Wadsworth, D.; Strunk, K.; Venezia, A.; Sassi, J.; Morris, M.; Merritt, M. Changes in Fundamental Motor-Skill Performance Following a Nine-Month Mastery Motivational Climate Intervention. Res. Q. Exerc. Sport 2019, 90, 517–526. [Google Scholar] [CrossRef]
- Koedijk, J.B.; Van Rijswijk, J.; Oranje, W.A.; Van Den Bergh, J.P.; Bours, S.P.; Savelberg, H.H.; Schaper, N.C. Sedentary Behaviour and Bone Health in Children, Adolescents and Young Adults: A Systematic Review. Osteoporos. Int. 2017, 28, 2507–2519. [Google Scholar] [CrossRef]
- Krahenbühl, T.; Guimarães, R.D.F.; Barros Filho, A.D.A.; Gonçalves, E.M. Geometria óssea e atividade física em crianças e adolescentes: Revisão sistemática. Rev. Paul. Pediatr. 2018, 36, 230–237. [Google Scholar] [CrossRef]
- Su, Y.; Chen, Z.; Xie, W. Swimming as Treatment for Osteoporosis: A Systematic Review and Meta-Analysis. BioMed Res. Int. 2020, 2020, 6210201. [Google Scholar] [CrossRef]
- Papadopoulou, S.K.; Papadimitriou, K.; Voulgaridou, G.; Georgaki, E.; Tsotidou, E.; Zantidou, O.; Papandreou, D. Exercise and Nutrition Impact on Osteoporosis and Sarcopenia—The Incidence of Osteosarcopenia: A Narrative Review. Nutrients 2021, 13, 4499. [Google Scholar] [CrossRef]
- Salari, N.; Ghasemi, H.; Mohammadi, L.; Behzadi, M.H.; Rabieenia, E.; Shohaimi, S.; Mohammadi, M. The Global Prevalence of Osteoporosis in the World: A Comprehensive Systematic Review and Meta-Analysis. J. Orthop. Surg. Res. 2021, 16, 609. [Google Scholar] [CrossRef]
- Cheng, C.-H.; Chen, L.-R.; Chen, K.-H. Osteoporosis Due to Hormone Imbalance: An Overview of the Effects of Estrogen Deficiency and Glucocorticoid Overuse on Bone Turnover. Int. J. Mol. Sci. 2022, 23, 1376. [Google Scholar] [CrossRef]
- Chinoy, A.; Mughal, M.Z.; Padidela, R. Metabolic Bone Disease of Prematurity: Causes, Recognition, Prevention, Treatment and Long-Term Consequences. Arch. Dis. Child.-Fetal Neonatal Ed. 2019, 104, F560–F566. [Google Scholar] [CrossRef]
- Swanson, C. Sleep Disruption and Bone Health. Curr. Osteoporos. Rep. 2022, 20, 202–212. [Google Scholar] [CrossRef]
- Baxter-Jones, A.D.; Faulkner, R.A.; Forwood, M.R.; Mirwald, R.L.; Bailey, D.A. Bone Mineral Accrual from 8 to 30 Years of Age: An Estimation of Peak Bone Mass. J. Bone Miner. Res. 2011, 26, 1729–1739. [Google Scholar] [CrossRef]
- Tan, V.P.; Macdonald, H.M.; Kim, S.; Nettlefold, L.; Gabel, L.; Ashe, M.C.; McKay, H.A. Influence of Physical Activity on Bone Strength in Children and Adolescents: A Systematic Review and Narrative Synthesis. J. Bone Miner. Res. 2014, 29, 2161–2181. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Rico-González, M.; Pino-Ortega, J.; Clemente, F.M.; Los Arcos, A. Guidelines for Performing Systematic Reviews in Sports Science. Biol. Sport 2022, 39, 463–471. [Google Scholar] [CrossRef]
- Maher, C.G.; Sherrington, C.; Herbert, R.D.; Moseley, A.M.; Elkins, M. Reliability of the PEDro Scale for Rating Quality of Randomized Controlled Trials. Phys. Ther. 2003, 83, 713–721. [Google Scholar] [CrossRef]
- Anliker, E.; Dick, C.; Rawer, R.; Toigo, M. Effects of Jumping Exercise on Maximum Ground Reaction Force and Bone in 8- to 12-Year-Old Boys and Girls: A 9-Month Randomized Controlled Trial. J. Musculoskelet. Neuronal Interact. 2012, 12, 56–67. [Google Scholar] [CrossRef]
- Daly, R.M.; Ducher, G.; Hill, B.; Telford, R.M.; Eser, P.; Naughton, G.; Seibel, M.J.; Telford, R.D. Effects of a Specialist-Led, School Physical Education Program on Bone Mass, Structure, and Strength in Primary School Children: A 4-Year Cluster Randomized Controlled Trial: Effects of school pe on bone mass, structure and strength in children. J. Bone Miner. Res. 2016, 31, 289–298. [Google Scholar] [CrossRef]
- Fuchs, R.K.; Bauer, J.J.; Snow, C.M. Jumping Improves Hip and Lumbar Spine Bone Mass in Prepubescent Children: A Randomized Controlled Trial. J. Bone Miner. Res. 2001, 16, 148–156. [Google Scholar] [CrossRef]
- Goldstein, E.; Rosenstreich, E.; Arnon, M.; Shoval, E. The Effects of a Physical Education Intervention Program on the Bone Properties of Second- and Third-Grade Pupils: A Cluster Randomized Controlled Trial. J. Phys. Act. Health 2022, 19, 425–435. [Google Scholar] [CrossRef]
- Gutin, B.; Yin, Z.; Johnson, M.; Barbeau, P. Preliminary Findings of the Effect of a 3-Year after-School Physical Activity Intervention on Fitness and Body Fat: The Medical College of Georgia Fitkid Project. Int. J. Pediatr. Obes. 2008, 3, 3–9. [Google Scholar] [CrossRef]
- Larsen, M.N.; Nielsen, C.M.; Helge, E.W.; Madsen, M.; Manniche, V.; Hansen, L.; Hansen, P.R.; Bangsbo, J.; Krustrup, P. Positive Effects on Bone Mineralisation and Muscular Fitness after 10 Months of Intense School-Based Physical Training for Children Aged 8–10 Years: The FIT FIRST Randomised Controlled Trial. Br. J. Sports Med. 2018, 52, 254–260. [Google Scholar] [CrossRef]
- Macdonald, H.M.; Kontulainen, S.A.; Khan, K.M.; McKay, H.A. Is a School-Based Physical Activity Intervention Effective for Increasing Tibial Bone Strength in Boys and Girls? J. Bone Miner. Res. 2007, 22, 434–446. [Google Scholar] [CrossRef] [PubMed]
- MacKelvie, K.J.; McKay, H.A.; Khan, K.M.; Crocker, P.R.E. A School-Based Exercise Intervention Augments Bone Mineral Accrual in Early Pubertal Girls. J. Pediatr. 2001, 139, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Ernst, D.; Zahner, L.; Schindler, C.; Puder, J.J.; Kraenzlin, M.; Rizzoli, R.; Kriemler, S. 3-Year Follow-up Results of Bone Mineral Content and Density after a School-Based Physical Activity Randomized Intervention Trial. Bone 2013, 55, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Meyer, U.; Romann, M.; Zahner, L.; Schindler, C.; Puder, J.J.; Kraenzlin, M.; Rizzoli, R.; Kriemler, S. Effect of a General School-Based Physical Activity Intervention on Bone Mineral Content and Density: A Cluster-Randomized Controlled Trial. Bone 2011, 48, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Weeks, B.K.; Young, C.M.; Beck, B.R. Eight Months of Regular In-School Jumping Improves Indices of Bone Strength in Adolescent Boys and Girls: The POWER PE Study. J. Bone Miner. Res. 2008, 23, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Weeks, B.K.; Beck, B.R. Are Bone and Muscle Changes from POWER PE, an 8-Month In-School Jumping Intervention, Maintained at Three Years? PLoS ONE 2012, 7, e39133. [Google Scholar] [CrossRef] [PubMed]
- Mello, J.B.; Pedretti, A.; García-Hermoso, A.; Martins, C.M.L.; Gaya, A.R.; Duncan, M.J.; Gaya, A.C.A. Exercise in School Physical Education Increase Bone Mineral Content and Density: Systematic Review and Meta-Analysis. Eur. J. Sport Sci. 2022, 22, 1618–1629. [Google Scholar] [CrossRef] [PubMed]
- Ciancia, S.; Dubois, V.; Cools, M. Impact of Gender-Affirming Treatment on Bone Health in Transgender and Gender Diverse Youth. Endocr. Connect. 2022, 11, e220280. [Google Scholar] [CrossRef]
- Lobelo, F.; Muth, N.D.; Hanson, S.; Nemeth, B.A.; Council on Sports Medicine and Fitness; Section on Obesity; LaBella, C.R.; Brooks, M.A.; Canty, G.; Diamond, A.B.; et al. Physical Activity Assessment and Counseling in Pediatric Clinical Settings. Pediatrics 2020, 145, e20193992. [Google Scholar] [CrossRef]
- Legerlotz, K.; Marzilger, R.; Bohm, S.; Arampatzis, A. Physiological Adaptations Following Resistance Training in Youth Athletes—A Narrative Review. Pediatr. Exerc. Sci. 2016, 28, 501–520. [Google Scholar] [CrossRef]
- Morseth, B.; Emaus, N.; Jørgensen, L. Physical Activity and Bone: The Importance of the Various Mechanical Stimuli for Bone Mineral Density. A Review. Nor. Epidemiol. 2011, 20, 1338. [Google Scholar] [CrossRef]
- Sun, Y.; Yuan, Y.; Wu, W.; Lei, L.; Zhang, L. The Effects of Locomotion on Bone Marrow Mesenchymal Stem Cell Fate: Insight into Mechanical Regulation and Bone Formation. Cell Biosci. 2021, 11, 88. [Google Scholar] [CrossRef] [PubMed]
- Almeida, M.B.D.; Leandro, C.G.; Queiroz, D.D.R.; José-da-Silva, M.; Pessôa Dos Prazeres, T.M.; Pereira, G.M.; das-Neves, G.S.; Carneiro, R.C.; Figueredo-Alves, A.D.; Nakamura, F.Y.; et al. Plyometric Training Increases Gross Motor Coordination and Associated Components of Physical Fitness in Children. Eur. J. Sport Sci. 2021, 21, 1263–1272. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Canavese, F.; Nan, G.; Lin, R.; Huang, Y.; Pan, N.; Chen, S. Is Femoral Neck System a Valid Alternative for the Treatment of Displaced Femoral Neck Fractures in Adolescents? A Comparative Study of Femoral Neck System versus Cannulated Compression Screw. Medicina 2022, 58, 999. [Google Scholar] [CrossRef] [PubMed]
- Babatunde, O.O.; Bourton, A.L.; Hind, K.; Paskins, Z.; Forsyth, J.J. Exercise Interventions for Preventing and Treating Low Bone Mass in the Forearm: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2020, 101, 487–511. [Google Scholar] [CrossRef]
- Jinnah, D.B. A Comprehensive Review of Minerals and Vitamins Synergy: Impacts on Childhood and Adolescent Bone Development. Am. J. Health Med. Nurs. Pract. 2023, 8, 12–30. [Google Scholar] [CrossRef]
- Delalande, L.; Moyon, M.; Tissier, C.; Dorriere, V.; Guillois, B.; Mevell, K.; Charron, S.; Salvia, E.; Poirel, N.; Vidal, J.; et al. Complex and Subtle Structural Changes in Prefrontal Cortex Induced by Inhibitory Control Training from Childhood to Adolescence. Dev. Sci. 2020, 23, e12898. [Google Scholar] [CrossRef]
- Hart, D.A. Regulation of Bone by Mechanical Loading, Sex Hormones, and Nerves: Integration of Such Regulatory Complexity and Implications for Bone Loss during Space Flight and Post-Menopausal Osteoporosis. Biomolecules 2023, 13, 1136. [Google Scholar] [CrossRef]
- Ansdell, P.; Thomas, K.; Hicks, K.M.; Hunter, S.K.; Howatson, G.; Goodall, S. Physiological Sex Differences Affect the Integrative Response to Exercise: Acute and Chronic Implications. Exp. Physiol. 2020, 105, 2007–2021. [Google Scholar] [CrossRef]
- Hart, N.H.; Newton, R.U.; Tan, J.; Rantalainen, T.; Chivers, P.; Siafarikas, A.; Nimphius, S. Biological Basis of Bone Strength: Anatomy, Physiology and Measurement. J. Musculoskelet. Neuronal Interact. 2020, 20, 347. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).