1. Introduction
The spread of antibiotic-resistant pathogens leads to serious health threats that affect clinical outcomes, including higher mortality rates and increased healthcare costs. A relevant review by Jim O’Neil in 2014 estimated that antimicrobial resistance could cause 10 million deaths each year by 2050 [
1]. Since 2014, the World Health Organization, European Union, the United Kingdom, and the United States have submitted strategic action plans to tackle the increasing challenge of antimicrobial resistance [
2,
3,
4]. In accordance with these guidelines, the National Action Plan on Antimicrobial Resistance was formulated in Japan in April 2016. The goals of the plan were to reduce the use of oral broad-spectrum antimicrobials, such as quinolones, cephalosporins, and macrolides (documented in 2013) by 50% by the year 2020 [
5]. To address this objective, in June 2017 and December 2019, the Government of Japan’s Ministry of Health, Labor, and Welfare issued the 1st and 2nd Edition of the
Manual of Antimicrobial Stewardship, respectively [
6,
7]. The goal of these manuals was to promote appropriate clinical management of infectious diseases as well as to reduce inappropriate and unnecessary use of antimicrobial agents without worsening patient outcomes [
6,
7]. To prevent the spread of antimicrobial resistance, optimal antimicrobial therapy was introduced in various hospitals.
The overuse and misuse of broad-spectrum antibiotics may lead to the development of resistant mutations and are associated with the following: antimicrobial resistance to bacteria, longer duration of hospital stay, increased medical costs, and increased risk of adverse drug reactions [
8,
9]. Overuse of quinolones induces resistance in bacteria through mechanisms such as specific mutations in the quinolone resistance-determining region or overexpression of efflux pumps [
10]. Therefore, reductions in inappropriate and unnecessary quinolone prescriptions are required to restrict the development of resistant pathogens. However, the prescription of broad-spectrum antibiotics is more common in Japan than in Europe and the United States [
5]. In particular, the use of oral quinolones in Japan increased from 2009 to 2013 [
11]. Antimicrobial stewardship programs (ASPs), including educational interventions, have been associated with appropriate antibiotic use, reduced prevalence of antibiotic-resistant pathogens, and improved clinical outcomes [
12,
13,
14]. Therefore, in addition to the issuance of several global and national ASP guidelines, we began conducting educational lectures in our hospital to promote appropriate oral quinolone usage. However, it remains unknown how antimicrobial therapy and the prevalence of resistant pathogens have changed in our hospital. The purpose of this study was to retrospectively investigate the prescription characteristics, oral quinolone use, and the antibiotic susceptibility of bacteria in our hospital from 2013 to 2020.
3. Discussion
In Japan, oral quinolone use increased from 2009 to 2013 [
11], and in 2016, Japan’s National Action Plan on Antimicrobial Resistance was implemented to achieve a 50% reduction in the use of broad-spectrum antibiotics by 2020 using the year 2013 as baseline [
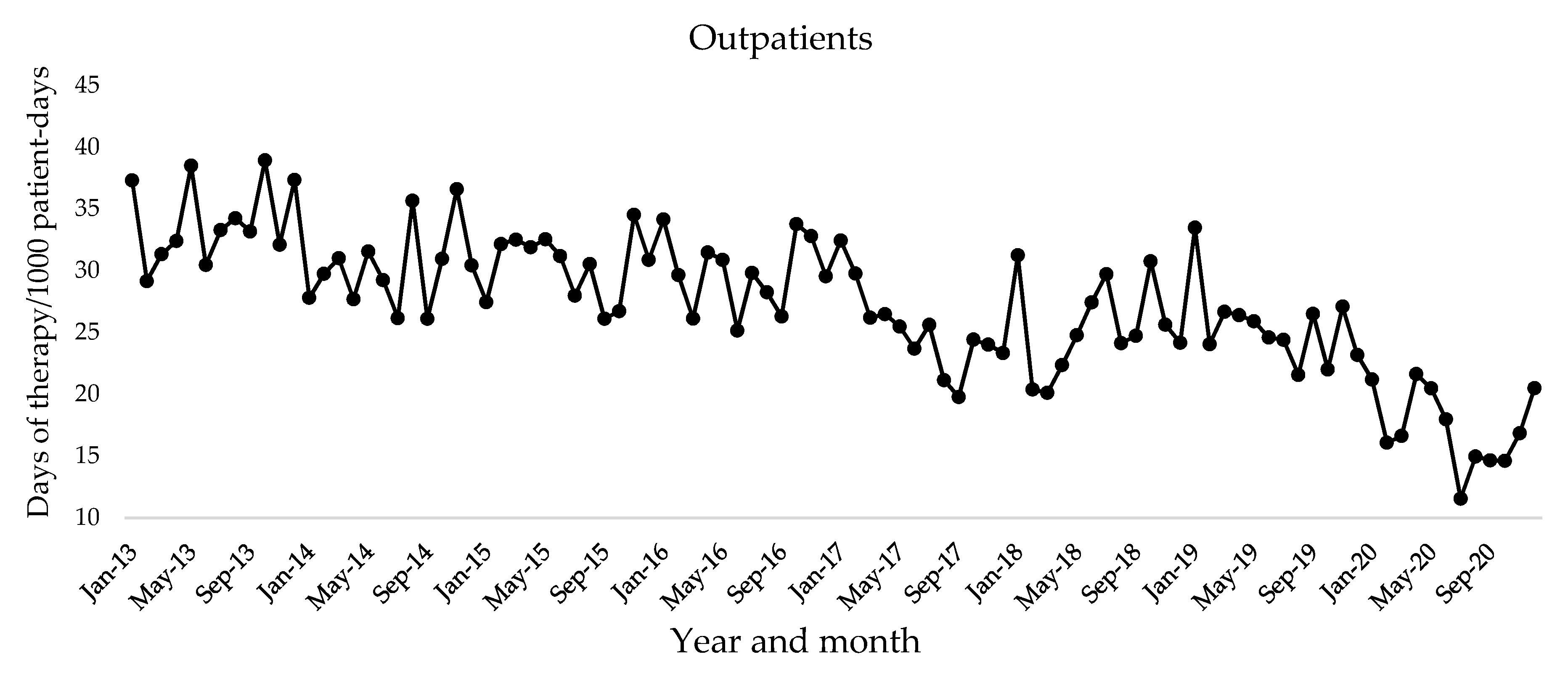
5]. The purpose of this study was to retrospectively investigate the following: prescription characteristics, antimicrobial use, and microbiological data from 2013 to 2020 in our hospital. We found a significant reduction in the prescription of oral quinolones for inappropriate indications from 2013 to 2020. A significant decrease in the oral use of quinolones for outpatients was observed in 2014, with a reduction to 49% by 2020. Furthermore, there was a positive trend in the susceptibility of
P. aeruginosa to levofloxacin. These results show that oral quinolone use was further reduced after educational intervention, and the susceptibility to
P. aeruginosa increased with optimal quinolone usage compared to that noted in 2013.
We previously reported that educational lectures are effective in reducing the use of oral third-generation cephalosporins [
15]. Educational intervention commenced in 2018, and the monthly mean DOTs per 1000 patient-days of oral quinolone for outpatients significantly decreased by 49% in 2020 compared to 2013. However, before the educational intervention, oral quinolone use had significantly decreased by 11% in 2014 and remained at a low level thereafter. Since 2014, several global and national guidelines were published to tackle the spread of antimicrobial resistance [
2,
3,
4,
5,
6,
7]. These guidelines may have affected changes in the prescriptions of oral quinolones. The
Manuals of Antimicrobial Stewardship state that patients with acute respiratory tract infections and acute diarrhea should not be prescribed antibiotics [
6,
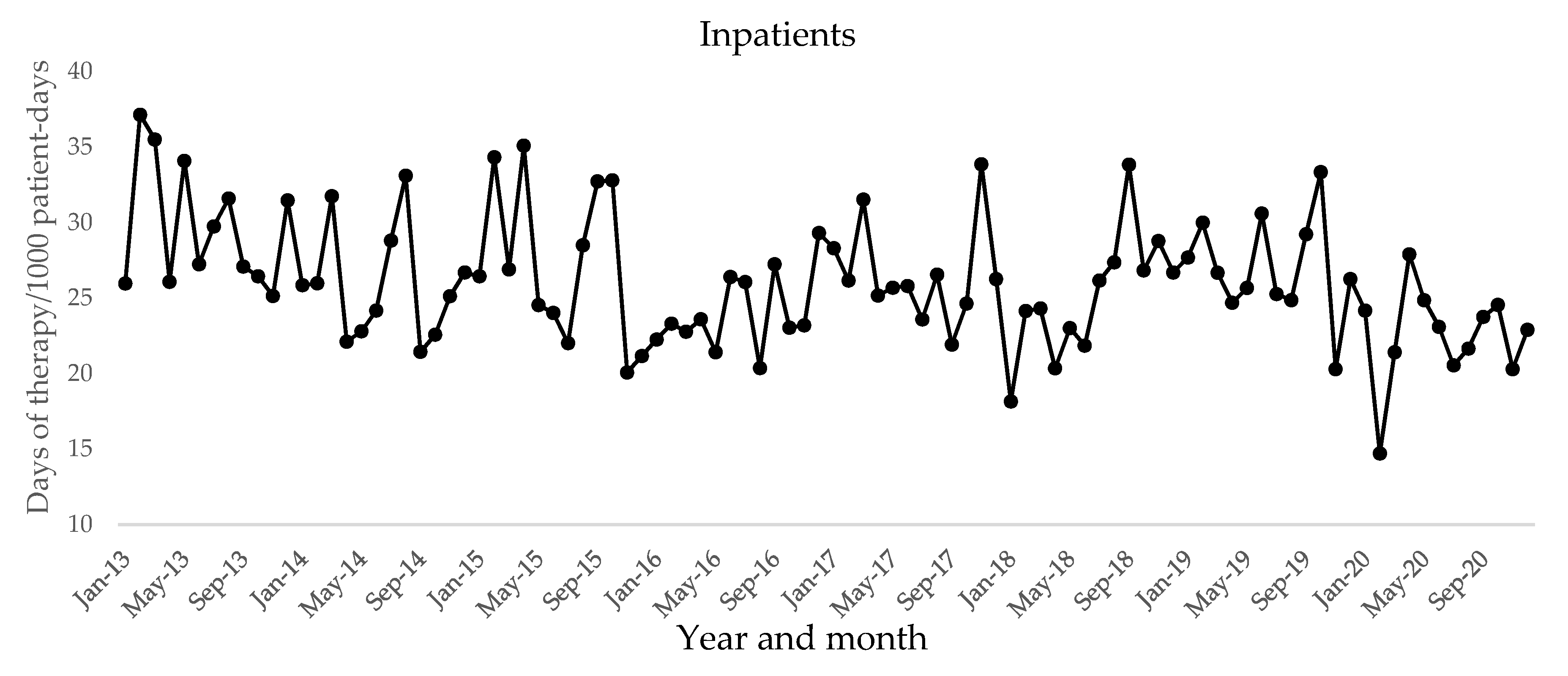
7]. In this study, to investigate the number of prescriptions for oral quinolones, representative data were collected during December 2013, December 2019, and December 2020. We found a significant reduction in unnecessary antibiotic prescriptions for outpatients. However, no prescriptions for these conditions were detected in hospitalized patients. This was because patients prescribed unnecessary antibiotics are usually mild and are treated in outpatient settings; therefore, they are not commonly treated as inpatient in hospitals. According to Asian guidelines for the prevention of surgical site infections, quinolones should be used as alternative agents for patients with a penicillin allergy [
16,
17]. We previously reported a reduction in the use of oral quinolones for outpatients in the Department of Oral and Maxillofacial Surgery between 2013 and 2018 after adopting the National Action Plan [
18]. Consistent with these reports, we found that prescriptions of oral quinolones were significantly reduced for perioperative prophylaxis in inpatients and dental infections in outpatients. The guidelines for acute cholangitis and cholecystitis recommend that quinolones should be prescribed to patients with a beta-lactam allergy or if the isolate is susceptible to quinolones [
19].
Bacteroides fragilis is one of the commonly isolated commensals in patients with intra-abdominal infections, and antibiotics used against anaerobic infections are often selected as empiric therapy [
20]. Most oral quinolones used in Japan have no activity against anaerobes [
21], and thus, oral quinolone use is considered to be inappropriate for these infections. In the present study, there was a significant reduction in the number of prescriptions for inpatients with intra-abdominal infections. These findings suggest that global and national guidelines, as well as educational interventions, may contribute to a significant downtrend in the use of oral quinolones. Although we found a considerable reduction in the use of oral quinolone for outpatients, no significant changes were detected in the number of patients who received intravenous therapy after oral quinolone prescriptions. This indicates that the reduction in quinolone prescription did not negatively influence the outcomes for these patients.
Prior use of broad-spectrum antibiotics, including quinolones, is a risk factor for acquiring quinolone-resistant
E. coli infections, which is an independent predictor of mortality [
22,
23]. Switching to narrower spectrum coverage antibiotics can prevent unnecessary broad-spectrum antimicrobial use, improve patient outcomes, and be cost effective in the treatment of infectious diseases [
24,
25]. A retrospective observational study demonstrated that the resistance rates of
E. coli and
P. aeruginosa to quinolones decreased through the reduced consumption of antibiotics and surgical antibiotic prophylaxis [
26]. In this study, we investigated the susceptibility of
P. aeruginosa,
E. coli and
K. pneumoniae because these bacteria have high antimicrobial resistance patterns and are commonly detected as sources of community and hospital infections. The susceptibility of
P. aeruginosa to levofloxacin significantly increased from 84.7% in 2013 to 93.3% in 2015 and remained at high levels during the study period. This improved susceptibility may be due to the reduction in unnecessary quinolone use. There were no significant changes in the susceptibility of
E. coli and
K. pneumoniae; E. coli is the most common bacteria identified in urinary tract infections, followed by
K. pneumoniae. In the Japanese guidelines for clinical management of infectious diseases, oral quinolones are recommended as the first-line empiric antibiotics for these conditions [
27]; a significant increase was observed in the number of oral quinolone prescriptions for outpatients in 2019. The unchanged susceptibility to levofloxacin may be related to the increase in the number of oral quinolone prescriptions for urinary tract infections in outpatients. The susceptibility of
E. coli was low (in the 70% range) throughout the study period. In Kobe, non-extended-spectrum-β-lactamase-producing
E. coli and
K. pneumoniae have approximately 90% susceptibility to first-generation cephalosporins [
28], and the Infectious Diseases Society of America guidelines recommend trimethoprim/sulfamethoxazole as an appropriate choice for therapy [
29]. A previous study reported that restriction of oral quinolone use could lead to an increase in the susceptibility of
E. coli [
30]. To further increase susceptibility, oral quinolone use should be decreased and replaced with narrow-spectrum antibiotics.
Between December 2019 and December 2020, significant reductions were observed in the number of prescriptions for infections not requiring antibiotic prescriptions and acute respiratory tract infections. Since the beginning of 2020, we provided additional lectures directly to the representative physicians from the departments where no particular improvement was observed. This intervention could have led to the reductions in 2020; however, the world faced the threat of the coronavirus disease 2019 (COVID-19) pandemic. Many hospitals struggled with the problems posed by COVID-19, such as delaying or avoiding medical care for non-urgent cases [
31]. The COVID-19 pandemic may have influenced the pattern of prescribing oral antibiotics in the year 2020.
This study had some limitations. Since it was conducted at a single institution and focused on the low incidence of non-susceptible strains to quinolones, our findings may not be generalizable. The indications for antibiotic use were collected by reviewing each patient’s medical records. We collected data over three months as representative data; hence, a measurement and sample size bias may exist. Because the study was conducted retrospectively, we could not directly assess the impact of the guidelines on physician prescribing trends. In many cases, physicians tend to shift their prescription preferences rather than using oral quinolones; however, to accurately assess the changes in oral quinolone use, we excluded the data on patients who required long-term oral quinolone prescriptions. This makes it difficult to investigate trends in the use of other antibiotics. In 2020, COVID-19 wreaked havoc in many hospital settings worldwide. Influences of COVID-19 on the prescription of antibiotics were reported [
32,
33]. To assess changes due to COVID-19 in the number of prescriptions, we compared the data between 2019 and 2020; however, the impact of COVID-19 on the results from 2020 could not be sufficiently investigated. Lastly, we implemented other ASPs, such as audit and feedback programs to promote appropriate intravenous antibiotic use [
13,
34], and educational interventions to optimize oral third-cephalosporin use during the investigation period [
15,
18]. Therefore, we may not have fully evaluated the effects of our educational interventions to promote appropriate oral quinolone use.


 ,
, 


{kind=link}
{kind=link}