
Surgical Outcomes and Complications of Custom-Made Prostheses in Upper Limb Oncological Reconstruction: A Systematic Review

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction and Analysis
3. Results
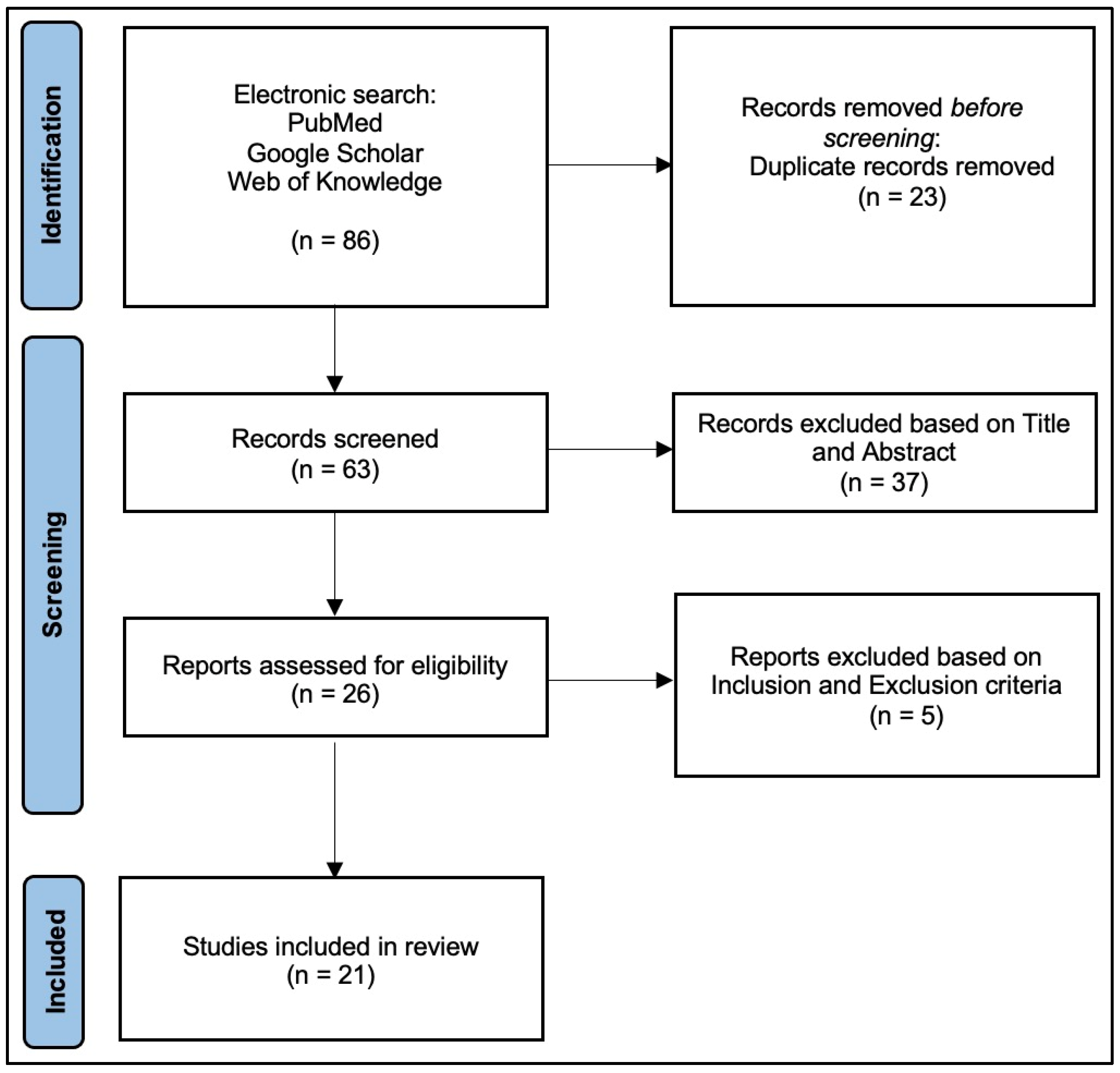
3.1. Search and Literature Selection
3.2. Characteristics and Evaluation of Studies
3.3. Demographics
3.4. Bone Segment or Joint Involved
3.5. Type of Tumor
3.6. Other Treatments
3.7. Surgical Complications
3.8. Functional Score
4. Discussion
Limitations and Strengths of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Perisano, C.; Greco, T.; Fulchignoni, C.; Maccauro, G. The IlluminOss® System: A Solution in Elderly Patients with Upper Limbs Bone Metastases. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Greco, T.; Fulchignoni, C.; Cianni, L.; Maccauro, G.; Perisano, C. Surgical Management of Tibial Metastases: A Systematic Review. Acta Biomed. Atenei Parm. 2022, 92, e2021552. [Google Scholar] [CrossRef]
- Spiro, I.J.; Rosenberg, A.E.; Springfield, D.; Suit, H. Combined Surgery and Radiation Therapy for Limb Preservation in Soft Tissue Sarcoma of the Extremity: The Massachusetts General Hospital Experience. Cancer Investig. 1995, 13, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Serletti, J.M.; Carras, A.J.; O’Keefe, R.J.; Rosier, R.N. Functional Outcome after Soft-Tissue Reconstruction for Limb Salvage after Sarcoma Surgery. Plast. Reconstr. Surg. 1998, 102, 1576–1583; discussion 1584–1585. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Chen, G.; Coles-Black, J.; Chuen, J.; Hardidge, A. Three-Dimensional Printing in Orthopaedic Preoperative Planning Improves Intraoperative Metrics: A Systematic Review. ANZ J. Surg. 2020, 90, 243–250. [Google Scholar] [CrossRef]
- Wong, K.C.; Kumta, S.M. Computer-Assisted Tumor Surgery in Malignant Bone Tumors. Clin. Orthop. Relat. Res. 2013, 471, 750–761. [Google Scholar] [CrossRef] [PubMed]
- Caravelli, S.; Ambrosino, G.; Vocale, E.; Di Ponte, M.; Puccetti, G.; Perisano, C.; Greco, T.; Rinaldi, V.G.; Marcheggiani Muccioli, G.M.; Zaffagnini, S.; et al. Custom-Made Implants in Ankle Bone Loss: A Retrospective Assessment of Reconstruction/Arthrodesis in Sequelae of Septic Non-Union of the Tibial Pilon. Medicina 2022, 58, 1641. [Google Scholar] [CrossRef] [PubMed]
- Hanna, S.A.; David, L.A.; Aston, W.J.S.; Gikas, P.D.; Blunn, G.W.; Cannon, S.R.; Briggs, T.W.R. Endoprosthetic Replacement of the Distal Humerus Following Resection of Bone Tumours. J. Bone Jt. Surg. Br. 2007, 89, 1498–1503. [Google Scholar] [CrossRef] [PubMed]
- Handels, H.; Ehrhardt, J.; Plötz, W.; Pöppl, S.J. Three-Dimensional Planning and Simulation of Hip Operations and Computer-Assisted Construction of Endoprostheses in Bone Tumor Surgery. Comput. Aided Surg. 2001, 6, 65–76. [Google Scholar] [CrossRef] [PubMed]
- Rooppakhun, S.; Surasith, P.; Vatanapatimakul, N.; Kaewprom, Y.; Sitthiseripratip, K. Craniometric Study of Thai Skull Based on Three-Dimensional Computed Tomography (CT) Data. J. Med. Assoc. Thai 2010, 93, 90–98. [Google Scholar]
- A Novel Rapid Prototyping and Finite Element Method-Based Development of the Patient-Specific Temporomandibular Joint Implant—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/22414075/ (accessed on 14 March 2024).
- Diment, L.E.; Thompson, M.S.; Bergmann, J.H. Three-Dimensional Printed Upper-Limb Prostheses Lack Randomised Controlled Trials: A Systematic Review. Prosthet. Orthot. Int. 2018, 42, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Campanacci, M.; Baldini, N.; Boriani, S.; Sudanese, A. Giant-Cell Tumor of Bone. J. Bone Jt. Surg. Am. 1987, 69, 106–114. [Google Scholar] [CrossRef]
- Malek, F.; Somerson, J.S.; Mitchel, S.; Williams, R.P. Does Limb-Salvage Surgery Offer Patients Better Quality of Life and Functional Capacity than Amputation? Clin. Orthop. Relat. Res. 2012, 470, 2000–2006. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Spindler, K.P.; Kuhn, J.E.; Dunn, W.; Matthews, C.E.; Harrell, F.E.; Dittus, R.S. Reading and Reviewing the Orthopaedic Literature: A Systematic, Evidence-Based Medicine Approach. J. Am. Acad. Orthop. Surg. 2005, 13, 220–229. [Google Scholar] [CrossRef] [PubMed]
- Enneking, W.F.; Spanier, S.S.; Goodman, M.A. A System for the Surgical Staging of Musculoskeletal Sarcoma. 1980. Clin. Orthop. Relat. Res. 2003, 415, 4–18. [Google Scholar] [CrossRef] [PubMed]
- Sambandam, S.N.; Gul, A.; Priyanka, P. Analysis of Methodological Deficiencies of Studies Reporting Surgical Outcome Following Cemented Total-Joint Arthroplasty of Trapezio-Metacarpal Joint of the Thumb. Int. Orthop. 2007, 31, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Lu, M.; Zhang, Y.; Gong, T.; Min, L.; Zhou, Y.; Luo, Y.; Tu, C. 3D-Printed Custom-Made Short Stem with Porous Structure for Fixation of Massive Endoprosthesis in Joint-Preserving Reconstruction after Tumor Resection. J. Orthop. Surg. Res. 2023, 18, 468. [Google Scholar] [CrossRef] [PubMed]
- Beltrami, G.; Ristori, G.; Nucci, A.M.; Galeotti, A.; Tamburini, A.; Scoccianti, G.; Campanacci, D.; Innocenti, M.; Capanna, R. Custom-Made 3D-Printed Implants as Novel Approach to Reconstructive Surgery after Oncologic Resection in Pediatric Patients. J. Clin. Med. 2021, 10, 1056. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Guo, W.; Yang, R.; Tang, S.; Yang, Y. Custom-Made Prosthesis Replacement for Reconstruction of Elbow after Tumor Resection. J. Shoulder Elb. Surg. 2009, 18, 796–803. [Google Scholar] [CrossRef]
- Vitiello, R.; Matrangolo, M.R.; El Motassime, A.; Perna, A.; Cianni, L.; Maccauro, G.; Ziranu, A. Three-Dimension-Printed Custom-Made Prosthetic Reconstructions in Bone Tumors: A Single Center Experience. Curr. Oncol. 2022, 29, 4566–4577. [Google Scholar] [CrossRef] [PubMed]
- Liang, H.; Yang, Y.; Guo, W.; Yan, L.; Tang, X.; Li, D.; Qu, H.; Zang, J.; Du, Z. Elbow Hemiarthroplasty with a 3D-Printed Megaprosthesis for Defects of the Distal Humerus or Proximal Ulna after Tumour Resection: A Preliminary Report. Bone Jt. J. 2022, 104-B, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Luo, Y.; Gong, T.; Wang, Y.; Zheng, C.; Min, L.; Tu, C.; Zhou, Y. Intercalary Reconstruction with Successful Joint Preservation by Uncemented 3D-printed Endoprosthesis Following Tumor Resection in Distal Radius: A Case Report. Exp. Ther. Med. 2022, 24, 719. [Google Scholar] [CrossRef] [PubMed]
- Szostakowski, B.; Staals, E.; Onwordi, L.; Pollock, R.; Skinner, J.A. Reconstruction with a Custom Made Prosthetic Wrist Arthrodesis after Bone Tumor Resections of the Distal Radius. Single Centre Experience. Rev. Bras. Ortop. 2021, 56, 224–229. [Google Scholar] [CrossRef]
- Beltrami, G.; Nucci, A.M.; Tamburini, A.; Innocenti, M. Custom-Made 3D-Printed Prosthesis and Free Vascularised Fibula for Humeral Reconstruction after Osteosarcoma Resection in a 13-Year-Old Patient. BMJ Case Rep. 2021, 14, e240726. [Google Scholar] [CrossRef] [PubMed]
- Kuptniratsaikul, V.; Luangjarmekorn, P.; Charoenlap, C.; Hongsaprabhas, C.; Kitidumrongsook, P. Anatomic 3D-Printed Endoprosthetic with Multiligament Reconstruction after En Bloc Resection in Giant Cell Tumor of Distal Radius. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2021, 5, e20.00178. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Min, L.; Lu, M.; Zhou, Y.; Wang, J.; Zhang, Y.; Yu, X.; Tang, F.; Luo, Y.; Duan, H.; et al. The Functional Outcomes and Complications of Different Reconstruction Methods for Giant Cell Tumor of the Distal Radius: Comparison of Osteoarticular Allograft and Three-Dimensional-Printed Prosthesis. BMC Musculoskelet. Disord. 2020, 21, 69. [Google Scholar] [CrossRef] [PubMed]
- Damert, H.G.; Kober, M.; Mehling, I. Custom-Made Wrist Prothesis (UNI-2TM) in a Patient with Giant Cell Tumor of the Distal Radius: 10-Year Follow-Up. Arch. Orthop. Trauma. Surg. 2020, 140, 2109–2114. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Liu, W.; Zeng, Q.; Wang, S.; Zhang, Z.; Liu, J.; Zhang, Y.; Shao, Z.; Wang, B. The Personalized Shoulder Reconstruction Assisted by 3D Printing Technology After Resection of the Proximal Humerus Tumours. Cancer Manag. Res. 2019, 11, 10665–10673. [Google Scholar] [CrossRef] [PubMed]
- Beltrami, G.; Ristori, G.; Scoccianti, G.; Tamburini, A.; Capanna, R.; Campanacci, D.; Innocenti, M. Latissimus Dorsi Rotational Flap Combined with a Custom-Made Scapular Prosthesis after Oncological Surgical Resection: A Report of Two Patients. BMC Cancer 2018, 18, 1003. [Google Scholar] [CrossRef] [PubMed]
- Pruksakorn, D.; Chantarapanich, N.; Arpornchayanon, O.; Leerapun, T.; Sitthiseripratip, K.; Vatanapatimakul, N. Rapid-Prototype Endoprosthesis for Palliative Reconstruction of an Upper Extremity after Resection of Bone Metastasis. Int. J. CARS 2015, 10, 343–350. [Google Scholar] [CrossRef] [PubMed]
- Damert, H.-G.; Altmann, S.; Kraus, A. Custom-Made Wrist Prosthesis in a Patient with Giant Cell Tumor of the Distal Radius. Arch. Orthop. Trauma. Surg. 2013, 133, 713–719. [Google Scholar] [CrossRef] [PubMed]
- Natarajan, M.; Sameer, M.; Kunal, D.; Balasubramanian, N. Custom-Made Endoprosthetic Total Humerus Reconstruction for Musculoskeletal Tumours. Int. Orthop. 2012, 36, 125–129. [Google Scholar] [CrossRef] [PubMed]
- McGrath, A.; Sewell, M.D.; Hanna, S.A.; Pollock, R.C.; Skinner, J.A.; Cannon, S.R.; Briggs, T.W.R. Custom Endoprosthetic Reconstruction for Malignant Bone Disease in the Humeral Diaphysis. Acta Orthop. Belg. 2011, 77, 171–179. [Google Scholar] [PubMed]
- Ahlmann, E.R.; Menendez, L.R. Intercalary Endoprosthetic Reconstruction for Diaphyseal Bone Tumours. J. Bone Jt. Surg. Br. 2006, 88, 1487–1491. [Google Scholar] [CrossRef] [PubMed]
- Rolf, O.; Gohlke, F. Endoprosthetic Elbow Replacement in Patients with Solitary Metastasis Resulting from Renal Cell Carcinoma. J. Shoulder Elb. Surg. 2004, 13, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Wu, Q.; Liu, J.; Chen, S.; Zhang, Z.; Shao, Z. What Are the Functional Results, Complications, and Outcomes of Using a Custom Unipolar Wrist Hemiarthroplasty for Treatment of Grade III Giant Cell Tumors of the Distal Radius? Clin. Orthop. Relat. Res. 2016, 474, 2583–2590. [Google Scholar] [CrossRef] [PubMed]
- Dhammi, I.K.; Kumar, S. Osteosarcoma: A Journey from Amputation to Limb Salvage. Indian. J. Orthop. 2014, 48, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Han, L.; He, Z.; Li, X.; Yang, S.; Yang, J.; Zhang, Y.; Li, D.; Yang, Y.; Yang, Z. Advances in Limb Salvage Treatment of Osteosarcoma. J. Bone Oncol. 2017, 10, 36–40. [Google Scholar] [CrossRef] [PubMed]
- D’Arienzo, A.; Ipponi, E.; Ruinato, A.D.; De Franco, S.; Colangeli, S.; Andreani, L.; Capanna, R. Proximal Humerus Reconstruction after Tumor Resection: An Overview of Surgical Management. Adv. Orthop. 2021, 2021, 5559377. [Google Scholar] [CrossRef] [PubMed]
- Perez, J.R.; Jose, J.; Mohile, N.V.; Boden, A.L.; Greif, D.N.; Barrera, C.M.; Conway, S.; Subhawong, T.; Ugarte, A.; Pretell-Mazzini, J. Limb Salvage Reconstruction: Radiologic Features of Common Reconstructive Techniques and Their Complications. J. Orthop. 2020, 21, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; Fishman, E.K.; Corl, F.; Carrino, J.A.; Weber, K.L.; Fayad, L.M. Imaging of Limb Salvage Surgery. AJR Am. J. Roentgenol. 2012, 198, 647–660. [Google Scholar] [CrossRef] [PubMed]
- Capanna, R.; Campanacci, D.A.; Belot, N.; Beltrami, G.; Manfrini, M.; Innocenti, M.; Ceruso, M. A New Reconstructive Technique for Intercalary Defects of Long Bones: The Association of Massive Allograft with Vascularized Fibular Autograft. Long-Term Results and Comparison with Alternative Techniques. Orthop. Clin. N. Am. 2007, 38, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Myers, G.J.C.; Abudu, A.T.; Carter, S.R.; Tillman, R.M.; Grimer, R.J. Endoprosthetic Replacement of the Distal Femur for Bone Tumours: Long-Term Results. J. Bone Jt. Surg. Br. 2007, 89, 521–526. [Google Scholar] [CrossRef] [PubMed]
- Gkavardina, A.; Tsagozis, P. The Use of Megaprostheses for Reconstruction of Large Skeletal Defects in the Extremities: A Critical Review. Open Orthop. J. 2014, 8, 384–389. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.G.; Burgess, E.M. The Use of CAD/CAM Technology in Prosthetics and Orthotics—Current Clinical Models and a View to the Future. J. Rehabil. Res. Dev. 2001, 38, 327–334. [Google Scholar]
- Lee, D.H.; Hills, J.M.; Jordanov, M.I.; Jaffe, K.A. Common Tumors and Tumor-like Lesions of the Shoulder. J. Am. Acad. Orthop. Surg. 2019, 27, 236–245. [Google Scholar] [CrossRef] [PubMed]
- SEER Cancer Statistics Review, 1975–2018. Available online: https://seer.cancer.gov/csr/1975_2018/index.html (accessed on 14 March 2024).
- Cecchini, M.G.; Wetterwald, A.; van der Pluijm, G.; Thalmann, G.N. Molecular and Biological Mechanisms of Bone Metastasis. EAU Update Ser. 2005, 3, 214–226. [Google Scholar] [CrossRef]
- Gautam, D.; Malhotra, R. Megaprosthesis versus Allograft Prosthesis Composite for Massive Skeletal Defects. J. Clin. Orthop. Trauma 2018, 9, 63–80. [Google Scholar] [CrossRef] [PubMed]
- Arguello, A.M.; Sullivan, M.H.; Mills, G.L.; Moran, S.L.; Houdek, M.T. Pedicled Functional Latissimus Flaps for Reconstruction of the Upper Extremity Following Resection of Soft-Tissue Sarcomas. Curr. Oncol. 2023, 30, 3138–3148. [Google Scholar] [CrossRef] [PubMed]
- Steinau, H.-U.; Daigeler, A.; Langer, S.; Steinsträsser, L.; Hauser, J.; Goertz, O.; Lehnhardt, M. Limb Salvage in Malignant Tumors. Semin. Plast. Surg. 2010, 24, 18–33. [Google Scholar] [CrossRef] [PubMed]
- Shine, J.; Efanov, J.I.; Paek, L.; Coeugniet, É.; Danino, M.A.; Izadpanah, A. Negative Pressure Wound Therapy as a Definitive Treatment for Upper Extremity Wound Defects: A Systematic Review. Int. Wound J. 2019, 16, 960–967. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year | Type of Study | No. Patients | M | F | Age | Location | Diagnosis | mCMS |
|---|---|---|---|---|---|---|---|---|
| Li et al., 2023 [19] | RE | 7 | 5 | 2 | 29.3 | Humerus/Radius | OS/ES | 47 |
| Vitiello et al., 2023 [22] | RE | 1 | 0 | 1 | 80 | Humerus | CS | 31 |
| Liang et al., 2022 [23] | CR | 1 | 0 | 1 | 49 | Humerus | Breast | 37 |
| Wang et al., 2022 [24] | CR | 1 | 1 | 0 | 14 | Radius | EH | 42 |
| Beltrami et al., 2021 [20] | RE | 4 | 1 | 3 | 13 | Humerus/Radius/Scapula | OS/EW/RS | 45 |
| Szostakowski et al., 2021 [25] | RE | 4 | 2 | 2 | 42 | Radius | GCT | 43 |
| Beltrami et al., 2021 [26] | CR | 1 | 0 | 1 | 13 | Humerus | OS | 42 |
| Kuptniratsaikul et al., 2021 [27] | CR | 1 | 0 | 1 | 34 | Radius | GCT | 42 |
| Wang et al., 2020 [28] | RE | 15 | 6 | 9 | 38 | Radius | GCT | 38 |
| Damert et al., 2020 [29] | CR | 1 | 1 | 0 | 36 | Radius | GCT | 37 |
| Hu et al., 2019 [30] | RE | 7 | 3 | 4 | 34.9 | Humerus | OS/CS/GCT | 43 |
| Beltrami et al., 2018 [31] | RE | 2 | 0 | 2 | 26.5 | Scapula | ES/SS | 43 |
| Wang et al., 2016 [38] | RE | 10 | 7 | 3 | 39 | Distal Radius | GCT | 46 |
| Pruksakorn et al., 2015 [32] | PR | 16 | / | / | 37.5 | Humers/Ulna | Metastasis | 53 |
| Damert et al., 2013 [33] | CR | 1 | 1 | 0 | 36 | Radius | GCT | 46 |
| Natarjan et al., 2012 [34] | RE | 11 | 6 | 5 | 17 | Humerus | OS/EW/AF | 47 |
| McGrath et al., 2011 [35] | RE | 13 | 9 | 4 | 35 | Humerus | ES/OS/CS/MFH/PS/Metastasis | 35 |
| Tang et al., 2009 [21] | RE | 26 | 10 | 6 | 38.8 | Humerus Ulna/Elbow | EW/OS/MFH/SS/Metastasis | 37 |
| Hanna et al., 2007 [8] | RE | 18 | 11 | 7 | 48.2 | Humerus | EW/GCT/OS/CS/Metastasis | 35 |
| Ahlmann and Menendez, 2006 [36] | RE | 1 | 1 | 0 | 66 | Humerus | Metastasis | 43 |
| Rolf and Gohlke, 2004 [37] | RE | 4 | 4 | 0 | 32 | Elbow | Metastasis | 35 |
| Total Cases | Male | Female | ||
|---|---|---|---|---|
| 145 | 86 (59.31%) | 59 (40.69%) | ||
| Mean age | 33.68 years old | |||
| Follow-up | Mean | 43.37 months | ||
| MSTS score | 112 (77%) | 59.35% | ||
| Location | Proximal Humerus | 35 (24.13%) | 19 | 16 |
| Distal Humerus | 37 (25.51%) | 24 | 13 | |
| Humeral Diaphysis | 21 (14.48%) | 13 | 8 | |
| Proximal Ulna | 6 (4.13%) | 4 | 2 | |
| Proximal Radius | 2 (1.37%) | 1 | 1 | |
| Distal Radius | 34 (23.44%) | 18 | 16 | |
| Scapula | 3 (2.06%) | 0 | 3 | |
| Elbow | 7 (4.82%) | 7 | 0 | |
| Diagnosis | Giant Cells Tumor | 36 (24.82%) | 20 | 16 |
| Osteosarcoma | 25 (17.24%) | 18 | 7 | |
| Ewing’s Sarcoma | 17 (11.72%) | 10 | 7 | |
| Chondrosarcoma | 7 (4.82%) | 2 | 5 | |
| Metastasis | 40 (27.58%) | 25 | 15 | |
| Others | 20 (13.79%) | 11 | 9 | |
| Complications | Aseptic loosening | 13 (8.96%) | ||
| Dislocation | 8 (5.51%) | |||
| Infection | 5 (3.44%) | |||
| Nerve Injury | 4 (2.75%) | |||
| Periprosthetic fractures | 4 (2.75%) | |||
| Hardware failure | 3 (2.06%) | |||
| Vascular Injury | 1 (0.68%) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fulchignoni, C.; Pietramala, S.; Lopez, I.; Mazzella, G.G.; Comisi, C.; Perisano, C.; Rocchi, L.; Greco, T. Surgical Outcomes and Complications of Custom-Made Prostheses in Upper Limb Oncological Reconstruction: A Systematic Review. J. Funct. Morphol. Kinesiol. 2024, 9, 72. https://doi.org/10.3390/jfmk9020072
Fulchignoni C, Pietramala S, Lopez I, Mazzella GG, Comisi C, Perisano C, Rocchi L, Greco T. Surgical Outcomes and Complications of Custom-Made Prostheses in Upper Limb Oncological Reconstruction: A Systematic Review. Journal of Functional Morphology and Kinesiology. 2024; 9(2):72. https://doi.org/10.3390/jfmk9020072
Chicago/Turabian StyleFulchignoni, Camillo, Silvia Pietramala, Ivo Lopez, Giovan Giuseppe Mazzella, Chiara Comisi, Carlo Perisano, Lorenzo Rocchi, and Tommaso Greco. 2024. "Surgical Outcomes and Complications of Custom-Made Prostheses in Upper Limb Oncological Reconstruction: A Systematic Review" Journal of Functional Morphology and Kinesiology 9, no. 2: 72. https://doi.org/10.3390/jfmk9020072