
Robust Ultrafast Projection Pipeline for Structural and Angiography Imaging of Fourier-Domain Optical Coherence Tomography


Abstract
1. Introduction
2. Materials and Methods
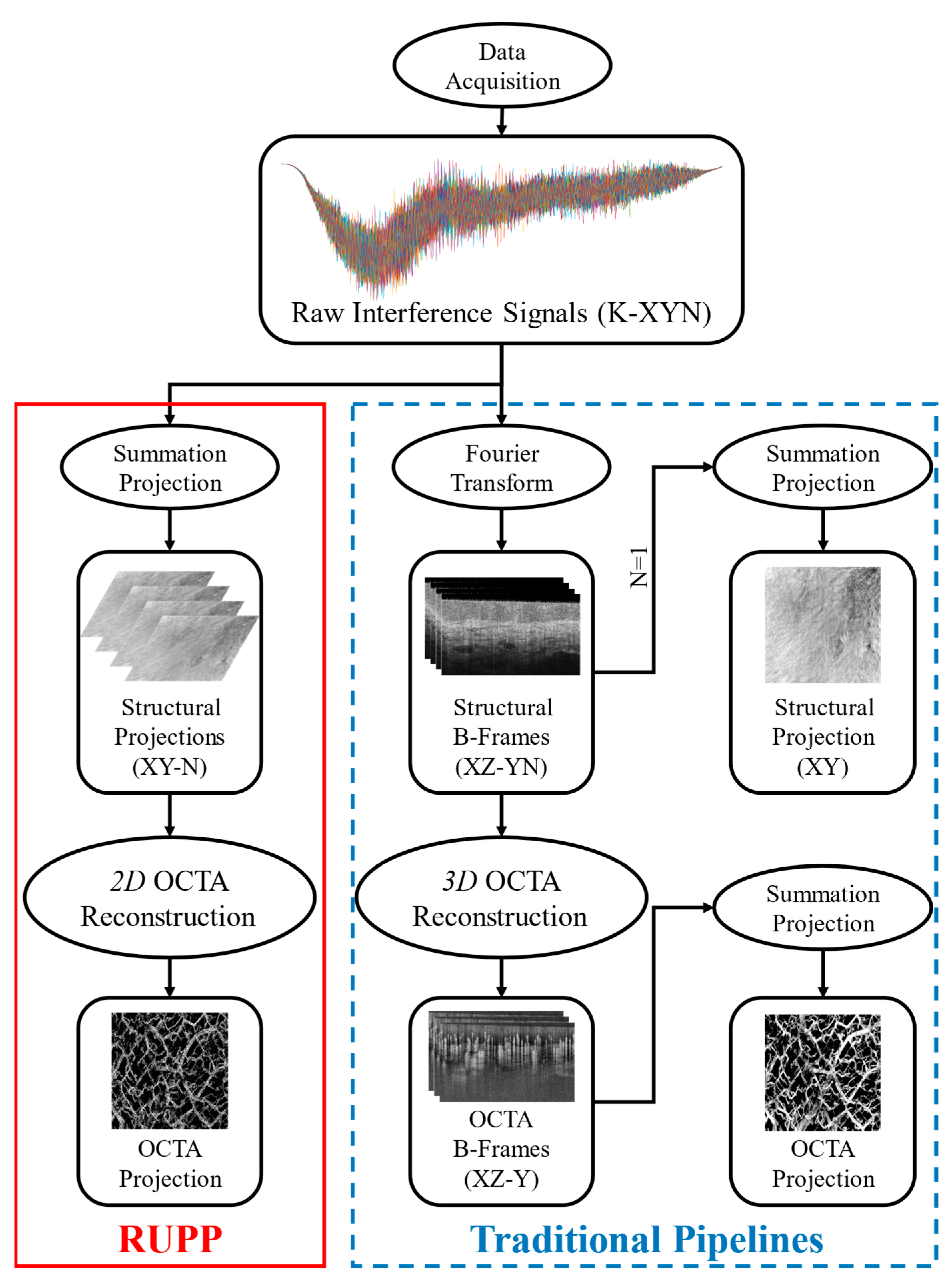
2.1. Mathematics Explanations
2.2. Experiment Setup and Participants
2.3. Evaluation Methods
3. Results
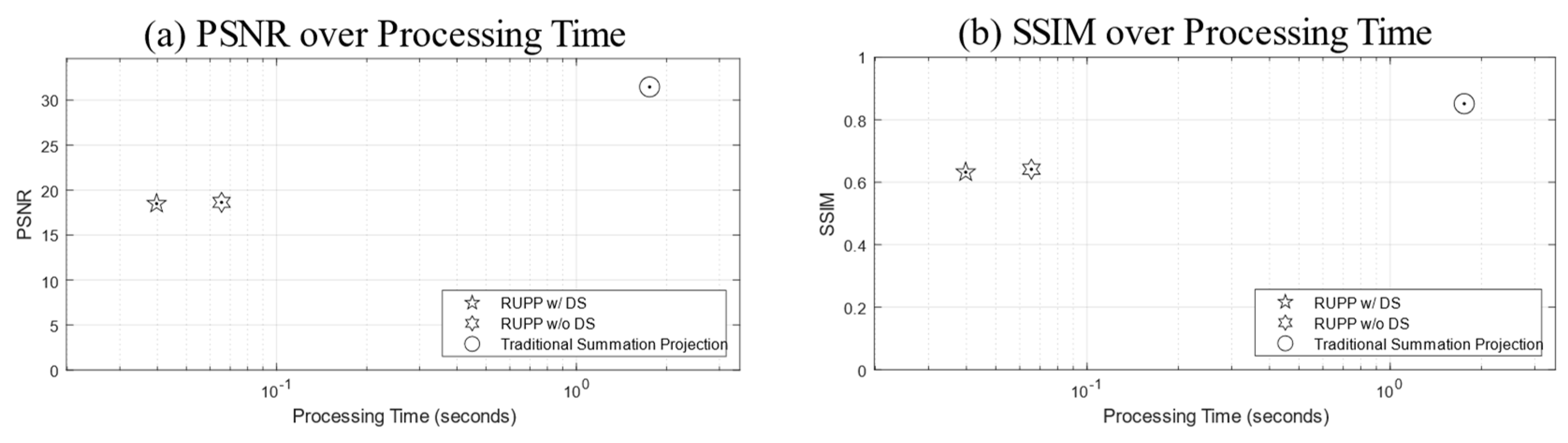
3.1. Structural Projections
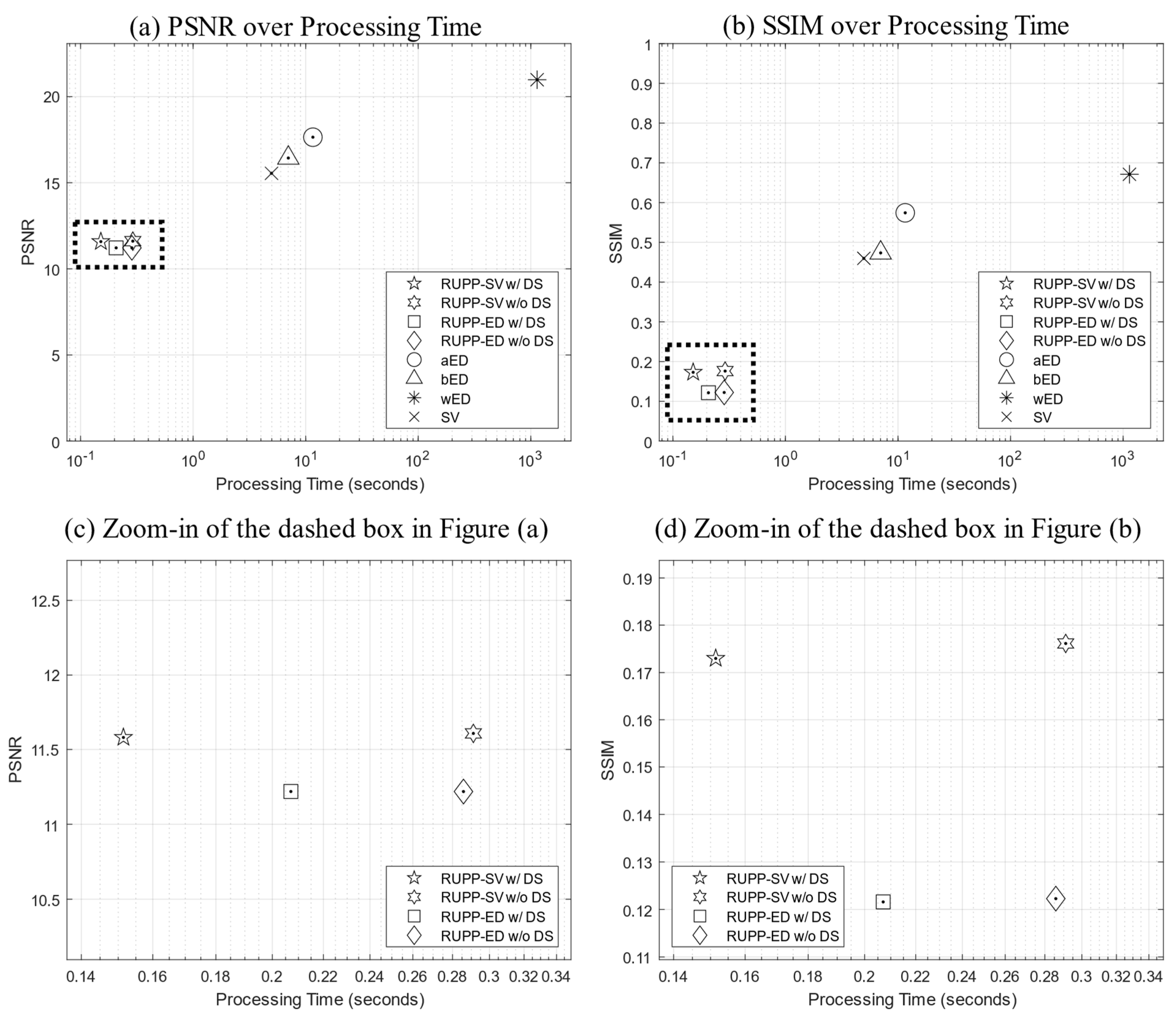
3.2. Angiography Projections
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, D.; Swanson, E.A.; Lin, C.P.; Schuman, J.S.; Stinson, W.G.; Chang, W.; Hee, M.R.; Flotte, T.; Gregory, K.; Puliafito, C.A.; et al. Optical Coherence Tomography. Science 1991, 254, 1178. [Google Scholar] [CrossRef] [PubMed]
- Fujimoto, J.G.; Pitris, C.; Boppart, S.A.; Brezinski, M.E. Optical Coherence Tomography: An Emerging Technology for Biomedical Imaging and Optical Biopsy. Neoplasia 2000, 2, 9. [Google Scholar] [CrossRef]
- Tomlins, P.H.; Wang, R.K. Theory, Developments and Applications of Optical Coherence Tomography. J. Phys. D Appl. Phys. 2005, 38, 2519. [Google Scholar] [CrossRef]
- Fercher, A.F.; Drexler, W.; Hitzenberger, C.K.; Lasser, T. Optical Coherence Tomography—Principles and Applications. Rep. Prog. Phys. 2003, 66, 239. [Google Scholar] [CrossRef]
- Leitgeb, R.; Fercher, A.F.; Hitzenberger, C.K. Performance of Fourier Domain vs. Time Domain Optical Coherence Tomography. Opt. Express 2003, 11, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-L.; Wang, R.K. Optical Coherence Tomography Based Angiography [Invited]. Biomed. Opt. Express 2017, 8, 1056–1082. [Google Scholar] [CrossRef] [PubMed]
- de Carlo, T.E.; Romano, A.; Waheed, N.K.; Duker, J.S. A Review of Optical Coherence Tomography Angiography (OCTA). Int. J. Retin. Vitr. 2015, 1, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Spaide, R.F.; Fujimoto, J.G.; Waheed, N.K.; Sadda, S.R.; Staurenghi, G. Optical Coherence Tomography Angiography. Prog. Retin. Eye Res. 2018, 64, 1–55. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.S.; Jia, Y.; Zhang, M.; Su, J.P.; Liu, G.; Hwang, T.S.; Bailey, S.T.; Huang, D. Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, OCT27–OCT36. [Google Scholar] [CrossRef]
- Zhang, A.; Zhang, Q.; Chen, C.-L.; Wang, R.K. Methods and Algorithms for Optical Coherence Tomography-Based Angiography: A Review and Comparison. J. Biomed. Opt. 2015, 20, 100901. [Google Scholar] [CrossRef]
- Jia, Y.; Bailey, S.T.; Hwang, T.S.; McClintic, S.M.; Gao, S.S.; Pennesi, M.E.; Flaxel, C.J.; Lauer, A.K.; Wilson, D.J.; Hornegger, J.; et al. Quantitative Optical Coherence Tomography Angiography of Vascular Abnormalities in the Living Human Eye. Proc. Natl. Acad. Sci. USA 2015, 112, E2395–E2402. [Google Scholar] [CrossRef] [PubMed]
- Hagag, A.M.; Gao, S.S.; Jia, Y.; Huang, D. Optical Coherence Tomography Angiography: Technical Principles and Clinical Applications in Ophthalmology. Taiwan J. Ophthalmol. 2017, 7, 115–129. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.; Drexler, W. Optical Coherence Tomography Angiography and Photoacoustic Imaging in Dermatology. Photochem. Photobiol. Sci. 2020, 18, 945–962. [Google Scholar] [CrossRef] [PubMed]
- Ulrich, M.; Themstrup, L.; De Carvalho, N.; Manfredi, M.; Grana, C.; Ciardo, S.; Kästle, R.; Holmes, J.; Whitehead, R.; Jemec, G.B.E.; et al. Dynamic Optical Coherence Tomography in Dermatology. Dermatology 2016, 232, 298–311. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.-T.; Chen, Y.; Lee, C.-Y.; Huang, B.-H.; Trung, N.H.; Lee, Y.-J.; Wang, Y.-L. Noninvasive Structural and Microvascular Anatomy of Oral Mucosae Using Handheld Optical Coherence Tomography. Biomed. Opt. Express 2017, 8, 5001. [Google Scholar] [CrossRef] [PubMed]
- Le, N.M.; Song, S.; Zhou, H.; Xu, J.; Li, Y.; Sung, C.E.; Sadr, A.; Chung, K.H.; Subhash, H.M.; Kilpatrick, L.; et al. A Noninvasive Imaging and Measurement Using Optical Coherence Tomography Angiography for the Assessment of Gingiva: An in Vivo Study. J. Biophotonics 2018, 11, e201800242. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Shepherd, S.; Huang, Z.; Li, C.; Macluskey, M. Development of an Intraoral Handheld Optical Coherence Tomography-Based Angiography Probe for Multi-Site Oral Imaging. Opt. Lett. 2023, 48, 4857–4860. [Google Scholar] [CrossRef] [PubMed]
- Leitgeb, R.A. En Face Optical Coherence Tomography: A Technology Review [Invited]. Biomed. Opt. Express 2019, 10, 2177. [Google Scholar] [CrossRef] [PubMed]
- Rogers, J.A.; Dunne, S.; Jackson, D.A.; Podoleanu, A.G. Three Dimensional OCT Images from Retina and Skin. Opt. Express 2000, 7, 292–298. [Google Scholar] [CrossRef]
- Yousefi, S.; Zhi, Z.; Wang, R.K. Eigendecomposition-Based Clutter Filtering Technique for Optical Microangiography. IEEE Trans. Biomed. Eng. 2011, 58, 2316–2323. [Google Scholar] [CrossRef]
- Zhang, Q.; Wang, J.; Wang, R.K. Highly Efficient Eigen Decomposition Based Statistical Optical Microangiography. Quant. Imaging Med. Surg. 2016, 6, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Wolff, B.; Matet, A.; Vasseur, V.; Sahel, J.A.; Mauget-Faÿsse, M. En Face OCT Imaging for the Diagnosis of Outer Retinal Tubulations in Age-Related Macular Degeneration. J. Ophthalmol. 2012, 2012, 542417. [Google Scholar] [CrossRef] [PubMed]
- Riazi-Esfahani, H.; Khalili Pour, E.; Fadakar, K.; Ebrahimiadib, N.; Ghassemi, F.; Nourinia, R.; Khojasteh, H.; Attarian, B.; Faghihi, H.; Ahmadieh, H. Multimodal Imaging for Paracentral Acute Maculopathy; the Diagnostic Role of En Face OCT. Int. J. Retin. Vitr. 2021, 7, 13. [Google Scholar] [CrossRef] [PubMed]
- Kostanyan, T.; Wollstein, G.; Schuman, J.S. OCT Technique—Past, Present and Future. In OCT in Central Nervous System Diseases: The Eye as a Window to the Brain; Springer: Cham, Switzerland, 2016; pp. 7–34. [Google Scholar] [CrossRef]
- Ji, Y.; Yang, S.; Zhou, K.; Rocliffe, H.R.; Pellicoro, A.; Cash, J.L.; Wang, R.; Li, C.; Huang, Z. Deep-Learning Approach for Automated Thickness Measurement of Epithelial Tissue and Scab Using Optical Coherence Tomography. J. Biomed. Opt. 2022, 27, 015002. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Zheng, F.; Motulsky, E.H.; Gregori, G.; Chu, Z.; Chen, C.L.; Li, C.; De Sisternes, L.; Durbin, M.; Rosenfeld, P.J.; et al. A Novel Strategy for Quantifying Choriocapillaris Flow Voids Using Swept-Source OCT Angiography. Investig. Ophthalmol. Vis. Sci. 2018, 59, 203. [Google Scholar] [CrossRef] [PubMed]
- Ji, Y.; Yang, S.; Zhou, K.; Li, C.; Huang, Z. A Machine Learning Based Quantitative Data Analysis for Screening Skin Abnormality Based on Optical Coherence Tomography Angiography (OCTA). In Proceedings of the IEEE International Ultrasonics Symposium, IUS, Xi’an, China, 11–16 September 2021. [Google Scholar] [CrossRef]
- Gao, S.S.; Jia, Y.; Liu, L.; Zhang, M.; Takusagawa, H.L.; Morrison, J.C.; Huang, D. Compensation for Reflectance Variation in Vessel Density Quantification by Optical Coherence Tomography Angiography. Investig. Ophthalmol. Vis. Sci. 2016, 57, 4485–4492. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jia, Y.; Hwang, T.S.; Bailey, S.T.; Huang, D.; Hormel, T.T. Maximum Value Projection Produces Better En Face OCT Angiograms than Mean Value Projection. Biomed. Opt. Express 2018, 9, 6412–6424. [Google Scholar] [CrossRef]
- Zhang, T.; Zhou, K.; Rocliffe, H.R.; Pellicoro, A.; Cash, J.L.; Wang, W.; Wang, Z.; Li, C.; Huang, Z. Windowed Eigen-Decomposition Algorithm for Motion Artifact Reduction in Optical Coherence Tomography-Based Angiography. Appl. Sci. 2022, 13, 378. [Google Scholar] [CrossRef]
- Li, M.; Chen, Y.; Ji, Z.; Xie, K.; Yuan, S.; Chen, Q.; Li, S. Image Projection Network: 3D to 2D Image Segmentation in OCTA Images. IEEE Trans. Med. Imaging 2020, 39, 3343–3354. [Google Scholar] [CrossRef]
- Cooley, J.W.; Lewis, P.A.; Welch, P.D. The Finite Fourier Transform. IEEE Trans. Audio Electroacoust. 1969, 17, 77–85. [Google Scholar] [CrossRef]
- Jiang, J.; Mariampillai, A.; Yang, V.X.D.; Cable, A.; Standish, B.A.; Munce, N.R.; Leung, M.K.K.; Khurana, M.; Moriyama, E.H.; Wilson, B.C.; et al. Speckle Variance Detection of Microvasculature Using Swept-Source Optical Coherence Tomography. Opt. Lett. 2008, 33, 1530–1532. [Google Scholar] [CrossRef]
- Wang, R.K.; Jacques, S.L.; Ma, Z.; Hurst, S.; Hanson, S.R.; Gruber, A.; Fercher, A.; Drexler, W.; Hitzenberger, C.K.; Lasser, T.; et al. Three Dimensional Optical Angiography. Opt. Express 2007, 15, 4083–4097. [Google Scholar] [CrossRef] [PubMed]
- Biedermann, B.R.; Wieser, W.; Eigenwillig, C.M.; Palte, G.; Adler, D.C.; Srinivasan, V.J.; Fujimoto, J.G.; Huber, R. Real Time En Face Fourier-Domain Optical Coherence Tomography with Direct Hardware Frequency Demodulation. Opt. Lett. 2008, 33, 2556. [Google Scholar] [CrossRef]
- Wei, X.; Camino, A.; Pi, S.; Hormel, T.T.; Cepurna, W.; Huang, D.; Morrison, J.C.; Jia, Y. Real-Time Cross-Sectional and En Face OCT Angiography Guiding High-Quality Scan Acquisition. Opt. Lett. 2019, 44, 1431–1434. [Google Scholar] [CrossRef] [PubMed]
- Benedetto, J.J.; Zimmermann, G. Sampling Multipliers and the Poisson Summation Formula. J. Fourier Anal. Appl. 1997, 3, 505–523. [Google Scholar] [CrossRef]
- Fischer, J.V.; Srivastava, H.M. On the Duality of Discrete and Periodic Functions. Mathematics 2015, 3, 299–318. [Google Scholar] [CrossRef]
- Kruse, D.E.; Ferrara, K.W. A New High Resolution Color Flow System Using an Eigendecomposition-Based Adaptive Filter for Clutter Rejection. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 2002, 49, 1384–1399. [Google Scholar] [CrossRef]
- Aumann, S.; Donner, S.; Fischer, J.; Müller, F. Optical Coherence Tomography (OCT): Principle and Technical Realization. In High Resolution Imaging in Microscopy and Ophthalmology; Springer: Cham, Switzerland, 2019; pp. 59–85. [Google Scholar] [CrossRef]
- Marvasti, F. Nonuniform Sampling: Theory and Practice. Springer: Berlin/Heidelberg, Germany, 2012. [Google Scholar]
- Shannon, C.E. Communication in the Presence of Noise. Proc. IRE 1949, 37, 10–21. [Google Scholar] [CrossRef]
- Liao, J.; Li, C.; Huang, Z. A Lightweight Swin Transformer-Based Pipeline for Optical Coherence Tomography Image Denoising in Skin Application. Photonics 2023, 10, 468. [Google Scholar] [CrossRef]
- Liao, J.; Yang, S.; Yang, S.; Zhang, T.; Li, C.; Huang, Z. Fast Optical Coherence Tomography Angiography Image Acquisition and Reconstruction Pipeline for Skin Application. Biomed. Opt. Express 2023, 14, 3899–3913. [Google Scholar] [CrossRef]
- Wang, R.K.; Zhang, A.; Choi, W.J.; Zhang, Q.; Chen, C.-L.; Miller, A.; Gregori, G.; Rosenfeld, P.J. Wide Field OCT Angiography Enabled by 2 Repeated Measurements of B-Scans. Opt. Lett. 2016, 41, 2330. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.A. Statistical Methods for Research Workers. In Breakthroughs in Statistics: Methodology and Distribution; Kotz, S., Johnson, N.L., Eds.; Springer: New York, NY, USA, 1992; pp. 66–70. ISBN 978-1-4612-4380-9. [Google Scholar]
- Kendall, M.G. The Advanced Theory of Statistics; Charles Griffin & Co., Ltd.: London, UK, 1946. [Google Scholar]
- Fürnkranz, J.; Chan, P.K.; Craw, S.; Sammut, C.; Uther, W.; Ratnaparkhi, A.; Jin, X.; Han, J.; Yang, Y.; Morik, K.; et al. Mean Squared Error. In Encyclopedia of Machine Learning; Springer: Boston, MA, USA, 2011; p. 653. [Google Scholar] [CrossRef]
- Wang, Z.; Bovik, A.C.; Sheikh, H.R.; Simoncelli, E.P. Image Quality Assessment: From Error Visibility to Structural Similarity. IEEE Trans. Image Process. 2004, 13, 600–612. [Google Scholar] [CrossRef] [PubMed]
- van den Boomgaard, R.; van Balen, R. Methods for Fast Morphological Image Transforms Using Bitmapped Binary Images. CVGIP Graph. Models Image Process. 1992, 54, 252–258. [Google Scholar] [CrossRef]
- Liao, J.; Zhang, T.; Li, C.; Huang, Z. U-Shaped Fusion Convolutional Transformer Based Workflow for Fast Optical Coherence Tomography Angiography Generation in Lips. Biomed. Opt. Express 2023, 14, 5583–5601. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Projection Generation Methods | Evaluation Metrics | ||
|---|---|---|---|
| PSNR | SSIM | Processing Time (s) | |
| Traditional summation projection | 31.45 ± 4.45 | 0.85 ± 0.08 | 1.76 ± 0.02 |
| RUPP w/o DS a | 18.63 ± 4.03 | 0.64 ± 0.09 | 0.066 ± 0.0025 |
| RUPP w/DS b | 18.49 ± 4.11 | 0.63 ± 0.09 | 0.040 ± 0.0054 |
| Projection Generation Methods | Evaluation Metrics | ||
|---|---|---|---|
| PSNR | SSIM | Processing Time (s) | |
| wED | 20.98 ± 1.34 | 0.67 ± 0.059 | 1139 ± 5.10 |
| aED | 17.64 ± 2.25 | 0.57 ± 0.076 | 11.59 ± 0.23 |
| bED | 16.44 ± 1.29 | 0.47 ± 0.085 | 7.01 ± 0.22 |
| SV | 15.55 ± 1.72 | 0.46 ± 0.095 | 4.97 ± 0.19 |
| RUPP-SV w/o DS a | 11.61 ± 1.52 | 0.18 ± 0.036 | 0.29 ± 0.0060 |
| RUPP-ED w/o DS b | 11.23 ± 1.53 | 0.12 ± 0.021 | 0.29 ± 0.0098 |
| RUPP-ED w DS c | 11.23 ± 1.51 | 0.12 ± 0.020 | 0.21 ± 0.0098 |
| RUPP-SV w/DS d | 11.58 ± 1.51 | 0.17 ± 0.036 | 0.15 ± 0.011 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, T.; Liao, J.; Zhang, Y.; Huang, Z.; Li, C. Robust Ultrafast Projection Pipeline for Structural and Angiography Imaging of Fourier-Domain Optical Coherence Tomography. Diagnostics 2024, 14, 1509. https://doi.org/10.3390/diagnostics14141509
Zhang T, Liao J, Zhang Y, Huang Z, Li C. Robust Ultrafast Projection Pipeline for Structural and Angiography Imaging of Fourier-Domain Optical Coherence Tomography. Diagnostics. 2024; 14(14):1509. https://doi.org/10.3390/diagnostics14141509
Chicago/Turabian StyleZhang, Tianyu, Jinpeng Liao, Yilong Zhang, Zhihong Huang, and Chunhui Li. 2024. "Robust Ultrafast Projection Pipeline for Structural and Angiography Imaging of Fourier-Domain Optical Coherence Tomography" Diagnostics 14, no. 14: 1509. https://doi.org/10.3390/diagnostics14141509
APA StyleZhang, T., Liao, J., Zhang, Y., Huang, Z., & Li, C. (2024). Robust Ultrafast Projection Pipeline for Structural and Angiography Imaging of Fourier-Domain Optical Coherence Tomography. Diagnostics, 14(14), 1509. https://doi.org/10.3390/diagnostics14141509