Dolutegravir (DTG) is a potent anti-HIV drug that is used to treat HIV globally. There have been reports of mutations in the HIV-1 3′-polypurine tract (3′PPT) of the
nef gene, contributing to DTG failure; however, there are limited ‘real-world’ data on this. In
[...] Read more.
Dolutegravir (DTG) is a potent anti-HIV drug that is used to treat HIV globally. There have been reports of mutations in the HIV-1 3′-polypurine tract (3′PPT) of the
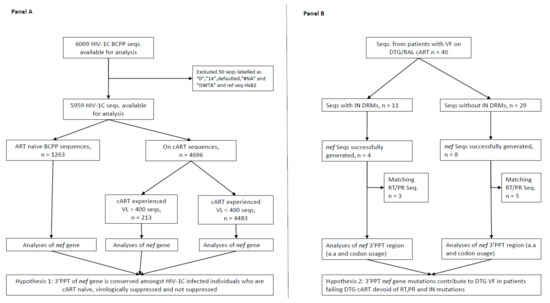
nef gene, contributing to DTG failure; however, there are limited ‘real-world’ data on this. In addition, there is a knowledge gap on the variability of 3′PPT residues in patients receiving combination antiretroviral therapy (cART) with and without viral load (VL) suppression. HIV-1 subtype C (HIV-1C) whole-genome sequences from cART naïve and experienced individuals were generated using next-generation sequencing. The
nef gene sequences were trimmed from the generated whole-genome sequences using standard bioinformatics tools. In addition, we generated separate integrase and
nef gene sequences by Sanger sequencing of plasma samples from individuals with virologic failure (VF) while on a DTG/raltegravir (RAL)-based cART. Analysis of 3′PPT residues was performed, and comparison of proportions computed using Pearson’s chi-square test with
p-values < 0.05 was considered statistically significant. A total of 6009 HIV-1C full genome sequences were generated and had a median log
10 HIV-1 VL (Q1, Q3) copies/mL of 1.60 (1.60, 2.60). A total of 12 matching integrase and
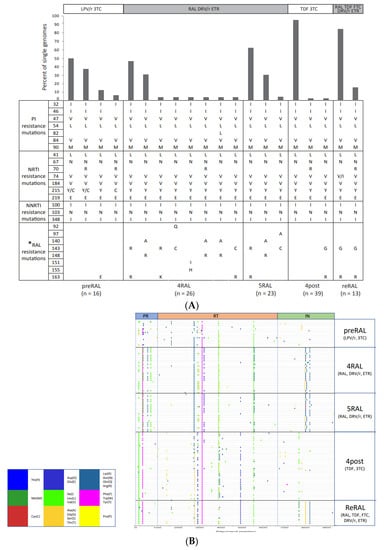
nef gene sequences from therapy-experienced participants failing DTG/ RAL-based cART were generated. HIV-1C 3′PPT
nef gene sequences from therapy-experienced patients failing DTG cART (
n = 12), cART naïve individuals (
n = 1263), and individuals on cART with and without virological suppression (
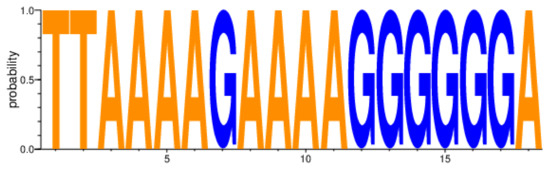
n = 4696) all had a highly conserved 3′PPT motif with no statistically significant differences identified. Our study confirms the high conservation of the HIV-1
nef gene 3′PPT motif in ‘real-world’ patients and showed no differences in the motif according to VL suppression or INSTI-based cART failure. Future studies should explore other HIV-1 regions outside of the pol gene for associations with DTG failure.
Full article






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}