
Safety of a Porous Hydroxyapatite Bone Substitute in Orthopedics and Traumatology: A Multi-Centric Clinical Study

 , ,
, , 
Abstract
:1. Introduction
- -
- They reduce the risk of disease transmission because they are easily sterilizable;
- -
- They do not induce a host inflammatory response;
- -
- They are versatile in use and can be supplied in different formats and conformations;
- -
- They are ready to use;
- -
- They have remarkable mechanical and biomimetic properties;
- -
- They eliminate the problems related to the donor site occurring with the use of autografts.
- -
- Treating bone defects of the axial and appendicular skeletal system;
- -
- Filling bone gaps and reconstructing damaged or excised areas;
- -
- Surgical treatments for pathological conditions such as primary or secondary degenerative diseases (e.g., pseudoarthrosis in non-critical defects), as well as corrective surgery for malformation diseases of the skeletal system;
- -
- Orthopedic, cranial, and spinal surgery applications, using techniques such as osteosynthesis and bone reconstruction, prosthetic or intervertebral implants, prosthetic revision, and spinal fusion.
2. Materials and Methods
2.1. Objective of the Study
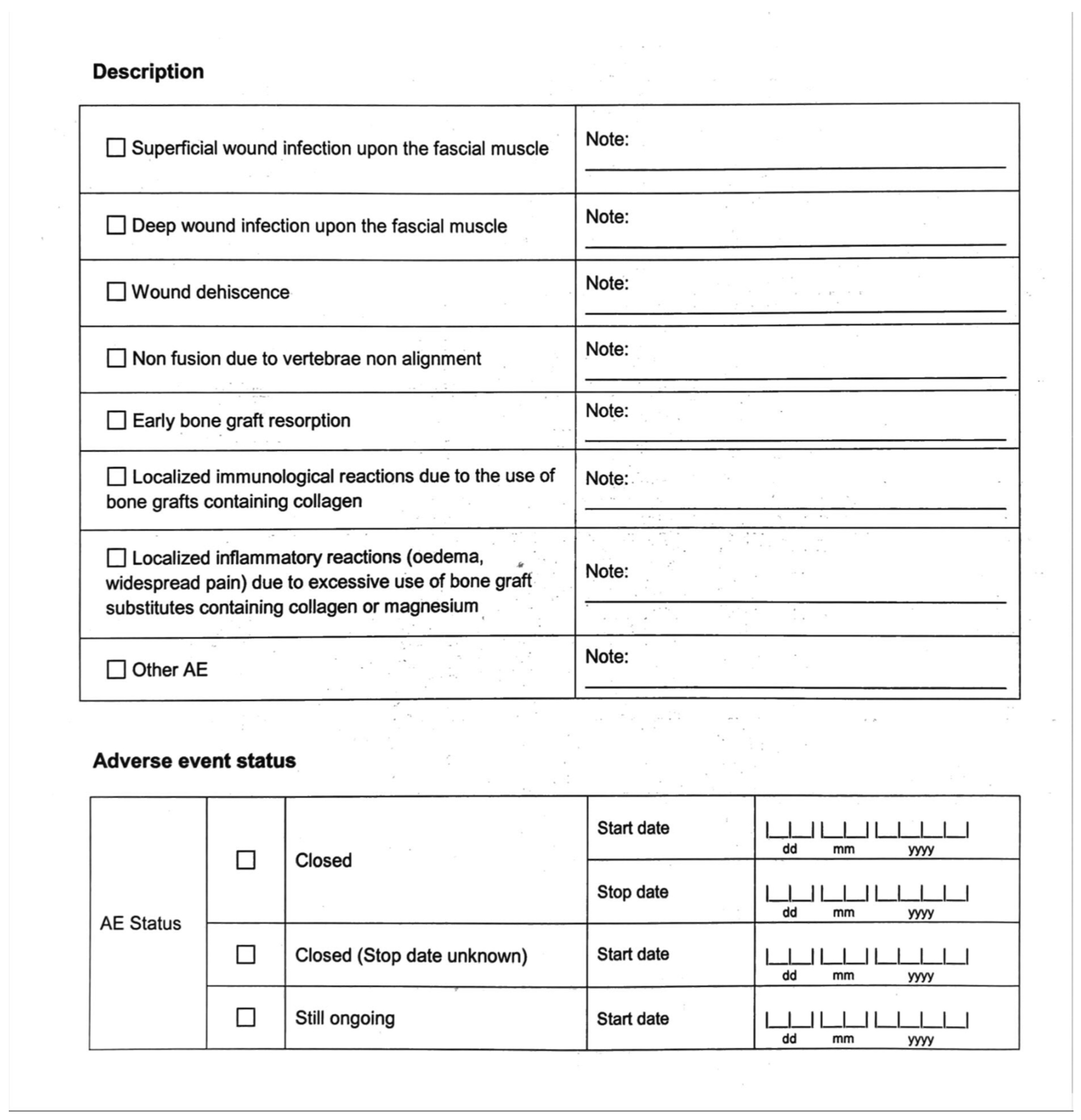
2.2. Definition of an Adverse Event
- -
- Description of an AE
- -
- AE status (closed or still ongoing)
- -
- Evolution/outcome (recovered, recovered with sequelae, death, or unknown)
- -
- Device explanted (NO or YES)
- -
- AE related to the use of the device (NO or YES)
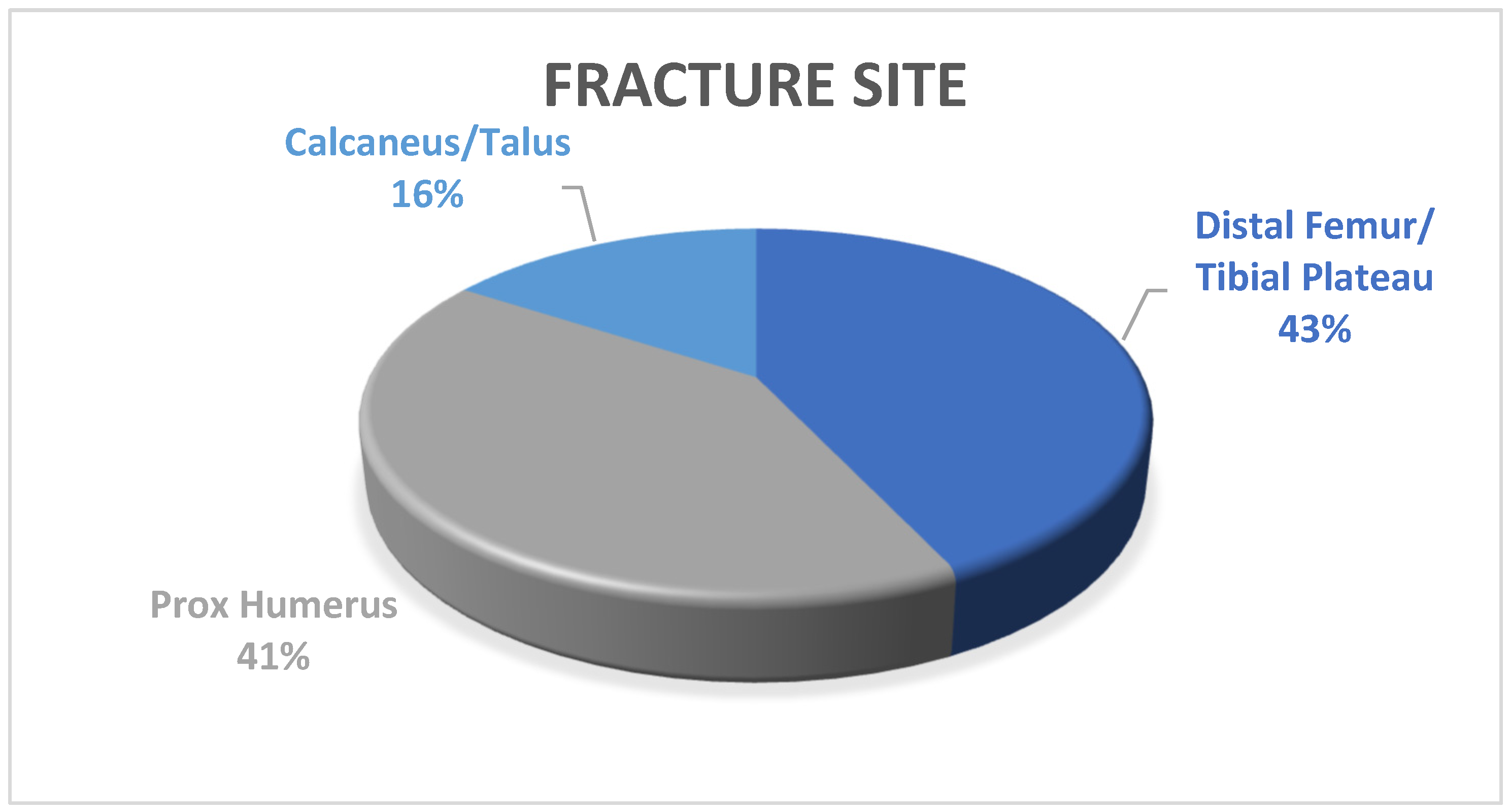
3. Results
- -
- 49 (43%) fractures of the tibial plateau and distal portion of the femur;
- -
- 47 (41%) fractures of the proximal portion of the humerus;
- -
- 18 (16%) fractures of the calcaneus or talus.
4. Discussion
Limitations and Advantages of the Study
5. Conclusions
Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Adverse Event Form

References
- Donati, D.; Zolezzi, C.; Tomba, P. Bone grafting: Historical and conceptual review, starting with an old manuscript by Vittorio Putti. Acta Orthop. 2007, 78, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Kwong, F.N.K.; Harris, M.B. Recent developments in the biology of fracture repair. J. Am. Acad. Orthop. Surg. 2008, 16, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Fayaz, H.C.; Giannoudis, P.V.; Vrahas, M.S.; Smith, R.M.; Moran, C.; Pape, H.C.; Krettek, C.; Jupiter, J.B. The role of stem cells in fracture healing and nonunion. Int. Orthop. 2011, 35, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- De Girolamo, L.; Arrigoni, E.; Stanco, D. Role of autologous rabbit adipose-derived stem cells in the early phases of the repairing process of critical bone defects. J. Orthop. Res. 2011, 29, 100–108. [Google Scholar] [CrossRef] [PubMed]
- Campana, V.; Milano, G.; Pagano, E. Bone substitutes in orthopaedic surgery: From basic science to clinical practice. J. Mater.Sci. Mater. Med. 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Gage, M.; Liporace, F.; Egol, K. Management of Bone Defects in Orthopedic Trauma. Bull. Hosp. Jt. Dis. 2018, 76, 4–8. [Google Scholar]
- Park, J.J.; Hershman, S.H.; Kim, Y.H. Updates in the use of bone grafts in the lumbar spine. Bull. Hosp. Jt. Dis. 2013, 71, 39–48. [Google Scholar]
- Dimar, J.R.; Glassman, S.D. The art of bone grafting. Curr. Opin. Orthop. 2007, 18, 8. [Google Scholar] [CrossRef]
- Almaiman, M.; Al-Bargi, H.H.; Manson, P. Complication of Anterior Iliac Bone Graft Harvesting in 372 Adult Patients from May 2006 to May 2011 and a Literature Review. Craniomaxillofac. Trauma Reconstr. 2013, 6, 257–266. [Google Scholar] [CrossRef]
- Pokharel, R.K.; Paudel, S.; Lakhey, R.B. Iliac Crest Bone Graft Harvesting: Modified Technique for Reduction of Complications. JNMA J. Nepal Med. Assoc. 2022, 60, 325–328. [Google Scholar] [CrossRef]
- Goulet, J.A.; Senunas, L.E.; DeSilva, G.L. Autogenous iliac crest bone graft. Complications and functional assessment. Clin. Orthop. Relat. Res. 1997, 339, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Dimar, J.R.; Glassman, S.D.; Burkus, J.K. Two-year fusion and clinical outcomes in 224 patients treated with a single-level instrumented posterolateral fusion with iliac crest bone graft. Spine J. 2009, 9, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Gruskay, J.A.; Basques, B.A.; Bohl, D.D. Short-term adverse events, length of stay, and readmission after iliac crest bone graft for spinal fusion. Spine 2014, 39, 1718–1724. [Google Scholar] [CrossRef] [PubMed]
- Basha, R.Y.; Sampath Kumar, T.S.; Doble, M. Design of biocomposite materials for bone tissue regeneration. Sci. Eng. C Mater. Biol. Appl. 2015, 57, 452–463. [Google Scholar] [CrossRef] [PubMed]
- Lovati, A.B.; Lopa, S.; Recordati, C. In Vivo Bone Formation Within Engineered Hydroxyapatite Scaffolds in a Sheep Model. Calcif. Tissue Int. 2016, 99, 209–223. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.T.; Rosenbaum, A.J. Bone grafts, bone substitutes and orthobiologics. Organogenesis 2012, 8, 114–124. [Google Scholar] [CrossRef]
- Gao, C.; Deng, Y.; Feng, P. Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int. J. Mol. Sci. 2014, 15, 4714–4732. [Google Scholar] [CrossRef] [PubMed]
- Giannoudis, P.V.; Dinopoulos, H.; Tsiridis, E. Bone substitutes: An update. Injury 2005, 36 (Suppl. S3), S20–S27. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, G.; Moghaddam, A. Allograft bone matrix versus synthetic bone graft substitutes. Injury 2011, 42 (Suppl. S2), S16–S21. [Google Scholar] [CrossRef]
- Turnbull, G.; Clarke, J.; Picard, F.; Riches, P.; Jia, L.; Han, F.; Li, B.; Shu, W. 3D bioactive composite scaffolds for bone tissue engineering. Bioact. Mater. 2018, 3, 278–314. [Google Scholar] [CrossRef]
- Blom, A.W.; Wylde, V.; Livesey, C. Impaction bone grafting of the acetabulum at hip revision using a mix of bone chips and a biphasic porous ceramic bone graft substitute. Acta Orthop. 2009, 80, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Cimatti, P.; Andreoli, I.; Busacca, M. An Observational Prospective Clinical Study for the Evaluation of a Collagen-Hydroxyapatite Composite Scaffold in Hip Revision Surgery. Clin. Med. 2022, 11, 6372. [Google Scholar] [CrossRef] [PubMed]
- Brodano, G.B.; Griffoni, C.; Zanotti, B.; Gasbarrini, A.; Bandiera, S.; Ghermandi, R.; Boriani, S. A post-market surveillance analysis of the safety of hydroxyapatite-derived products as bone graft extenders or substitutes for spine fusion. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 3548–3555. [Google Scholar]
- Liu, X.J.; Zhu, Q.S.; Sun, H.F. The clinical efficacy of hydroxyapatite and its composites in spinal reconstruction: A meta-analysis. Rev. Med. Pharmacol. Sci. 2022, 26, 4614–4624. [Google Scholar] [CrossRef]
- Marcacci, M.; Kon, E.; Moukhachev, V.; Lavroukov, A.; Kutepov, S.; Quarto, R.; Mastrogiacomo, M.; Cancedda, R. Stem Cells Associated with Macroporous Bioceramics for Long Bone Repair: 6- to 7-Year Outcome of a Pilot Clinical Study. Tissue Eng. 2007, 13, 947–955. [Google Scholar] [CrossRef]
- Mashhadinezhad, H.; Samini, F.; Zare, R. Comparison of outcomes and safety of using hydroxyapatite granules as a substitute for autograft in cervical cages for anterior cervical discectomy and interbody fusion. Arch. Bone Jt. Surg. 2014, 2, 37–42. [Google Scholar]


{kind=link}
{kind=link}
| Biomaterial | Osteoconductive | Osteoinductive | Osteogenic | Structural |
|---|---|---|---|---|
| Tricalcium Phosphate | + | - | - | ++ |
| Calcium Sulfate | + | - | - | ++ |
| Calcium Phosphate | + | - | - | +++ |
| Hydroxyapatite | ++ | + | + | + |
| Adverse Effect | Number of Patients (Percentage of the Total) | Bone Substitute Related (NO/YES) |
|---|---|---|
| Intolerance of fixation device | 2 (1.75%) | NO |
| Wound-healing problems | 2 (1.75%) | NO |
| ORIF failure | 2 (1.75%) | NO |
| Persistent pain | 2 (1.75%) | NO |
| Limited range of motion | 2 (1.75%) | NO |
| Malalignment | 1 (0.88%) | NO |
| Center | Number of Patients | Related AE (Percentage of the Total) |
|---|---|---|
| “M. Bufalini”—Cesena | 121 | 0 |
| “Maggiore”—Bologna | 81 | 1 * (1.23%) |
| “Osped. Degli Infermi”—Rimini | 65 | 0 |
| “Policlinico”—Modena | 51 | 2 * (3.92%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massari, L.; Saracco, A.; Marchesini, S.; Gambuti, E.; Delorenzi, A.; Caruso, G. Safety of a Porous Hydroxyapatite Bone Substitute in Orthopedics and Traumatology: A Multi-Centric Clinical Study. J. Funct. Morphol. Kinesiol. 2024, 9, 71. https://doi.org/10.3390/jfmk9020071
Massari L, Saracco A, Marchesini S, Gambuti E, Delorenzi A, Caruso G. Safety of a Porous Hydroxyapatite Bone Substitute in Orthopedics and Traumatology: A Multi-Centric Clinical Study. Journal of Functional Morphology and Kinesiology. 2024; 9(2):71. https://doi.org/10.3390/jfmk9020071
Chicago/Turabian StyleMassari, Leo, Achille Saracco, Sebastiano Marchesini, Edoardo Gambuti, Alessandro Delorenzi, and Gaetano Caruso. 2024. "Safety of a Porous Hydroxyapatite Bone Substitute in Orthopedics and Traumatology: A Multi-Centric Clinical Study" Journal of Functional Morphology and Kinesiology 9, no. 2: 71. https://doi.org/10.3390/jfmk9020071
APA StyleMassari, L., Saracco, A., Marchesini, S., Gambuti, E., Delorenzi, A., & Caruso, G. (2024). Safety of a Porous Hydroxyapatite Bone Substitute in Orthopedics and Traumatology: A Multi-Centric Clinical Study. Journal of Functional Morphology and Kinesiology, 9(2), 71. https://doi.org/10.3390/jfmk9020071